
Abstract
Many ideas were implemented to protect the health of Indian citizens and refugees, rural and urban population, young and old, and men and women over several decades. Some of the policies are translated to programmes in the ground level and help improve the measurable rates and ratios of the health system successfully. There is an improvement in life expectancy at birth, reduction of child mortality and maternal mortality, control, and reduction of epidemics over a period spanning more than seven decades post-independence. However, the comparison of the health achievement of India with the global south and north brings much disparity in the achievement rates, of which India clearly belongs to the global south. This article highlights many salient features of relevant healthcare policies and the progress thereof in the crucible of time. The article discusses the key historical developments in the Bhore Committee report 1946, Planning Commission of India, Alma Atta Declaration 1978, Health for All by 2000, National health policy 2002, High-Level Expert Group Report 2011, National Health Policy 2017, Astana Declaration 2017, and Prime Ministers Jan Arogya Yojna 2018, along with other policy documents having a strong bearing on the healthcare system of India.
Keywords
Introduction
India, from the infantile stage of independence to a highly aspiring economic growth stage, there is a varied level of achievement in healthcare (Rao, 2016). Universal healthcare is always a target for realising the goals of ordinary Indian citizens (Park, 2005). From time to time, there is massive pressure on the state and central government to provide healthcare to the people of various walks of life. Over time, governments also develop policies, proposals, and ground-level implementation plans to enhance the delivery of health services (Rao, 2016; Reddy, 2019). However, meager budgetary provisions and a lack of hard and soft healthcare infrastructure never help pave the way for the achievement of goals in the health sector (Dehury et al., 2020; Park, 2005). The government in India is crippled with a lack of human resources, especially doctors and paramedics, a lack of affordable medicines, a shortage of infrastructure, non-availability of timely financial resources, unavailability of modern technology, and a lack of stewardship in the health sector (Dehury et al., 2020; Reddy, 2019). All these things make India’s health sector one of the weakest in the world, for providing essential healthcare services for millions concerned. All the health parameters reported by reputed agencies such as World Health Organization (WHO), UNICEF, and some nationally reliable sources were found to be low performing on India’s health achievement in maternal health, reproductive and child health, communicable diseases, non-communicable diseases (NCDs), geriatric care and vaccination (Park, 2005; Rao, 2016). India is a hub of information technology, healthcare innovation, producers of several medicines and medical devices, and an exporter of human resources worldwide (Dehury et al., 2019). In contrast, India faces challenges in providing healthcare to its citizens. Many Southeast Asian and African countries also have better healthcare achievements with less economic growth in the world (Dehury et al., 2020). This shows something needs to be fixed so far healthcare leadership is concerned, which is currently a rudderless approach to achieving an extraordinary goal of ensuring healthcare rights of millions.
Many countries such as Thailand, Chili, Singapore and Cuba have started providing healthcare with their low-performing economy and needed more required resources for overall development (Dehury et al., 2020). However, they achieve the set target for the nations with much efficiency in universal health coverage (UHC) within a few years by integrating various health sector planning procedures. The countries usually follow sound principles of healthcare to achieve the targets in fewer years. India has a lot to learn from the experiences of other countries in achieving UHC by adopting the right policy. India needs to address healthcare access for its over 1.2 billion population in a changing world with emerging disease and healthcare issues. The country must move at a steady pace in the health sector development while targeting global leadership and economic prowess.
Medical science and the provision of health services in India are discussed on a time scale to understand various policy aspects (Rao, 1968). Overall, any sector’s policy determines the progress of the community’s plans, programmes, and implementation. The health policy of a nation cannot belong to a particular government, political party, or pressure group. Instead, the country’s central health policy belongs to its people, who would benefit from it over several decades and realise their dreams (Rao, 1968; Reddy, 2019). The elected governments usually come and go, but the guiding vision of health policy would help maintain the health and wellbeing of the population. The strategic decisions should be robust enough to curb the existing challenges in the health sector and help in the near future, based on forecasting and evidence of the health sector (Dehury et al., 2020; Rao, 2016).
The health policy’s ownership should be deeply entrenched in the micro-level healthcare issues, which can only be possible through widespread discussion among various stakeholders (Dehury et al., 2020; Park, 2005). Expert consultations and the need of the people should gather the evidence to generate sufficient steam to achieve the targets. Usually, in a country like India, with diverse health needs, it is impossible to follow a single approach across the length and breadth. Therefore, local needs with global standards can help develop guiding principles to cater to the masses in the health sector. Historical evidence and discussions often help gather a unique way of looking at things. The lesson from failure and success would help devise tailor-made plans for the health and human services of the Indians (Dehury et al., 2020; Rao, 2016).
The article vividly discusses policy matters and strategic steps from Bhore Committee 1946 to National Health Policy (NHP) 2017. This period in India is eventful, with many success stories and failures in the post-independence period with open-minded thinking on the health sector. However, a glimpse of the medical services in the nineteenth century and the first half of the 20th century also discussed the health sector developments before independence. The provision of healthcare for the improvement of health is required according to the time. Evidence of UHC and the global narratives forced India to make it a buzzword, though it has been a mirage for many years in the health sector development.
The rise of private hospitals lacking accountability after the 1990s provides evidence of failed attempts to achieve the government’s set targets across decades. The National Rural Health Mission (NRHM) aims to push for a homegrown plan with tangible achievements in the health sector. The recent developments in the health sector, like ABPMJAY, are also briefly discussed to figure out the recent health sector achievement. Overall, the article discusses significant policy departures in Indian health sector developments.
Medical Services in the Nineteenth Century and First Half of the Twentieth Century in India
India’s public health movement started with the effectiveness of the quarantine act of 1825 to manage various communicable epidemics by British administrators. The services such as vaccination, registration of birth, and death started in the 1880s and 1890s to understand the demography and provision of care (Rao, 1968). The epidemic disease act of 1897 was promulgated to control India’s epidemics, which is effective today with its stringent measures to curb the spread of various diseases. The colonial power of Great Britain introduced services such as Indian Medical Services, Central and Provincial Medical Services, and Subordinate Medical Services to provide medical care in India, which helped in the services of the military, cantonment towns, industrial hubs, and administrative units (Mushtaq, 2009; Rao, 1968). At the district level, medical services were provided to a few selected populations under civil surgeon and medical officers’ leadership.
The Government of India Act of 1935 delineates the roles and responsibilities of the state and central government to provide specific medical services that are followed till now in many respects (Harrison, 1994; Mushtaq, 2009; National Library of Scotland, 2007; Park, 2005). The broad divisions of healthcare administration distinguish the role of the federal government, the provincial government, and concurrent medical services, where both governments have to work hand in hand (Mushtaq, 2009; Rao, 1968). This provides impetus in handling medical education, control of epidemics, screening of diseases, surveillance of the population and treatment of the people. The delineation of power helps in taking expeditious decisions and implementing programmes for effective treatment (Government of India [GoI], 1909; Government of Punjab,1937; Harrison, 1994; Mushtaq, 2009; National Library of Scotland, 2007; Park, 2005). Some of the health-sector developments in British India are given in Figure 1.
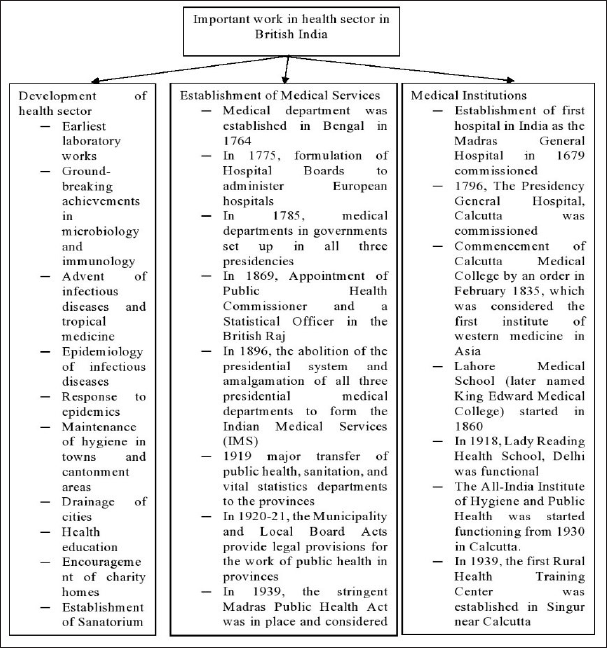
As an aspiring country during World War II, a detailed committee was set up under the chairmanship of Sir Joseph Lister Bhore to study the details of health services across the nation in the name of the Health Survey and Development Committee (Mushtaq, 2009; Park, 2005; Rao, 2016; Reddy, 2019). Sir Bhore tabled the report with an extraordinarily detailed presence of health services in the country with far-reaching recommendations for developing the health sector in India.
Post-Bhore Committee Period and Medical Services
A research article argues that India tried to develop sufficient medical schools and healthcare facilities for almost a quarter-century after the Bhore Committee report (Rao, 1968). The tangible developments were visible in creating more healthcare services as per the laid down principles, which are at par with the then European standards (Park, 2005). Efforts were there to catch up with the health services of developed countries in quality and quantity. A comparison of complex data between 1946 and 1963 shows the relative achievement in the health sector inching towards India’s targeted development post-independence. India inherited a brigade of 47,000 doctors in 1946, with only 13,000 doctors in the government sector and the rest in the private sector (Rao, 1968). Further, the prevailing situation was worse, with nearly two doctors per government health facility during the 1950s. So far, the health coverage in villages is concerned the situation is even worse. Only 2.5% of villages are lucky enough to have modern medical practitioners. Only 5% had Vaids or Hakims involved in providing the Indian system of medicine (Park, 2005; Rao, 1968). However, in 1963, the situation improved relatively, with the implementation of five-year plans and the utilisation of foreign aid in health sector development (Rao, 1968).
The overall bed capacity in health facilities increased to 238,000 by 1963 compared to a mere 73,000 hospital beds in 1946 (Rao, 1968). Further, the PHCs are established in rural India to provide healthcare services to the masses, making them accessible for primary and secondary care services. The PHCs, by and large, help provide medical care, maternity and child healthcare, health awareness, minimising communicable diseases, family planning services, environmental sanitation, health intelligence and vital statistics (Park, 2005).
The Planning Commission of India, in its very first plan, made provisions for improvement in water supply and sanitation, malaria control programme, preventive healthcare of the rural areas, improvement of maternal and child healthcare, medical education and capacity building, adequate provision of drugs and equipment, and population control (Rao, 1968). In this context of upgrading the services, the first five-year plan suggests a five-time increase of resources from a meagre ` 1.4 to ` 5.9 with an additional provision of ` 2.8 per capita per year towards a recurring budget (Park, 2005; Rao, 1968). The expenditure by various foreign governments in 1946 on healthcare services was relatively higher than India’s mere 4% of the budgetary provision. The fiscal provision for health in India could have been more satisfactory to cater already sulking health system ravaged by foreign occupation for more than three centuries. It has been reported that the UK spent 20%, and the USA spent 13% of the national income on the improvement of healthcare during 1946, which is way ahead of India in keeping their population healthy and productive (Indian Medical Journal on Bhore Committee, 1946; Rao, 1968).
India was marred with severe healthcare problems undermining the socio-economic development during independence. The western border was reeling from Punjab’s partition, with the migration crisis at the top (Rao, 1968). The eastern border faced with similar features and famine of worst of its type due to a lack of civil supply and other essential nutrition. The hinterland is nothing good; instead, the factors such as poverty, illiteracy and deprivation took centre stage, hindering population health and wellbeing. It has been estimated that three million people lost their lives due to health and related causes during independence (Rao, 1968). Hence, India has a daunting challenge to provide primary healthcare, sanitation, hygiene, and nutrition across the country, which shakes the soul of a newly born nation-state from the womb of Great Britain (Park, 2005).
There is some success in the programmatic approach towards disease control in India. The reduction of high-burden infectious diseases reduced, for example, malaria, which was found to be two million cases in 1947, to 75,000 cases a year after the implementation of the malaria control programme (Rao, 2016). The focus on control of infectious diseases and family planning during the first three decades of independence paid limited results. The overall development of the public health system still needs to be achieved (Park, 2005).
According to scholarly analysis, various committees set by India’s government look at the health problem in a piecemeal rather than a holistic approach, in which public health should be at the centre stage. Numerous committees such as Mudaliar (1959), Chadda (1963), Mukherjee (1972), Kattar Sing (1972), Srivastava (1975) and as many as 25 had provided recommendations to solve a particular problem instead of a holistic approach to solve the public health issues in an integrated manner (Rao, 2016). Overall, the systems approach towards achieving health sector goals was not found in the recommendations of the panel of experts, which was heavily represented by clinical and medical professionals (Park, 2005). By and large, the committees focus on something other than the community’s social, economic, and cultural aspects in providing health services that were found to be the cornerstone in many countries’ health policy.
Health Policy Evolution for Wellbeing of the Population in the Post-independence Period
India has 18% of the global population, which is approximately the combined population of six most populous countries of USA, Indonesia, Brazil, Pakistan, Bangladesh and Japan in the world (Patel, 2015; United Nations, 2017). With a large population comes a huge responsibility to feed and nurture human resources (Central Bureau of Health Intelligence, 2018). Initially, the population was a big burden on the development of India, which was understood even by the colonial government. Further, India is suffering from a double burden of infectious diseases, malnutrition, hygiene, immunisation, sanitation and infectious diseases at one hand, and NCDs stemming from lifestyle, environment and diseases having the web of causation on the other hand. Further, diseases such as cardiac origin, emerging tuberculosis, rising cancer, increasing diabetics and various vector and water-borne diseases threaten the Indian healthcare system to the hilt (Central Bureau of Health Intelligence, 2016).
Despite mammoth challenges, the spending on healthcare could be better, with only 4.10% of GDP in 2010 the system became more feeble (ASSOCHAM, 2011; World Health Statistics, 2010). Whereas the global average spending on healthcare is 9.7% of GDP. Further, the contribution of both state government and central government consists of only 26.20% compared to private and personal spending of 73.80%, of the total health expenditures. For many countries, the expenditure is more than or around 50% in the world from the government-sponsored programmes. Evidence shows that even in hardcore capitalist countries like the USA, the government spends 45.5% with one of the highest spending on healthcare, the UK (81.70%) with good social security schemes, Brazil (41.60) and China (44.70%) being BRICS countries similar to India (Grover & Singh, 2020; World Health Statistics, 2010). India spends very low compared to similar development-level countries for various reasons. However, efforts in policy documents promise to increase healthcare spending to a great extent, which is yet to be seen despite political up roaring for better health and social welfare. To make sure healthcare activities increase in India, the government made provision in the constitution and amendments favouring the people.
Role of the Indian Constitution in Shaping the Health System in India
India adopted a new constitution with much hope for improving the lives of citizens through different acts and statutes. However, health was primarily kept as a subject of directive principles of state policy in the entire constitution making process, which means as per availability of resources the problem of healthcare would be solved rather than right based approached of European countries (Grover & Singh, 2020). With an emphasis on improving health, the system gears for providing resources to enable the fullest development of an Indian citizen. There are provisions in the original constitution for the improvement of health in many acts that help the judiciary and civil society to enable enforcement. The constitution has a firm understanding that public health, sanitation, dispensaries and hospitals function under the state list (Entry 6, State List II). However, many things such as population control and family planning, regulation of medical education are on the Concurrent list (Entry 20 A, List III) (GoI, 2015; Gupta, 2002)
Article 21 ensures the right to life as a fundamental right, where the state has to protect it at any cost for its citizens. Whereas, Article 23 forbids human trafficking, which includes the protection of life from many eventualities. Prohibition of child labour is implemented through different arms according to Article 24. Article 39 empowers the state to direct policies by removing abuse of its citizen and strengthening men, women and children. Special provisions for conditions such as old age, sickness and disability-related issues are in Article 41. Article 42 ensures creation of humane conditions at the workplace and maternity benefits for working women. Without nutrition, nothing is possible, and Article 47 ensures that. Interestingly Article 243G, 243 W, with the 73rd and 74th amendments in 1992, decentralised power to the local bodies for portable drinking water, health improvement, sanitation provision, the functionality of PHCs, promoting family welfare, women and child development and mentally retarded persons (Grover & Singh, 2020).
The constitutional provisions enshrined in the constitution look rosy in writings and readings of literature. The fundamental transformation happened by the functional government at the ground level. These constitutional provisions were taken as pool star, and policies and programmes were devised according to the requirement of the system. The transformation happened in a very different way across India over time. The southern states have especially done well in many human indicators of health relating to mortality and morbidity. The rural–urban divide also became more glaring over time even in developed states of India. The social determinants of health played a role in healthcare achievements across social strata, despite consciously negating the effect in policy documents, so that the government aid reaches the marginalised.
Five-year Plans and Effort for Galvanising Health Sector
The grave condition of the healthcare system in India with communicable diseases remains an unchallenged problem, which is evident from conferences on health across the globe and planning commission data sources. The five-year plans make some arrangements to improve health conditions by limiting death and diseases. The first-, second- and third-five-year plans in the 1950s and 1960s focused on managing the ravaging epidemics across India. One good thing that happened was the nationwide campaigns to curb diseases such as malaria, smallpox, tuberculosis, leprosy, filaria and cholera were reduced to a great extent. The techno-centric approach helps in the prevention and control of diseases with help from well-known expert groups and ideologues across the world. By and large, India depends on medications and technical know-how from foreign countries, United Nations bodies, multilateral agencies and many international bodies. Evidence shows that there needs to be more awareness of many factors such as social, economic, and environmental factors, dietary regimen, nutritional level, housing and clothing in majority parts of the country. It is also noted that the urban-centric approach marginalised the rural folks to a great extent, even today perpetuating across states and regions. Mudaliar Committee in 1959 observed that the first two plans had success stories in control of disease-specific deaths, improvements in life expectancy and reduction in death rate. The committee pointed out the need for more staff in primary health centres (PHCs), which also needs immediate human resources and infrastructure revamping to serve the rural folks (Grover & Singh, 2020; Sharma, 2017).
The third five-year plan emphasised the numerical and quality of setting up of medical colleges, research institutes and training centres for clinical and para-clinical staff. The fourth plan perpetuates some suitable government activities across India and focuses more on water and sanitation issues. The fifth five-year plan through the Minimum Needs Programme focused more on rural areas for good health to minimise the gap between rural and urban areas. This phase was marred by an emergency declaration, which limited the rights of people. However, a programme for controlling communicable diseases continues (Grover & Singh, 2020).
The sixth five-year plan coincided with the international declaration of ‘Health for all (HFA) by 2000
The eleventh five-year Plan coincides with inclusive growth which was also reflected in health sector planning and development. NRHM played an essential role in providing healthcare in rural India and tried to improve the health of the rural population. The twelfth five-year plan comes up with ideas of realising UHC through an Essential Health Package (EHP) with robust private sector involvement through different purchase mechanisms (Planning Commission of India, 2013). Many activities relating to systems strengthening with proper economic growth helped in capacity building, which led to further planning through a brand-new health policy in 2017 (Gupta & Kumari, 2017). Overall, the five-year plans have an indelible mark on the health and wellbeing of the Indian population (Grover & Singh, 2020).
The First Health Policy of 1983 and the Vision Thereof
The first health policy of 1983 was discussed, in a given situation of structural adjustment plans and the opportunity to catch up with Western standards. With its limited economic prowess, India developed an efficient policy document for the health sector in 1983 after realising the Western models of diseases specific approaches do not work in the land (Rao, 2016). Hence, there was a tectonic shift in health policy from the existing disease-specific critical and curative approach to a more holistic promotive, preventive and curative approach by strengthening the primary healthcare centre with an integrative approach (Park, 2005). Community participation in health services was augmented for preventive care and screening of diseases, which usually help tackle communicable and NCDs in the community.
The 1983 health policy advocated for an integrative approach rather than compartmentalisation of programmes with a limited focus on a few components of health (Park, 2005). However, overall healthcare architecture remained the same. The resource crunch was palpable, which hindered augmenting people’s healthcare services according to the vision of the health policy in 1983. Authors also opine that due to the structural adjustment plan and governments’ favour towards privatisation, India thought of healthcare as marketable goods that were otherwise primarily considered a welfare measure in the past (Dehury, 2020; Rao, 2016). Considering healthcare as a commodity in the hands of the private sector does not allow the government to go ahead with the vision of NHP 1983 (Park, 2005).
The liberalisation of the 1990s put the death nail by not considering healthcare services as a matter exclusively for the public domain. Instead, healthcare was left to private sector investments with technology-intensive and curative patient care services (Dehury et al., 2019). Evidence found that despite the massive increase in economic growth during the 1980s and 1990s, there is a widening gap between India’s rich and poor, which was detrimental for the poor and marginalised to access private facilities for healthcare services (Rao, 2016). In the socialist phase, the government was a dominant player that funded, owned, and provided healthcare to the people. Overnight, healthcare situation was changed to a capitalist set-up with minimal government role and provision of healthcare. The invisible and fragmented private sector soon becomes a significant organisation for providing healthcare for fee-for-services. The competition has become fierce in healthcare for different private players (Dehury et al., 2019). Despite improving the quality of the health services, there needed to be more healthcare services for the marginalised. Overall, the commodification of healthcare was found to be a lucrative business for the capitalist, which was a norm even until the 2020s. The Indian nation–state fails to protect its people even during health emergencies such as life and death. It has often been argued why the principled welfare nation–state of India fails to provide essential healthcare services and pushes the majority of the population into risk of health vulnerability (Dehury et al., 2019). For whose interest India left its people to the brink of suffering. The question of universal heath coverage still hunts the past governments and the governments have yet to answer.
Pressing Provision of Healthcare and Policies for the Improvement of Health
UHC later became a buzzword in global narratives on healthcare irrespective of the paying capacity of the people who needs care. The UHC needs a sustained approach to achieve healthcare goals where the marginalised would get sufficient protection for essential healthcare. In this context, many countries see Essential Health Packages (EHPs) with minimum services guaranteed to provide care to the citizens and refugees (Kieny & Evans, 2013). The concept of transformation of EHP happened with the 58th World Health Assembly’s resolution in the year 2005 with regard to UHC among many countries (World Health Organization [WHO], 2005). India also tried its share to achieve healthcare progress towards achieving UHC. India’s trial for providing better health services to all was there in policy since the Health Survey and Development Committee (1946), which is popularly known as the Bhore Committee (Health Survey and Development Committee, 1946). The catchy words such as equity in healthcare, quality healthcare, and universal provision of healthcare were always there in the Bhore Committee recommendations. Nobody knows what went wrong in the implementation process, so these words are still catchier at the current time. The architectural overwhelming happened only in 2005 with the NRHM’s launch, which provides proper guidance for the UHC (Reddy, 2015).
Much of the demystification of UHC comes from the Alma Atta declaration of 1978. Research in the 1980s reported that the Alma Atta declaration of 1978 agreed on indicators 1 and 2 of the document by many of the countries that primarily focused on people’s involvement in implementing developmental health programmes (Roy, 1883). However, the problem started when the third indicator of the document was discussed, which advocated provision of at least 5% of the gross national product (GNP) specifically for the health by all countries (Roy, 1883). The developing countries are not satisfied with healthcare investment explicitly; instead, they argue that socio-economic development is linked with the country’s overall development. Further, the GNP’s 5% investment is quite tricky for the least developed countries to spend on healthcare. The low- and middle-income countries were reeling with problems in many sectors, which force them to postpone investment in the health sector instead of understanding and agreeing on a multilateral convention like the World Health Assembly. In its sixth five-year plan, India allocated 2.40% of the GNP towards the health sector in the budgetary year of 1978–1979 and 2.10% in 1979–1980, which coincides with the Alma Atta declaration year (Roy, 1883). So, from a historical perspective, the spending of the Indian government is much below the targeted 5% for healthcare.
Another study of the 1980s argues that despite health gain in those days, the rural and urban divide was vast, which undermines the cause of achieving HFA by 2000, set in the 30th World Health Assembly in 1977 (Sinha, 1983). Hence, the emphasis was on mobilising resources for the rural area to provide preventive and curative healthcare with the village as a base. There has been a massive problem in society so far, as health achievement among geographies and social groups is concerned in India. The post-independence gains in the social sector had not percolated throughout the length and breadth of India. At the time of the Alma Atta declaration, the population load on PHC and sub-centres were 0.1 million and 8000, respectively, which is very high in the Indian context (Sinha, 1983). Instead, efforts must be there to achieve the recommended workload for PHC and sub-centre for a population of 30,000 and 5000, respectively, to provide optimum healthcare (Park, 2005).
Evidence found in the late 1990s that the population explosion was a big concern in achieving HFA (Tabish, 1997). Most public health programmes geared towards reproductive and child health services which is mooted by the idea of controlling the population explosion. The health systems have to be given importance to achieve primary care despite the shortage of doctors in rural areas. The specific programmes to prevent communicable and NCDs are few and regulated by the central government, primarily influenced by vertical healthcare programmes. The resource crunch is the main huddle to achieve HFA by the target date (Tabish, 1997). Health financing remains a nightmare for India’s government due to the low prioritisation of health in a politically charged Indian governance system.
Evidence for UHC in India
The Indian health sector continually adopts reform mechanisms with informed policy evidence to achieve UHC (Prinja et al., 2020). The latest Ayushman Bharat Yojna targeting UHC is believed to be the world’s largest programme of inpatient care services (Singh, 2018). The scheme targets marginalised groups’ coverage in the first phase and gradually include more people (GoI, 2011). The scheme also focuses more on preventive and primary care services with its new arms, such as health and wellness centers, rather than depending on existing healthcare structures.
According to WHO, the essential component of UHC constitutes the strategies for financing such as efficient taxation, adequate government budgets for healthcare, innovative methods for financing health services, and mustering development assistance for healthcare (WHO, 2010). However, the mentioned strategies are out of the ambit of the Ministry of Health (MOH) in India; instead, the health ministry has to depend on other government divisions’ mercy to garner all the required resources. Authors argue that the health ministries must put forth evidence-based policymaking and budgetary provision in the government to gather adequate fiscal requirements (Zodpey & Farooqui, 2018). The arguments for more funds for UHC have to be supported by the concepts of return on investment and other health economic metrics such as disability-adjusted life years, quality-adjusted life years, net lives saved, and overall pressing need of the population (Dehury et al., 2020; Zodpey & Farooqui, 2018). Many more socio-economic concerns in India are more critical than health concerns for a democratically elected government. Hence, as a matter of politics, health never gains the currency to attract the masses to pressure the government to spend more on healthcare services. Most state governments (provincial governments) easily get away with little development in the health sector and manage to win elections after elections. Public opinion for better health services is at rock bottom; thus, demand for health services is not concerned in many Indian states except very few such as Kerala, Tamil Nadu and Goa (Dehury et al., 2019, 2020). At this juncture, the health ministries are doing routine jobs with little increase in the overall health budget as a percentage of the GDP of India (Park, 2005).
There are suggestions for enhancing the tax revenue in low- and middle-income countries to generate resources for the healthcare system. There is a requirement to collect an additional amount of $9.86 towards public health expenditure per capita, for which the effective tax collection has to be increased by $100 per capita (Reeves et al., 2015). The WHO focuses on achieving UHC by making sure of the workability of core components like the population coverage by existing healthcare systems along with the range of services available to a population, and the coverage of financial risk availability to the local community (Rahman et al., 2017; WHO, 2014). This is how India has to follow the intricacies of recommendations by the World Health Assembly and WHO to achieve UHC.
Bhore Committee (1946) to Astana Declaration (2017): Response of India Towards Health Care
India continually formulates many things to work out for the achievement of health among the masses. The Bhore Committee developed such aspiration during the time of independence. It is well known that India struggled to achieve UHC during the formative years of government. However, the effort continued to accomplish essential healthcare targets. India also showed its eagerness to achieve global standards by putting effort into improving healthcare targets (Park, 2005). In the meantime, in 1978, an international declaration in Almaty, Kazakhstan, was given for providing healthcare to all on the aspects of primary healthcare. This conference brought health experts and world leaders in a vigorous engagement to achieve HFA with enormous commitment. Since the last four decades at the global level, this Alma Atta Declaration 1978 has played a pivotal role in providing primary care services (Rao, 2016). As India is a signatory to the declaration of Alma Atta and a world leader in enforcing many conventions, it has followed many aspects of the declaration on various health sector targets.
Forty years after the Alma Atta declaration, another high-profile Global Conference on Primary Health Care was held in Astana, Kazakhstan, recently in the year 2018 to enforce the vigorous effort of the role of primary healthcare. The Astana declaration reinforces providing the highest standard of healthcare to everyone in every place (Declaration on Primary Health Care Astana, 2018; WHO, 2018). The new declaration advocates the successful primary healthcare model with commitment from the elected governments, functioning non-governmental organisations, active professional organisations, action-oriented academia and development organisations. The Astana Declaration mentions primary healthcare features, having tested quality, safe in form, comprehensive in nature, highly integrated, easily accessible, readily available and cost-effective for everyone. In addition to the essential features, the health service has to be provided with a high degree of compassion, respect, and dignified manner by well-trained doctors and paramedics with a high degree of motivation and commitment (Declaration on Primary Health Care Astana, 2018; WHO, 2018).
The Astana declaration also shows unhappiness about the abysmal achievement in healthcare services primarily for the poor and marginalised despite a similar declaration in Alma-Ata, erstwhile USSR four decades ago. The declaration mentions that it is ethically, politically, socially and economically unacceptable that equity is not maintained and that health outcomes have long been showing disparity (WHO, 2019). The Astana declaration also advocates for immediate action against NCDs, tobacco and alcohol abuse, poor lifestyle, harmful behaviors, lack of physical activity, and unhealthy diets. Concerns are shown in the declaration for short lives due to fierce wars, violence in society, wide epidemics, natural calamities, climate change effects and unexpected changes in weather (WHO, 2018).
The Astana declaration must act as a guiding star for India’s policies in the health sector. The very concept of primary care has to be integrated into India’s healthcare system to serve the large population. The current scenario for primary healthcare still needs to be revised on aspects of low capacity to reach more people in India, especially the marginalised section of society. India swung into action according to the Astana declaration due to many obligations. The Bhore Committee focuses on health infrastructure, including primary care services, at the national level. In the changing scenario, the Astana Declaration also reiterates similar primary care services for the masses, in which India also extensively participates. Hence, the philosophy of fair provision of healthcare services needs to be taught in the coming days.
Exclusive Government Resources in the Progress of Healthcare in India
The Bhore Committee report suggested a massive investment in the nation’s primary healthcare system, looking at the population and geography in the 1950s. However, at the central and state level, India needs to earmark sufficient resources over decades. The objective of public finance for ameliorating the health issues just remained in the documents of bureaucrats and just keep peeping towards the people’s awful health conditions over several decades. The state governments are entrusted with much more responsibilities in their geographical jurisdiction with minimal support from the central government. Only some state governments have shown progress with their local resources and efficient teamwork in the health sector, but most state governments fail to understand the responsibility. The central government’s guidelines and expert knowledge remain in cold storage for many years due to a lack of fiscal provisions in the government budgets. In between, being a country of the global south, some foreign aid came to India, which helped in controlling of diseases such as malaria, filarial, leprosy and HIV/AIDS. During the 1980s, the structural adjustment plan forces us to consider the vigorous provision of healthcare financing to augment investment in the health sector (Guruswamy et al., 2008). A lack of resources and stabilisation of macroeconomic parameters in mainland India mooted the adoption of a structural adjustment plan.
Overall, the provision of healthcare services as public goods to support people’s health is deeply entrenched in the economic theories of development. In addition to many externalities, there is uncertainty in the healthcare services and huge information asymmetry in the health sector, leading to market failure (Guruswamy et al., 2008). Thus, the government must provide healthcare, considering it a public good to the people. Further, the equitable distribution of healthcare services is necessary for countries like India to achieve a minimum level of healthcare for people of various socio-economic gradients (Dehury et al., 2019).
The argument for government financing at different times strengthened due to numerous factors. As a country, India has two different types of progress in healthcare, which can otherwise be called a health system at crossroads (Peters et al., 2002). There are healthcare achievements and deprivation simultaneously in the disease patterns, success stories and paradoxes across regions in healthcare. There are substantial demographic, epidemiological, and social transitions across the geographies and strata of the societies in India (Guruswamy et al., 2008). Fundamental public health issues such as sanitation, hygiene, drinking water and nutrition marred the health system. Further, the addition of communicable diseases, and HIV/AIDS, makes the situation more complex in a fluid state of affairs (Misra et al., 2003).
The public expenditure on health is quite low and has hovered around 0.9% of GDP for decades, far below India’s counterparts of middle-income countries across the globe (Peters et al., 2002). The health domain is classified as a state subject that puts the onus on the state governments to spend more on curative and public health. The states cover around 75% of the expenditure compared to a 25% share of the central government in various programmes (Peters et al., 2002). Insurance in different forms, such as private insurance, social insurance, community insurance and employers’ share, covers nearly 14% of the citizens in India (CII & McKinsey, 2002). Therefore, the risk pooling is near non-existent among the Indians, causing huge financial pressure for hospital-related expenditures. Due to borrowing and a high percentage of annual expenditure towards healthcare costs, about one-fourth of Indians go into the poverty trap with catastrophic expenditure (MoH & FW, 2006). Evidence galore from many studies that there are biases and utter inequalities in providing financial resources in the public health system (Duggal & Amin, 1989; Duggal et al., 1992; Gill, 1987; Prinja et al., 2019). A study confirms that the subsidy in healthcare often disproportionately benefits the rich rather than the poor in the Indian set-up (Mahal et al., 2000).
The arguments show the heavily commercialised condition of healthcare in India. The government is also unable to help the population receive decent healthcare services. Instead, the majority is allowed to be slide into catastrophic healthcare expenditure despite the presence of a functional government by and large claiming to work for the people to the hilt. It is mind-boggling to understand why the exclusive provision of resources is not made to create healthcare services despite its cascading effect on the positive role in the Indian economy. The political demand for health services can flip the situation and force the government to allocate exclusive resources for health sector development.
The Rise of Private Hospitals with a Lack of Accountability After 1990s
The private sector hospitals made a footprint in the late 1990s to support the sulking government health system by adopting modern healthcare technology and advanced processes in the healthcare delivery system. Every effort was given to complement and supplement the gap in the health sector by encouraging the private health sector to remove the bottlenecks in establishing hospitals. There was the provision of free land, government subsidies, relaxing the regulation, and a conducive atmosphere to promote the establishment of private corporate hospitals across India (Kurian, 2015; The Hindu, 2011). The creation of additional beds, access to millions of population and provision of the Western standard of care was the motivational force for encouraging private sector hospitals in India. However, private hospitals were found to serve a minuscule affluent population with a profit motive at the centre stage (Dehury et al., 2019). All the subsidies given by the government to increase access were futile over time. The situation is even worse, with only a tiny section of society covered by health insurance in the 2020s, which creates some additional access to private hospitals. The out-of-pocket (OOP) expenditure is continued to pauperise the Indian population in case of hospitalisation in a private hospital (Prinja et al., 2019).
There is evidence of exploitation and blackmailing by private hospitals to recover the healthcare bill from indigent patients despite the provision of government subsidies (Mamdani, 2004; The Diplomat, 2016). The matters such as overpricing, unnecessary treatment, and malpractices are commonly reported in various private hospitals in India (Satyameba Jayate, 2016; Times of India, 2016). Over some time, it has been observed that Indian private-sector hospitals are not sensitive towards patient care (Mamdani, 2004; The Diplomat, 2016; Times of India, 2016). Private hospitals usually provide services to patients with health insurance, corporate tie-ups, and general physician referrals for care provision. Access to private hospitals is more for higher socio-economic people, making it an affair of elites in India (Dehury et al., 2019).
The rise of private tertiary hospitals helps only a few elites of the urban areas mostly. So, the motto of establishing a private hospital is a futile attempt to achieve UHC. The capitalist model of healthcare services in India is only helping a small section of society (Dehury et al., 2019). Therefore, it is advised that the government provide healthcare services to its people by securing them financially (Prinja et al., 2019). The highest level of care available with recent technological development must be subsidised for the Indian masses to achieve population health.
Accountability of Government and Provision of Financial Resources
Accountability is an essential aspect of government and has to be enforced as per the system’s need for the overall outcome of the programmes. Without accountability, no programme can be significantly transformed in public services, including healthcare services. Accountability has been paramount in many policy documents and programmes catering to the public in India over several decades. In the health sector, accountability is a more significant concern for the delivery of healthcare services. Healthcare services are often in need, so an accountable system can only provide services for maintaining good health across communities and social groups. Many healthcare programmes need long-term implementation strategies to achieve the health programme’s goals (Dehury et al., 2019). Here also, accountability plays a role in deciding the outcomes.
Governments worldwide are not just safeguarding the boundaries and maintaining law and order in their respective countries but also care a lot about health and social security in their jurisdiction. Further, governments must deliver on specific aspects of public services and act as providers of services, including healthcare. This put enormous pressure on the governments to toe the line of accountability for the swift provision of healthcare services to the nation’s esteemed citizens. This necessitates accountability for improved health systems and essential governance (Barbazza & Tello, 2014; Mikkelsen-Lopez et al., 2011; WHO, 2007). The literature argues that answerability for an obligation is required, and there is a requirement for transparency and enforceability (George, 2009). Conceptually though there is an agreement about the meaning of accountability, authors still found accountability as a vague, nebulous or chameleon-like concept (Mulgan, 2000; Schedler, 1999; Van Belle & Mayhew, 2016). Accountability has various political, fiscal, administrative, legal and constitutional aspects to address the concerns (George, 2003). The recent trends show accountability is more community based than the older form of bureaucratic-centred factors (Ackerman, 2011). The Indian healthcare programmes have been less accountable to the people over several decades. That is why people are more dissatisfied with the government so far as health services are concerned. Instead, the citizens resort to private-sector healthcare providers for better accountability in India. Despite the private sector’s exploitative nature, people found more accountability in providing care to private healthcare providers. Evidence also emerges that government, when it wants to do things quickly, it trust the private sector to deliver the products.
The health sector’s accountability is unique due to the influence of various factors from the other public services in a government. Stakeholders influence the accountability of the health sector. Specific interest groups may influence the policy on accountability (Walt & Gilson, 1994). Studies also found that the size and scope of the healthcare organisations and the private and public ownership of the healthcare organisation also influence policymaking and accountability (Brinkerhoff, 2004). Studies found that patients have less say in the process of participation in the decision-making of any healthcare organisation. Patients need more choices in receiving healthcare services. There is no political concern for a participatory process (Yishai, 2012).
One study reported using National Sample Survey data that poor people spend more on health services in public (government) hospitals of poorer states in India. The poor people of rich states like Tamil Nadu spend less than poor people of poor states like Bihar, which spends more for each hospitalisation episode. Hence, this study suggested the free supply of medicines, surgical interventions and relevant diagnostic tests, especially in public health centers, leads to low out-of-pocket expenditure (OOPE) for the poor (Dash & Mohanty, 2019). The paradox is that the people who need more government services are left with fewer healthcare services. The poor in India have difficulty with the accessibility and affordability of health services. If he is a poor citizen, the matter worsens in a poor state. The regional disparity is very much in the provision of healthcare services. Here the accountable system can only help address the problem of disadvantaged people. It is also evident that the low-performing states need more accountability to address the issues with limited resources.
A study in 14 low- and middle-income group countries of Asia shows a high degree of dependence on direct payments for healthcare without sufficient social protection (Van Doorslaer et al., 2006; WHO, 2010). Whereas any sensible country does not advise direct payment for purchasing healthcare services; rather, the purchase can be subsidies or an insurance model for the benefit of people. Accountability is low in India, which is evident from the significant presence of the private sector in healthcare services. The government needs to involve more in reducing the direct purchase of healthcare services by the citizens (Prinja et al., 2019). A few subsidy and insurance model in private sector has been given importance in the last few decades, making the Indian healthcare market more unaffordable for the marginalised.
Usually, the increase of OOPE is strongly correlated with rising NCDs, more elderly population, escalation in cost of care, improvement of overall spending, lack of penetration of health insurance, lack of modernisation of medical technology, and less government provision for healthcare spending (Kumara & Samaratunge, 2016; Li et al., 2012; Molla et al., 2017; Pandey et al., 2018). The rising expenditure on health is always a concern for the regional differences in the utilisation of healthcare services and among various socio-economic category people (Xie et al., 2014; Xu et al., 2007). According to sustainable development goals (SDGs) the governments have to take care of the people’s health and reduce the direct expenditure on healthcare spending, which would usher goodwill in the community (Balarajan et al., 2011; UNDP, 2015). The accountabilities in line with societal philosophy on care have to be addressed by the Government of India.
A study suggests the requirement of EHPs is essential with considerable emphasis on overall coverage, equitable distribution, financial protection and the morbidity and mortality burden. It has been seen that there is a reduction of expenditure for treatment by including poverty-ridden people in the treatment plans, which is established by analyzing the data on morbidity, unmet need for treatment, and poverty due to OOPE. The government’s protection of healthcare expenditure for the people has many externalities and positive health gains in India. Unlike the Western world, Southeast Asian countries need the government’s intervention to show accountability.
The disease requiring primary healthcare contributes to the highest burden in outpatient care. At the same time, maternal and reproductive health services follow the highest burden in India’s government scheme’s inpatient care. Outdoor services of the hospital take respiratory infection care. In comparison, injuries of varied types were taken care of by indoor services. Another study confirms that mostly 27% of patients suffer from respiratory disorders among those who visit outdoor patient care services (Gupta et al., 2015). The attendance of all kinds of healthcare problems in government facilities creates much accountability for the government.
In India, one of the essential issues always ignored is equity in the distribution of government services. The efficiency of addressing the problems of the poor is always ignored. The insurance schemes need to explain the amount and extent of coverage while making programmes. What types of services must be covered in a programme, and for whom are they missing? It has no specific target to solve the problem in a time-bound manner. In a study on health equity, factors such as maximisation of health, optimal benefits to the poorest and finance provision for risk were studied and found to be against the marginalised groups (Prinja et al., 2019).
Evolution of the National Health Mission (NHM) Since 2005 and Achievement in Healthcare
Under the National Common Minimum Programme (NCMP), Dr Manmohan Singh’s Government tried to bridge the divide between the rural and urban areas in the provisioning of healthcare services by improving the healthcare human resources, infrastructure, and medical supplies across India. A welfare measures in the name of NRHM was hoisted on the 12th of April 2005 to provide reasonable healthcare for India’s people, which aims to improve accountability, accessibility and affordability, especially for the marginalised section (Dhingra & Dutta, 2011). Later on, NRHM was renamed as NHM, which contains both NRHM (rural) and NUHM (urban) for both rural and urban areas. The goals of the NRHM were to enable community ownership and higher demand for health services along with strengthening health systems. The NRHM is a homegrown model of care with a holistic approach, which was the integral model rather than a piecemeal approach. Besides integrating the Indian systems of medicine into the existing health system, the mission focused on related health issues such as nutritional aspects, sanitation and hygiene, and safe drinking water for the Indian populace. The very Indian Public Health Standards (IPHS) are also patronised for improving quality in implementing NRHM at health centre level (Dhingra & Dutta, 2011).
A study in 2011 reported that with the augmentation of health facilities, NRHM helped to create health infrastructure of the tune of 146,036 sub-centres, 23,458 PHCs, 4,276 Community Health Centres, 2,463 First Referral Units (FRUs) to meet people’s health Needs in partnership with the States, 2010). All the improvements and provision of healthcare services are possible by maintaining a network of healthcare providers with government subsidies.
The Accredited Social Health Activists (ASHAs) helps in building the rural health infrastructure by liaisoning between the healthcare facilities and communities using Janani Surakhya Yojna, specifically focusing on maternal and child healthcare services. The ASHA workers found to be beneficial in reducing maternal and child mortality and many public health achievements (Ministry of Health and Family Welfare [MoH & FW], 2010; NRHM, 2011). Despite all the accomplishments of NRHM, there are many challenges in India’s health system in terms of lack of inter-sectoral coordination, lack of timely resources and insufficient supporting infrastructure from other departments for improving healthcare of people.
The decentralised planning at the district level and involvement of Panchayati Raj Institutions are supposed to enhance people-centred healthcare. NHP 2002’s goals were translated into the NRHM to implement at the ground level (Taneja, 2005). The NRHM also tried to remove the age-old inefficiency of healthcare programmes and brought accountability to the system. Further, the display of the citizen’s charter at health centres and functional Health committee (Rogi Kalyan Samitis) with members of civil society and NGOs helped improve the quality of the service at the grassroots level. However, the record of Indian states is highly influenced by socio-cultural aspects, making the rural areas inaccessible to healthcare and basic infrastructure. There is also the influence of the state’s politics in undermining the functionality of NRHM (Taneja, 2005). The mission mode programme keeps funding many rural health infrastructures for improvement of healthcare services.
High-level Expert Group (HLEG) Report on UHC
The High-Level Expert Group (HLEG) on UHC was set up under the aegis of the Planning Commission of India in 2010 to undertake a study and suggest measures for the overall health of India. The central proposition of HLEG recognised that Indians could be provided with required healthcare through available financial resources by revamping healthcare infrastructure and financial mechanisms for health protection. The private sector must be included in providing at least 75% of outpatient care and 50% of in-patient services under the state-sponsored schemes to achieve Universal healthcare. The areas of Health Financing and Financial Protection, Health Service Norms, Human Resources for Health (HRH), Vaccines and Technology, Community Participation and Citizen Engagement, Access to Medicines, and Management and Institutional Reforms have to be undertaken to achieve the UHC (Thakur, 2011).
The report has 10 guiding principles for the achievement of UHC; these are universality of population, equity among citizens, non-exclusion and non-discrimination, provision of comprehensive care, financial protection of marginalised people, right-based approach for population, strong public health approach, accountability and transparency in functionality, maximum community participation, and creating responsible citizenry by putting health in people’s hands (Planning Commission of India, 2011).
There are many shortfalls in achieving the recommendations of the HLEG report in a given timeline. Evidence found that the human resources for health required for both the private and government sector involvement. Ultimately this needs enormous capital investment, along with the creation of infrastructure and systems strengthening (GoI, 2017b; GoI, 2017c). The financial protection of healthcare for the entire population is difficult, especially in a populist democracy where many other investments need priority (Sen, 2012). After HLEG report and passage of time the National Democratic Alliance (NDA)-led government brought a fresh NHP in 2017 as a promise quality healthcare for everyone.
NHP 2017 and the Envisioned Future of Healthcare
The Government of India brought the NHP 2017 on 15th March 2017 after wide-range consultation with various stakeholders. However, the initial draft was kept for 34 months in public domain facing many hurdles before being finalised (GoI, 2017a). The NHP 2017 has a clear objective to implement the healthcare agenda of NDA-1 Government, especially the proposed National Health Assurance Plan. The goals, policy principles and objectives of the NHP 2017 were supposed to lead and achieve UHC (Sundararaman, 2017). The policy tries to lower the financial barrier and generate demand for health services for the Indian population, especially marginalised groups, in the first phase. The NHP 2017 focuses explicitly on eradicating many diseases and improving people’s health. The health policy usually tries to save patients from catastrophic expenditure and indirectly improve the economic situation (Maruthappu et al., 2016; Weissman et al., 1991). The policy targets assured healthcare services by providing drugs, diagnostics, and emergency services.
The fundamental principles of the NHP 2017 are professionalism, ethics, equity, affordability, quality of care, collaboration and pluralism. The healthcare services must be committed to integrity, the highest degree of professionalism with strong alignment to ethical standards. Maintenance of transparency and a sustainable environment is also a priority for the service providers. The focus of the policy over several years would be to reduce inequity and disparity based on various socioeconomic factors such as caste system, gender group, disability, and economic status, especially in the government sector. Affordability and accessibility across social structures must be increased with a solid policy to provide the highest standards of care (Health-related Policies and Programmes of Government of India, Karnataka and Kerala, 2018). Further, quality of care is given much more importance with confidentiality regarding safety, gender-sensitivity and convenience healthcare services. The existing corrupt practices must end irrespective of government, trust or private sector. The concept of collaborativeness must be inculcated along with a multi-stakeholder approach among health ministries and communities. The role of academic institutions and non-profit agencies is also highlighted in the initiative of health and wellbeing. The AYUSH system of medicine and community-based health facilities would bring harmony with medical pluralism and the emphasis on indigenous practices in the community and preferences.
The NHP 2017 has an inherent strategy for achieving good health and wellbeing by improving India’s healthcare system. It has spelt out the outcomes in termsof numbers, ratios, percentages, years of achievement and specific parameters of health-related states and events. Traditionally, there has been an incursion of central government activities over the country in healthcare’s relevant functional areas since independence (Peters et al., 2003). The NHP is a departure from such practices and more devolution of functions to the state, at least in the document. However, the central government acts as the provider of technical support to many healthcare programmes across the country.
The NHP 2017 provides the states’ scope to run the programmes with their targets within a time frame to execute within their jurisdiction. The national policy is a guideline for providing technical support and international collaborations rather than directing without sufficient fiscal provision. However, the numerical targets set for achievement by the NHP 2017 were found to be low or too slow, like an incremental pace, than other South Asian countries (Sundararaman, 2017). Further, under NHP 2017, the health systems strengthening was given utmost importance for achieving health finance, development of health infrastructure and human resources, and health management information system to support the nation’s entire health system (NHP, 2017).
To discuss some of the salient points of the NHP 2017, there are many tangible targets in terms of ratio, rates and measures. The document sets a target for life expectancy and healthy life, which must be increased from 67.5 in 2017 to 70 years by the year 2025 (NHP, 2017). The reduction of the Total Fertility Rate to the replacement level of 2.1 is an important target enshrined in the policy document (NHP, 2017). There is a tangible target to reduce the disease prevalence/incidence with sufficient provisions in the policy document. Achieving the global target of 2020, which is also the target of 90:90:90, for HIV/AIDS is one of the sole aims (NHP, 2017). The reappearance of TB leads to significant policy prescriptions in the NHP to consider it one of the document’s significant targets. The aim is to achieve and maintain a cure rate of more than 85% in new sputum-positive patients for TB and reduce the incidence of new cases, to reach elimination status by 2025 (NHP, 2017). The importance of health systems strengthening by maximisation of public health services coverage is considered an integral part. One of the focuses is to enhance the utilisation of public health facilities by 50% from the current level in the year 2017 to the target year 2025 (NHP, 2017). NHP 2017 also provide scope for health and wellness centres across country for preventive and promotional care along with Ayushman Bharat Yojna for financial and healthcare protection for marginalised sections of society.
Role of Ayushman Bharat–Pradhan Mantri Jan Arogya Yojana (AB–PMJAY)
The NHP 2017 (NHP-2017) provides sufficient ammunition for UHC by giving a direction for creating a sustainable healthcare infrastructure across India. In the quest for the achievement of UHC the Ayushman Bharat Program needs to scale up every year according to the original plan to cover as many as disadvantaged people possible. The effort by Atal Bihari Bajpayee Prime Ministers Jan Arogya Yojna (AB–PMJAY) to bring proper healthcare to India is well thought of and launched by the union government in 2018. The scheme target to provide coverage up to ` 500,000 to those figures as poorest of poor in the Socio-Economic Caste Census data (National Health Authority, 2018). However, the authors argue that the scheme has less understanding of the exact provision of services (Prinja et al., 2019). The scheme largely depends on experts’ consultation rather than a grassroots-level understanding of the essential public health issues. Further, the health and wellness centers envisioned in the document target to address the curative and promotive aspects of the diseases.
Scholars argue that for the practical and forceful achievement of tangible health outcomes, the Ayushman Bharat programme must be fully implemented with adequate resources (Lahariya, 2018). However, there are simmering challenges in achieving UHC translated into increased access to healthcare, high-quality healthcare services, affordable cost of care and services for all people (WHO, 2010).
The NHP 2017, which aligns with global healthcare aspirations, needs more political stewardship. UHC in India has yet to find much traction in political discourses. Instead, it is evident from a lack of leadership and low funding of resources (Editorial, 2017; GoI, 2017; Health in India, 2017; Shiva Kumar et al., 2011).
Significant challenges to healthcare achievement still exist in the provision of healthcare. To start with health infrastructure and human resources, there needs to be sufficient infrastructure in PHC, CHC, and district hospitals compared to IPHS. The shortage of specialists, general physicians and nurses is a common rule in addition to the lack of sanitation, water and electricity in the healthcare facilities (Central Bureau of Health Intelligence, 2018; MoH & FW, 2017; National Health Profile, 2017; MoH & FW, 2017).
The quality of health services reported by researchers was found to be low, with limited information on the quality of healthcare services in India (Planning Commission of India, 2017). The low quality of services in India is attributed to unqualified health services providers, lack of human resources, absenteeism in service among qualified doctors, and lack of updated skills of qualified doctors (Das et al., 2012; Planning Commission of India, 2017). Against this backdrop, the quality improvement measures like the clinical establishment (registration and regulation) act 2010 still need to be implemented with letter and spirit by many states to improve the quality of health facilities (GoI, 2010). When there is a need to standardise everything in healthcare across globe, the essential quality parameters are found in medical protocols only without being transferred to ground zero in India. Hence, to optimise Ayushman Bharat Yojna, the government must work hard with the highest commitment level.
Role of Technology in the Achievement of Healthcare Over Several Decades
Health technology, over some time, has been changed for the provision of healthcare for the masses. There is also a need to upgrade technology in different parts of India, especially in healthcare. With technology, the government can provide healthcare services effectively. Modern healthcare technology is not just limited to providing care within the hospital; it is found in the entire health system. The responsive health system must adopt those technologies to reduce costs, increase service quality and reach the masses. The health technology assessment is not used widely in India for many years. Of late Department of Health Research, a body of the Indian government helps conduct and commission the health technology assessment based on evidence. The said government body assesses many technologies and advises the health ministry to adopt the technology (Downey et al., 2017).
A concept like value for money has to be in place before adopting any technology. So, the commissioning of health services that include human resources in health, medical services, non-medical sundries and long-term capital investments must be assessed thoroughly for cost-effectiveness. All these things need cost data to evaluate healthcare services’ procurement and disbursement (Prinja et al., 2020). However, evidence found that there needs to be more cost data in the government and private sectors for informed decision-making (Prinja et al., 2018). In health technology assessment, arguments can also factor culture, value, and politics to yield good results. The cultural values and politics influence health technology assessment (HTA), which pose challenges in decision-making, the regulatory framework, data and capacity (Swami & Srivastava, 2020).
A study with recent expenditure data for the years 2014–2017 on five states of India shows a need for uniform spending of resources on primary, secondary, tertiary, social security and medical education to promote health (Gupta et al., 2020). But most states spend a fair amount on developing primary care services. To achieve UHC, there is a need to spend in all the health sector domains. The health system has to be strengthened by upgrading all the curative and public health aspects. To boost the health system, the low-performing states must raise more budgetary resources. The safety net on health is vital and needs a specific approach for marginalised and vulnerable sections.
Sustainable Development Goals (SDG) and Health Sector Targets
The SDGs in 2016 across the globe set 17 goals to be achieved by the world by 2030. Many of the goals, directly or indirectly, can be achieved only if health sector development happens appropriately. Hence, India, a signatory aspiring to achieve its goals and targets, needs to over-emphasise development. The major SDG issues are poverty, hunger, health, education, global warming, gender equality, water, sanitation, energy, urbanisation, environment and social justice. The set goals must ensure meaningful life with wellbeing for all age groups. Further, clean water and sanitation affect the core of the healthcare system. Goals like affordable and clean energy directly relate to health and wellbeing. Sustainable cities and communities play a role in the promotion of healthy behaviours. Climate action is the day’s call to save our citizens’ present and future. In a country like India, zero hunger must be there for good health. These SDGs must be achieved within time to attain good health and a progressive society (WHO, 2019a; WHO, 2019b).
India, of course, delineates these targets with the Millennium Development Goals (MDGs) to achieve good health across the country. The SDGs would help reiterate the importance of human value and health across the spectrum. However, the regional disparity across the country may impede regional health sector achievement from an equity angle. The SDGs are not just a promise but have a strong commitment from the developed countries to improve the situation of the global south. India, hosting one-sixth of the global population, must be successful for global achievement in many parameters. The health sector reforms adopted during the last two decades would be helpful in health sector achievement in the context of SDGs. However, India needs to be vigilant to help both government and private sector to achieve goals without putting pressure on the marginalised population. The objective of SDG’s Leave no One behind has to be materialised in India. The disadvantage in one sector for people will affect their health and further vulnerability. They cannot overcome the vicious cycles of ill health and poverty. SDG3 focuses on the health and development of the overall community, and the Indian government aims to achieve this in the set timelines (WHO, 2019a; WHO, 2019b).
Lessons from the Policy Conundrums in India
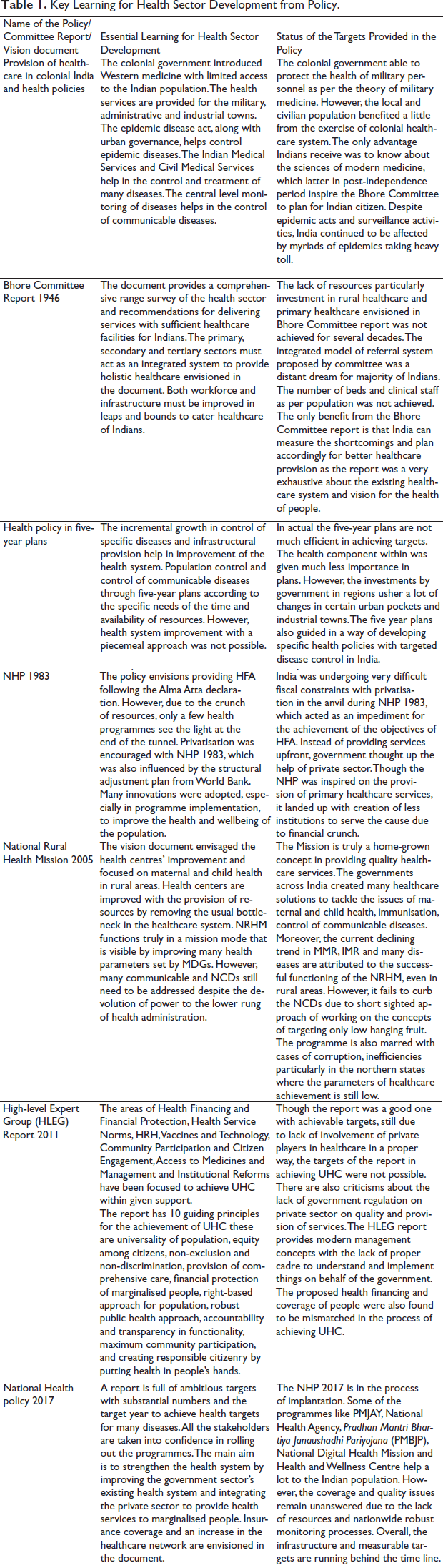
The policies and vision documents help achieve many things over time. The health policies also guide, to a great extent, in terms of programme implementation in a specified period. The well-researched approaches, with due deliberation in the health sector, try to create value in the Indian system. However, many policies could not be implemented fully due to changes in governments, resource crunch, lack of support from stakeholders and a precursor for a conducive health structure. Table 1 shows some of the guiding principles and key learnings of the health policy across time in India.
Key Learning for Health Sector Development from Policy.
Way Forward
The health policies over several decades have had a mixed impact on the health of the population. India, a developing country, has adopted many Western health standards for the benefit of citizens. However, many more things must be adopted to deliver healthcare to include a sizable population.
The healthcare of pre-independence time was very dismal for the public due to the insensitive colonial government, the decimation of the existing Indian system of medicine, and the lack of basic amenities for the public to improve health. However, the silver line was that India got exposure to the modern medical system even many Indian doctors were trained abroad with cutting-edge skills. All of India’s medical services help implant the nucleus for the quest for modern medical knowledge through various reforms.
The Bhore Committee report showed us the mirror of the existing health infrastructure and the vision for independent India. The essential things such as access, equity, primary care and referral system in healthcare for all Indians envisioned in the Bhore Committee, which help the Indian government even today in programme formulation. Though the Bhore Committee report was very old, still, the underlying philosophical concepts of health for the Indian populace can be drawn from it.
The targets of the national health policy in 1983 were ambitious in preventing diseases across the country and ushering in economic development. The failure of a policy can be attributed to a lack of resources despite flawless recommendations in the document. Hence, the creation of infrastructure—hard and soft is much more critical for achieving any goal. Health care’s vertical and horizontal plans need human resources, finance and infrastructure to accomplish any policy’s set target.
National Rural Health Mission 2005 confirms that a homegrown plan can be transformed into reality with proper monitoring and evaluation. The vision document of NRHM 2005 put primacy on the state government’s support in the long run for the maintenance of health infrastructure in the county. NRHM, till today functions on the concepts of devolution of power to the ground-level administrators and the provision of resources from the state and centre.
NHP 2017 would guide India in achieving the health targets mostly aligned with Sustainable Development Goals in the next decades. The targets are again ambitious with health systems strengthening at the centre stage. However, the document needs to promise remarkable progress in establishing a vehicle for delivering healthcare services. The Jan Arogya Yojna and wellness centers have to go a long way ahead to achieve the target of universal healthcare. A strong impetus is required to galvanise India’s entire health structure with investments to the tune of 2.5% of the GDP as envisaged in the policy. Health is a public good that has to be significantly subsidised, which would help indirectly achieve India’s economic goals. Let health and education get financial planners’ attention to unleash the potential of India’s demographic dividends.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Dr. Ranjit Kumar Dehury acknowledges financial support to University of Hyderabad grants of UoH-IoE by MHRD (F11/9/2019-U3(A)). However, the grant authority have no role in designing and conducting of the study.