
Abstract
Confronted with the problem of ageing populations since the 1990s, many European welfare states have massively expanded public support for the care of the elderly. This expansion occurred during the neoliberal era in which the marketisation of social services was high on European countries’ political agendas. There are many studies concerned with cross-national differences between national policies regarding the marketisation of care, but little comparative research has been carried out at the local level. This article is innovative in that it explores the role of welfare cultures and local governance structures in local policies regarding the marketisation of long-term care (LTC). We present the findings of a historical comparative case study of four medium-sized cities in Germany for the period 1995–2007. Our empirical study took a multi-level approach to exploring the extent to which the central German state affords local governments operational autonomy for LTC marketization, then analysed the differences in local policies regarding LTC marketisation. According to our findings, German LTC policies are rather centralised and afford local governments operational autonomy towards marketisation only in a few fields. In these fields, local LTC policies differ substantially between eastern and western German cities. We find that differences in the relevant political actors’ main cultural ideas and in local governance structures contribute to this variation, whereas the financial and demographic differences that were analysed do not.
Introduction
Since the 1990s, as a reaction to the challenges of an ageing population, many European welfare states have considerably increased financial support and public provisions for long-term care (LTC) of the elderly (Bode, 2012; Ranci and Pavolini, 2013; Theobald, 2015). This restructuring of societal organisation as it pertains to care work overlaps with another major change in European welfare states, namely the strengthening of market principles in the organisation of social welfare service provision (Brennan et al., 2012; Burau et al., 2017; Clarke et al., 2007; Streeck, 2009).
In the academic debate and research around the restructuring of welfare state policies regarding LTC marketisation, the primary focus has been on welfare state policies at the central state level (Kleider and Silva Lopes, 2021), whereas local policies regarding LTC marketisation have received relatively little attention. This apparent lack of interest may be due to the common assumption that local-level policymaking simply reflects the central welfare state’s LTC policies. Contrary to this assumption, several scholars stress the role of local governments in the organisation of care provision and local variations in LTC policies (Kazepov, 2010; Trydegård and Thorslund, 2010). On this basis, our research addresses differences between local LTC policies regarding LTC marketisation. We aim to explore how such differences can be explained.
This paper contributes to the existing literature in that it emphasises the role of welfare cultures and local governance structures in explaining the differences between local policies regarding LTC marketisation. Our primary assumption is that differences in what the main political actors, as a product of their cultural orientations, consider ‘ideal’ ways of organising LTC—along with differences between municipal LTC governance structures—are relevant to explaining the differences between policies. In our definition, ‘culture’ comprises a set of (potentially diverse, contradictory and changeable) values, ideals and belief systems about a ‘good’ society and (morally) ‘good’ behaviour at a society’s macro level—in sum, ‘cultural ideas’ towards which people orient their behaviour (Pfau-Effinger, 2005). We use the term ‘local governance structures’ to refer to locally established relationships between the relevant public and non-public actors in the field of social policy (Och, 2017).
We evaluate these assumptions in a historical comparative case study on local LTC policies in the German welfare state for the period 1995–2007. During this period, the marketisation of public infrastructure and, in particular, of care services played an important role in the German welfare state’s political discourses and reforms. Our study includes four medium-sized cities in eastern and western Germany. Germany’s local LTC policies are interesting to study because the central welfare state introduced a groundbreaking reform of LTC policies in the mid-1990s, based on the introduction of social care insurance and a massive strengthening of the role of the central state in LTC regulation, together with a relatively strong enforcement of LTC marketisation (Daly et al., 2022). This policy turn was confronted with the significantly different historical backgrounds of local LTC policymaking between East and West Germany.
Our study takes into consideration that the policies of local governments are embedded in a division of responsibilities, tasks and power between the central state and the local level that may differ cross-nationally regarding the degree of centralisation/de-centralisation and the extent to which the central state affords local governments operational autonomy (Hendrikse, 2015; Jensen and Lolle, 2013). The empirical study therefore takes a multi-level approach to exploring the extent to which the central German state leaves local governments room to manoeuvre local LTC policies, then analyses the local differences between policies regarding LTC marketisation. The study is based on a triangulation of methods, using in-depth analyses of policy documents and public statistics, interviews with 10 local experts on LTC policies, and 28 semi-structured, theme-centred interviews with relevant actors in local social policy decision-making on LTC.
Section 2 discusses the state of research in in regard to marketisation of LTC. Section 3 introduces the theoretical framework; Section 4 explains the study’s methodological approach; and Section 5 presents the findings. The paper concludes with Section 6.
Literature overview
Marketisation of care in European welfare states
The welfare state has long been considered an institution that aims to organise social solidarity and restrict the potential of markets to create social risks and exclusion (Esping-Andersen, 1990). However, since the 1990s, many welfare states have been restructured according to principles of marketisation (e.g., Bode, 2012; Gingrich, 2011; Klenk and Pavolini, 2015) such as provider competition, the outsourcing of care services to for-profit providers, and the transformation of citizens requiring care into ‘consumers’ who ‘buy’ care services in ‘care markets’. During the 1990s and 2000s, such reforms were propagated by the Organization for Co-operation and Development (OECD), the European Union (EU) and national governments, with the argument that markets and consumer choice are particularly efficient ways of organising LTC (Bode, 2012; Brennan et al., 2012; Gingrich, 2011; Theobald, 2015; Vabø, 2006).
Several authors have stressed that the increasing popularity of neoliberal ideas in the early 1990s’ discourse on the welfare state was an important precondition for the major role that market principles have played in welfare state reforms. Neoliberalism resembles classical liberalism in that it views liberty, universalism, the free market, a weak role of the state in the provision of welfare and the self-reliance of the social citizen as the main principles of a functioning economy and society (Eggers et al., 2019; Frericks and Höppner, 2019). However, it places even more stress on the priority of market principles, the enforcement of which is considered to be a main task of the state (Harvey, 2005; Slobodian, 2018; Streeck, 2009). The demand for social policies that emerge from such ideas has led to the ‘marketisation of policies’, i.e. deregulation, privatisation, reductions in social spending (Brennan et al., 2012; Clarke et al., 2007; Gingrich, 2011).
During the welfare state reforms of the last few decades, market principles have also been strengthened in European welfare states’ LTC policies. The public provision of social services declined substantially as contractualisation and outsourcing brought parts of these services into the market (Gilbert, 2015). Additionally, the establishment of competition among provider organisations led to a substantial increase in the share of for-profit providers (Brennan et al., 2012). With the introduction of the Long-Term Care Insurance Act (SGB XI) at the central-state level in 1995/1996, the German welfare state’s LTC policies have also promoted LTC marketisation (Pfau-Effinger et al., 2008; Rothgang, 1997).
Explaining variation in the marketisation of local LTC policies
There are many studies about cross-national differences among national policies regarding the marketisation of care (see Theobald 2015), but comparative studies at the local level are rare. Some authors argue that the positioning of governing political parties on the left/right spectrum is relevant to explaining cross-national differences in the extent of social service marketisation (see Gingrich 2011). According to this argument, social democratic parties are less oriented towards marketisation than conservative and liberal parties are, as this orientation may contradict their electorates’ interests (Allan and Scruggs, 2004; Hibbs, 1977). However, this argument, which is based on partisan theory, has been contested by authors arguing that there are also left-wing political actors endorsing the choice with which markets tend to provide users (Gingrich, 2011). Regarding local differences in LTC policies more generally, Jensen and Lolle (2013) conclude that the ‘colour’ of the local governing party does not explain such differences.
Jensen and Lolle (2013) and Yeandle et al. (2012) have identified some other factors that may contribute to explaining differences in the generosity of local LTC policies, such as the availability of financial resources for supporting local social policies and demographic structures. However, there is an overall lack of research about factors contributing to the variation in local governments’ policies regarding LTC marketisation.
Theoretical framework
We define the marketisation of LTC policies as the adoption of measures that support market principles in publicly financed or provided LTC services (such as provider competition, the outsourcing of public care provision to non-public providers, and the inclusion of for-profit providers (Pfau-Effinger and Rostgaard, 2011)).
The degree of local governments’ operational autonomy in LTC policymaking
The degree to which local LTC policies towards marketisation vary within a country depends considerably on how and to what extent LTC policies are centralised, as well as on the degree of operational autonomy granted to local governments by the central welfare state regarding LTC marketisation (Hendrikse, 2015; Jensen and Lolle, 2013). Many social scientists have interpreted the move towards marketising LTC as indicative of a central welfare state weakened by neoliberal values. However, scholars who have studied the development of neoliberalism argue, in part, that although it emphasises the priority of market principles and a weak role for the welfare state in the provision of social services, it nonetheless relies on a strong role for the state in enforcing neoliberal reforms (Harvey, 2005; Slobodian, 2018; Streeck, 2009). To explain the differences between local LTC policies towards marketisation within a country, it is therefore important to analyse the strength of the central welfare state in the regulation of LTC marketisation, as well as to analyse how much operational autonomy it affords local governments around the regulation of LTC policies.
The role of culture and governance structures in local policies towards LTC marketisation
This paper aims to explore the roles of two main factors in explaining the differences among local LTC policies towards the marketisation of LTC: the cultural ideas of the main actors in local social policies and the governance structures of local social policies.
The role of cultural ideas
It has been shown that differences in the ideas surrounding the welfare state’s ‘welfare culture’ (Kaufmann, 1991) contribute to explaining the differences in national welfare state policies (Béland, 2005; Fleckenstein, 2011; Pfau-Effinger, 2005). This article applies this finding to local-level social policies, arguing that differences in local welfare cultures are a key factor in understanding differences in the degrees to which actors in local LTC policies promote LTC marketisation.
To do this, we apply Pfau-Effinger’s (2005: 4) concept of ‘welfare culture’, i.e. a system of cultural ideas surrounding the welfare state in a given society, and the way in which these ideas are embedded in that society. A welfare culture comprises society’s and its social-political actors’ values, ideals and belief systems regarding a ‘good’ society and (morally) ‘good’ behaviour. At the macro level, welfare culture offers an action orientation to actors on the micro and meso levels, but does not determine their actions. The welfare culture can be either ordered or logically inconsistent and is potentially fragmented, contested, contradictory and changeable. The values and ideals that dominate the welfare culture narrow the spectrum of policies that a welfare state can adopt (Pfau-Effinger, 2005).
The cultural ideas towards which policymakers are oriented may differ between municipalities. The particular cultural ideals that are relevant to our study include ideals about the societal spheres in which LTC should be provided, that is, by the family, the state or the market. We assume that differences between the welfare cultures of local LTC policymakers can make a pertinent contribution to explaining local differences in political support for LTC marketisation. The precondition is that a country’s central welfare state affords local governments some operational autonomy. We argue that local governments are more likely to support LTC marketisation in municipalities in which the relevant political actors have stronger market-liberal cultural ideas than in municipalities in which these ideas are weaker among political actors.
Our argument regarding differences between local welfare cultures is related to the differences between the historical development paths of the welfare cultures in eastern and western Germany. In western Germany, there was a long-standing welfare tradition that supported a strong role for the state and civil society organisations in the provision of social services, institutionalised as ‘corporatism’ (Archambault et al., 2014). In eastern Germany, however, under the German Democratic Republic (GDR), the state played the main role in the provision of LTC, even if non-profit providers were also involved. However, after the German unification of 1990, state responsibility for the public provision of social services was in part delegitimised in eastern Germany. Therefore, it is plausible to assume that political actors in eastern Germany were more open to the neoliberal ideas promoted by the EU and the OECD in the 1990s (Eichler and Pfau-Effinger, 2009). Accordingly, we assume that care policy in the West German welfare state was more closely connected to a state- and non-profit-centred welfare culture, whereas care policy in eastern Germany was more closely connected to a market-oriented welfare culture.
The role of local governance structures
We assume that local governance structures in local social policies are another key factor in local differences in LTC policy marketisation. Certain governance structures may better facilitate the implementation of new principles in local social policies than others. The term ‘local governance’ is useful in that it considers that besides the relevant political actors, actors in civil society or market organisations and special-purpose ad hoc bodies might participate in the policy process (Denters and Rose, 2005; Pierre and Peters, 2000; Stoker, 1998). We use the term ‘local governance structures’ to indicate locally established relationships between relevant public and non-public actors. Many authors restrict the term ‘governance’ to horizontal structures in the decision-making process. Conversely, we argue that governance structures can take different forms: they may be horizontal or based on more centralised and hierarchical decision-making processes (e.g. Mayntz, 2004: 69). Hierarchical local governance structures have been shown to favour policy innovations such as marketisation more strongly than horizontal governance structures do (Hill and Hupe, 2009; Och, 2017). Therefore, we assume that there is a greater probability of there being local social policy actors who introduce LTC policies mandating the marketisation of care in municipalities with vertical governance structures than in ones with horizontal governance structures.
Social policy governance in western Germany has been characterised as ‘horizontal corporatist negotiation’ (Archambault et al., 2014; Grohs, 2010; Och, 2017), whereas eastern German municipalities seem to have developed, because of their socialist heritage, a more top-down structure wherein most power is wielded by public actors (Grohs, 2010). Therefore, we assume that LTC policies support marketisation more strongly in the East than in the West.
The role of financial, demographic and political factors in local policies towards LTC marketisation
We take the multi-causality of policy outputs into account by considering three additional factors to control for their impact, namely the availability of resources for local social policy, the demographic structure of a city’s population, and positioning of the governing parties on the left-right spectrum.
It is plausible to assume that the availability of financial resources for local social policies plays a role in local differences in the generosity of local LTC policies. We therefore assume that local governments that have fewer economic resources tend more than others to marketise LTC.
The demographic structure—the proportion of elderly in the population—may also be a relevant factor in local differences. It is reasonable to assume that in cities with a higher share of elderly residents, municipalities are confronted with more people requiring care, and, therefore, with higher social care costs. We thus assume that those municipalities tend more to promote the marketisation of care since it may lower public LTC expenditures.
Regarding the role of the governing parties’ positioning on the left-right spectrum, we do not expect there to be a clear connection between this positioning and the extent of LTC marketisation policy. The reason for this is that there is no clear difference between left and right political parties when it comes to political support for marketisation ideas (Gingrich, 2011; Jensen and Lolle, 2013).
Methodological approach
Case selection
Our historical study includes cities from both western and eastern Germany. The reason for this is that in the time after their unification in 1990, the two regions represented two different types of welfare culture with respect to social care marketisation policies, and their governance structures also differed (Pfau-Effinger et al., 2008). The study period ranges from 1995 (when the marketisation of LTC policies was introduced in the form of SGB XI) to 2007.
The cities for the case studies were selected according to the ‘Most Similar Systems Design’ (Anckar, 2008). They are similar in major factors such as size (75,000–100,000 inhabitants each) and overall economic situation (in terms of the purchasing power of both public budgets and private households). They vary, however, in relation to public spending (with three below €2000/inhabitant and one well above that) and ageing (with two ageing rather rapidly and two more slowly). Both latter variables are used to explore the effects of public resources and demographic structure on marketisation (for details, see the Findings section). The cities are treated anonymously, with their study names based on their regions: W = western Germany, with the cities named W1 and W2, and E = eastern Germany, with the cities named E1 and E2 (see, also, Table A1 in the Appendix for the characteristics of the selected municipalities).
Indicators, measurement and data
As a first step, we considered the municipalities’ room to manoeuvre regarding LTC marketisation in the context of the German central welfare state. For this purpose, we analysed the German Constitution’s general regulation regarding the relationship between the central state and the municipalities, and SGB XI Act’s particular regulation regarding this relationship, SGB XI being the main institutional basis for the regulation of LTC in the German central state.
It is common to analyse care policies based on the actual structures of care, such as the provider mix. However, these structures are not only the outcomes of policies, but are also influenced by cultural, social, economic and demographic factors. Therefore, we analysed the degree of marketisation of LTC policies based on political instruments and institutional regulations.
For the selection of indicators, we first determined the extent to which local governments are afforded operational autonomy towards LTC marketisation in the context of the German welfare state. We identified two main fields in which the German municipalities’ local governments have some operational autonomy around LTC marketisation. On this basis, we decided which dimensions of LTC marketisation to place at the centre of the comparative local analysis (see the Findings section). These are (1) the outsourcing of public care homes and assisted-living facilities and (2) the active integration of for-profit providers into the provider mix for care homes and assisted living.
The degree of outsourcing of public LTC or assisted-living facilities to non-public and, particularly, for-profit providers indicates the degree to which local LTC policies strengthen the role of the market in the public provision of these services. It is measured by the share of public LTC homes or assisted-living facilities that the municipalities have sold to non-public providers during the study period. The actual share of non-public LTC homes or assisted-living facilities would not be an adequate measure, as it might also include some that were already non-public at the start of the study period. 1
The degree to which municipalities actively integrate for-profit providers into the local provider mix demonstrates the extent to which local care policies treat LTC as a commodity that provides enterprises with the possibility of making a profit. This, in turn, is measured by the degree to which local government activities for developing the care infrastructure have included a greater role for for-profit providers in LTC.
Methods
In order to gain an in-depth understanding of the marketisation of local LTC policies, we used a triangulation of methods (Denzin, 1989; Flick, 2018). To analyse local social policies on the marketisation of care, we analysed documents such as the minutes of municipal social committee meetings and statistical and administrative reports. We also conducted interviews with 10 experts, including at least two experts in each of the four cities (a responsible administrator and a representative of the local welfare associations), enquiring about the development of policies on LTC marketisation during this period. Additionally, we conducted expert interviews following a network approach in order to identify the most relevant actors in the field (Adam and Kriesi, 1999) and to collect information about the key types of actors, the nature of their relationships, the power relations between them, the main forms of cooperation, the degree to which social networks exist and the types of decision-making processes that have formed.
We then conducted 28 semi-structured, theme-centred interviews (on average seven interviews in each city) for the analysis of the cultural ideas. In each municipality, relevant political and administrative actors were interviewed, among them the heads of social departments and social committees representing institutional veto points (Immergut, 1990); important civil society actors from the for-profit and non-profit sectors; and senior citizens’ interest-group representatives. Except for one CEO of a for-profit provider in E2, all the interviewees were born and socialised in the same eastern or western region in which they worked. Moreover, all the interviewees had long been active in LTC policymaking in their respective cities.
These actors’ cultural ideas were explored through questions about the ‘ideal’ type of LTC and how this relates to their ideas about marketisation, care quality, the participation of the elderly, and family care. The interviews included standardised and open-ended questions as well as scales and vignettes to enable the interviewees to express and evaluate their own value orientations (Finch, 1987). All the interviews were transcribed and analysed with MAXQDA, and the value scales were analysed quantitatively.
To compare the availability of financial resources for local social policies, we analysed the amount of public expenditure and the average purchasing power per inhabitant in each municipality. To compare the demographic structure of each municipality, we explored the proportion of persons older than 60 requiring care and the respective share of people older than 60 within the population. We also assessed the role of the dominant local political parties by analysing which parties held governing majorities in the cities during the study period. 2
Findings
Local governments’ operational autonomy in LTC marketisation in the context of the German central welfare state
We first analysed the municipal governments’ operational autonomy with regard to the marketisation of LTC in the context of German national law.
The German welfare state is rather de-centralised in terms of its federal structure. The German Constitution regulates the relationship between the national welfare state, the federal states (Länder) and local governments. The national state is primarily responsible for social affairs, but it is also obliged to collaborate with the Länder (Articles 20.1 and 28.1, p. 1 of the German Federal Constitution). The municipalities do not have legislative rights, but they can steer social welfare affairs in certain directions based on their right to ‘local self-governance’ (Article 28, Paragraph 2 of the German Federal Constitution). Through legislative acts, the central state may transfer duties to the municipalities, which generates a kind of balance between the central state and the federal states. However, given such a general legal context, it is possible that the extent of welfare state centralisation differs for different policy fields (Pollitt, 2007).
Traditionally, the former West German welfare state had a rather low level of centralisation of LTC policies. LTC was mainly performed by family members. Extra-familial care was regulated primarily by the federal states and local governments, which were also responsible for providing the means for LTC to those who could not afford it through means-tested social assistance. Publicly funded care was organised mostly as residential care that was usually provided by public or non-profit providers and by and large excluded for-profit providers from the provider mix (Behning, 1999). This was different in the former GDR, where social policy was highly centralised, with rather strong central steering by the communist party and state authorities (Dallinger and Naegele, 1993).
Since the 1995/1996 introduction of the Long-Term Care Insurance Act (SGB XI) at the central state level, the German welfare state’s LTC policies have become the most centralised LTC policies in Europe (Daly et al., 2022; Och, 2015). When the new policy came into place, the social right to publicly funded LTC services of people requiring care was extended substantially. At the same time, market principles were strengthened considerably: the Long-Term Care Insurance Act introduced the principle of public procurement and provider competition. Moreover, it promoted the integration of for-profit care service providers into the provide mix and motivated municipalities to give both for-profit and non-profit providers priority over public providers. Furthermore, the principle of ‘consumer choice’ was introduced, such that people whose state of health qualified them for care could choose between different types of care providers in either at-home or residential care facilities (Rothgang, 1997).Whereas the central state regulates the LTC, it is the task of the municipalities and the federal states to organise the LTC infrastructure according to SGB XI’s conditions. There is some limited operational autonomy for local governments to promote LTC marketisation, mainly in two fields: the outsourcing of residential care in care homes and assisted-living facilities, and the integration of for-profit providers into the provider mix. By contrast, local governments have nearly no operational autonomy regarding, for example, the marketisation of home-based LTC services.
Differences in local LTC policies on care marketisation
Local policies towards long-term care marketisation in four medium-sized German cities.
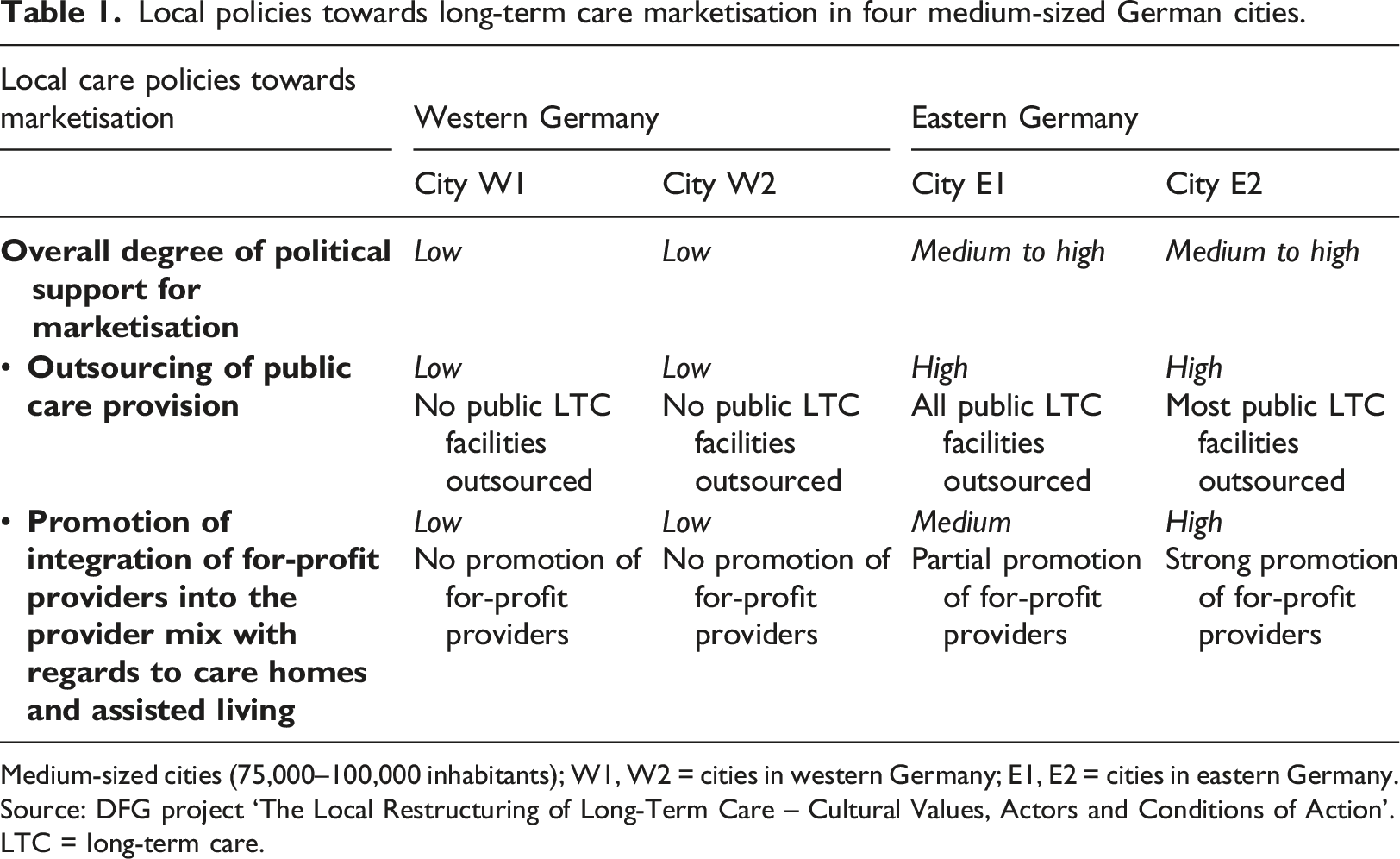
Medium-sized cities (75,000–100,000 inhabitants); W1, W2 = cities in western Germany; E1, E2 = cities in eastern Germany. Source: DFG project ‘The Local Restructuring of Long-Term Care – Cultural Values, Actors and Conditions of Action’.
LTC = long-term care.
Outsourcing of public LTC infrastructure
Regarding the first indicator, namely the outsourcing of public LTC infrastructure, E1 and E2’s local governments were rather active in selling off their public LTC homes. E1’s local government sold all four of the public care homes it had owned during the 1990s, while E2’s municipality sold two of its three care homes. The third home remained public because the workers’ council voted against the planned outsourcing via public tendering, and the city decided to specialise the home for high-quality dementia care. Neither of the eastern German cities possessed any assisted-living homes during the study period. By contrast, W1 and W2’s local governments did not sell any of their public LTC infrastructures during the study period.
Promotion of the integration of for-profit providers
The eastern German cities’ local governments actively promoted the inclusion of for-profit providers into the provider mix during the study period. E1’s local government sold two of the city’s four public care homes to for-profit providers and two others to non-profit providers. E2’s local government sold two public care homes to for-profit providers. The third remained public because the workers’ council voted against the planned outsourcing via public tendering. By contrast, W1’s local government actively prevented the establishment of residential for-profit care service providers in the city. Although there have been several requests by providers addressed to public actors to accept the establishment of new for-profit care homes, the local government has always refused them, arguing against the need for increased LTC capacity in the city. Over the study period, local political actors did not take any steps to support the integration of for-profit providers. Consequently, there were no for-profit LTC homes in W1 until 2007. In W2, there were several small and a few larger for-profit providers long before the enactment of SGB XI. After its introduction, their market share increased somewhat, leading to overcapacities. None of the interviewees in this city approved of this development.
Another of the municipalities’ options for marketising LTC facilities was to support the establishment of new facilities for assisted living by selling suitable public buildings or by providing building grounds or subsidies to for-profit providers. By consequence, in E1, 59.2% of all assisted-living facilities (574 residential units) were established by for-profit providers. In E2, this amounted to 23.4% (451 residential units). Again, in contrast, neither W1’s nor W2’s local government supported the establishment of for-profit assisted living homes.
Altogether, the findings show that the eastern German cities’ local governments supported LTC marketisation to a substantially higher degree than did the governments of the western German cities. The local governments of both eastern German cities (E1, E2) actively sold nearly all their public residential care homes, a substantial part of them to for-profit providers. In the western German cities, by contrast, it is evident that political support for marketisation in LTC policy was low, since their governments did not sell any residential homes or assisted-living facilities during the study period, nor did they promote the introduction of for-profit providers into the provider mix.
Explaining the differences in local policies on the LTC of the elderly
In this section, we evaluate the study’s theoretical assumptions that account for differences in the degree of marketisation across the municipalities.
The role of differences in the relevant political actors’ main cultural ideas
Cultural ideas of relevant policy actors on the marketisation of long-term care in four medium-sized German cities.
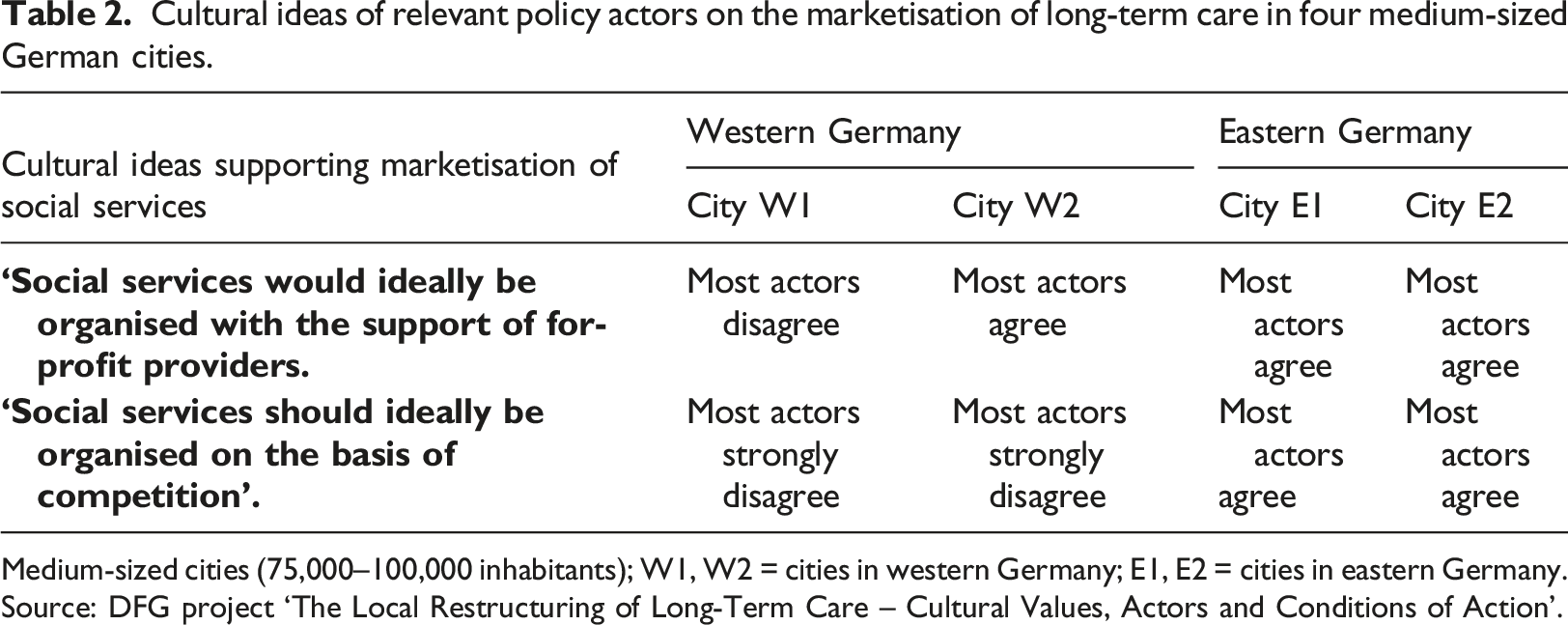
Medium-sized cities (75,000–100,000 inhabitants); W1, W2 = cities in western Germany; E1, E2 = cities in eastern Germany. Source: DFG project ‘The Local Restructuring of Long-Term Care – Cultural Values, Actors and Conditions of Action’.
In the western German cities, which had rather low levels of political support for LTC marketisation, the majority of relevant political actors highly valued the public provision of LTC and the integration of non-profit providers into the cities’ LTC provisions. Conversely, they had negative attitudes towards the inclusion of for-profit care providers. In W1, most political actors had strongly negative views about this form of marketisation. According to the main cultural ideas shared by most relevant actors, the provision of LTC would ideally be based on cooperation instead of competition, and care would ideally be provided by public and non-profit providers and not by for-profit providers, since it is a public good that should not be traded on markets. Many of these actors also believed that the market-based provision of LTC often has negative consequences regarding the quality of care and working conditions. This is shown, for example, in the following citation from an interview with a political actor in W1: I think the risk of getting lower care quality because of cost pressure is greater because I have seen here in W1 how for-profit care providers have billed services not delivered… I also have more confidence in the long-established non-profit providers which belong to the big welfare associations, such as AWO, Caritas, Diakonie and others. (Long-time leading civil servant for social affairs W1)
It is likewise reflected in the following citation from an interview with a political actor in W2: It is usually assumed that within a market, the better provider asserts himself. This is not the case… and that means that the less expensive providers prevail because they employ staff who are not so well trained, because they do not need to have a nursing home manager because of the size of their nursing home, etc. In this regard, the market is not a convincing regulative instrument. (Head of Welfare Committee W2)
The outcome was different in eastern Germany, where most of the actors’ cultural values supported the outsourcing of LTC provision and the introduction of for-profit providers into the provider mix. A common belief was that strong provider competition and the integration of for-profit providers can help improve the quality of LTC. The relevant actors also assumed that this offers older people in need of care more autonomy and freedom of choice in the provision of care, even though most of these actors did not have the necessary data or experience related to understanding the differences in care quality and older people’s autonomy in different types of LTC settings. The following argument from a political actor in E1 is a good example: In general positive. That means everything related to liberalisation or an opening, I think, is good from the point of view of markets, because it is possible to compare different providers, and there is more flexibility regarding the relationship between demand and supply in comparison with (non-profit) welfare associations as providers. (Mayor and long-time Head of Social Department E1)
Another political actor in E2 exclusively emphasised the positive aspects of LTC marketisation and argued that he did not see anything negative about it. He added: And we think that this market has opened up and has further developed quite smartly, and we of course recognise that it has established itself in the city. (Head of Department of Social Affairs E2)
These findings indicate that differences in political actors’ cultural ideas about LTC marketisation contribute to the variations in political support for LTC marketisation between East and West German cities.
The role of differences in local governance structures
The findings from our expert interviews and document analyses show that differences in the main governance structures of LTC policies also help explain the differences in local policies towards LTC marketisation among the four cities Table 3. The local governance structures in the western German cities, which have a relatively low degree of policy marketisation, tend to have more horizontal decision-making structures that involve actors other than local politicians and civil servants, such as non-profit organisations, market-based enterprises, and care user self-help groups. The governance structures in the eastern German cities, which have a rather high degree of LTC policy marketisation, are, by contrast, more centralised and hierarchical, with public authorities occupying the central position.
In the two western German cities, we found two different types of horizontal governance structure. In W1, the governance structure is distinctly divided into a core group of actors and a peripheral group of actors. There is a traditionally strong and relatively fair cooperation (‘corporatism’ – see Archambault et al., 2014; Grohs, 2010) between the municipality’s public actors and main welfare association representatives. This core group manages various steering committees that make the main decisions in local LTC policy matters by consensus. Other actors, such as the representatives of for-profit organisations or other civil society organisations, play a small role by comparison.
Governance structures in local long-term care policies in four medium-sized German cities.
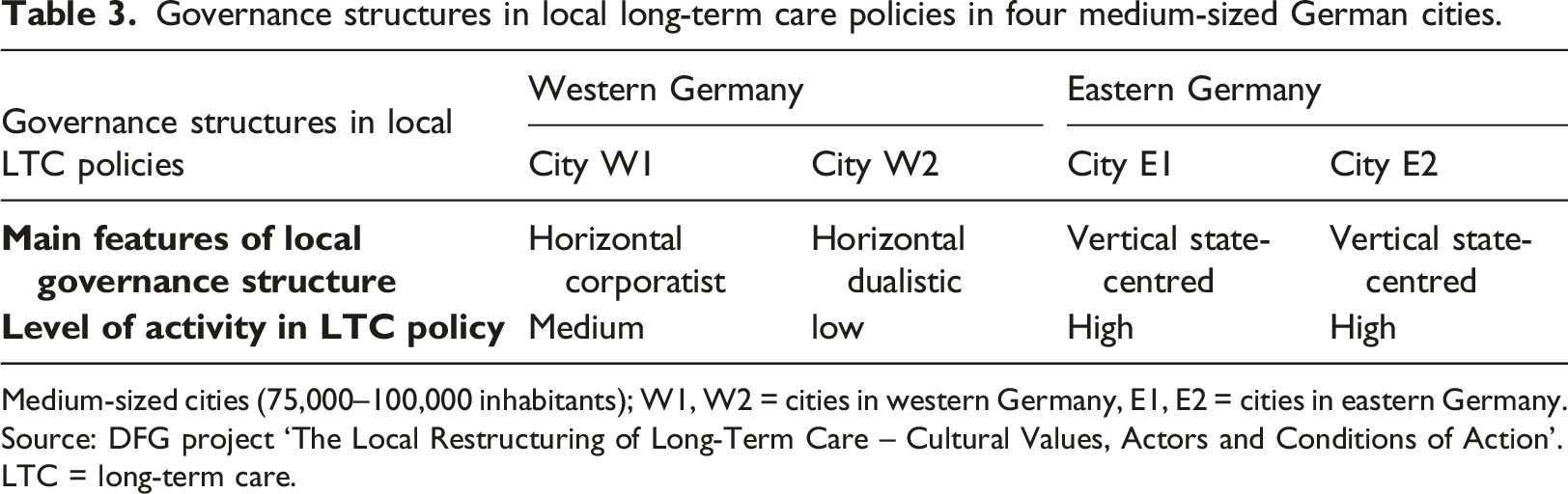
Medium-sized cities (75,000–100,000 inhabitants); W1, W2 = cities in western Germany, E1, E2 = cities in eastern Germany. Source: DFG project ‘The Local Restructuring of Long-Term Care – Cultural Values, Actors and Conditions of Action’.
LTC = long-term care.
In both eastern German cities, with their relatively high degree of policy marketisation, the governance structures have a more hierarchical, state-centred structure in which political and administrative actors are most powerful. This is partially due to the region’s socialist history and events of the unification process. In socialist times, welfare associations were not supported by the state, which steered social policy centrally (Dallinger and Naegele, 1993). The top-down reunification process (Lehmbruch, 1993) also placed local public actors in a central position, as they had to make decisions on allocating funds for the restructuring of the local care infrastructure. The welfare associations were rather weak, since they did not have strong roots in civil society and depended heavily on local administrations and public resources (Angerhausen, 1998). To illustrate this point: In E2, the city organises regular consultations with welfare providers, which include separate meetings for each provider (at least once a year) as well as collective meetings. In E1, almost all initiatives to further develop the local LTC system have their roots in the local administration. Since the financial resources for those measures are mostly provided by local, federal and, in a few cases, European funds acquired by the cities, the local authorities have some advantage in negotiations.
Thus, the findings regarding local governance structures in LTC policies support our main assumption, which is that the eastern German municipalities had more vertical governance structures, compared to the western German municipalities’ more horizontal ones. It seems that the vertical governance structures in the East offered more favourable conditions for policy innovation based on the strengthening of market principles, by contrast with the western German municipalities.
The role of differences in the municipalities’ financial resources
We also analysed whether local policies towards LTC marketisation are connected to the municipalities’ access to financial resources. Our findings indicate that the degree of marketisation does not vary systematically with the amount of resources available to the municipality. Two cities show higher purchasing power per inhabitant than the others, one in the eastern and one in the western part of the country (W1: €30.807: W2: €29.039; E1: €30.454; E2: €28.187 [Federal Statistic Office of Germany, 2007, all figures for 2003]; see, also, Table A1 in the appendix). One eastern German municipality (E1) also has significantly higher expenditures per inhabitant (€2793.4 per year) than the two western German cities (W1: €1627.89; W2: €1905.3), while E2 has the lowest expenditures (€1725.5 [Federal Statistic Office of Germany, 2007]). These results indicate that there is no clear connection between the level of available financial resources and the degree to which the marketisation policy is applied.
The role of differences in the demographic structure of the population
The share of residents aged over 60 and requiring care (2003 data 3 ) is greater in both western German municipalities (2.8% each) than in either eastern German city (E1: 2.2%; E2: 2.1%) (Bertelsmann Stiftung, 2006; Federal Statistical Office, 2006). The comparative strength of local policies promoting LTC marketisation in eastern Germany is thus not traceable to any particular age-related care problem.
Other factors: the positioning of the governing parties on the left-right spectrum
As expected, the findings do not show any clear connection between the extent of LTC marketisation and the positioning of the governing political parties on the left-right spectrum. The municipal parliaments of both western German cities were dominated by the social-democratic SPD party from the second half of the 1990s to 2000. However, since the early 2000s, coalitions of the conservative CDU together with changing partners (the liberal FDP, the Greens and local citizens’ voter associations [Wählergemeinschaften]) have dominated in both cities. Nevertheless, despite these cities’ changing positions on the political spectrum, a policy of avoiding both the outsourcing of residential homes for LTC and the inclusion of for-profit providers has persisted in both of them. In the municipal parliaments of the eastern German cities, there was no clearly dominant political party or political orientation; each of the three biggest parties (SPD, CDU and Post-communists) was, by turn, the strongest party in the elections, but none was able to win a majority during the study period.
Conclusion
Our study aimed to explore the roles of culture and governance structures in explaining the differences between local policies towards the marketisation of LTC by using Germany’s LTC policies as an example. So far, there have been very few studies analysing the factors that may contribute to differences in this regard. This paper is innovative in that it explores the role of local welfare cultures and local governance structures in variations between local policies towards LTC marketisation.
We argue that comparative analyses of political support for LTC marketisation should take a multilevel approach that, as a first step, explores how and to what extent central state-level policies afford operational autonomy for local policies towards LTC marketisation. Our study shows that the German central state’s LTC policies have a rather high level of centralisation; they only afford local governments operational autonomy with regards to the outsourcing of care homes and assisted-living facilities, as well as the integration of for-profit providers into the provision of care in care homes and assisted-living facilities. We used these two fields of LTC in our historical study, which comparatively analysed LTC policies in four medium-sized German cities between 1995 and 2007 in order to explain the differences in the degrees to which LTC marketisation was brought about by local governments.
The findings show substantial differences among our studied municipalities regarding political support for LTC marketisation, with a higher degree of LTC marketisation in both eastern German cities. The findings support the study’s main assumption that differences in political actors’ dominant cultural ideas and in local LTC policies’ governance structures account significantly for the differences in local policies on LTC marketisation. The roles played by the availability of financial resources to local social policies, the demographic structures of the population, and the positioning of the governing political parties on the left/right spectrum were also evaluated, but these apparently did not contribute significantly to the differences in question.
The empirical study is based on an exploratory analysis of four comparative case studies. Future research will have to evaluate these theoretical assumptions in a cross-national perspective for countries with different types of welfare states, and with different degreed of centralisation of LTC policies. Furthermore, future studies will have to include a more comprehensive number of cities and a broader range of policies.
Footnotes
Acknowledgements
We would like to thank the German Research Foundation for their generous support and the anonymous EPC reviewers for their valuable comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was funded by the German Research Foundation (DFG) under the grant agreement number PF 578112.
Notes
Appendix
Selected characteristics of the municipalities. Sources: Federal Statistical Offices, Bertelsmann Stiftung, 2006, author’s own compilation. Provider mix in residential care in terms of market share (available beds) in the four cities (2007/2010). Source: author’s own compilation.
Municipal characteristics
City W1
City W2
City E1
City E2
Federal state
Hessen
Lower Saxonia
Thüringia
Saxony-Anhalt
Number of inhabitants (2003)
74,100
84,586
102,634
78,380
GDP in €/inhabitant (2003)
rnd 27,000
rnd 27,000
rnd 25,000
rnd 21,000
Structure of public revenues and municipal spending (2003 in Mio. Euro)
Public revenue per inhabitant
Public spending per inhabitant balance of public revenues and spending per inhabitant1,585
1,628
−431,855
1,905
−502,179
2,793
−6142,250
1,725
525
Purchasing power in €/household (2003)
30,807.4
29,039.2
30,454.1
28,167.3
Recipients of social assistance in % (2003)
7.2
6.7
2.5
3.8
Median age in 2003
37.2
42.9
38.6
46

Provider mix in residential care
For-profit
Non-profit
Public
City W 1 (2007)
0
100
0
City W 2 (2010)
19.2
61.8
23.3
City E 1 (2010)
29.3
70.7
0
City E 2 (2007)
68.1
12.9
19.0