
Abstract

Keywords
Introduction
Osseous tuberculosis is an uncommon form of extrapulmonary tuberculosis. Mycobacterium tuberculosis spreads via inhalation and, following pulmonary infection, may disseminate hematogenously or through the lymphatic system to the skeleton. 1 Diagnosis is often delayed because of its indolent course, and infection may remain latent. 1 Skeletal tuberculosis of the foot is rare, with only isolated reports describing individual tarsal bone involvement. Extrapulmonary tuberculosis accounts for 10% of all tuberculosis cases, 0.1% to 0.3% of which are seen in the foot and ankle.2,3
To our knowledge, tuberculosis involving the medial tarsometatarsal joints managed surgically with retained internal fixation has not been reported. We present a 31-year-old man initially diagnosed with sarcoidosis who underwent arthrodesis of the first through third tarsometatarsal joints and the naviculocuneiform joint using plates, cannulated screws, and structural osteoconductive synthetic bone graft substitute, with intraoperative specimens confirming midfoot tuberculosis.
Case Report
A 31-year-old man born in India who immigrated to the United States in his 20s presented with progressive right midfoot pain over 1 year. He reported a remote twisting injury but developed symptoms months later. Conservative management, including prednisone, physical therapy, casting, and immobilization, failed. Physical examination revealed a tender dorsal midfoot prominence with crepitus at the second tarsometatarsal joint. Radiographs were unremarkable (Figure 1); computed tomography (CT) revealed severe lytic, moth-eaten changes and magnetic resonance imaging demonstrated bone marrow edema across the tarsometatarsal joints (Figures 2, 3).
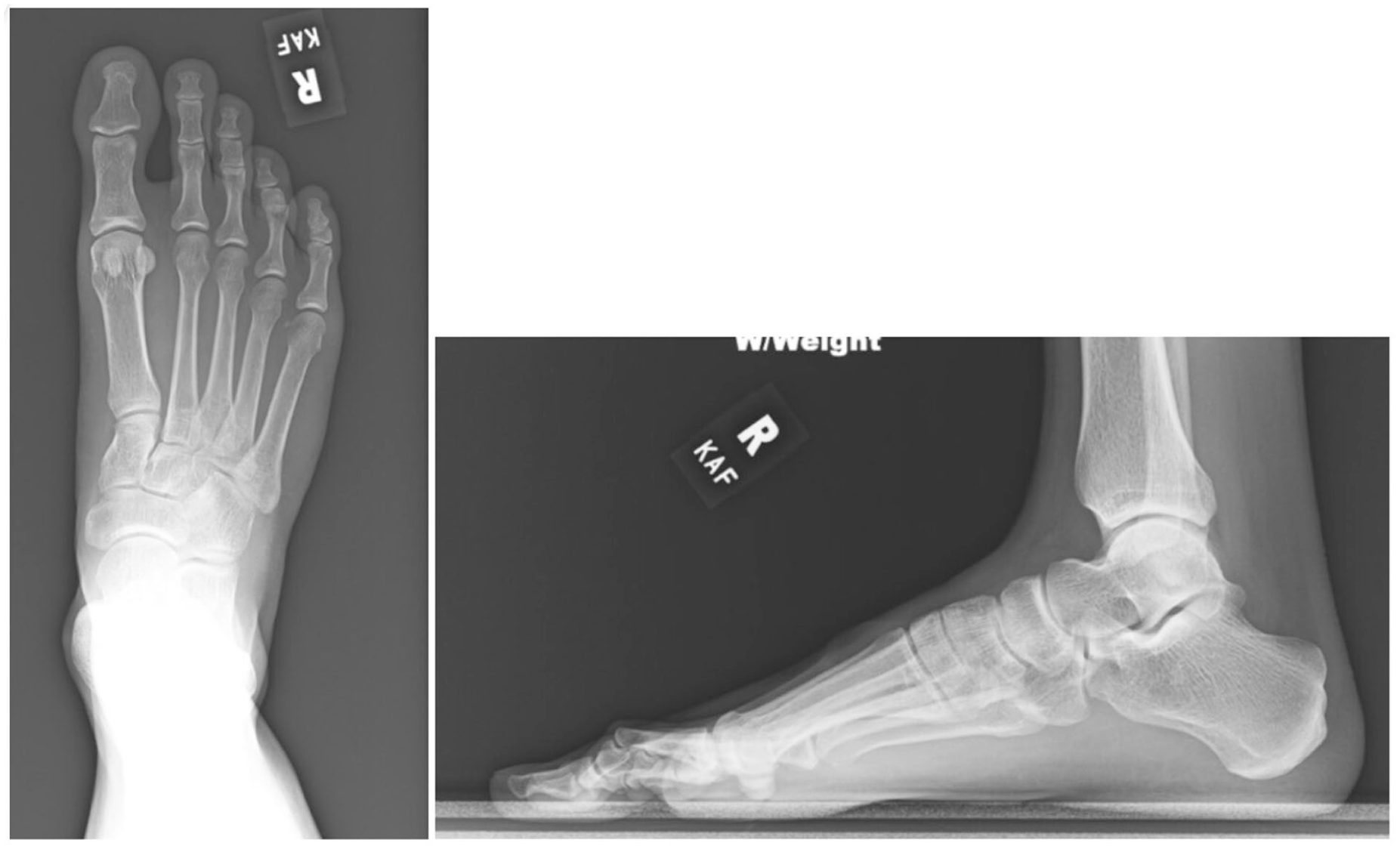
AP and lateral foot radiograph at the time of patient presentation and symptom onset. No overt lytic or degenerative changes noted to the tarsometatarsal joint complex. AP, anteroposterior.

Coronal and sagittal T2-weighted magnetic resonance imaging showing bone marrow edema to the second and third tarsometatarsal joint.

Coronal and sagittal computed tomography illustrating severe lytic changes with moth-eaten osseous appearance to the tarsometatarsal joint complex.
Laboratory evaluation, including complete blood count, erythrocyte sedimentation rate, C-reactive protein (CRP), human leukocyte antigen B27 (HLA-B27), rheumatoid factor, Lyme serology, and uric acid, was unremarkable except for mildly elevated CRP. Fluoroscopic-guided biopsy of the second metatarsal showed noncaseating granulomatous inflammation; cultures for bacteria, fungi, and acid-fast bacilli were negative (Figure 4). Orthopaedic oncology and rheumatology consultations were obtained. Additional testing revealed pulmonary nodules on chest CT, elevated ACE, and a negative interferon-gamma release assay. The patient was diagnosed with sarcoidosis and started on methotrexate and leucovorin.

Fluoroscopic-guided biopsy of second metatarsal base on AP fluoroscopic image. AP, anteroposterior.
Despite therapy, pain progressed, lytic destruction worsened, and a new dorsolateral cyst developed. Radiographs demonstrated further tarsometatarsal and naviculocuneiform joint destruction (Figure 5). Arthrodesis was performed for presumed sarcoid arthropathy, including first through third tarsometatarsal joints and naviculocuneiform fusion due to intermediate cuneiform involvement and its importance as a keystone of the midfoot (Figure 6). A 2 × 2 × 2-cm defect at the second tarsometatarsal joint was filled with a structural osteoconductive synthetic bone graft substitute to restore stability and promote osseous integration for fusion. Abyryx calcium phosphate bone putty with vitamin E acetate was a nonfrozen product selected for its moldability, rapid setting, structural support, and complete resorption during bone remodeling.

AP, medial oblique, and lateral foot radiograph 1.5 years after initial patient presentation showing progressive lysis to the tarsometatarsal joint and naviculocuneiform joints with worsening degenerative changes. AP, anteroposterior.
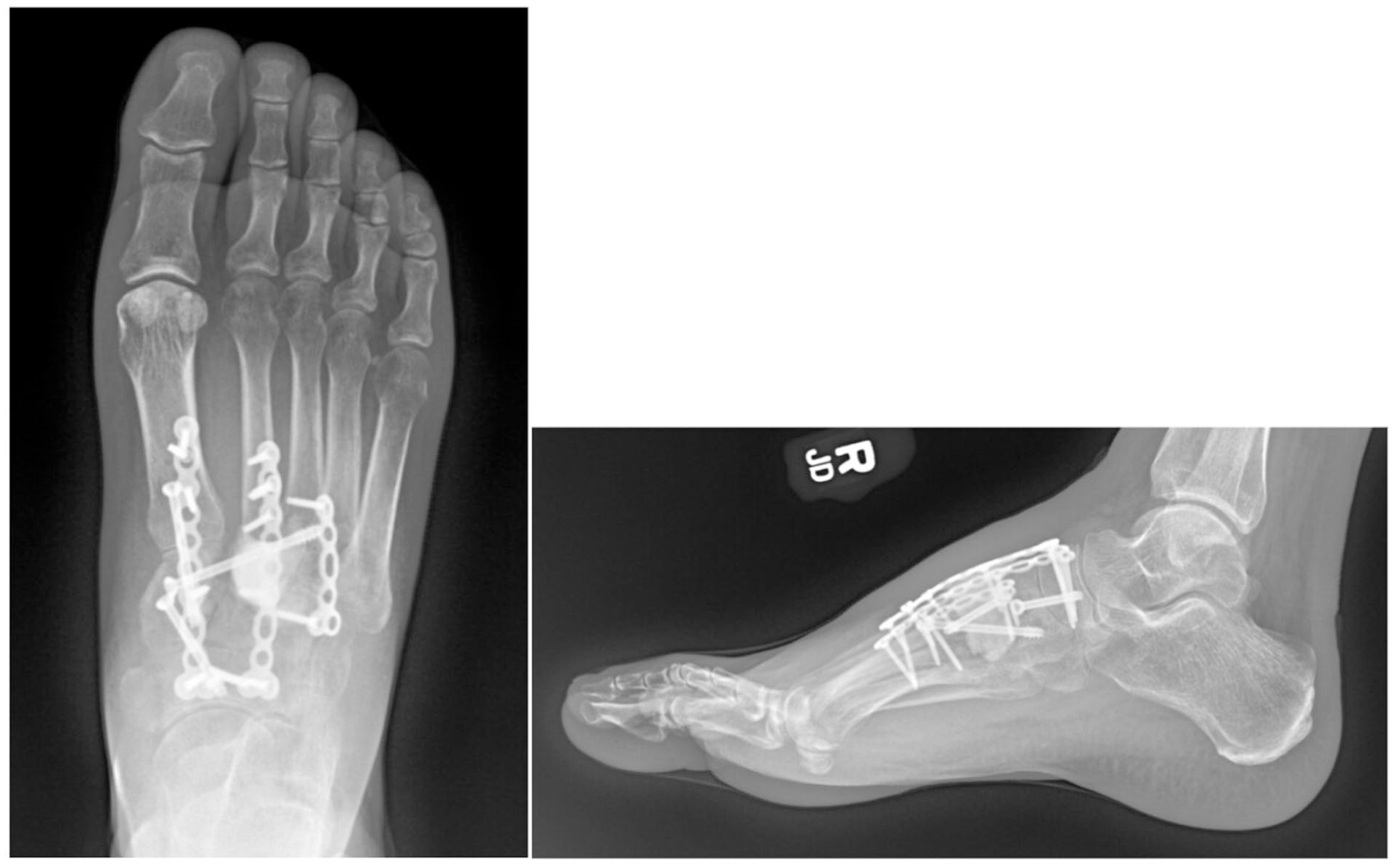
Postoperative AP and lateral radiographs 1 month status post first, second, and third tarsometatarsal joint and naviculocuneiform joint arthrodesis. Synthetic bone graft substitute was used to fill the void at the second tarsometatarsal joint. AP, anteroposterior.
Frozen section ruled out malignancy. Specimens from the second metatarsal base, periarticular tissue, and lateral midfoot mass were sent for microbiologic and histopathologic analysis. Fixation was performed in a single stage with plates and cannulated screws, as infection was not suspected preoperatively. Histopathology showed focally necrotizing granulomatous inflammation, and both bone and soft tissue cultures grew M tuberculosis despite negative initial smears. Postoperatively, sputum cultures confirmed pulmonary tuberculosis; HIV testing was negative. The patient received 4-drug antitubercular therapy for 4 months, followed by rifampin and isoniazid for 8 months because of retained hardware. Methotrexate and leucovorin were discontinued.
Postoperative rehabilitation included 3 weeks nonweightbearing, then protected weightbearing in a CAM boot. By 4 months, he ambulated in regular footwear, and pain improved substantially by 6 months. Radiographs demonstrated progressive fusion without new lysis. At 11 months, he had completed therapy and remained asymptomatic. Follow-up at 14 and 21 months confirmed continued stability and intact hardware (Figure 7). Although hardware removal may be needed in the future, the patient remains pain-free and functionally stable nearly 2 years after surgery.
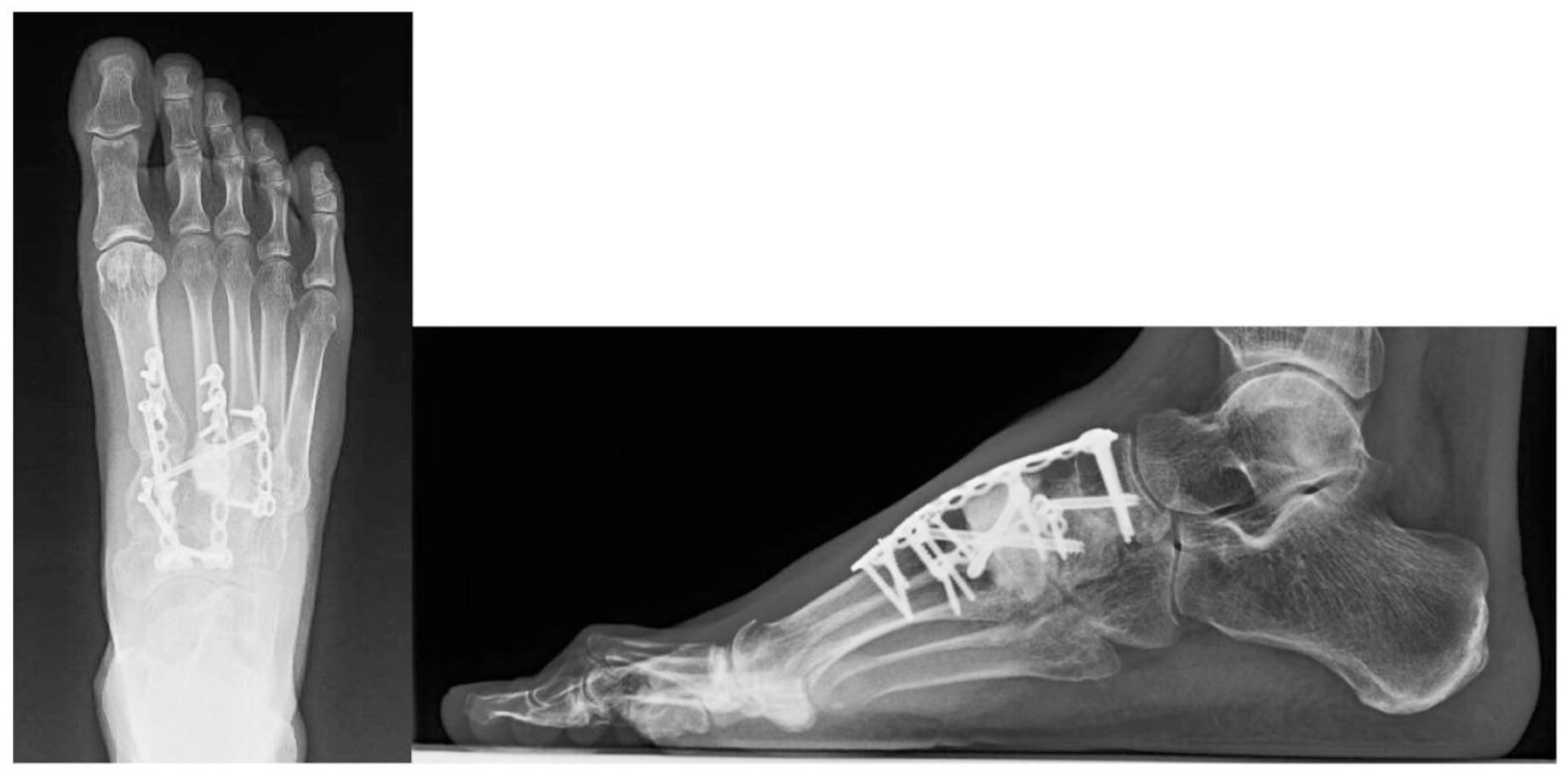
Postoperative AP and lateral radiographs 14 months from surgery, showing progressive bony fusion across first through third tarsometatarsal joints and naviculocuneiform joint with hardware intact. AP, anteroposterior.
Discussion
Skeletal tuberculosis represents roughly 10% of extrapulmonary cases. 4 In the United States, most cases occur in foreign-born individuals, particularly from India, Mexico, Vietnam, and China; 71.5% of cases in 2020 were in this population. 5 Reactivation of latent infection is the most common mechanism. 5
Hematogenous spread from pulmonary disease likely caused midfoot involvement in this patient. The case highlights the diagnostic challenge of skeletal tuberculosis, as imaging and biopsy initially mimicked sarcoidosis and interferon-gamma testing was negative. Our decision to proceed with single-staged arthrodesis was supported by the presumed preoperative diagnosis. Definitive diagnosis required open surgical sampling. Infectious Diseases Society of American (IDSA), American Thoracic Society (ATS), and Centers for Disease Control (CDC) guidelines recommend 6-9 months of rifampin-based therapy for osteoarticular tuberculosis, often extended to 12 months when hardware is retained. 6
Prior reports describe staged procedures, external fixation, and bone grafting for midfoot tuberculosis.7 -9 Compton et al 9 reported a 65-year-old man from India with distal tibia, talus, and calcaneus osteomyelitis treated with debridement; cultures later grew M tuberculosis. Our case differs in that a single-stage arthrodesis with retained fixation was performed before diagnosis, followed by prolonged antimicrobial therapy, achieving stable fusion and favorable short- to midterm outcomes.
A key consideration is the risk of late hardware complications and disease recurrence, necessitating long-term follow-up. Tuberculosis can reactivate even after therapy, and retained hardware may serve as a nidus for infection or biofilm formation. 3 Extended clinical and radiographic surveillance is recommended, and patients should be counseled regarding potential future hardware removal. 3
This case underscores the importance of maintaining a high index of suspicion for tuberculosis in patients with granulomatous musculoskeletal disease and relevant epidemiologic risk factors. Single-stage arthrodesis with structural synthetic bone graft substitute and internal fixation, combined with appropriate antimicrobial therapy, can provide pain relief, preserve midfoot stability, and achieve fusion even when diagnosis is uncertain. We recognize the limitations inherent to a single case report and its ability to inform a formal treatment algorithm in these difficult cases.
Conclusion
Osseous tuberculosis of the midfoot is challenging to diagnose, especially when clinical, imaging, and histologic findings mimic sarcoidosis and initial microbiologic studies are negative. Intraoperative specimen analysis was critical to definitive diagnosis. Single-stage arthrodesis with retained internal fixation and structural synthetic bone graft substitute, followed by prolonged antitubercular therapy was associated with pain relief, midfoot stability, and successful osseous fusion. Clinicians should maintain suspicion for tuberculosis in at-risk patients; in cases of refractory destructive midfoot pathology with inconclusive preoperative workup, surgical sampling may provide definitive diagnosis and allow concurrent stabilization.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261445963 – Supplemental material for Midfoot Skeletal Tuberculosis Managed With Single-Stage Tarsometatarsal and Naviculocuneiform Arthrodesis and Antitubercular Therapy
Supplemental material, sj-pdf-1-fao-10.1177_24730114261445963 for Midfoot Skeletal Tuberculosis Managed With Single-Stage Tarsometatarsal and Naviculocuneiform Arthrodesis and Antitubercular Therapy by Julia C. Tolin, Christine Jones, Akshay Jain, Jeffrey Manway and Ricardo Arbulu in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Data Availability Statement
All data underlying the results are available as part of the article and no additional source data are required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.