
Abstract
The aim of this paper is to empirically examine the influence of organizational context on the implementation effectiveness of human resource management (HRM) practices with the aim of maintaining the health and well-being of employees, known as health promotion programs (HPPs). HPPs are a strategic function in HRM and play a crucial role in creating and maintaining human capital. Effective implementation is typically viewed as a critical prerequisite for the success of HPPs. By exploring the influence of organizational context on the implementation of HPPs, this paper offers a fresh approach to understanding HRM implementation in a relatively neglected area of research. To uncover contextual influences a multiple-case study in four German organizations operating in the chemical industry was conducted. Data was collected using a multi-method design consisting of an analysis of documents and 28 semi-structured interviews. The study is among the first to apply the categorical model of context by Johns to the investigation of the implementation of health promotion programs. The results contribute to a more nuanced view of HRM implementation by highlighting the interrelationships between contextual factors stemming from the physical, social, and task context and implementation fidelity. By providing initial empirical evidence of the mechanisms underlying this relationship, this study sheds light on the complexity and breadth of contextual influences during the implementation of HPPs and offers several theoretical and practical implications.
Introduction
Due to aging workforces, shrinking labor supply, and increasing work demands, the creation of safe and healthy workplaces is becoming a key concern for organizations in the western world (Sonntag and Stegmaier, 2015). To contribute to the health and well-being of their employees’ organizations are increasingly relying on health promotion programs (HPPs). In Germany alone, 26% of organizations implemented HPPs in recent years and a further 37% are currently implementing HPPs (Bieling et al., 2015; Walter and Krapf, 2017). HPPs can be defined as coordinated and systematic approaches to manage health and safety risks, covering areas such as health management, ergonomic work design, and sports programs. Due to their focus and scope, HPPs are considered to be an integral part of HRM (Brandl and Fink, 2009; Zwetsloot et al., 2010). While there seems to be little doubt that well designed and implemented HPPs can reduce illness and injury-related costs, increase productivity, and improve recruitment and retention (Hasson et al., 2014; Lerner et al., 2013; Weiner et al., 2009), studies suggest that implementation failures frequently undermine the effectiveness of these programs (Augustsson et al., 2015; Carroll et al., 2007).
For this reason, the investigation of why implementation failures occur and how they can be avoided has been receiving an increasing amount of attention within both the HRM (Bondarouk et al., 2016) and occupational health and safety (OHS) literature (Nielsen and Randall, 2013). Most existing studies are focused on the different HRM actors involved in the implementation, most notably line managers (LMs), HR professionals, and senior management (Hasson et al., 2014; Stanton et al., 2010; Trullen et al., 2016). However, it has been increasingly recognized that the influence of these actors is affected by the context in which the implementation occurs (Bondarouk et al., 2018; van Mierlo et al., 2018). Research into the conditions under which context enables or prevents effective implementation is therefore considered a prerequisite for better understanding why implementation failures occur and how they can be avoided. However, despite repeated calls for a more refined treatment of context in the HRM literature, research to date has overwhelmingly acknowledged context in a narrow and static way (Bondarouk et al., 2016; Cooke, 2018; Lundmark et al., 2020). In general, OHS research remains poorly integrated into the field of HRM, even though promoting employee health and well-being is a key area of HRM. Moreover, idiosyncrasies or determinants of the implementation of HPPs have been largely neglected in HRM research (Fan et al., 2020; Harney and Collings, 2021).
The aim of this study is to address these gaps by answering the following question: How and why does the organizational context influence the implementation of HPPs? Drawing on the categorical model of context by Johns (2006) this study specifically examines the influence of the contextual dimensions of physical, social, and task context on the implementation fidelity of HPPs through a multiple-case study conducted in four German organizations. In doing so, it provides a new angle of analysis and addresses the call for the contextualization of implementation research (Bondarouk et al., 2016; Cooke, 2018). The central contribution of this article is the conceptualization of the mechanisms through which contextual factors across the different contextual dimensions influence the implementation fidelity of HPPs. These mechanisms form the basis of a preliminary conceptual framework, which illustrates the interrelationships between the contextual dimensions and implementation fidelity. By outlining these mechanisms, this study contributes to a more nuanced and holistic conceptualization of context as an antecedent of effective implementation. Moreover, by exploring the implementation of HPPs from the perspective HRM, the study sheds light on the idiosyncrasies of HPP implementation and addresses the call to integrate research on OHS and HRM (Fan et al., 2020; Harney and Collings, 2021; Trullen et al., 2020).
Theoretical background
Implementation has been conceptualized as a dynamic process “during which relevant HRM actors (such as line managers, HRM professionals, employees) engage with it [the HRM practices], interacting among themselves and attempting to shape it to fit their requirements and needs” (Trullen et al., 2020: 155). Effective implementation is considered to be a prerequisite for HRM programs and practices to address the needs of an organization and its employees (Chow, 2012; Trullen et al., 2016). Within the OHS literature, implementation effectiveness is typically measured in terms of the “implementation fidelity.” It is conceptualized as the adherence of the HRM actors to the intended design of the HPP and the coverage of the program, that is, whether all employees who should benefit from an HPP actually do so (Augustsson et al., 2015; Carroll et al., 2007). Empirical evidence clearly indicates that both lack of adherence and coverage can undermine the effectiveness of otherwise well-designed HPPs (Cunningham et al., 2020; Nielsen and Abildgaard, 2013).
Implementation of HRM practices in general and HPPs in particular is considered to be a complex process, that entails the adaptation of processes and the involvement of numerous organizational actors (Hasson et al., 2014). While the literature suggests that HR professionals hold primary responsibility for the implementation and application of HPPs, studies also show an increasing devolution of responsibilities for HRM practices including health management to LMs (McDermott et al., 2015; Sheehan, 2005; Van Buren et al., 2011). Unsurprisingly, most of the existing research regarding implementation within both the HRM and OHS literature has been focused on the way personal resources, attitudes, and behaviors of these actors influence implementation outcomes (Bos-Nehles et al., 2013; Hasson et al., 2014; McDermott et al., 2015). Studies in the field of HRM identified numerous barriers to an effective implementation of HRM practices, including lack of knowledge, experience, or motivation of LMs (Bos-Nehles et al., 2013; Purcell and Hutchinson, 2007), as well as lack of guidance, support, or involvement from senior management and HRM professionals (Link and Müller, 2015; McDermott et al., 2015; Stanton et al., 2010; Trullen et al., 2016). These findings have been echoed within the OHS literature, where line managers’ readiness for change, workload, and attitudes toward health management as well as the involvement and support of senior managers and HRM professionals were identified as factors influencing the implementation fidelity of HPPs (Augustsson et al., 2015; Hasson et al., 2014; Mellor and Webster, 2013).
Together, these studies provide important insights into the role and influence of these actors and made a valuable contribution toward a better understanding of the implementation process. However, it has been increasingly recognized within both the HRM and OHS literature that these actors do not act within a vacuum. Each organization is characterized by a unique context that shapes the personal resources and interactions among these actors and, as a result, implementation fidelity. Thus, the influence of these actors on the effectiveness of implementation cannot be understood without considering the context in which the implementation occurs (Bondarouk et al., 2016; Bos-Nehles and van Riemsdijk, 2014; Mirfakhar et al., 2018). Therefore, if we are to gain a better understanding of the conditions needed for HRM actors to efficiently implement HPPs, considering the influence of context is crucial (Cooke, 2018; Johns, 2006).
To date, however, most studies have acknowledged context in a narrow and static way, by treating context as a single variable or by relegating contextual characteristics to the status of “control variables” (Cooke, 2018). For example, Bos-Nehles et al. (2013) found that the organizational context has a strong influence on the competencies of LMs, the effort they devote to implementation and the way they are supported. However, as they controlled for context only in terms of the industry in which the organizations operated, they were unable to explain how or why this influence occurs. Similarly, based on the assumption that smaller organizations lack the resources and capabilities to implement more complex HRM practices, such as HPPs, size or structure have frequently been investigated as contextual factors in implementation research (Brandl and Fink, 2009; Harris et al., 2014; McLellan et al., 2015; Saksvik et al., 2002; Trullen et al., 2016; Watson et al., 2006). However, studies regarding the influence of organizational context on implementation effectiveness provided only inconsistent or even contradictory results.
This clearly shows that focusing on broad, overarching aspects of context such as size or industry, as well as limiting context to a single variable, does not do justice to the diverse and multi-facetted nature of “context.” Thus, to explain how and why context influences implementation outcomes, one should take a full range of contextual factors into account. Johns (2006) provides one of the most comprehensive and frequently cited categorical models of “context” (Cooke, 2018; Johns, 2017; Lundmark et al., 2020; McDermott et al., 2013; Nielsen and Randall, 2013). He defines “context” as “situational opportunities and constraints that affect the occurrence and meaning of organizational behavior as well as functional relationships between variables.” (Johns, 2006: 386) and differentiates between omnibus and discrete contexts. Omnibus context refers to the broad, overarching aspects of context, which can be exemplified through the journalistic imperatives of reporting who, what, when, where, and why something is investigated (Bell et al., 2018; Johns, 2017). Nested within the omnibus context is the discrete context, which represents “the particular contextual variables or levers that shape behaviour or attitudes.” (Johns, 2006: 391). It consists of three interrelated contextual dimensions: the task, social, and physical context.
The task context refers to contextual features that are related to specific work requirements such as uncertainty, accountability, and autonomy. For example, the implementation of HPPs can add conflicting duties to the already extensive list of tasks performed by different HRM actors. Thus, a lack of guidance, training, or support might strain the limited resources in terms of time and energy, these actors have at their disposal and, as a result, undermine implementation (Bos-Nehles et al., 2013; Lundmark et al., 2020; Nielsen et al., 2010b).
The social context is related to the interpersonal elements of context. Given that an effective implementation rests on the collaboration of several HRM actors (Trullen et al., 2020), factors such as organizational culture, climate, or spans of control can influence the involvement and interactions of LMs and other relevant HRM actors (Lundmark et al., 2020; Saksvik et al., 2002; Stirpe et al., 2015).
Finally, the physical context refers to contextual elements of the built environment (Bell et al., 2018; Johns, 2006; McDermott et al., 2013). This might include where organizations or their subsidiaries are located, the layout of buildings or machinery, and the nature or interdependence of workflows. It could, for instance be suggested that the implementation within larger, international organizations is more difficult due to the greater need for coordination between different actors (Mirfakhar et al., 2018; Nielsen and Randall, 2013).
Johns (2006) suggests that factors across these three dimensions are interrelated and can have countervailing effects, that is, a supportive social context might countervail a lack of resources (Johns, 2006, 2017). Together, these factors and their interrelationships are expected to mediate the impact of the omnibus context and influence organizational actors’ behaviors and attitudes (Johns, 2006; Lundmark et al., 2020). Thus, to understand what conditions are needed for HRM actors to efficiently implement HPPs, a full range of discrete contextual levers (and their interactions) must be considered.
However, while the conceptualization by Johns (2006) has repeatedly been identified as a particularly useful approach to illuminate contextual effects, studies, to date, have largely explored contextual factors in a piecemeal fashion, and insights into the role of the organizational context are still limited (see e.g. Lundmark et al., 2020; Nielsen and Randall, 2013; Stirpe et al., 2015). To date, no integrated model or theory of contextual effects has emerged, and it remains largely unknown which discrete contextual factors influence implementation fidelity, and whether or how they are interrelated.
This study draws on the model of Johns (2006) as a starting point for the collection and analysis of data (Eisenhardt, 1989) to explore how and why discrete contextual factors across the task, social and physical contexts influence the implementation of HPPs. By focusing on a full range of discrete contextual effects, this study provides a new angle of analysis and addresses the call for the contextualization of implementation research. Moreover, by delineating interrelationships between contextual factors and implementation effectiveness it contributes to a more holistic understanding of contextual effects and provides a guide for further research (Bondarouk et al., 2016; Cooke, 2018).
Method
To this end, this study employs a multiple-case study approach (Eisenhardt and Graebner, 2007; Yin, 2018). 1 Qualitative studies are considered to yield particularly rich insights into the multifaceted nature of context while avoiding the “omitted variables problem” of many quantitative approaches (Cooke, 2018; Johns, 2006). Moreover, this research design is appropriate for addressing “how and why” questions within areas where there is little empirical substantiation, as targeted here. By enabling the replication of findings across cases, it facilitates the identification of constructs and their relationships (Eisenhardt, 1989; Ridder, 2017). The next sections outline the research setting and data collection. By addressing the questions of what, where, when, why, and who was studied, these descriptions reflect the omnibus context of this investigation (Bell et al., 2018; Johns, 2006).
Research setting
To answer the research question, the implementation of HPPs within four organizations operating in the chemical industry in northern Germany (where?) were investigated in 2016 (when?). This research setting is considered particularly appropriate for answering the research question for several reasons (why?). First, the chemical industry is characterized by a particularly high demand for skilled labor, physically demanding jobs, and a high average age of the workforce of above 50 years (Bundesarbeitgeberverband Chemie e.V, 2012). As such, the creation of safe and healthy workplaces is particularity important for organizations in this industry. Second, organizations within the chemical industry are subject to strong pressures from both the German government and social partners (i.e. trade unions and works councils) to adopt HPPs. For example, while the German government obliged organizations to implement reintegration management for physically or mentally challenged workers (“Betriebliches Eingliederungsmanagement (BEM)”), the social partners implemented a far-reaching collective agreement in 2008 called “Working life and Demography” (“Lebensarbeitszeit und Demografie”) to address the challenges associated with the demographic change in the chemical industry. Among other things, this collective agreement included best-practices recommendations for the design of HPPs and strongly encouraged their implementation (Flynn et al., 2013; Schröder et al., 2014).
As a result, all investigated organizations have implemented similar HPPs during the same time (what?). Although they differed in scope and complexity, all organizations adopted reintegration management, company sports programs, as well as occupational safety and health management practices, including risk assessments, regular medical check-ups, and ergonomic work-design (see Table 1).
Omnibus context (case overview and summary of data collection).
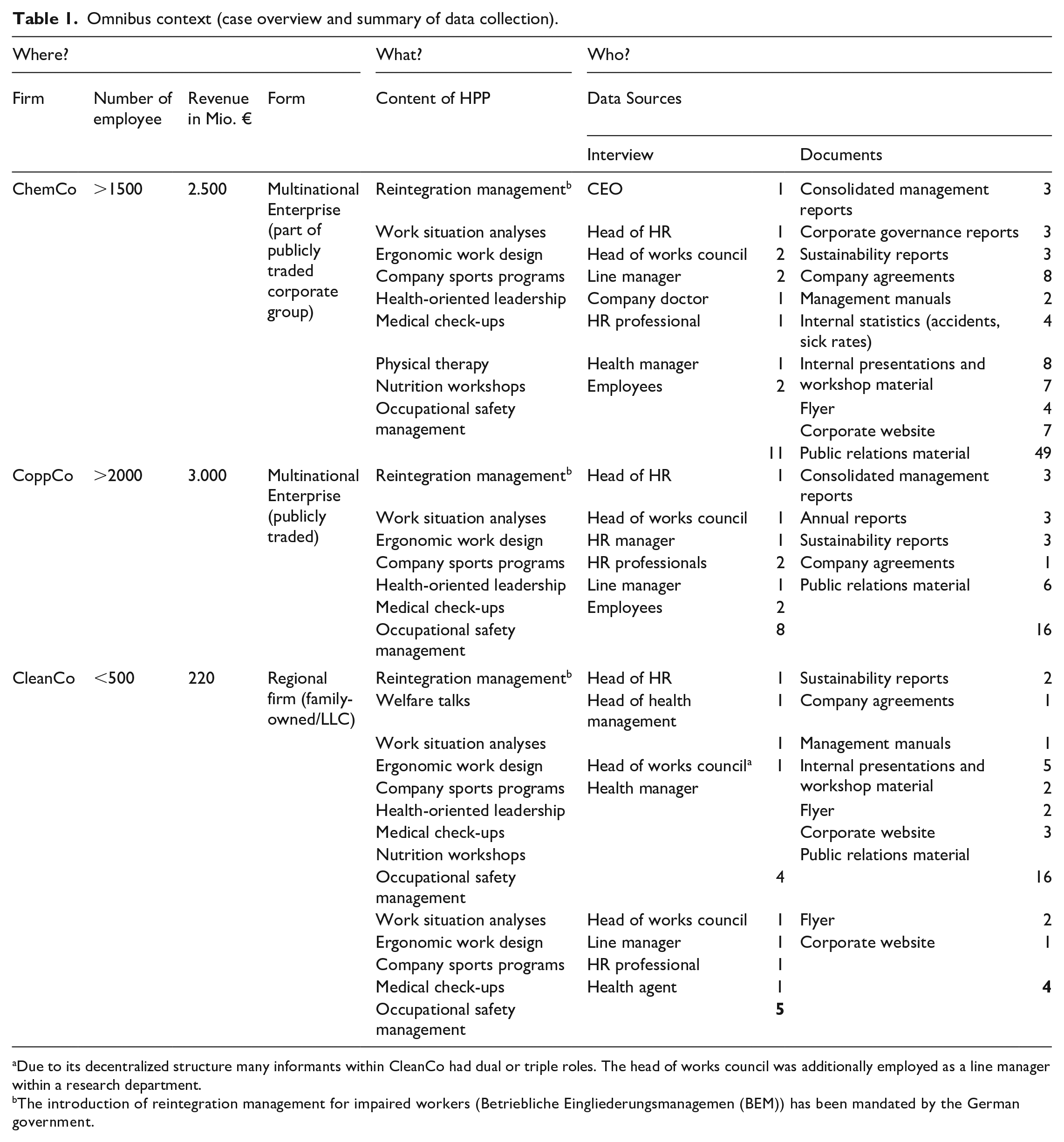
Due to its decentralized structure many informants within CleanCo had dual or triple roles. The head of works council was additionally employed as a line manager within a research department.
The introduction of reintegration management for impaired workers (Betriebliche Eingliederungsmanagemen (BEM)) has been mandated by the German government.
Finally, to facilitate the replication of the findings and provide particularly detailed insights into contextual effects (Eisenhardt and Graebner, 2007; Yin, 2018), two small- and medium-sized enterprises (SMEs), CleanCo and PlastCo, and two multinational enterprises (MNEs), ChemCo and CoppCo were investigated. 2 Although HPPs are applicable regardless of the size of the organization, organizational size has been widely viewed as a particularly important contextual factor. Therefore, it can be expected that the systematic replication of findings across organizations of different sizes provides detailed insights into whether and how size leads to variations in the physical, social, and task contexts and, as a result, implementation fidelity.
Data collection
To facilitate triangulation, the study employed a multi-method design consisting of two data sources: an analysis of documents and semi-structured interviews (see Table 1 for an overview) (Eisenhardt, 1989).
In total, more than 1000 pages of documents (e.g. bylaws, company agreements, and annual reports) were collected and analyzed. Consistent with previous studies, the main source of data were 28 semi-structured interviews, lasting between 45 and 90 minutes (see e.g. Piening et al., 2014; Trullen et al., 2016). To avoid information bias and to capture comprehensive information about the implementation, this study followed the call to rely on multiple informants (Mirfakhar et al., 2018; Trullen et al., 2017). Interviews included the key HRM actors responsible for implementing the HPPs within each organization. They were identified through prior meetings with the heads of the HR departments or CEOs and included LMs, members of the senior management, HR professionals, as well as health management specialists and members of the work councils (who?). Due to a different distribution of tasks and responsibilities, the number and type of actors interviewed varied across cases (see Table 1).
The interview questions were informed by the conceptualization of task, social, and physical context as well as the HRM and OHS literature on implementation. For example, to assess the social context, informants were asked how tasks and responsibilities were allocated among different actors, whether and how they cooperated, and what kind of support they received during implementation. Finally, the interviews included questions about problems that occurred during implementation, as well as follow-up questions to issues raised by informants (see Supplemental Appendix 1 for more detailed information). Altogether more than 35 hours of interviews were recorded, transcribed, and anonymized.
The triangulation within and between data sources helped to elucidate divergent perspectives, interpretations, and observations, leading to a deeper understanding of the issue under investigation thus increasing the trustworthiness of findings (Flick, 2004; Stake, 2005). Moreover, tentative relationships identified during the initial data analysis were presented before panels consisting of the head of the HR department, HR professionals, and members of the works council for all participating organizations except CleanCo. 3 This practice, known as member checking, was used to determine whether these participants felt that the interpretations were accurate and to supplement and refine data analysis (Creswell, 2009).
Data analysis
Data analysis occurred in several iterative steps. In line with the underlying replication logic, the implementation of the HPP within each organization was treated as a distinct analytical unit (within-case analysis) (Yin, 2018). The within-case analysis began with the coding and compilation of data. Following the case study approach by Eisenhardt (1989), a priori constructs based on the conceptualization of context by Johns (2006) and the existing literature were used to guide the initial data analysis (Eisenhardt, 1989; Eisenhardt and Graebner, 2007).
During the second step, the data was condensed into “case histories,” containing details about the HPPs and the organizations (Bingham and Eisenhardt, 2011; Eisenhardt and Graebner, 2007). Next, the implementation fidelity was assessed and scored from high to low (Miles et al., 2014). Following the OHS literature, implementation fidelity was measured in terms of adherence to the intended design of the HPP and the coverage of employees (Carroll et al., 2007). To assess the implementation fidelity, the intended designs were evaluated by analyzing documents such as company agreements, annual reports, or employee manuals (see Supplemental Appendix 1). Adherence was assessed by comparing these intended practices with informants’ statements, which emerged in two ways: The first was in response to a nondirective request to describe the implemented and applied HPP. The second was in response to follow-up questions directly asking respondents to describe the implementation fidelity and discuss problems that occurred during the implementation.
During the final step of the within-case analysis, inferences about the contextual conditions were made by “working backwards” from the implementation fidelity scores to uncover how and why they were influenced by contextual factors (Eisenhardt, 1989; Johns, 2006). After gaining a good understanding of the individual cases, a cross-case analysis using replication logic was conducted (Eisenhardt and Graebner, 2007; Miles et al., 2014).
Using tables and charts, preliminary patterns were listed and systematically compared across cases. Based on these patterns, tentative constructs and their relationships were identified and symmetrically verified by cross-case analysis (Edmondson and Mcmanus, 2007; Eisenhardt, 1989). Being aware of the HRM and OHS literature, the data was examined for the emergence of these constructs. Combining theory generation and theory elaboration, it was also accounted for new and unexpected contextual factors (Bingham and Eisenhardt, 2011; Edmondson and Mcmanus, 2007). Using content-analytic matrices that contained these constructs, the conditions under which high or respectively low implementation fidelity occurred were repeatedly compared across cases until no new insights could be gained from the data (Miles et al., 2014).
Findings
Nine highly interrelated contextual factors across the physical, social, and task contexts that influence implementation fidelity have been identified. Table 2 portrays these contextual factors and their underlying concepts. which will be described in detail below.
Data structure.
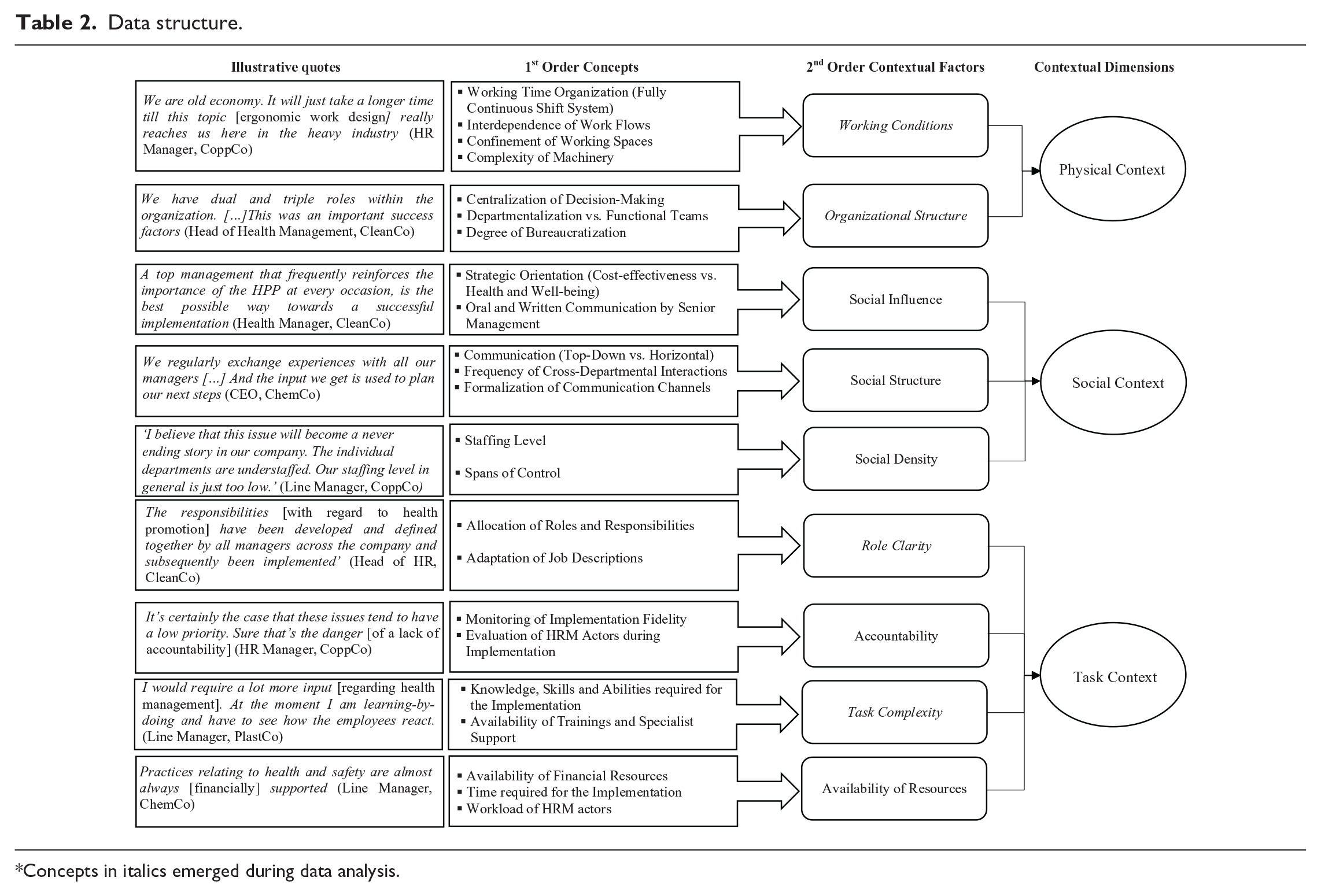
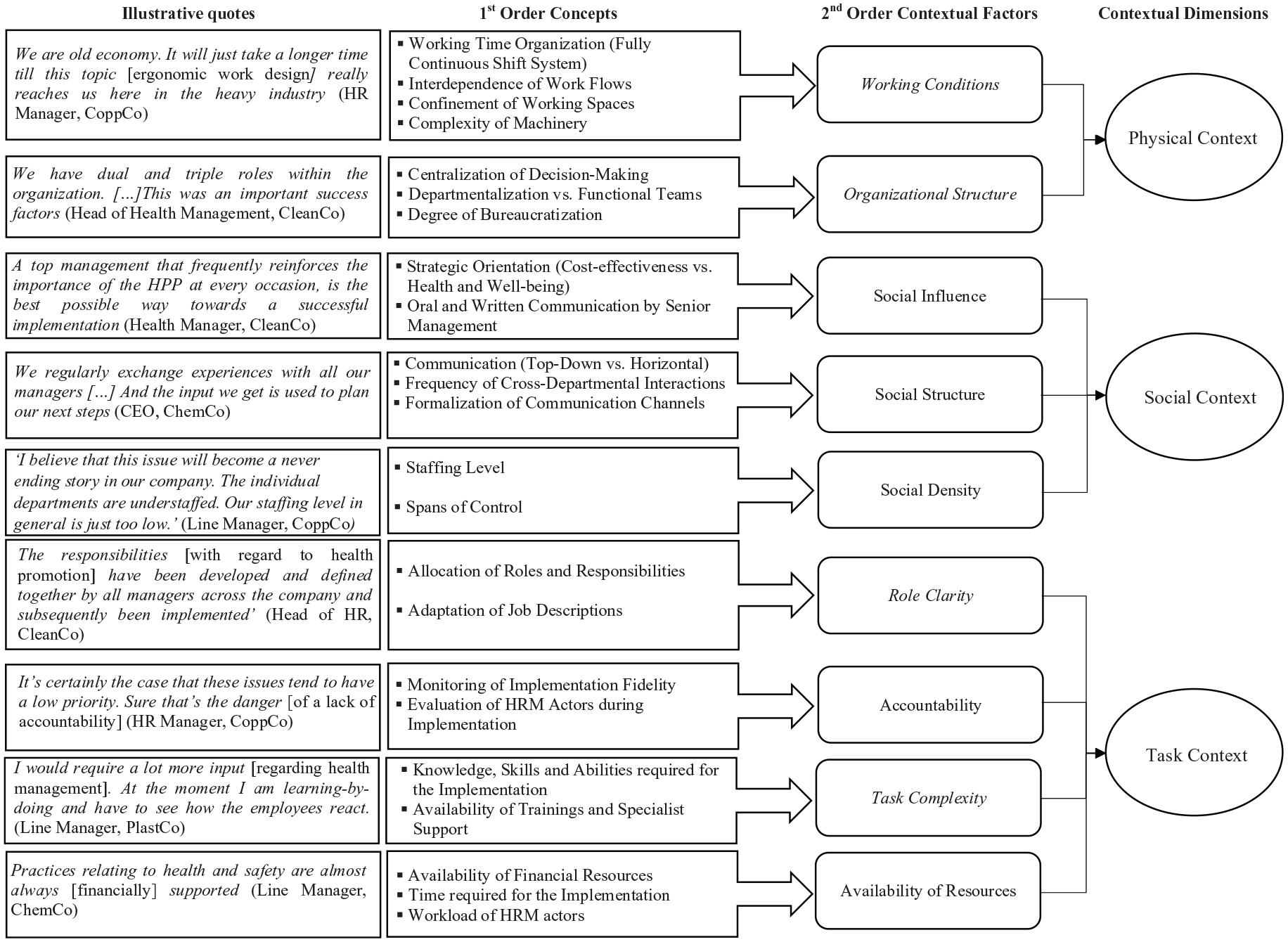
Concepts in italics emerged during data analysis.
Physical context
Two types of contextual factors, stemming from elements of the built environment were found to influence implementation fidelity (see Table 2). First, regarding the working conditions, the findings show that the nature of production processes, working spaces, equipment used, and the working time organization influence implementation fidelity. Multiple informants across the organizations noted, that due to the interdependence of production processes, confined working spaces, and the use of complex machinery, the implementation of ergonomic work design was only possible at high cost and time, as it required the purchase of new machines, a restructuring of work processes, and production downtime. Particularly at ChemCo and CoppCo, measures of ergonomic work design could only be implemented with high production downtime costs due to the fully continuous shift system (three shifts per day, every day of the week). In addition, the fully continuous shift system also reduced the HPPs coverage, as multiple employees were unable to participate in company sports or health management workshops: “Shift workers often do not have the opportunity to attend these events. Even if we offer several dates.” (Member of the HR Department, CoppCo).
The central role of appropriate working conditions for high implementation fidelity was also evident in CleanCo. The interviewees pointed out that comprehensive implementation of the measures was facilitated by the fact that the prerequisites necessary for this, for example, appropriately equipped workrooms and machinery, were taken into account in a planned expansion of the production facilities: “You can only do it [establish healthy working conditions] if you rebuild it [the production plants]. Luckily, we are now able to do that. We are currently expanding all our production sites, and we can make these changes in the process.” (Health Manager, CleanCo).
The organizational structure, that is, how activities such as task allocation, coordination, and supervision are organized, emerged as another important feature of the physical context. Although all organizations operated in the same industry, their structures differed significantly. The structures in CoppCo and PlastCo were highly mechanistic and characterized by rigid departmentalization, centralized decision-making, as well as a high degree of bureaucratization and division of labor. A common characteristic of both organizations was a high control over HRM tasks by centralized departments at the corporate headquarters (e.g. formulation and design of HRM strategies, policies, and practices). These departments not only decided on the content of the HPP, but also instructed the local units on how to implement it. The role of HR managers in the individual divisions was limited to relaying instructions and verifying compliance with rules and regulations. As HR managers were seen more as control authority than a source for support, LMs were hesitant to approach them for help or to address problems that occurred during implementation: “It is important to remember that our HR department has primarily a disciplinary and regulatory function. This sometimes makes the implementation more difficult.” (Head of HR, CoppCo).
In contrast, the matrix-organization of ChemCo and, even more so, the decentralized organic structure of CleanCo, was characterized by joint specialization, job-sharing, and the extensive use of cross-functional teams. Within these organizations, the headquarters only defined the strategic objectives and provided broad guidelines for the implementation. The individual units had a significant amount of discretion in adapting and implementing the HPPs. Moreover, the lower functional barriers between the departments facilitated a closer exchange and intensive collaboration during implementation: “Often it only needs an impulse. [. . .] Our department heads often know best how to approach these issues and just need a helping hand.” (Head of health management, CleanCo).
In sum, the data suggests that while working conditions influence whether and how measures can be implemented, the organizational structure influences the role of actors during implementation and how they interact with each other, thereby shaping the social and task context of implementation. In line with these findings, Figure 1 portrays the physical context as the largest and most distal contextual dimension, with others intersecting.

Influence of organizational context on the implementation effectiveness of health promotion programs.
Social context
Regarding the interpersonal aspects surrounding the implementation both subtle factors such as the social structure, that is, norms of communication and cooperation and the social density, as well as the social influence exerted by authority figures emerged as important factors.
Multiple informants noted that open and trustworthy communication and a close cooperation between the different HRM actors can help to avoid implementation failures, as it facilitates the clarification of ambiguities and the identification of problems: “The simplest and most effective way is to just talk to each other. And for that I require an open culture, which is actively lived here.” (Health manager, ChemCo).
However, data analysis suggests that the mechanistic structures of CoppCo and PlastCo restricted bottom-up communication, which reduced the ability of lower level HRM actors, such as LMs to provide feedback or seek support. Moreover, the rigid departmentalization was mentioned as a reason for limited interaction and cooperation between different functional areas and actors involved in implementation: “You would first have to change the entire leadership culture. The entire culture here is strictly hierarchical. So, if you really want it to work, you would require an open and trusting cooperation.” (Head of works council, PlastCo).
In contrast to that, informants within CleanCo noted that the use of cross-functional teams and flat hierarchies, contributed to more frequent interactions and close cooperation within and between different departments and functional areas: “We have dual and triple roles within the organization. [. . .] The chairman of the work council works within my department. We see each other frequently and there are no reservations between us. This was an important success factor.” (Head of health management, CleanCo).
In addition, social density was identified as another factor that shaped the social context of implementation. The data indicates that larger spans of control and a low staffing level further reduced interactions between the stakeholders and the time available for the implementation. Particularly the health management specialists, whose expertise was urgently needed for implementation, repeatedly mentioned a low social density as a factor that decreased the availability and quality of support. For example, while both ChemCo and CleanCo employed multiple health managers and established dedicated health management departments, PlastCo and CoppCo employed a single health agent each: “Because we are so big, we would need a department dedicated to health management. We only had a single person who worked part-time as a health agent.” (Chairman of works council, CoppCo).
Finally, the findings suggest that the social influence exerted by senior management affects, at least to some extent, the attitudes and behavior of the actors involved in the implementation. Both direct oral and written communication as well as the strategic priorities set by senior management were identified as powerful sources of social influence in this regard. In ChemCo and CleanCo, health promotion was a central component of the corporate strategy. The importance of health and well-being was also emphatically emphasized by senior management during workshops and company meetings. As a result, the stakeholders involved perceived the implementation of the HPP as a central part of their responsibilities (see Supplemental Appendix 1). In contrast, within CoppCo and PlastCo no strategic objectives regarding health and well-being were formulated prior to implementation: “It must be strategically integrated to communicate these things effectively. However, we neglected this and now we have to rectify it.” (Head of HR, CoppCo).
Instead, both companies were characterized by a strong focus on cost-effectiveness. As a result, the LMs frequently prioritized other, more tangible business objectives over their vaguely defined responsibilities regarding the implementation: “So far, it’s been more incidental. Everybody knows there’s something to do but I think that’s secondary for most people.” (Line manager, PlastCo).
Task context
The task context has been identified as the final and most proximal layer of context. On this dimension, four contextual factors were identified that influenced implementation fidelity: role clarity, accountability, task complexity, and the availability of resources.
Informants from all organizations noted that implementing comprehensive HPPs is very costly and time-consuming. Thus, the availability of the necessary resources in terms of both time and money emerged as a prerequisite for high implementation fidelity. Surprisingly, informants indicated that financial constraints were usually not a reason for low implementation fidelity. Only within PlastCo, were corporate headquarters halted investments due to a potential sale of a business unit, this was mentioned as a factor that undermined implementation: “At the moment we have huge problems [. . .]. Our group is trying to sell us [the business unit]. That means we are no longer getting any [financial] support from the group.” (Head of employee council, PlastCo).
In contrast, lack of time was of particular concern for actors within organizations characterized by low social density and large spans of control: “The departments simply become larger and you have to work more in the office and so on. You no longer spend time in the production area and you can’t deal with the equipment and employees. The line managers must be relieved so that they can take care of the implementation.” (Line manager CoppCo).
This was abetted by a lack of role clarity. Within CoppCo and PlastCo, roles and responsibilities for implementation were distributed only informally and often based on personal preferences. This further increased the need for coordination and time required for the implementation: “I know who is responsible for certain things, but not for others. But the responsibilities also change frequently [. . .]. Then, I must call the personnel department and ask: “Who is responsible and who can help me? Sometimes I must wait longer for an answer.” (Line manager, CoppCo).
Within ChemCo and CleanCo, on the other hand, tasks and responsibilities were clearly allocated to the individual HRM actors and their performance was frequently monitored and evaluated. Informants indicated that this led to a high accountability, which, along with the strong social influence exerted by senior management, ensured that the responsible actors prioritized implementation accordingly: “So lack of time cannot be a problem. We can ensure that they take their time. ‘I don’t have time’ means only ‘it is not important to me’.” (Head of health management, CleanCo).
Finally, task complexity was seen as a challenge for high implementation fidelity across the organizations. Multiple informants noted that the implementation of HPPs requires extensive knowledge and skills about issues such as health promotion, work processes, legislation, and an engaging leadership style. Within ChemCo and CleanCo, however, this task was shared among multiple knowledgeable actors including health management specialists, HR managers, and LMs. Facilitated by the high social density and collaborative social structure, this division of tasks reduced the perceived task complexity: “They [the health management specialists] usually know what has been done in other departments. They have the necessary knowledge and information that help us to find solutions to our specific problems.” (Line manager, ChemCo).
Within CleanCo, the task complexity was further reduced through extensive mandatory trainings and guidelines: “We decided to make the trainings obligatory. Otherwise, we wouldn’t have reached one-third of the managers. But now everybody has the same understanding of the topic.” (Head of health management, CleanCo).
In contrast, CoppCo and PlastCo were characterized by lower levels of knowledge sharing and support, which could be attributed to the lower social density and bureaucratic social structure. Moreover, although both organizations appointed health agents, they were formerly members of the HR department and had no prior experience with the implementation of HPPs. As a result, they were unable to efficiently support the implementation and decrease task complexity: “I would say that I have a different sense for this topic [health management] based on my meetings with the employees but I am still unable to see the bigger picture. [. . .] There is always something that you do not know about and this could be of importance for an employee.” (Health agent, PlastCo).
Linking context to effective HPP implementation
Based on the findings presented here, the next section will be used to develop a tentative framework, specifying the conditions under which certain contextual characteristics contribute to or undermine implementation fidelity. Table 3 summarizes the patterns between contextual factors and implementation fidelity observed across the organizations and, hence, forms the basis for developing the tentative framework. As shown in Table 3, the analysis revealed that the four cases vary in their implementation fidelity due to differences in their physical, social, and task context.
Patterns of context and implementation effectiveness.

While CleanCo managed to implement the HPPs as intended and achieve high implementation fidelity, departmental differences and a lack of coverage undermined the implementation fidelity within ChemCo. Nonetheless, many aspects of the HPP were consistently implemented across the organization, leading to a medium implementation fidelity (See Table 3). In contrast to that, PlastCo and CoppCo only achieved a low implementation fidelity. Within both organizations, the HPPs were only partially or inconsistently implemented and unavailable for large parts of the workforce: “I will be totally honest, many of these things have not really been implemented. Some things are just incredibly tedious.” (HR-manager, CoppCo).
Interrelationships among the contextual factors across the contextual dimension are vital for understanding these differences in implementation fidelity. It is striking that the implementation fidelity between ChemCo and CoppCo differs significantly from each other although the physical context is similar (i.e. large multi-national organizations, fully continuous shift systems, and highly structured workflows). Based on this, the physical context has been conceptualized as the most distal contextual dimension that provides the backdrop for the influence of more subtle contextual factors related to the social and task context.
The cross-case analysis suggests that a strategic focus on health and well-being, and a social structure that increases communication and cooperation, as well as support by experienced health management professionals (i.e. the social context) are common underlying factors that support high implementation fidelity. Specifically, the cases reveal that a social context characterized by a high social density and collaborative social structure provides opportunities to clarify ambiguities and seek support regarding the implementation, and as a result is likely to increase implementation fidelity. Similarly, social influence of senior managers affected the perceived importance of health and well-being and effort devoted to the implementation of the HPPs.
Yet, the data also shows that the organizational structure (i.e. physical context) influences the potential to exert social influence. This is reflected in the cases of ChemCo where the large hierarchical and geographical distance between senior management, LMs and employees prevented direct social influence: “This topic [health management] is frequently promoted from the top-management but I think it gets lost in translation. I frequently ask myself if we really reach the managers on the lower levels or if it gets lost somewhere along the way.” (Head of works council, ChemCo).
Moreover, the case data suggests that the high or respectively medium implementation fidelity in ChemCo and CleanCo can also be traced to contextual factors stemming from the task context, including a clear allocation of roles and responsibilities, accountability as well as the perceived task complexity. However, these factors alone are insufficient for understanding the link between organizational context and the implementation fidelity of HPPs. Instead, the data yields a more nuanced picture in which the task context was also influenced by the social and physical context. The analysis reveals that a high social density and a supportive social structure decreased the perceived task complexity. In a similar vein, the social influence exerted by senior management increased the accountability of the LMs responsible for the implementation within ChemCo and CleanCo.
These findings are summarized in the tentative framework depicted below (see Figure 1). The depiction of the different dimensions of context as layered squares illustrates that the contextual dimensions are interrelated and the extent to which these dimensions are more distal (e.g. physical context) or proximal (e.g. task context) to implementation fidelity. Consistent with the data, the framework indicates that the physical context influences implementation fidelity, through more proximal layers of context. For example, while working conditions, such as a fully continuous shift system or confined working spaces impede the implementation of measures such as company sports programs or ergonomic work design, other features of the physical context, such as the size and structure of the organization influences implementation fidelity through its impact on the social context. Similarly, the framework shows that the social context influences elements on the task context and thereby implementation fidelity. An example would be, that that a supportive and collaborative working environment and a high social density increase the availability and quality of support, thereby reducing the perceived task complexity. Finally, the framework depicts the task context as the most proximal layer of context.
Discussion and conclusion
Repeated calls have been made to for the investigation of contextual influences in research on implementation in general (Cooke, 2018; Mirfakhar et al., 2018; Trullen et al., 2020) and with regard to HPPs specifically (Augustsson et al., 2015; Lundmark et al., 2020; Nielsen and Miraglia, 2017). By exploring the impact of a broad range of discrete contextual factors on the implementation fidelity of HPPs, the findings contribute to a more nuanced view of HRM implementation as previous research has widely ignored contextual influences or relegated contextual characteristics to the status of “control variables.”
The main contribution of this study is the conceptualization of the relationships between contextual factors stemming from the physical, social, and task context and implementation fidelity as well as their interrelationships (depicted in Figure 1). The findings highlight, that context is a broad, multi-dimensional construct. Thus, to gain insights into why implementation failures occur and how they can be avoided, the interrelationships among a variety of different contextual factors across different contextual dimensions need to be considered. By providing initial empirical evidence of these interrelationships, this is one of the first studies to provide insights into the complexity and breadth of contextual influences on the implementation process, as well as several theoretical and practical contributions.
Theoretical implications
First, at a broad level, this study supports previous findings that the implementation of HPPs is a complex and cross-disciplinary process involving multiple stakeholders in which implementation failures frequently undermine the adherence to the intended HPPs and the coverage of employees (Augustsson et al., 2015; Carroll et al., 2007; Nielsen and Randall, 2013). Out of the four investigated organizations, only one managed to implement the HPPs as intended, while in two organizations, CoppCo and PlastCo, large parts of the HPPs were not or only inconsistently implemented and applied.
In line with the HRM and OHS literature, LMs were identified as the actors primarily responsible for implementation (Bos-Nehles et al., 2013; Khilji and Wang, 2006). Furthermore, it was confirmed that LMs require support and guidance of HR professionals and senior management (see e.g. Hutchinson and Purcell, 2010; McDermott et al., 2015; Stirpe et al., 2015; Trullen et al., 2016). In addition, the study also highlights the central role of health management specialists during the implementation of HPPs, which has rarely been addressed in the OHS and HRM literature to date (Guennoc et al., 2019). The findings suggest that this type of specialized support is pivotal in implementing more complex and cross-disciplinary HR practices such as HPPs. As such, future research should move beyond its almost exclusive focus on LMs and HR professionals and start exploring the role and influence of other actors such as health management specialists or employee representatives, especially in the context of OHS.
Beyond that, the study also contributes to our knowledge regarding what supports effective collaboration between these actors during the implementation of HPPs (Khilji and Wang, 2006; McDermott et al., 2015; Purcell and Hutchinson, 2007). Specifically, it suggests that a greater geographical or hierarchical distance between these actors (physical context) as well as bureaucratic and hierarchical workflows and a low social density limits opportunities for interaction, and in turn, their ability to support the implementation.
In this regard, the findings extend prior research by showing that the role of these actors during the implementation is highly dependent on the context of the organization. For example, studies have frequently shown that LMs HR-related skills (Bos-Nehles et al., 2013; Evans, 2015; Trullen et al., 2016) and motivation for HR work (Bos-Nehles et al., 2006; McGovern et al., 1997; Whittaker and Marchington, 2003) influence implementation outcomes. The present findings suggest that the HR-related skills required for the implementation are at least partially determined by role clarity and social structure. A clear allocation of roles and responsibilities, and the support by well-staffed HR and health management departments can decrease perceived task complexity as it leads to a clearer understanding of what needs to be done for effective implementation. Similarly, the results illustrate that social influence exerted by senior management and the accountability of LMs likely influence the degree to which they proactively take charge of implementation, that is, their motivation.
Finally, while previous studies were primarily focused on individual contextual factors or relegated contextual factors to the status of mere control variables (Cooke, 2018; Johns, 2017), the present findings clearly emphasize the multi-dimensional nature of organizational context by highlighting the interrelationships between contextual factors across different contextual dimensions (Bell et al., 2018; Johns, 2006). For example, organizational size has frequently been investigated as a contextual factor affecting implementation outcomes (Bos-Nehles et al., 2013; Mirfakhar et al., 2018; Nielsen et al., 2010a; Saksvik et al., 2002). A common argument has thereby been that smaller organizations dispose of fewer resources and less professional HRM processes, which limits their ability to efficiently implement complex HR practices such as HPPs efficiently (Mirfakhar et al., 2018; Woodhams and Lupton, 2006). In contrast to that, this study suggests that organizational size itself has no direct influence on implementation fidelity. While it could be confirmed that the implementation of HPPs presupposes an allocation of resources and an adequate infrastructure of qualified experts, these factors were unrelated to the size of the organization. Instead, the findings provide initial evidence that smaller organizations can leverage their resources more efficiently. For example, due to its smaller size, CleanCo was characterized by a lower degree of formalization of corporate structures and communication, resulting in lower functional barriers between departments and management levels. This enabled the senior management to positively influence the implementation. Additionally, due to the low functional barriers and physical proximity, human resources, and health management professionals were often in direct contact with LMs and therefore more easily able to reduce the perceived task demands and increase role clarity. This allowed CleanCo to effectively support implementation with relatively few professionals.
In this regard, the study provides evidence that focusing purely on broad omnibus factors such as size or industry, oversimplifies the complexity underlying contextual influences. Instead, forthcoming studies should take a broader range of more proximal, discrete contextual factors and their interrelationships into account when studying implementation effectiveness.
Practical implications
From a practical perspective, the results indicate that organizational decision-makers need to be aware of these contextual influences and their interrelationships when planning and implementing HPPs. Important examples are the prevailing working conditions and the organizational structure (e.g. the physical context) as these factors have far reaching consequences for the implementation. For example, fully continuous shift systems may prevent some employees from taking in health promotion activities. Tailoring the design of the HPPs to the physical context, specifically the predominant working conditions, that is, interdependence of workflows, the kind of machinery used and the working time systems employed, might therefore be a first step to facilitate implementation.
Second, the results suggest that by creating greater opportunities for interaction, for example, by forming cross-functional teams or reducing functional barriers, the level and quality of support can be positively influenced, allowing problems to be resolved more efficiently during implementation.
Furthermore, adapting HRM processes might be another useful measure to improve implementation fidelity. For example, by simplifying reporting relationships, specifying roles and responsibilities during the implementation, and systematically monitoring the implementation process, organizations might be able to decrease (perceived) task complexity and increase accountability.
Moreover, while it has been argued that offering a HPP by itself, reflects some level of management support for health and well-being, the findings indicate that this message can be fragmented, indistinct, or inconsistent with other apparent priorities. To send a strong signal about the importance of health management, the promotion of health and well-being should be explicitly integrated into the corporate strategy and visibly emphasized by senior management.
Finally, the results illustrate that given the complexity and interdisciplinary nature of HPP implementation, health management professionals are needed in addition to HR specialists to support implementation. As such, practitioners should audit and if necessary, establish adequate support systems prior to the implementation. This might require hiring additional (health management) specialists or providing training and development opportunities for existing employees.
Limitations and future research
The findings of this case study should be considered in light of its limitations. To control for the influence of external factors, organizations that operated in the same country were chosen for the investigation. However, the investigated organizations were subject to strong pressures from both the German government and social partners, which could limit the generalizability of the findings. Nonetheless, this setting provided a unique opportunity to study organizations that implemented similar HPPs during the same period, which facilitated the exploration of the organizational context and the systematic replication of findings (Eisenhardt, 1989; Yin, 2018).
Furthermore, given the nature of the cases, the relative importance of the contextual factors, as well as countervailing effects, could not be assessed. However, it is likely that some of the contextual factors have a stronger impact on implementation fidelity than others. For it could be argued that when health and well-being are integrated into the strategic objectives, it will be more likely that relevant adjustments in the physical, social, and task context will be made, that is, by hiring additional health managers. Similarly, it was not possible to assess whether certain factors have substitutive or synergistic effects, for example, whether a supportive social context may be less needed in situations with lower task demands or whether accountability might be less important in contexts with a strong social influence. Finally, the performance implications of the HPPs implementation fidelity have not been assessed. Thus, it remains unknown whether the higher implementation fidelity within ChemCo and CleanCo led to the desired outcomes.
Future research may be conducted to address the abovementioned issues and to extend and validate the findings. For example, the relationships underlying the framework can be operationalized and tested within large-scale qualitative surveys or comparative case studies, to refine the framework and provide additional insights regarding the relative importance of each contextual factor. Additionally, longitudinal research designs might provide deeper insights into how contextual factors influence the implementation process over time to illuminate cross-level effects (Cooke, 2018). Similarly, forthcoming studies could be conducted in different settings (i.e. different countries or industries) to increase the generalizability of the framework and explore the influence of the external context on implementation fidelity.
Despite these limitations, this study provides in-depth insights into the diverse and multi-faceted nature of context and its influence on the implementation fidelity of HPPs. It is among the first to link contextual factors across different contextual levels to the implementation fidelity of HPPs. As such, it contributes to the contextualization of implementation research and can help practitioners to facilitate the implementation of HPPs.
Supplemental Material
sj-docx-1-gjh-10.1177_23970022221108117 – Supplemental material for Putting implementation into context: Exploring the influence of physical, social, and task contexts on the implementation of health promotion programs
Supplemental material, sj-docx-1-gjh-10.1177_23970022221108117 for Putting implementation into context: Exploring the influence of physical, social, and task contexts on the implementation of health promotion programs by Maximilian Tim Roehl in German Journal of Human Resource Management: Zeitschrift für Personalforschung
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.