
Abstract
Abstract
Better solid waste management (SWM) is a critical need for many industrialising cities in the world, with institutional and financial issues critical to improving management. Great progress was made from 1970–2000 in estimating the costs for healthcare in industrialising cities, while to date very little progress has been made in improving cost function analyses on SWM. The similarities between the two sectors are strong, and the history of healthcare cost function analysis used to elucidate a pathway to improved cost function analyses for industrialising cities. The following cost function issues are explored: economy of scale, marginal cost analysis, cost function analysis, economies of scope, relationship between size of service provider and costs, accounting for outpatient and informal sector activities, input prices and ownership and control. The recommendation is that future work on SWM cost analysis should prioritise (1) analysis of which variables need to be included or can be excluded in cost function analysis, (2) use of cost functions to analyse questions related to service provision and (3) collection of more and more appropriate data to allow development of cost functions analysis methods specifically suited to SWM in industrialising cities.
Keywords
Introduction
Cost Analysis for Solid Waste Management (SWM) in Industrialising Cities
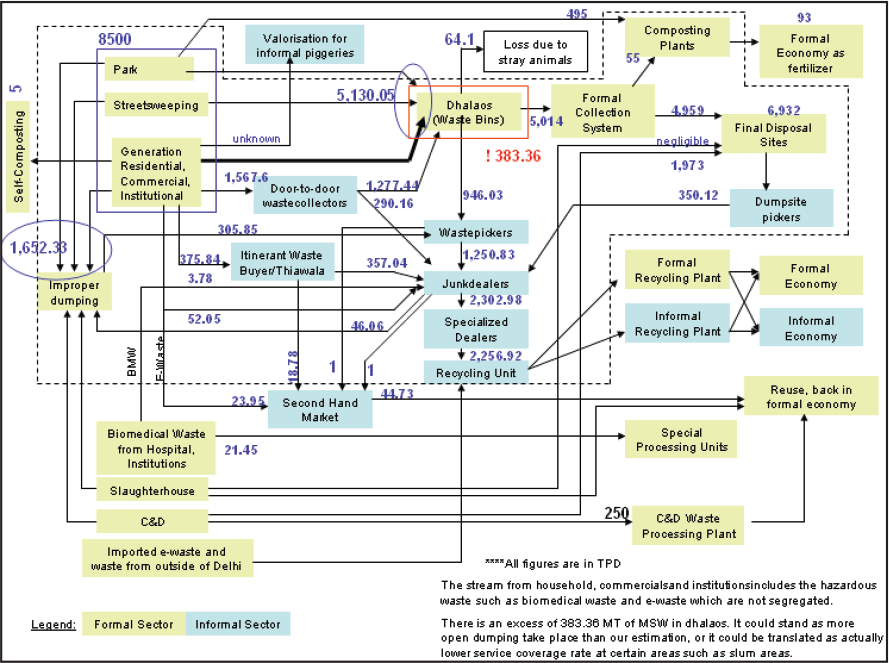
Municipal SWM refers to the public service of handling municipal solid waste via collection and subsequent transfer, treatment, disposal and recycling. In industrialising cities, the organisational structure of this service is complex, and generated wastes are often managed in parallel by multiple organisations: municipalities, private contractors, non-governmental organisations, community-based organisations, resident welfare organisations and the informal sector. An example for Delhi, India, depicting these complex inter-relationships between waste management activities and stakeholders is shown in Figure 1.
The underlying complexities resulting from having multiple organisations involved in managing waste makes cost estimation and analysis extremely challenging in industrialising cities. Parthan, Milke, Wilson, and Cocks (2012a, 2012b) suggest that an integrated approach that combines the potential of the past cost estimation approaches in developing country literature (i.e., the unit cost method, benchmarking techniques and the cost modelling approach using cost functions) could be a way towards improving cost planning. The first step for improved cost estimation is to map out the flow of material and costs, through different stages and including all providers, in the existing waste management system using a process flow diagram. Cost functions based on the unit cost method (e.g., Rupees/tonne) for each stage in the system could then be developed. These would most likely be different for different providers of the service; for example, with informal recycling, there is the income to account for. These costs or rates could be used as future benchmarks and could also be useful to compare with benchmarks from other cities. A set of activity-based cost functions could be aggregated into an overall system model of costs. Such a model when calibrated for geographic areas where there are good data could be used for municipalities or areas with limited data. In addition, development of cost models may assist in understanding data deficiencies, which is a common issue affecting cost planning in developing countries. In summary, the challenges with cost estimation for SWM in industrialising cities have been great, the demand for progress high, and the rate of progress has been slow.
Most industrialising cities are unable to sustain an acceptable level of solid waste service due to poor cost recovery from some combination of users, government or non-governmental organisations (Diaz, Savage, Eggerth & Golueke, 1996). This can be partially blamed on inadequate planning. Consider a municipality that is planning on expanding its solid waste collection services to include informal settlements adjoining the present municipal limits. The municipality intends to apply to a NGO for funds to offset the initial costs of expanding the service. Cost functions would be valuable to estimate the cost of the expansion (Parthan et al., 2012a). The World Bank has highlighted that institutional and financial issues are the most important ones limiting improvements in SWM in industrialising economies (Hanrahan, Srivastava & Ramakrishna, 2006; Hoornweg, Lam & Chaudhry, 2005).
Past Cost Function Research in Solid Waste and Health Care
The desire to improve health in industrialising cities led to similar concerns regarding institutional and financial issues, which in turn has resulted in special attention to be directed in the past four decades towards better understanding the cost structure, cost drivers and cost behaviour of healthcare management (Eldenburg & Krishnan, 2006). The issue of costs became an important topic of research for developed nations like the United States as expenditures on the service was growing rapidly (Lave & Lave, 1984), and soon developing nations also focussed on costs in healthcare research, as the issues facing policymakers were similar (Wagstaff & Barnum, 1992).
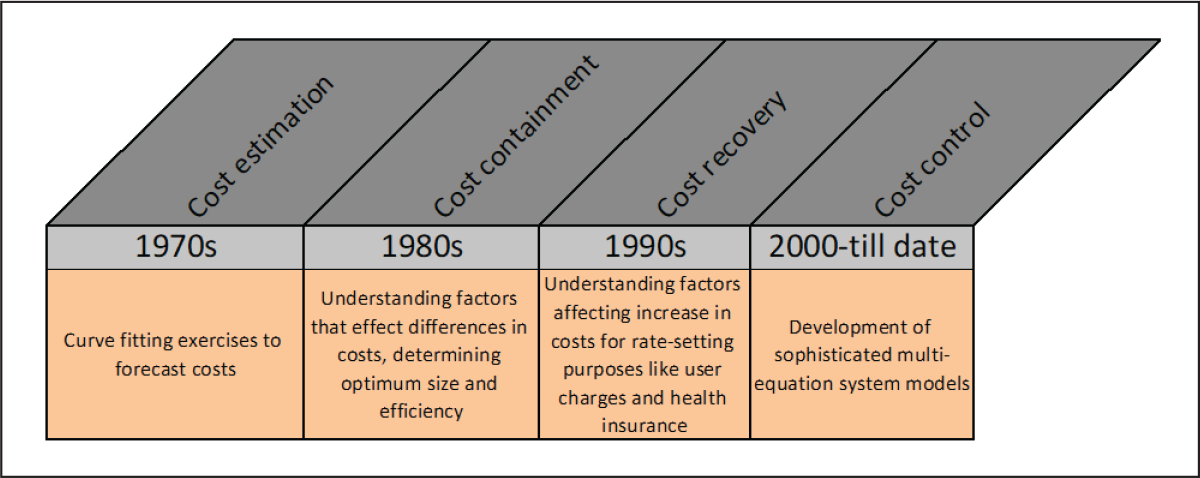
Since the late sixties, there has been a torrent of research publications on the topic of estimation and interpretation of healthcare or hospital cost functions. For example, Ellis (1991) estimated that in just the five years from 1986–91, at least 3,500 books and articles were published on the subject. Cost function research in the healthcare sector progressed gradually over the past 40 years (see Figure 2). From crude beginnings in the 1970s, which were cost-analytic exercises to forecast costs, more elaborate cost estimation techniques and analyses started to emerge (Lave & Lave, 1984). The 1980s research progressed to cost containment measures, such as understanding the factors contributing to differences in costs of healthcare. In the 1990s, researchers not only focussed upon factors affecting costs, but also started looking into factors affecting increase in costs over time, as cost recovery measures through health insurance schemes became popular. Another direction of 1980s research was to estimate the costs of various diseases, which developed into burden-of-disease studies (Murray & Lopez, 1996). By the late 1990s, the results of this research were informing financing decisions of the World Bank. More recent research seems to be focussing upon using more sophisticated econometric techniques that are useful in developing a complete model of the healthcare system while also attempting to control cost increases.
Developing cost functions for planning is not new to solid waste researchers. Economists such as Bel (Bel & Fageda, 2010; Bel, Fageda & Warner, 2010; Bel & Mur, 2009; Bel & Warner, 2008), Kinnaman (Kinnaman & Fullerton, 2001; Kinnaman, 2005), Stevens (Edwards & Stevens, 1978; Stevens, 1978), Clark (Clark, Grupenhoff, Garland & Klee, 1971; Clark & Lee Jr, 1976; Clark & Stevie, 1981) and Hirsh (Hirsch, 1965, 1995) have made significant contributions to this particular field of research in developed countries. Excepting the authors’ own works (Parthan et al., 2012b), there is nothing comparable for waste management planning in industrialising cities, where problems of waste are more critical, expenditures are increasing significantly, but finances available for improving the service are constrained. The cost function success story from healthcare can be seen as a motivation for waste researchers to further contribute to the limited existing knowledge.
One objective here is to provide lessons on cost function analysis from the healthcare management sector; rather than comparing solid waste cost estimation methods with those used for sewer or drinking water costs (which might at first seem logical), it might be better to compare them to healthcare costs. A second objective is to propose future research directions for solid waste researchers on this topic. Next, readers will be directed to a specific set of research questions that early healthcare researchers had tried to answer. Much of that early research was in relation to the cost of hospitals in industrialising cities, rather than with the broader view towards healthcare provision today.
There is a reason for not basing this analysis on more recent developed economy cost function research applied to healthcare. The amount and quality of data that are available presently to estimate SWM cost functions best compare to what healthcare researchers used to work with at early stages of their research. As research progressed in healthcare, the quality and accessibility of cost data also improved. Although it is hoped that the same will happen for SWM, the type of analyses that can be done with the current level of data from industrialising cities is analysed in the ‘Healthcare Management Research Results and Analogous SWM Research Directions’ section. Finally, certain recommendations are suggested for progressive advancement of SWM cost function analyses for industrialising cities.
Comparison of Healthcare/Hospital Management and SWM
Similarities Between Healthcare Management and SWM in Industrialising Cities

Organisational Structure
Both healthcare and solid waste services in industrialising cities can be offered by a public, private or a community organisation. The difference in the type of organisation complicates the use of cost data for developing cost functions. For example, only public organisation data might be available, and biased analysis could be obtained. For industrialising cities, the challenges are greater because of the presence of non-governmental and charitable organisations (NGOs), and of informal sector workers, for example, as waste pickers at dumps, or as unregistered medical practitioners and drug dispensers in poor communities.
Difficulty in Defining and Measuring Output
Defining a measurable output is crucial for the development of reliable cost analysis methods. Unlike the cases of industrial or agricultural outputs, it is difficult to define and measure the output for both healthcare and SWM. Provision of healthcare aims at improving the patient’s health —something that is ambiguous and difficult to measure (Breyer, 1987). Provision of SWM services aims at improving public health, environmental protection and resource management (Scheinberg et al., 2010), each of which is difficult to quantify. As Gottinger (1991) points out, considering solid waste as a homogeneous output and considering tonnes managed as the ‘output’ for SWM, is not as clearly related to a policy aim when compared to a company that might have its output as the number of items manufactured, which is clearly related to the company’s income.
Although there is no simple ‘product’ or output definition of healthcare services, healthcare cost analysis researchers have used a number of different approaches. For example, with hospitals in industrialising cities, the analysis might consider the total number of patients treated or the total number of bed days. In terms of costs, the outputs could be cost per patient, per patient discharge, per patient day or per hospital bed. The most common proxy outputs in the case of SWM cost analysis are total tonnes collected or total population served, while cost outputs are mostly in terms of costs per tonne and costs per person.
Cost Classification
The third example in Table 1 is that, in both types of services, there are challenges with classifying costs. In multi-service systems (see ‘Multi-Service Systems’ section) such as healthcare and SWM, it is practically very difficult to arrive at a separate cost measurement for the different services provided; the classification of fixed and variable costs for each service will not capture all cost overheads. For healthcare in industrialising cities, one facility can be used for a wide variety of services (acute care, primary care, and outpatient services), while a community resource recovery facility might be used for waste re-use, household hazardous waste drop-off and a transfer station for general municipal solid waste.
Capital costs connote fixed costs for land, buildings and equipment and sometimes include costs that change with output, but cannot be attached to a single output as they can be spread over different services (e.g., privatisation and administration costs). Operating costs include those costs directly attributable to the service, connoting the variable cost, and commonly include components such as salaries and wages, regular maintenance of equipment, consumables and so on.
Industrialising City Challenges
A number of challenges in cost analysis are greater in industrialising economies than in developed ones, and both healthcare and solid waste services (along with a number of other services) are affected in distinct ways in industrialising cities. Severe shortages of resources exist in terms of capital in industrialising cities. The shortage might be in medical equipment in the case of healthcare and in waste collection and transport vehicles for SWM. Cost analysts in both fields need tools to analyse the relative value of capital expenditure options.
Poor accessibility (due to bad roading/transport infrastructure) of low-income-population regions or geographically remote locations in industrialising countries is another factor for such populations having little or no access to medical or SWM services, when compared to similar populations from developed nations. Cost estimation methods that are applicable to areas with poor accessibility can be particularly challenging.
Another common factor that is more severe in the case of industrialising cities is poorly motivated professionals, especially in the public sector. Salaries are generally below expectations, there are no regular evaluations to assess the performance of workers, and quality check inspections are challenged by issues such as corruption at supervisory staff levels. Information collection and management (accounting practices) are varied and datasets with sufficiently detailed information on costs in industrialising countries have been difficult to come by. Not only health care systems are similar to SWM systems in this respect; practically all services (e.g., transport, electricity) in industrialising cities suffer from similar problems.
User Fees
Many costs in both services are covered by funds collected from taxes (either general or local), while some costs are fully paid by users, and other costs are partly met by users with government subsidies. This situation complicates analysis of existing cost data and also complicates analysis of the fees that should be charged in various settings. If City A has a higher reliance on user fees than City B, and total (government plus user) costs are lower in City A, is it because the reliance on fees lead to more efficient organisations, or is it because of the use of less effective (as well as less costly) means to achieve goals? For the health sector, unlike solid waste, the issue of insurance and its relation to user fees further complicates analysis. Controlling for fees in cost analyses has been an ongoing challenge in both the health and solid waste sectors.
The issue of user fees and its effect on cost analysis are, if anything, more complex in industrialising cities. In poorer areas, there is greater reliance on not-for-profit organisations such as community-based or resident-welfare organisations that have little or no financial support from the municipality. Populations in those areas need to pay additional user fees for the same services that might be covered by government-funded services in nearby areas.
Multi-input Systems
Prediction of costs is simpler when the inputs, or types of problems, to be managed are fewer or more similar. Estimation of costs for wastewater management is simplified because of the similar nature of wastewater between cities. Healthcare cost analysis is more complicated because of the many conditions and diseases that need to be managed. Similarly, solid waste cost analysis is complicated because of the great differences in management of food waste, plastic waste, construction and demolition waste and so on. The more economically similar that people are within a industrialising economy, the easier it can be to conduct cost analyses because of the similar rates of disease and the similar rates of generation of specific solid waste components.
In healthcare, as cities progress due to industrialisation, there is a gradual shift from treating infectious diseases to more life-style-related diseases. This may be attributed to a decline in the incidence of infectious disease, people living longer and the increasing importance of chronic diseases. Similarly with SWM, as cities become more industrialised and average income levels rise, the characteristics of waste produced shifts from having more organics or putrescibles to an increase in recyclable content such as plastics and packaged materials (similar to the waste characteristics of industrialised economies). Many industrialising cities are midway through this industrialisation phase and in a situation where diverse diseases and diverse waste types are simultaneously prevalent.
Multi-Service Systems
In the final example, both healthcare and SWM are multi-product public services. Healthcare management can involve a number of different types of curative services, similar to the different types of solid waste services from collection through disposal. In an industrialising city, the diverse health care activities managed in a hospital can be handled by different types of hospitals (e.g., public, private or community) can have different sub-services (e.g., emergency departments for outpatients or operating theatres for inpatients) and have a variety of medical functions (e.g., pharmacies and diagnostic facilities). SWM is also a multi-product system. It consists of two broad activities of collection and treatment/disposal of waste. Especially in industrialising cities, these activities can be shared between the municipal and non-municipal organisations, can have different sub-services (such as door-to-door collection and collection from community bins or disposals in engineered landfills and open dump sites) and have intermediate functions (such as treatment units or transfer stations), similar to the multi-product characteristics of healthcare management.
Healthcare Management Research Results and Analogous SWM Research Directions
The objective of this section is not to provide a review of the cost function analyses from healthcare literature. Instead, we try to understand the basic intent of these historically relevant investigations and, because of the similarities in characteristics of healthcare and SWM, develop research questions for similar cost function investigations for solid waste researchers. The analysis here highlights issues specific to industrialising economies with a focus on urban areas.
Economy of Scale
An economy of scale is said to exist when average cost decreases as output increases. Early healthcare researchers were interested in determining whether economies of scale existed in hospitals. For example, Anderson (1980) found economies of scale in a sample of 75 government hospitals from Kenya. The author concluded that because cost savings were moderate (that a 1 per cent change in bed capacity can yield a 0.24–0.25 per cent change in unit costs), it was better to expand existing facilities instead of building a new small-scale hospital.
After further research, healthcare cost analyses have concluded that it is difficult to analyse for economies of scale because larger facilities will have greater case complexity and quality of care, and also concluded that after controlling for these factors, economies of scale are limited (Folland, Goodman, & Stano, 2007). There has been an increase in the size of health facilities in time, but this appears to be more a function of service coverage or market power than of economies of scale (Folland et al., 2007).
The indirect value of economy-of-scale approaches were appreciated in healthcare cost analysis research over time. Wagstaff and Barnum (1992) considered not whether outputs should be expanded to fully utilise the fixed inputs, which is a question of economies of scale, but whether optimal amounts of the fixed inputs are employed given the output levels of hospitals. In other words, the question is whether hospitals are allocatively efficient in their use of the capital. Determining economies of scale provides the health planner with other valuable information, such as applicable rates of reimbursement. These can be based, in part, on the relationship between the scale of operation and the associated unit cost of production.
Implications for SWM in Industrialising Cities
Constructing a cost curve is a simple way to examine the economies of scale effect for SWM (USEPA, 1997). Economy-of-scale factors in SWM for industrialised economies have been fit to curves using the logarithm of the cost in the past (Wilson, 1981; Tsilemou & Panagiotakopoulos, 2006). The great differences between industrialised and industrialising economies make these methods of little direct use.
A better understanding of economy-of-scale factors applicable to industrialising cities would assist with planning of expansion of service. With rapid population growth in urban areas in and around industrialising cities, service providers, mostly municipalities, need to expand current SWM operations to include more areas. Using existing data from that particular city, or using other data after adjustments, the question of whether or not it is cost-effective to do so can be answered by studying the economy of scale for the service.
Capital-intensive services exhibit significant economies of scale due to higher fixed costs (Bel, 2012). With this in mind, it would be valuable to separately evaluate the levels at which economies of scale are exhausted for solid waste in industrialising countries, activity-wise, as some activities are more labour intensive and some others capital intensive. For example, for waste collection in industrialising countries, economies of scale might be exhausted soon due to the more labour-intensive nature of the activity, than, say, secondary collection and treatment activities that involves bigger capital investments such as transfer stations and composting plants.
Similar to the findings of Wagstaff and Barnum (1992) in healthcare economics, for SWM in industrialising cities, answering the economies of scale question could help with expansion planning programmes for a start, and then lead to assistance with other planning questions. However, the more recent experience of cost function research in healthcare has highlighted that economy of scale is not a strongly useful concept in describing cost variations, and SWM researchers should proceed with full awareness of why the focus in healthcare has moved away from examining economies of scale.
Marginal Costs
The marginal cost is the change in total variable costs incurred when producing each additional unit of output. Marginal cost is a first derivative, MC = ∂TC/ ∂Q, where TC = total cost, and Q = quantity of output. In the case of non-tradable goods or services, depending on how resource-need varies during a particular time period being considered, marginal costs include all costs that vary with the quantity of output; all other costs are considered as fixed costs. As an example, the total cost of a medical general practitioner’s (GP) services for treating 10 patients is $500 or $50 per patient. In the flu-season, 11 patients can be treated for $528. In this case, the marginal cost of the eleventh patient is $28, while the average cost for 11 patients has changed from $50 to $48. The marginal cost could be lower than the average cost because the additional patient does not change certain fixed costs such as receptionist’s salary, daily cleaning of premises and power supply.
Healthcare researchers have clearly distinguished between estimating marginal costs (the cost of producing an additional unit of output) and average costs (the total cost of all units divided by the total units produced). Economists have shown that marginal costs will be lower than average costs so long as the capacity created by the fixed cost is not fully utilised (Kurup, 2010). If economies of scale exist up to a certain level in the production of hospital services, the average and marginal costs will fall until this level leads to diseconomies. For example, if the same doctor’s office were to treat 20 patients, the total cost might rise to $1,200 because of the cost of overtime for staff, and for hiring extra space. Estimating the link between scale of production and average and marginal costs helps in planning (Kurup, 2010).
Healthcare cost analysts more recently have made use of both marginal and average costs. Marginal costs are used increasingly to assign user fees, or the terms of cost recovery. Because estimation of marginal costs can vary greatly between analyses or over time, many payment incentive schemes (such as diagnostic-related groups [ref. from Ian?]) are based on average costs that are updated with time.
Implications for SWM in Industrialising Cities
If an industrialising city’s average SWM cost is a certain x per tonne, and if the city experiences a significant increase in the quantity of a separate fraction of the waste (e.g., food waste) due to a programme change (e.g., from separate collection to a part of the city), it is unlikely that the costs would increase by x for each extra (or marginal) tonne managed. If the extra tonnage to be handled can be managed by existing capital equipment, certain fixed costs that are not affected by the amount of waste collected will not contribute to marginal costs. Examples are overhead and central administration costs, salaries of full-time employees, time taken for trucks to reach collection areas. Examples of costs that might contribute to marginal costs could be employment of part-time collection workers, additional maintenance costs due to increased wear on vehicles from the extra tonnage, extra tipping fees, additional cost of fuel due to increased coverage and so on.
The relevant question to ask would be, which costs will change and which costs won’t when making changes to the SWM system? If the service is expanding to the extent that an additional five trucks need to be purchased to transport waste, the marginal cost should include the purchase of those trucks. External factors as diverse as training by collection staff and supervisors, poor cooperation from waste generators, truck sizes and configuration can significantly affect marginal cost estimation.
Cost Function Analysis
Because so many different variables can affect the cost, identifying a marginal cost relies on controlling for many other variables that can affect cost. The development of a series of marginal costs can lead to development of cost functions. For healthcare, cost functions are found by multiple regression techniques on large datasets. Over time, healthcare cost analysts have used larger cost functions. These cost functions identify marginal costs associated with individual characteristics that can help in better assessing user fees, or the individual marginal costs can help in identifying causes for higher or increasing costs. A challenge with the effective use of cost functions in the healthcare sector has been the rapidly changing nature of both the services and the people served. New services or more popular old services can arise quickly leading to outdated cost functions. Changes in the population or demographics or income level of a community can also make cost functions become quickly outdated. The development of cost functions is a highly evolved process in many organisations, including those involved in SWM. The challenge today for improving practice is the limited exchange of information and results between organisations. For private organisations, publication of cost functions for their activities would allow competitors to exploit opportunities to take business away from more expensive competitors. Publication of cost functions might also lead to private companies increasing their costs because they believe they can do so without losing market share to a competitor. Even within government operated services, the publication of cost functions is rare. This could be because of the potential for others to take the findings out of context and compare one city’s costs relative to others. Although the lack of published cost functions is perhaps understandable, the lack of documents indicating best practice in analysis of data to develop cost functions indicates that, industry-wide, there is a potential for more knowledge development and dissemination to improve performance.
Implications for SWM in Industrialising Cities
Cost functions appear to be less developed in industrialising cities than in industrialised economies, while at the same time, the larger fraction of external funding of services indicates the potential that funding agencies would be very eager to develop and use them in funding decisions.
Cost functions are used often in healthcare cost estimation applications, and predicting accurate waste quantities should be slightly easier than predicting patient flow in healthcare centres. Cost functions for industrialising cities would need updating, but the rate of change for SWM might be expected to be less than for healthcare systems, because of the slower rate of technology change over time with SWM, and the less strong (though still significant) changes expected in demand for SWM services with change in demography and income.
Economies of Scope
Economies of scope are said to exist if the joint output of a single organisation is greater than the output that could be achieved by several separate organisations each delivering one service but together employing the same amount of input. An implication of economies of scope is that production costs can be reduced by delivering services jointly, rather than specialising.
Healthcare economists have frequently explored the questions: should hospitals specialise or provide a broad range of services? Is it more or less costly to provide inpatient and outpatient services in a single facility or by two specialised facilities?
Healthcare studies indicate that the functional form of the cost function is important when exploring economies of scope. The study by Wagstaff and Barnum (1992) specifically focussed on exploring scope economies for four industrialising countries, namely Kenya, Peru, Ethiopia and Nigeria. They state that specifying an average cost function that considers the overall total costs as the sum of the product-specific total costs (i.e., sum of inpatient and outpatient costs) is not effective in measuring economies of scope. Specifying a multi-product cost function, that is, a cost function that jointly considers inpatient and outpatient services has proven to be more effective by healthcare researchers in general as it measures the source of economies of scope which is a characteristic known as ‘cost complementarities’ (meaning that the marginal cost of producing one output would decrease as the quantity of the other good is increased). To allow for cost complementarities, the cost function would need to include interaction terms between various outputs.
Implications for SWM in Industrialising Cities
Similar to healthcare, multiple service providers are involved in SWM in industrialising cities. Some private service providers are involved in just the collection of waste, whereas some others provide the whole service from collection through disposal. The solid waste researcher might be interested in answering the following questions related to ‘vertical’ integration of the service to explore the scope issue for industrialising cities:Do economies of scope exist between the various services used in SWM?
Does average cost decrease as the number of activities (from collection through disposal) conducted by the same service provider increases? Will costs per tonne be greater if each service provider handles a separate SWM activity?
Municipalities can be thought of as multi-service organisations because they generally handle two or more services (other than SWM) simultaneously. Grosskopf and Yaisawarng (1990) believe that the multi-product nature of municipalities is characterised by existence of economies of scope, that is, they achieve cost savings when joint services are provided. Questions related to ‘horizontal’ integration also arise: is there a benefit from merging two private collection companies into one or does this reduce competition too much?
A good analysis of the economies of scope question can be found in the study by Callan and Thomas (2001). They studied whether economies of scope existed when both disposal and recycling services are jointly provided in a sample of 110 municipalities in Massachusetts. Similar to the method used by healthcare researchers, the method used by Callan and Thomas involved including an interaction variable which was the product of the outputs (in their work it was the quantities of waste disposed and recycled), among other explanatory variables. They included this interaction variable in both the disposal and recycling cost functions (estimated separately), in order to study the cost effect of the alternate service. A negative coefficient for the interaction variable was an indication that economies of scope were present in that study. The method might be useful for similar studies for industrialising cities, in particular where less work has been done to evaluate options for horizontal or vertical integration.
Relationship Between Size of Service Provider and Costs
When studying the relationship between hospital costs and size, it became necessary to control for the variety of illnesses (commonly termed ‘case-mix’ variation), because larger hospitals also treated more complex illnesses. The appropriate method to control for the sheer number of diseases and conditions when estimating a healthcare management cost function is still an unsettled issue in cost function analyses literature. Early literature relied on surrogate measures by measuring differences either by the type of services offered by the hospitals or by the types of facilities available within the hospital (e.g.. blood banks, pharmacies, canteen). As research progressed, more sophisticated direct measures for case-mix were developed by forming groupings based on diagnosis, type of surgery, patient age and so on, that resulted in advanced cost function estimations (Lave & Lave, 1984). More recently, the research on case-mix cost estimation has developed to the point where the cost estimates are adopted internationally as part of an effort to provide incentives for allocative efficiency (Liu, 2003).
Implications for SWM in Industrialising Cities
The issue of service provider size is one that is quite complex to study for SWM. The variation in quantities and characteristics of wastes handled (examples include medical waste, hazardous waste, industrial waste, residential, commercial waste and institutional waste) and different activities performed by different service providers results in a very complex system.
SWM service providers come in various sizes and many also have multiple responsibilities alongside waste management. Large municipalities might service over a million residents in a city while also providing water supply and sewerage, or the SWM service provider might be as small as a resident welfare organisation exclusively collecting waste from 100 households. It is challenging to conduct a cost analysis to indicate the most economic combination of service providers.
Waste researchers might want to study the relationship between the size and type of service provider and costs. Such a study might be useful for decision makers in developing a mix of small- to medium-sized organisations able to manage a diverse suite of waste types.
Accounting for Outpatient Activities and Informal Sector Activities
Outpatient care is when the patient is treated, without being hospitalised, in a GP or physician’s office. Although, in general, inpatient care (especially if involving an overnight stay) costs more, a hospital that has significant outpatient activity will spend more than one that does not (Lave & Lave, 1984). And healthcare researchers have thought of outpatient activities as an important variable to measure, or account for, in a cost function. Depending on the nature of the data available, researchers either control for outpatient activities as dummy variables, include it as an independent variable for total cost estimation, or subtract it from inpatient costs when using inpatient cost as the dependent variable. Other more advanced econometric adjustment methods for outpatient activity are also available.
Implications for SWM in Industrialising Cities
In industrialising cities, the relation of the informal sector to the formal sector for SWM has similarities to the relation between inpatient and outpatient services. The formal system is run by the local government and manages collection, perhaps some processing and disposal. The informal system can include a higher quality of collection service (e.g., daily instead of twice-weekly, or unit-by-unit collection in multi-tenant buildings), as well as informal recycling of source-separated waste. Either the collection or the recycling part of the informal sector can be closely tied to the formal sector in industrialising economies.
Although some attention has been directed towards developing cost functions for the formal sector path for industrialising countries (see Parthan et al., 2012b), because few cost data are available, little attention has been devoted to doing the same for the informal sector path. Just as inpatient care is generally costlier when compared to outpatient care, the formal sector path for SWM is generally more expensive than the informal sector path.
The effects of changes in the informal sector on the costs to the formal sector are less clear. Like the healthcare sector where outpatient care can reduce the cost of inpatient care, in many situations, one might expect that more informal sector waste management leads to lower costs for the formal sector. Private collection and transport of recyclables should increase the time it takes to fill a formal-sector collection truck, thereby allowing for a reduction in costs. On the other hand, if formal sector workers are collecting recyclables and selling them to the informal sector, or if they stop their vehicles to load non-recyclables collected by the informal sector, then costs would increase. There is also the potential for informal sector collection of waste to lead to more waste dumping requiring more costs by the formal sector to clean up dump sites and reduce the rate of infringements.
Some research questions that waste researchers could address under this topic are as follows:
What are the cost components of the informal SWM sector? Is there a direct or inverse relationship between informal and formal sector costs? Is there an optimum level of participation by the informal sector?
Often, source separation measures are advocated in industrialising countries for better management of waste. Research studies on informal sector costs could try to answer the following: if source separation is introduced, how would the marginal costs of collection, processing and market price of recyclables change?
Input Prices
The prices that hospitals need to pay for their inputs (personnel, supplies and drugs) have an effect on costs and are called factor prices. To control for factor prices when developing cost functions, healthcare researchers incorporate dummy variables for regions, population divisions (e.g., less than 500, greater than 1 million etc.) and whether it is an urban or rural location. At first, healthcare cost function studies requiring control over factor prices were crude, especially with industrialising countries, where often the only information available was on wages of employees. Using wage rates, sometimes crude indexes of factor prices can be arrived at, such as the wage bill per full-time employee. The studies controlling for factor prices have shown that costs increase with city size, but it is still unclear what exactly the city size variable is measuring (Liu, 2003). Lave and Lave (1984) speculated that ‘the prices of factors of production other than wages could increase with city size, in which case the coefficient is reflecting factor price differences. Alternatively, the nature of the demand for hospital care could vary, in which case the coefficient could be reflecting some unknown product differences.’ WHO has tried to identify and specify costs for poorer countries through their WHO-choice programme (http://www.who.int/choice/costs/en/) as a step towards controlling for input prices in cost analyses. To manage consideration of input prices, WHO has moved to annual updates as part of their cost estimation techniques.
Implications for SWM in Industrialising Cities
Analogous to healthcare, SWM costs will differ due to variations in input prices for labour, capital equipment and fuel for transport vehicles. These differences might be seen between different regions within an industrialising country providing the same level of service, or during different time periods. The differences in factor prices can be especially difficult when analysing data from multiple countries. Accounting for input prices becomes important for a fair comparison. Solid waste researchers might want to answer the following question in order to incorporate variations in costs due to factor or input prices: what is the relationship between SWM costs and variables of interest such as user fee revenues after controlling for input prices?
Data on input prices might not be readily available for SWM. While input prices are best obtained from service provider datasets, it could be necessary to rely on questionnaires. Strict confidentiality measures could be required in order to make progress on developing SWM cost functions that incorporate variations in input prices. Generally, data for number of employees and corresponding salaries of employees by job type might not be difficult to obtain, especially for municipal employees. The price for labour could be roughly calculated by taking the ratio of the total salary expenses to the number of employees. Capital price could be obtained by dividing depreciation costs by capital stock. If input prices are included along with other regressors, the quality of cost functions would improve. Healthcare experience indicates that there will be value in ongoing, perhaps annual and updates of input prices as part of cost estimation for industrialising cities.
Ownership and Control
Healthcare service providers can be broadly classified as public, private and community. One question that healthcare researchers have tried to address is whether one type of ownership was more efficient than the other, other things being equal. Is the cost of a hospital day in, say, a public hospital lower than a private hospital of the same size? This question is very sensitive to how the cost and output data are standardised across different institutions.
Implications for SWM in Industrialising Cities
Similar to healthcare, the type of ownership varies widely for SWM in a city. The type of ownership in SWM could be an important variable to consider when estimating costs via a cost function analysis.
The issue has been debated by researchers for some developed economies. Waste researchers have arrived at contradictory results (Bel et al., 2010), similar to what healthcare researchers have experienced. For example, Stevens (1978) found that private firms were more costly when compared to public–private joint ownership and attributed this to higher billing costs borne by the private firm. Others like Dubin and Navarro (1988) and Callan and Thomas (2001) do not find lower costs with private delivery, but have not explored the details. Bel et al. (2010) have used an approach known as ‘meta-regression’ in order to assess these contradictory studies and arrive at a more generalised result. Their study investigates whether private delivery is less costly than public delivery when controlling for other attributes. Their dataset compiled all previous studies in literature that tried to answer the ownership vs. cost question. They do not find concrete evidence that one type of ownership achieves more cost savings over another and conclude that future research should instead be directed towards the cost characteristics of the service, transaction costs involved and the creation of a policy environment to stimulate competition (Bel et al., 2010).
Over the years in industrialising cities, privatisation has been encouraged, public–private partnerships have been promoted and intermunicipal alliances have been suggested for the more capital-intensive activities such as building engineered landfills (Zhu, Asnani, Zurbrugg, Anapolsky & Mani, 2008), but no detailed analyses are available in literature that provide strong evidence in terms of the type of ownership that leads to lower costs.
Conclusions and Recommendations for Future Progression of Cost Function Analyses for Industrialising Cities
What seems evident from the healthcare management experience is that there were initially three broad objectives of cost function research. One objective was to address planning issues such as optimum size and scope of the service and estimate marginal costs. Another was to develop a better understanding of cost differences through explanatory variables that vary between hospitals and vary with healthcare costs over time. The final objective had been refining healthcare cost functions using more sophisticated econometric techniques to model them as closely as possible to the real world. These historical objectives for the healthcare sector provide the SWM sector with objectives for future work.
Analysing the Variables to Include or Exclude from Cost Functions
It is of first and foremost importance to know how SWM costs in industrialising cities are influenced by output levels and other variables such as contracted services and user fee revenues. Such attempts need a better understanding of the determinants of solid waste costs. One line of research should be directed to understanding the factors that affect the relationship between costs and tonnes managed. Some important ones such as facility size, ownership type and informal sector involvement have been discussed in the ‘Healthcare Management Research Results and Analogous SWM Research Directions’ section. Economic variables expected to affect costs of SWM include costs for labour, capital and fuel, and these also need to find their way into a cost function. Interpreting the regression of costs on variables could reveal which coefficients are positive and significant for SWM.
Using Cost Functions to Analyse Service Provision Questions Relevant to Industrialising Cities
A second line of research could be directed towards improving the use of cost functions by more clearly relating them to the decisions faced in industrialising cities. This means exploring, for example, whether or not economies of scale and scope exist, or how the informal and formal sectors can be used together more economically, so as to develop recommendations on preferred methods for solid waste service delivery. For a review focussing on this particular objective of cost function research, for capital intensive services like SWM, among others, refer to Bel (2012).
Develop Cost Function Analysis Methods Suited to Industrialising Cities
The third line of research could be directed to the development of econometric techniques particularly suited to industrialising cities. Similar to the early experiences of healthcare, it is natural to start with simple cost functions that will surely be unable to capture standard microeconomic theory assumptions. Progress on the objectives above will likely highlight the need to collect more and different data in order to suit improving cost function analysis methods. As research progresses and data quality improves, it would be natural to refine existing models or develop models that would capture the complexities of solid waste systems in industrialising cities. For example, more advanced cost functions than simple linear forms, such as the flexible functional forms, hybrid flexible forms and translog forms, which account for the multi-product nature of the service, will be needed and can be a topic for future research.
Footnotes
Acknowledgments
The authors acknowledge the contribution of insight and support from David Wilson and John Cocks. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.