
Abstract
Background:
The influence of postoperative axial alignment on long-term recurrence and clinical outcome after hallux valgus correction has not been well characterized. Degenerative changes within the metatarsosesamoid and first metatarsophalangeal (MTPJ) joints are common, but their association with long-term function is not well defined. This retrospective study evaluated associations between axial alignment, recurrence, joint degeneration, and long-term outcomes after distal metatarsal reversed-L (ReveL) osteotomy.
Methods:
Seventy-four patients (110 feet) with mild to moderate hallux valgus deformity who underwent ReveL osteotomy between 2004 and 2012 were retrospectively evaluated at a mean follow-up of 14.4 years. Weightbearing radiographs were reviewed preoperatively and at final follow-up. Axial sesamoid radiographs obtained at long-term follow-up assessed sesamoid position, sesamoid rotation angle (SRA), and metatarsal pronation (α angle). First MTPJ and metatarsosesamoid arthritis were graded using a modified Coughlin and Shurnas classification. Clinical outcomes were assessed using Foot and Ankle Outcome Score (FAOS) and visual analog scale. Logistic regression identified predictors of recurrence, arthritis, and functional outcome.
Results:
Hallux valgus recurrence occurred in 11.8% of cases and was associated with residual sesamoid displacement (P < .001) and increased SRA (P < .01), whereas the α angle showed no relationship. In multivariable analysis, SRA greater than 6.2° demonstrated an odds ratio of 6.9 for recurrence, although this association was not statistically significant (P = .07). All axial parameters demonstrated univariate associations with metatarsosesamoid arthritis, but none correlated with MTPJ arthritis. Recurrence (odds ratio [OR] 4.8; P = .03) and SRA greater than 6.2° (OR 3.7; P = .04) independently predicted metatarsosesamoid arthritis. Higher grades of MTPJ arthritis were associated with significantly poorer FAOS scores, whereas metatarsosesamoid arthritis selectively affected the quality-of-life domain.
Conclusion:
First MTPJ arthritis was most strongly associated with long-term pain and function after hallux valgus correction. Postoperative axial malalignment was not statistically significantly associated with recurrence in this cohort. Although hallux valgus recurrence and residual axial malalignment were associated with metatarsosesamoid degeneration, these factors did not adversely affect overall clinical outcomes.
Level of Evidence:
Level IV, case series.
Keywords
Introduction
Hallux valgus is one of the most common forefoot deformities and is frequently associated with pain, functional limitations, and difficulty with footwear, prompting many patients to seek operative correction. Despite advances in operative techniques, postoperative recurrence remains a major concern, with long-term rates reported as high as 73%. 1 Although recurrence is often presumed to correlate with poorer clinical outcomes, this association has not been consistently demonstrated. 2 Numerous procedures have been described for hallux valgus correction, yet none has shown clear superiority in radiographic or functional outcomes. 3 Moreover, long-term outcome data remain limited.2,4,5
Recent studies have highlighted the potential role of first metatarsal pronation in the development and recurrence of hallux valgus. Defined as axial rotation of the first metatarsal, excessive pronation has been associated with incomplete correction and higher recurrence rates. 6 Consequently, derotational techniques have been introduced to address this component of the deformity. 7 The “round sign” introduced by Okuda et al 6 has served as a radiographic marker of metatarsal pronation, although subsequent studies using weightbearing computed tomography (CT) have questioned its reliability. 8 Although weightbearing CT offers more accurate 3-dimensional assessment, it is not yet widely available in routine clinical practice.
Postoperative sesamoid position has likewise been identified as an important determinant of deformity correction and maintenance of alignment. Although several studies have demonstrated that incomplete sesamoid reduction increases the risk of recurrence, others have reported no such relationship.2,9,10
Patients with hallux valgus frequently exhibit degenerative changes within the metatarsosesamoid and metatarsophalangeal joints.1,4,11,12 However, the clinical relevance of these arthritic changes, particularly their impact on long-term pain, function, and satisfaction, remains unclear. 13 Variability in imaging modalities, limited follow-up durations, and heterogeneous study designs likely contribute to these inconsistencies.
This study aimed to evaluate how axial alignment and metatarsosesamoid degeneration affect long-term recurrence and functional outcomes after hallux valgus correction. We hypothesized that long-term postoperative axial malalignment and degenerative changes of the metatarsosesamoid and first metatarsophalangeal joints would be associated with hallux valgus recurrence and inferior patient-reported outcomes. Improving insight into the roles of metatarsal pronation and the metatarsosesamoid complex may help refine operative strategies and enhance long-term results.
Materials and Methods
Study Design and Patient Selection
This investigation represents a focused subanalysis of the larger cohort previously reported by Weigelt et al, 4 which analyzed the long-term clinical and radiographic outcomes following hallux valgus correction with a distal metatarsal reversed-L (ReveL) osteotomy. The procedure represents the standard technique for hallux valgus correction at our clinic and was performed in a consistent, standardized manner as previously described. 4 The original study included 131 feet with a minimum 10-year follow-up. In contrast to that study, which analyzed global radiographic and functional results, the present work specifically examines long-term axial alignment and degenerative changes within the metatarsosesamoid complex.
For the present analysis, only patients with available and analyzable axial radiographs at final follow-up were included. To ensure consistency in imaging, standardized standing sesamoid radiographs were obtained at the final follow-up using a custom-made tangential positioning device similar to that described by Kuwano et al. 14 The device was fabricated as a contoured solid block with a 15° anterior incline and a 30° posterior slope, positioning the metatarsophalangeal joint (MTP) in 45° of dorsiflexion. Axial images were excluded if radiographic quality was insufficient for reliable measurement (n = 3) or axial sesamoid position could not be analyzed because of the absence of the intersesamoid ridge (n = 15), leaving 110 cases for this study. All patients provided written informed consent, and the study protocol was approved by the regional ethics committee (BASEC No. 2021-01192).
Radiographic Evaluation
Standardized weightbearing dorsoplantar radiographs were analyzed preoperatively and at the final follow-up for global alignment parameters, including the hallux valgus angle (HVA) and the intermetatarsal angle (IMA). An HVA threshold of >20° was selected to define hallux valgus recurrence in accordance with commonly used criteria in long-term hallux valgus outcome studies.1,2,4 Intermetatarsal angle measurements were performed using the center-of-metatarsal-head reference technique as described by Smith et al. 15 Given that the reversed-L procedure represents a distal metatarsal osteotomy, head-based reference points were used to reflect the functional position of the first metatarsal after distal translation and rotation, rather than relying on a diaphyseal axis that may be altered by the osteotomy.
Axial radiographs were available only at the final follow-up and were used to evaluate sesamoid position, metatarsosesamoid arthritis, and residual metatarsal pronation. Sesamoid position was classified according to the 4-stage system described by Smith et al, 15 based on the position of the tibial sesamoid relative to the intersesamoid ridge. In this system, grade 0 indicates that the tibial sesamoid is completely medial to the ridge; grade 1, less than half its width lateral to the ridge; grade 2, more than half its width lateral to the ridge; and grade 3, entirely lateral to the ridge. The sesamoid rotation angle (SRA) was measured as described by Kuwano et al. 14 Residual metatarsal pronation was quantified using the α angle, according to Kim et al, 16 with values greater than 15.8° considered pathologic.
Both first MTPJ arthritis on anteroposterior and lateral radiographs and metatarsosesamoid arthritis on axial radiographs were graded according to a modified Coughlin and Shurnas classification. 17 Grade 0 indicated a normal joint; grade 1, osteophyte formation with minimal joint-space narrowing or sclerosis; grade 2, moderate joint space narrowing and sclerosis; grade 3, complete loss of joint space; and grade 4, findings consistent with grade 3 accompanied by pain at midrange of motion. Two blinded observers independently assessed all radiographs, and the mean of the 2 measurements was used for analysis.
Clinical Evaluation
Clinical assessment at the final follow-up included the Foot and Ankle Outcome Score (FAOS) subscales—pain, symptoms, activities of daily living, sport and recreation, and quality of life—each ranging from 0 (worst) to 100 (best). Pain intensity was rated on a visual analog scale (VAS; 0-10).
Statistical Analysis
Statistical analysis was performed using SPSS (version 28.0; IBM Corp). Continuous variables were tested for normality and are presented as mean ± SD or median (IQR). Categorical variables are presented as absolute and relative frequencies. Group comparisons were performed using the χ2 or Fisher exact test for categorical data and the Mann-Whitney U or independent samples t test for continuous data, as appropriate. The Wilcoxon signed-rank test was used to assess changes in radiographic parameters between time points.
Logistic regression analysis identified predictors of recurrence, long-term metatarsosesamoid arthritis, and poor postoperative FAOS-QOL scores. A P value <.1 was used for variable inclusion to reduce the risk of excluding potentially relevant predictors. Radiographic parameters were dichotomized according to established thresholds or ROC-derived cutoffs. Model calibration was evaluated with the Hosmer-Lemeshow test, and statistical significance was defined as P <.05.
Results
The derivation of the study cohort, including inclusion and exclusion criteria, has been reported in detail previously. 4 In the present subanalysis, 110 feet with available and analyzable long-term axial radiographs were included. The final analysis included 74 patients (110 feet) with a mean age of 44.6 years (range, 19-73 years), and a mean follow-up of 14.4 years (range, 10.0-17.8 years).
Radiographic Findings
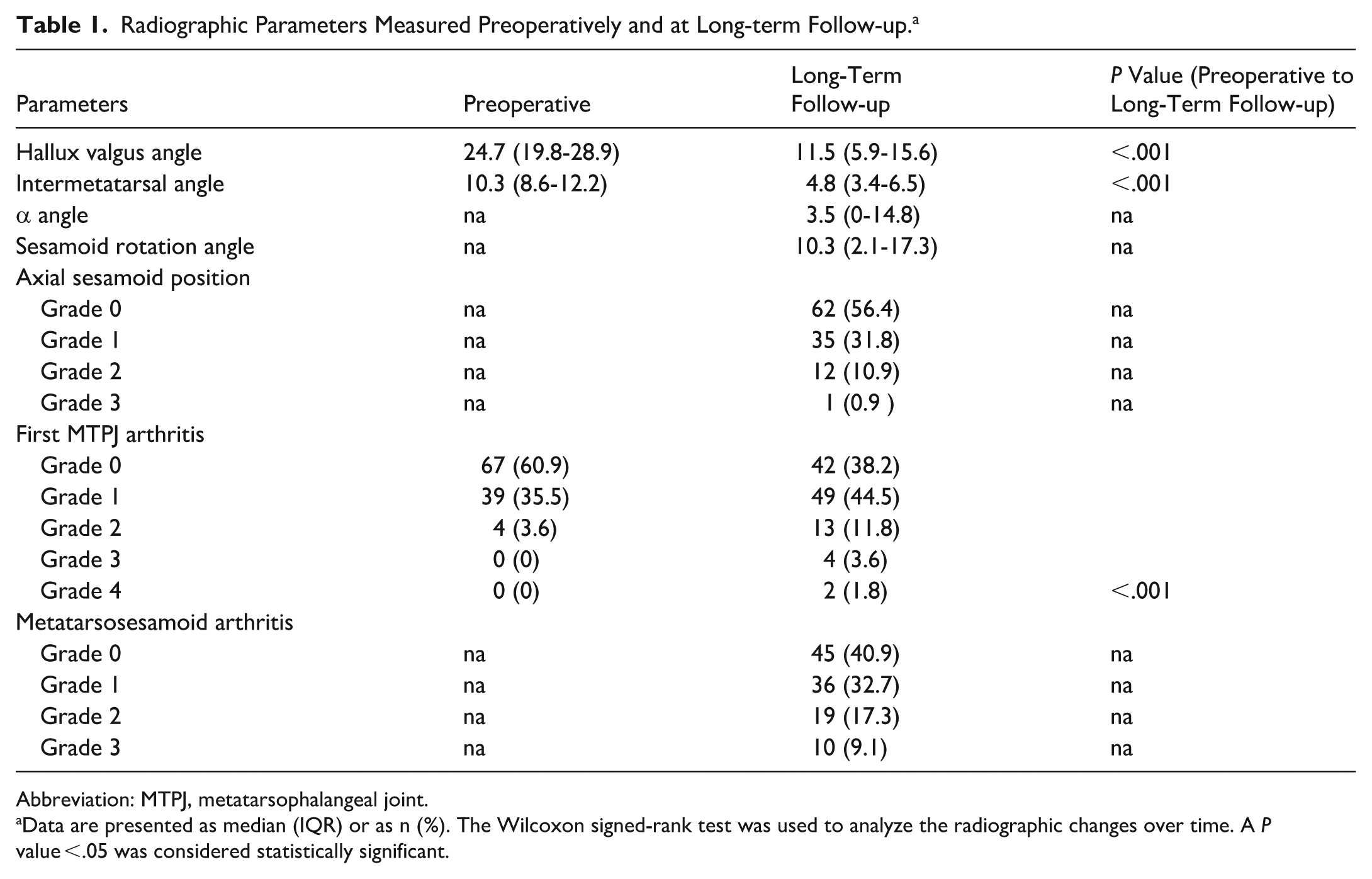
The radiographic parameters are shown in Table 1. The HVA and IMA demonstrated persistent, significant improvement from the preoperative assessment to long-term follow-up. Hallux valgus recurrence was detected in 13 of 110 cases (11.8%).
Radiographic Parameters Measured Preoperatively and at Long-term Follow-up. a
Abbreviation: MTPJ, metatarsophalangeal joint.
Data are presented as median (IQR) or as n (%). The Wilcoxon signed-rank test was used to analyze the radiographic changes over time. A P value <.05 was considered statistically significant.
On axial radiographs, the median α angle was 3.5° (IQR, 0-14.8). Residual metatarsal pronation (α angle greater than 15.8°) was present in 9 cases (8.2%). The median SRA was 10.3° (IQR, 2.1-17.3), with residual sesamoid displacement observed in 48 cases (43.5%). First MTPJ arthritis worsened from a median preoperative grade 0 (IQR, 0-1) to grade 1 (IQR, 0-1) at long-term follow-up. Advanced MTPJ arthritis (grade 2 or higher) was found in 19 cases (17.2%), whereas 29 cases (26.4%) showed metatarsosesamoid arthritis.
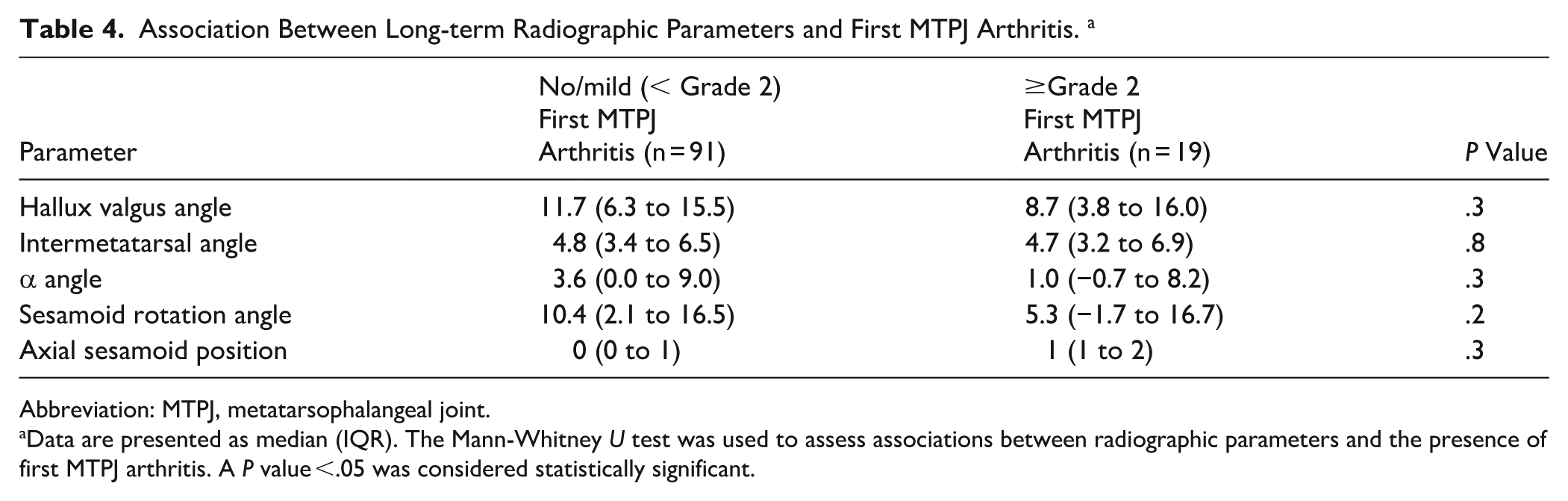
Patients with hallux valgus recurrence demonstrated significantly higher SRA values (P < .01) and greater residual sesamoid displacement (P < .001), whereas the α angle showed no difference (Table 2). All radiographic parameters, including the HVA, IMA, α angle, SRA, and axial sesamoid displacement, were significantly associated with higher grades of metatarsosesamoid arthritis (Table 3) at long-term follow-up (all P < .05), but not with first MTPJ arthritis (Table 4). However, logistic regression only identified an HVA greater than 20° and an SRA greater than 6.2° as independent predictors of metatarsosesamoid arthritis (OR 4.8, P = .03; OR 3.7, P = .04; Table 5).
Association Between Long-Term Radiographic Parameters and Hallux Valgus Recurrence. a
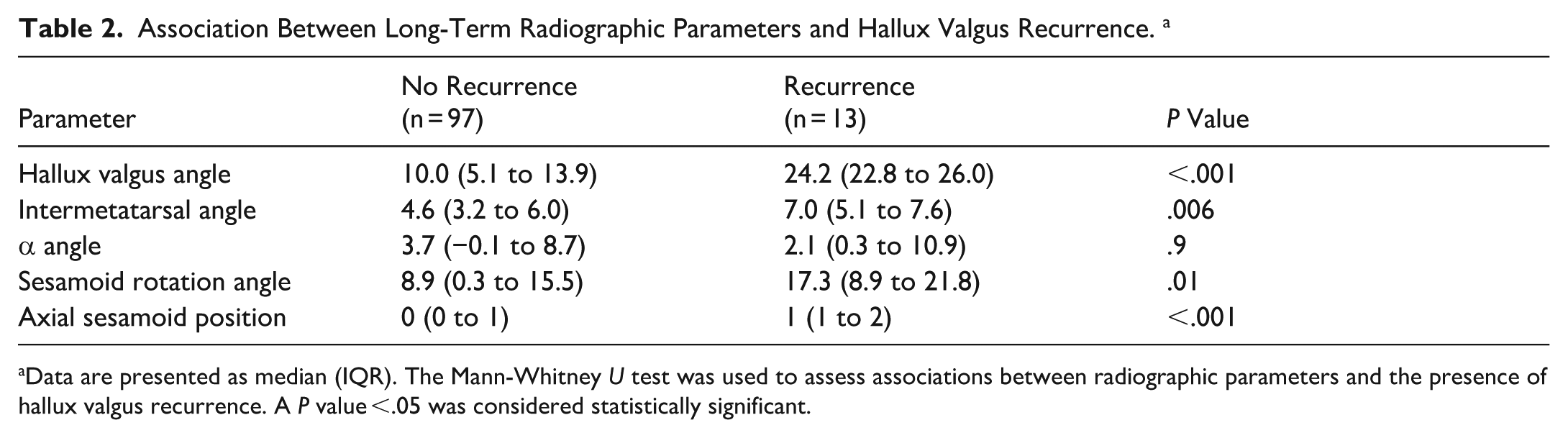
Data are presented as median (IQR). The Mann-Whitney U test was used to assess associations between radiographic parameters and the presence of hallux valgus recurrence. A P value <.05 was considered statistically significant.
Association Between Long-term Radiographic Parameters and Metatarsosesamoid Arthritis. a

Data are presented as median (IQR). The Mann-Whitney U test was used to assess associations between radiographic parameters and the presence of metatarsosesamoid. A P value <.05 was considered statistically significant.
Association Between Long-term Radiographic Parameters and First MTPJ Arthritis. a
Abbreviation: MTPJ, metatarsophalangeal joint.
Data are presented as median (IQR). The Mann-Whitney U test was used to assess associations between radiographic parameters and the presence of first MTPJ arthritis. A P value <.05 was considered statistically significant.
Binary Logistic Regression Analyses Identifying Predictors of Hallux Valgus Recurrence and Long-term Metatarsosesamoid Arthritis. a
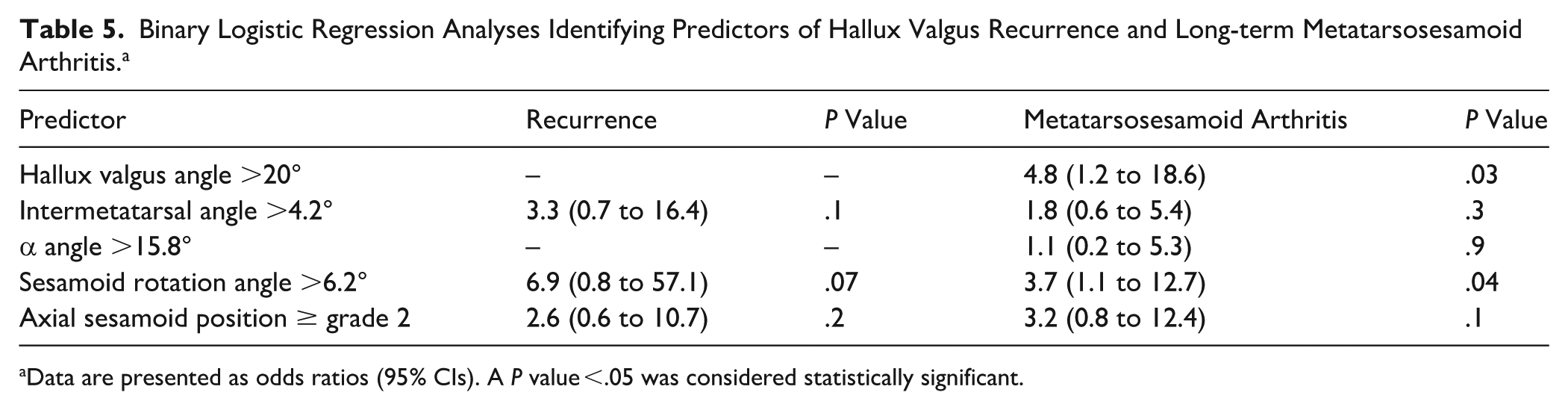
Data are presented as odds ratios (95% CIs). A P value <.05 was considered statistically significant.
Correlation Between Radiographic and Clinical Outcome
Higher MTPJ arthritis grades at the long-term follow-up were associated with significantly poorer results in all FAOS subscales except QOL. Metatarsosesamoid arthritis and elevated BMI were associated with significantly lower FAOS QOL. All FAOS subscales and VAS pain scores are reported across the predefined binary groupings used for univariate analysis to ensure transparent reporting of all tested associations, irrespective of statistical significance (Table 6). In multivariable analysis, only long-term metatarsosesamoid arthritis remained an independent predictor of poor QOL (OR, 2.9; P = .02).
Association of Hallux Valgus Recurrence, Degenerative Changes, and Demographic Factors With Long-Term Clinical Outcomes. a
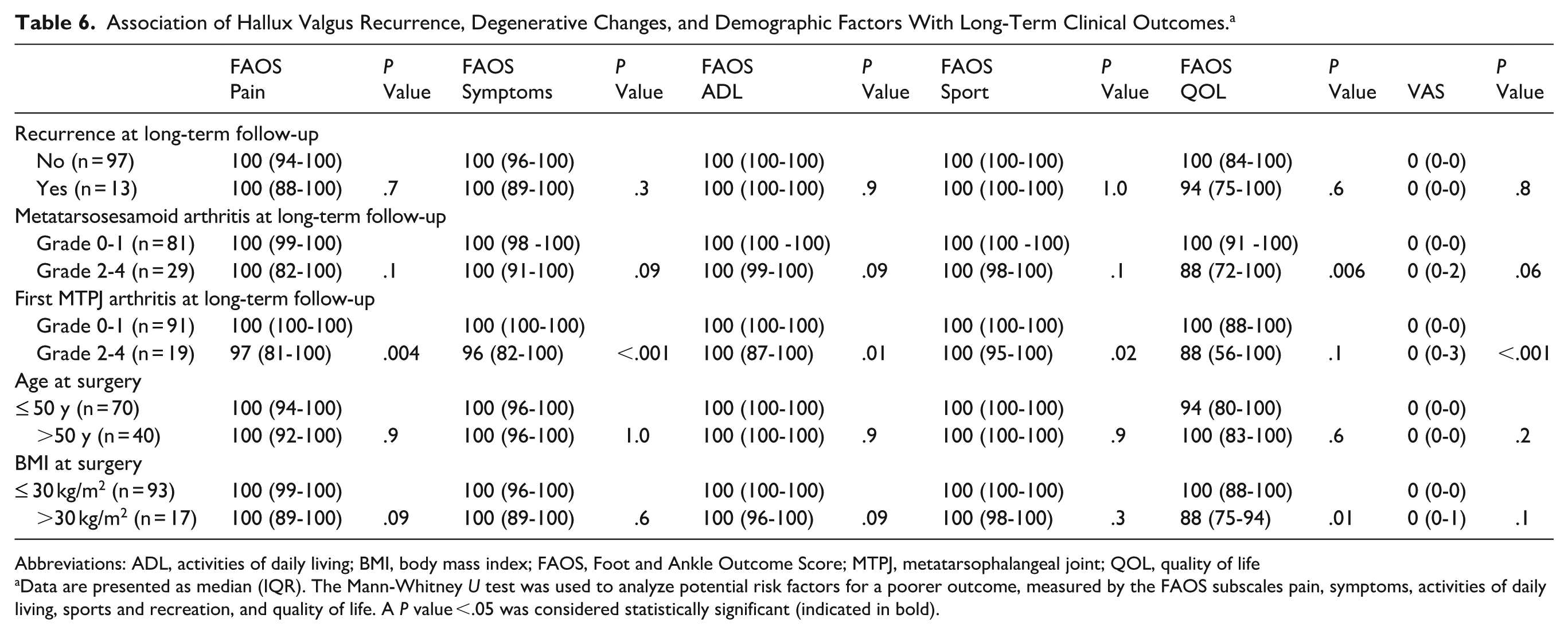
Abbreviations: ADL, activities of daily living; BMI, body mass index; FAOS, Foot and Ankle Outcome Score; MTPJ, metatarsophalangeal joint; QOL, quality of life
Data are presented as median (IQR). The Mann-Whitney U test was used to analyze potential risk factors for a poorer outcome, measured by the FAOS subscales pain, symptoms, activities of daily living, sports and recreation, and quality of life. A P value <.05 was considered statistically significant (indicated in bold).
Discussion
In this long-term retrospective cohort study, we found that first MTPJ arthritis was the primary factor associated with inferior long-term pain and functional outcomes following distal metatarsal reversed-L (ReveL) osteotomy. Although we observed elevated odds of recurrence with increased SRA, this association did not reach statistical significance. Furthermore, the presence of hallux valgus recurrence itself did was not significantly associated with inferior clinical long-term results. These findings suggest that degenerative changes may play a more critical role in long-term patient-reported outcomes after hallux valgus correction than minor residual axial and coronal malalignment.
A considerable proportion of cases demonstrated residual abnormalities on axial imaging, and both axial sesamoid displacement and the SRA were significantly associated with hallux valgus recurrence. These findings are consistent with the short-term results of Okuda et al, 9 who observed that incomplete postoperative sesamoid reduction increased recurrence risk.
In our multivariable analysis, the SRA showed the strongest postoperative association with recurrence, whereas the α angle showed no association, likely reflecting the relatively low degree of residual pronation in this cohort. It remains possible that in cohorts with greater residual pronation this parameter may still contribute to recurrence, although current evidence remains inconclusive. 18 Because preoperative axial measures were not available, the association with SRA cannot determine whether residual malalignment reflects incomplete correction, progression over time, or both.
Only limited data exist on risk factors for developing metatarsosesamoid arthritis. Katsui et al 19 demonstrated that persistent sesamoid displacement on simulated weightbearing CT correlated with progressive degeneration of the metatarsosesamoid joint, and Ono et al 20 reported similar findings in patients with marked metatarsal pronation, even in untreated deformities. In our study, all postoperative axial alignment parameters showed significant univariate associations with metatarsosesamoid arthritis; however, only hallux valgus recurrence and an elevated postoperative SRA remained independent predictors in multivariable analysis, supporting the concept that coronal and axial malalignment each contribute to degenerative changes within the metatarsosesamoid joint. These findings underscore the potential biomechanical relevance of the sesamoid complex in postoperative first-ray stability. Although we did not directly test causal pathways, persistent axial malalignment may plausibly be associated with altered load distribution across the metatarsosesamoid articulation, which could contribute to degenerative changes over time. Given the absence of preoperative axial imaging, it remains unclear whether the observed malalignment reflects incomplete correction, progression, or both.
Metatarsosesamoid arthritis was common at long-term follow-up and showed a significant association with inferior FAOS quality-of-life scores, whereas other FAOS subscales were not consistently affected. This finding suggests that degenerative changes at the metatarsosesamoid articulation may contribute to residual symptoms that are not fully captured by pain or function subscales alone. However, given the absence of preoperative axial imaging and the limitations of radiographic assessment for early degenerative changes, these findings should be interpreted as postoperative associations rather than evidence of progressive degeneration.
In contrast, first metatarsophalangeal joint arthritis demonstrated broader associations with pain and functional outcomes across multiple FAOS subscales and VAS pain scores, underscoring its clinical relevance at long-term follow-up. These findings suggest that postoperative degenerative changes at the first MTPJ appear to be more closely related to long-term symptoms.
In the current study, recurrence had no measurable effect on clinical outcomes. These findings are consistent with those of Bock et al, 2 who reported that recurrence affected FAOS pain but had little impact on broader functional measures. A possible explanation is that even in recurrent cases, defined by a hallux valgus angle exceeding 20°, the intermetatarsal angle generally remained corrected, thereby minimizing medial prominence and preventing recurrence-related bunion pain.
Taken together, these findings suggest that degenerative changes of the first metatarsophalangeal joint are most consistently associated with long-term functional outcomes, whereas residual axial alignment parameters appear to be more closely related to structural and radiographic findings. Further studies using dynamic or 3-dimensional imaging may help clarify the clinical relevance and thresholds of metatarsal pronation and sesamoid displacement.
Our study has several limitations. First, axial radiographs were available only at the final follow-up, preventing evaluation of early postoperative sesamoid position or its temporal changes. Second, only radiographs of sufficient quality with identifiable crista morphology were included, potentially introducing selection bias. Third, axial radiography provides a static, 2-dimensional assessment of the metatarsosesamoid joint, whereas weightbearing CT offers a more comprehensive 3-dimensional evaluation of rotational alignment. Kim et al 16 emphasized that more than one-quarter of apparent sesamoid displacements on anteroposterior radiographs reflect “pseudo-subluxation,” highlighting the limitations of conventional radiographs for assessing axial plane deformity. By employing standardized axial radiographs obtained with a tangential positioning device, we aimed to achieve reproducible and accurate evaluation of sesamoid alignment. Although Yildirim et al 21 demonstrated that hallux dorsiflexion may reduce the apparent degree of sesamoid subluxation, Soares et al 22 found that α-angle measurements from Bernard’s axial projection correspond more closely with anatomic findings from cadaveric dissection than those derived from CT scans. However, radiographic evaluation of metatarsosesamoid arthritis remains a 2-dimensional assessment and may lack sensitivity for early degenerative changes compared with weight-bearing CT. Within these constraints, the present study provides the first long-term assessment integrating postoperative metatarsal pronation, sesamoid alignment, and degenerative changes of both the metatarsosesamoid and first metatarsophalangeal joints after hallux valgus correction. Finally, the limited number of recurrence events may reduce the stability of multivariable estimates and warrants cautious interpretation, particularly for exploratory regression modeling involving multiple correlated axial parameters.
Conclusion
First MTPJ arthritis was the factor most strongly associated with long-term pain and functional limitation after hallux valgus correction, outweighing the influence of hallux valgus recurrence, residual axial malalignment, or metatarsosesamoid degeneration. Although recurrence and axial malalignment, particularly increased sesamoid rotation, were independently associated with the development of metatarsosesamoid arthritis, these radiographic changes did not translate into overall inferior patient-reported outcomes. These findings highlight the importance of achieving both coronal and axial alignment during hallux valgus correction while recognizing that degenerative changes within the first MTPJ remain the principal driver of long-term clinical results. However, these findings should be interpreted in light of the absence of preoperative axial imaging and the retrospective study design.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261427473 – Supplemental material for Long-term Associations Impact of Axial Alignment, Sesamoid Position, and Joint Degeneration and Recurrence and Clinical Outcomes After Hallux Valgus Correction
Supplemental material, sj-pdf-1-fao-10.1177_24730114261427473 for Long-term Associations Impact of Axial Alignment, Sesamoid Position, and Joint Degeneration and Recurrence and Clinical Outcomes After Hallux Valgus Correction by Lizzy Weigelt, Noah Davolio, Carlos Torrez, Florian Haug, Nathalie Kühne and Stephan H. Wirth in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the Cantonal Ethics Committee of Zurich (BASEC No. 2021-01192).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.