
Abstract
Background:
Surgical repair of the Achilles tendon (AT) requires high failure load while limiting elongation. Midsubstance repairs are particularly reliant on suture techniques and typically use either a whip stitch or a locking stitch, such as the Krackow. Enhancements to the Krackow, such as the gift box, epitendinous, or alternative locking stitch techniques, aim to simplify surgical processes and improve biomechanics. The purpose of this study was to evaluate biomechanical properties of 3 enhanced techniques for midsubstance AT repair. We hypothesized that locking stitch constructs would demonstrate improved biomechanical performance compared with nonlocking constructs by minimizing elongation and increasing failure load.
Methods:
A total of 30 cadaveric lower leg specimens with simulated midsubstance AT ruptures were divided into 3 repair groups: whip stitch with gift box (WG), locking whip stitch with gift box (LG), Krackow stitch with epitendinous baseball (KB) stitch. Samples were preconditioned and then loaded from 20 to 100 N for 1000 cycles, followed by load to failure. Elongation, stiffness, failure load, survival, failure mode, and suture weight (burden) were compared.
Results:
KB had the significantly lowest cyclic elongation, whereas LG had the significantly highest failure load. LG failure load increase was achieved while using less suture material than KB. All samples survived the cyclic loading protocol, and all whip stitch groups failed from tissue pull-through, whereas LG and KB failed only 40% from pull-through.
Conclusion:
This study presents 2 stitch techniques that can improve AT repair failure load (LG) and limit elongation (KB). Locking stitch techniques LG and KB demonstrated a significant improvement in biomechanical performance compared with nonlocking WG. Inferences should be limited to the 3 tested constructs rather than individual technical variables in isolation.
Clinical Relevance:
The locking whip stitch gift box and Krackow epitendinous baseball stitch techniques are both viable methods for Achilles tendon repair. Nonlocking whip stitch gift box does not provide sufficient fixation.
This is a visual representation of the abstract.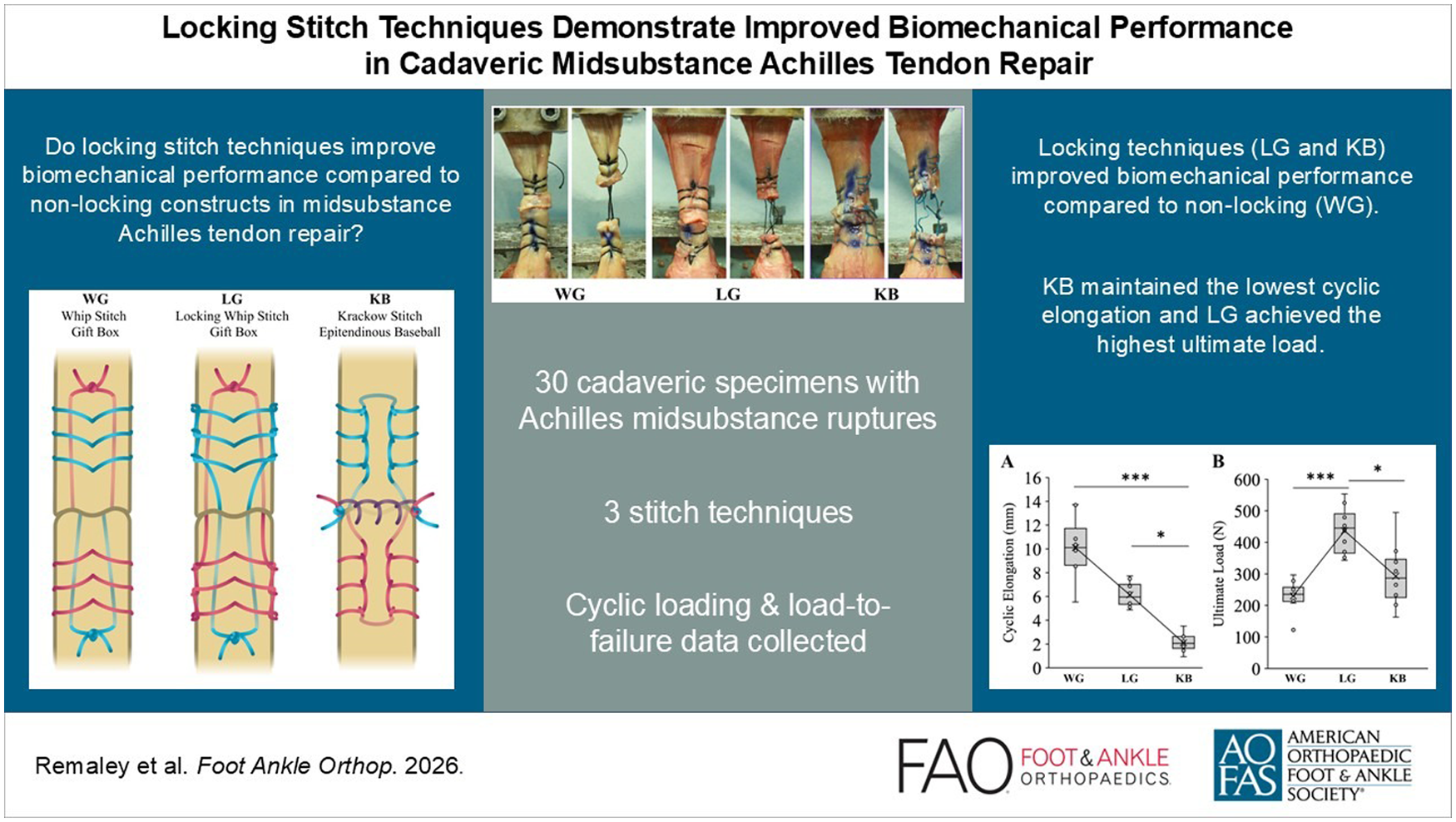
Introduction
The Achilles tendon (AT) is the strongest and thickest tendon in the human body, yet its exposure to high mechanical loads combined with limited vascularity makes it the most frequently ruptured tendon in the lower leg.1 -4 Relative to nonoperative care, surgical repair has been shown to lower rerupture risk; as such, surgical repair is typically a preferred method of treatment for highly active patients with few comorbidities.5,6 Midsubstance ruptures that are 4 to 7 cm proximal to the insertion lie in the watershed region and are particularly challenging because of poor blood supply. 1 These midsubstance repairs rely entirely on suture technique to achieve suture-tendon purchase for approximation and repair. A successful repair must limit gap formation and postoperative elongation to less than 10 mm and withstand physiologic loads of 300 N experienced during early rehabilitation.2,7 -10
In all-suture repairs, locking stitch configurations such as the Krackow are widely used over simpler Bunnell, baseball, or whip stitch techniques. These simple techniques offer speed from fewer needle holes, but they lack a locking element, raising concerns about suture pull-through under load in midsubstance repairs.11,12 The Krackow has been shown to withstand high loads, resist elongation, and fail from suture rupture rather than tissue pull-through.12 -14
Enhancements to the Krackow stitch have been developed to simplify surgical technique and improve repair strength. An epitendinous stitch helps limit elongation but requires additional suture material and more needle passes.11,13,15 A locking whip stitch enabled by a 2-part needle decreases the number of needle holes compared to a traditional Krackow (Figure 1) while still creating a locking suture mechanism more resistant to pull-through. 16 The “gift box” technique passes the suture tails back through the core of the opposing AT stump to move the knots away from the repair site, thus increasing failure load. 8 There are limited comparative evaluations of these advanced AT repair techniques in midsubstance repairs, particularly with respect to time-zero performance.17 -19
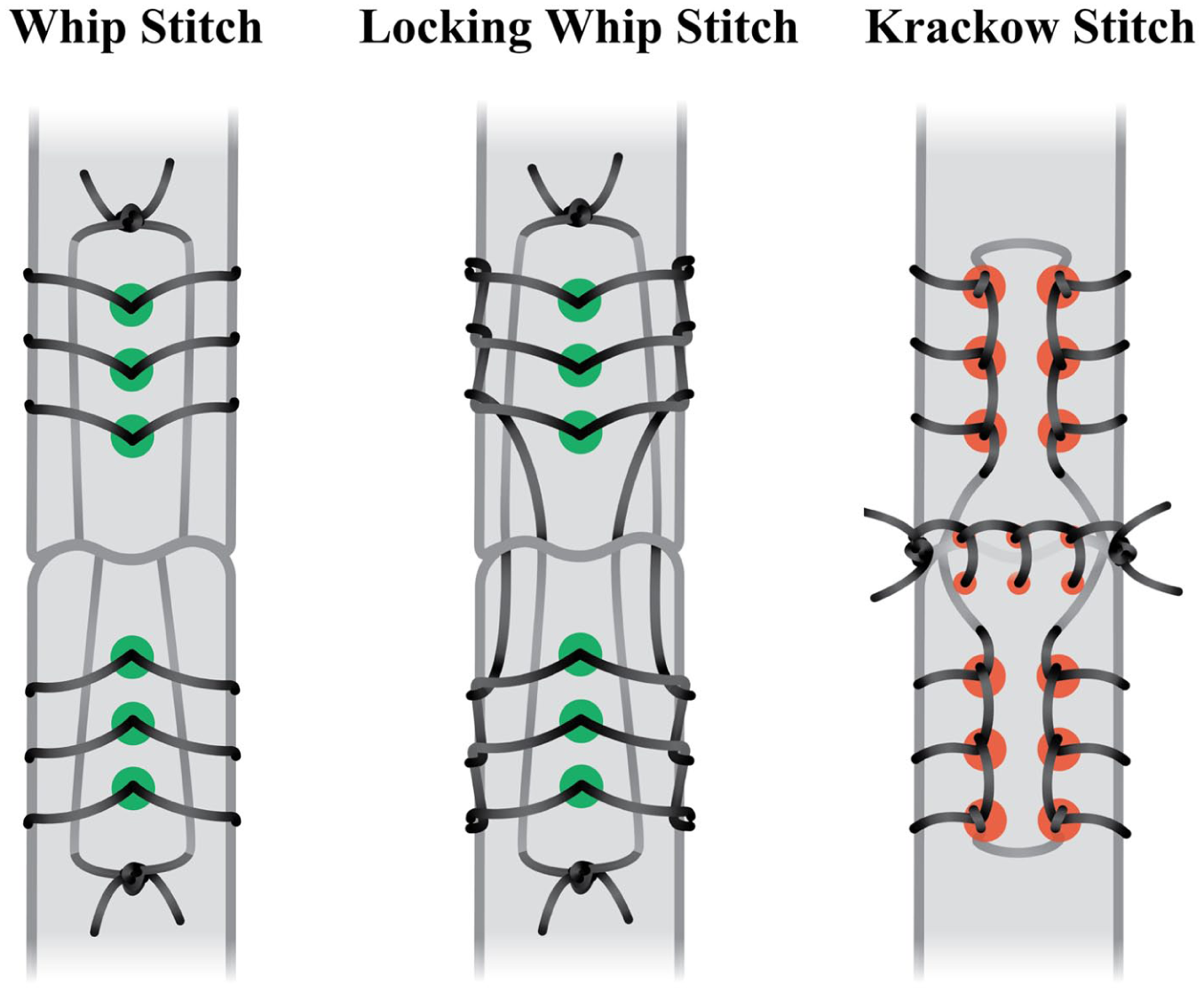
Comparison of needle holes required for whip stitch, locking whip stitch, and Krackow stitch techniques.
Although minimally invasive techniques have gained popularity, both open and minimally invasive repairs remain widely used, with comparable outcomes. Open repair continues to play a key role in complex or chronic presentations given its facilitation of direct visualization and tendon mobilization, and a broadly accessible and cost-effective surgical option. 20 We hypothesized that locking stitch constructs would demonstrate improved biomechanical performance compared with nonlocking constructs by minimizing elongation and increasing failure load.
Methods
Tissue preparation, simulated AT repair, sample harvesting, and biomechanical testing were performed at the Foundation for Orthopaedic Research and Education (FORE; Tampa, FL).
Group Design
A total of 30 fresh frozen human cadaveric mid-tibia to toe tip specimens were obtained and stored at –20 °C. Prior to instrumentation, dissection, and testing, specimens were thawed at room temperature for 24 hours. Before instrumentation, all specimens were visually evaluated for the presence of tears or other abnormalities. Specimens were randomized into 3 test groups (10 samples per group). The 3 groups were selected to represent clinically relevant, prespecified repair constructs rather than analysis of each technical variable.
Groups included (1) Whip stitch with gift box, (2) Locking whip stitch with gift box, and (3) Krackow stitch with epitendinous Baseball stitch (Figure 2).
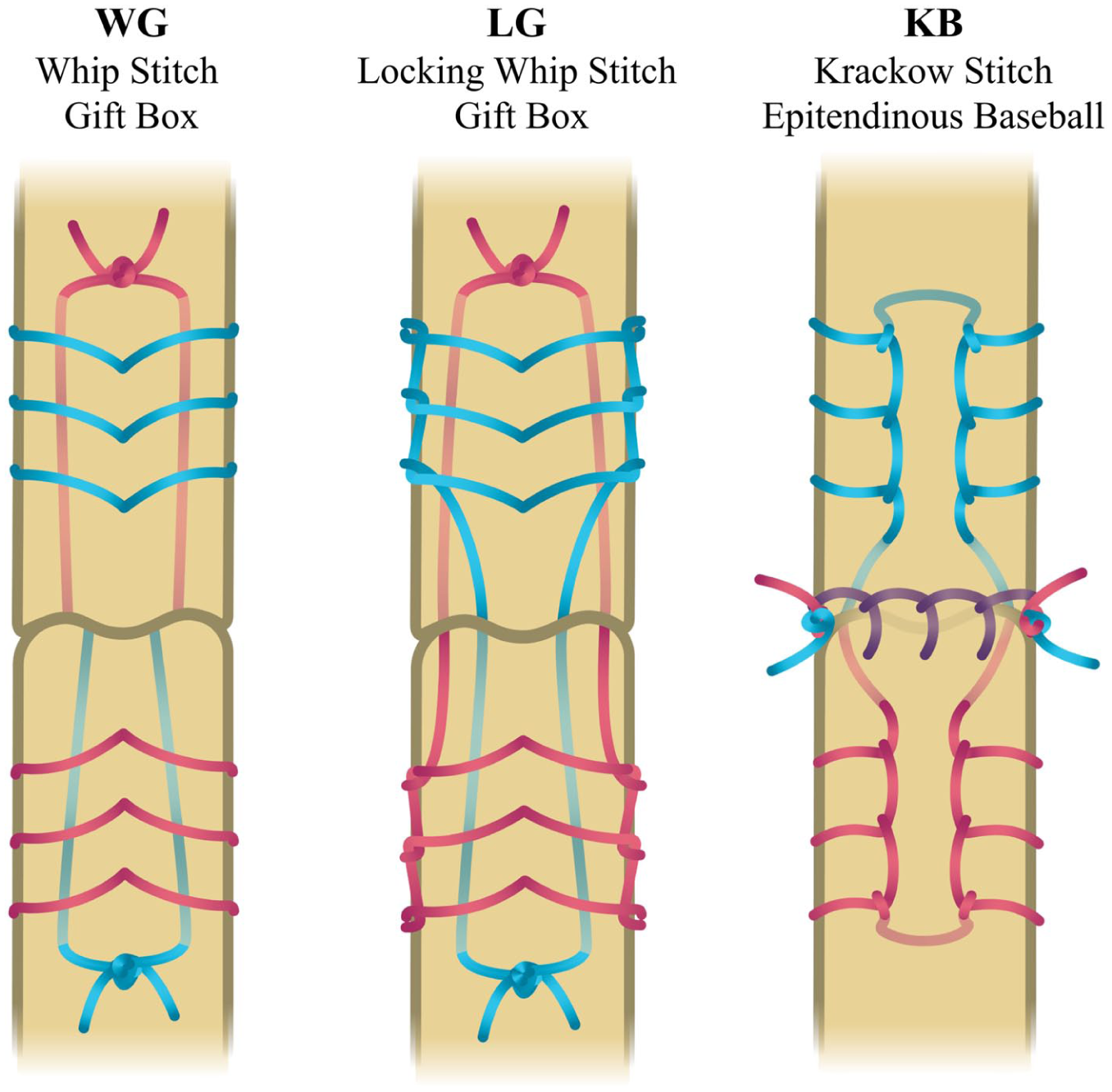
Test group illustrations and descriptions.
The first 2 groups used a 2-part needle with size 2 nonabsorbable braided suture (EasyWhip; Winter Innovations) to perform a whip stitch gift box (WG) or a locking whip stitch gift box (LG). One needle was used to secure 3 of the designated stitches on the proximal stump, and then a second needle was used to secure 3 stitches on the distal stump. The needle was then used to shuttle each of the suture tails across the rupture site and through the core of the proximal stump, emerging on the superficial surface of the tendon proximal to the furthest stitch. The same process was repeated to pass the suture tails through the core of the distal stump.
The result was that 4 suture strands were passed across the rupture site. The suture tails were then tensioned and tied away from the rupture site with 4 knots.
The third group used a curved needle with size 2 braided polyethylene/polyester composite suture (FiberWire; Arthrex) to perform the conventional Krackow with epitendinous baseball (KB). One needle was used to secure 3 Krackow stitches up and then 3 back down on the proximal stump, and a second needle was used to do the same on the distal stump. The opposing suture tails were tensioned and tied at the repair site with 4 knots. A third needle with the same size 2 suture was used to create an epitendinous running baseball stitch, which was finished by tying 4 knots.
All repairs employed size 2, nonabsorbable braided sutures. Size 2 indicates caliber and strength standards, and products from both manufacturers are rated to approximately 75 lb (330 N) breaking strength.
Specimen Preparation
Instrumentation consisted of simulated AT ruptures and repair procedures, which were conducted by a board-certified orthopaedic surgeon with support from residents. A surgical blade was used to make a longitudinal posterior incision exposing the AT. A midsubstance rupture was then simulated by cutting the AT with the blade 4 cm above the calcaneus insertion. A repair was performed by completing the designated technique. On each stump, 3 stitches were placed 0.5 cm apart, beginning 1 cm from the end of simulated rupture (Figure 3).
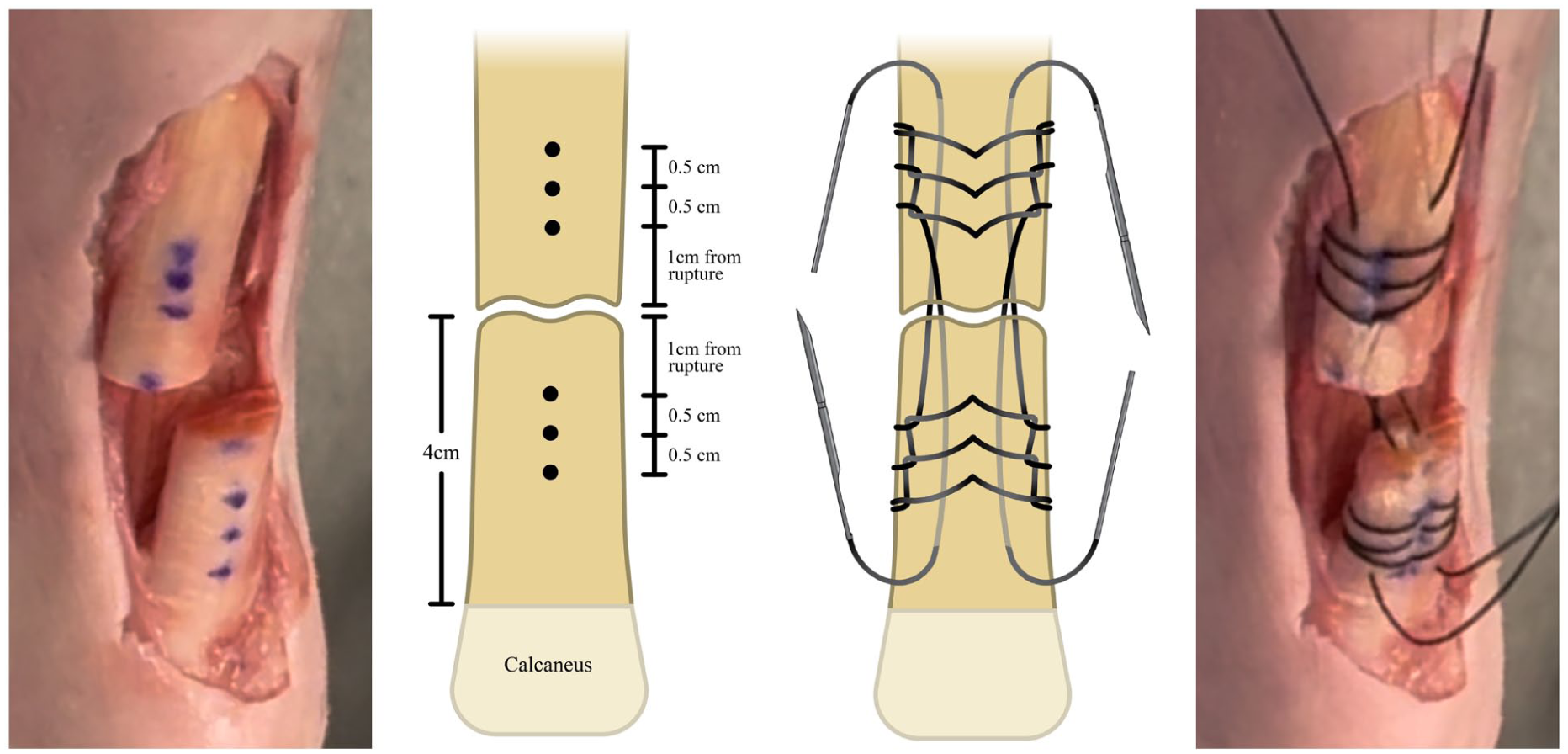
Example of specimen preparation and stitching.
Dissection was then performed to isolate the combined AT and calcaneus. The tendon was released proximally, and the muscle belly of the gastrocnemius sharply debulked to permit adequate fixation of the cryoclamp on the proximal tendon. Soft tissues surrounding the calcaneus were removed and the calcaneus was isolated prior to potting. Tendon dimensions were measured with a digital caliper after dissection. Length was recorded as the tendons’ longitudinal axis over the isolated test segment, width was measured in the mediolateral plane, and thickness in the anteroposterior plane, both at the midsubstance.
The calcaneus was potted using high-strength resin (Bondo; 3M) and then secured with a threaded bolt to the testing fixture in a neutral position to simulate standing. The direction and line of action of the AT was in line with direction of tensile force. The proximal end of the AT was then passed through a cryoclamp cooled by dry ice to a temperature of –5 °C, continuously monitored by a digital temperature probe (Figure 4).
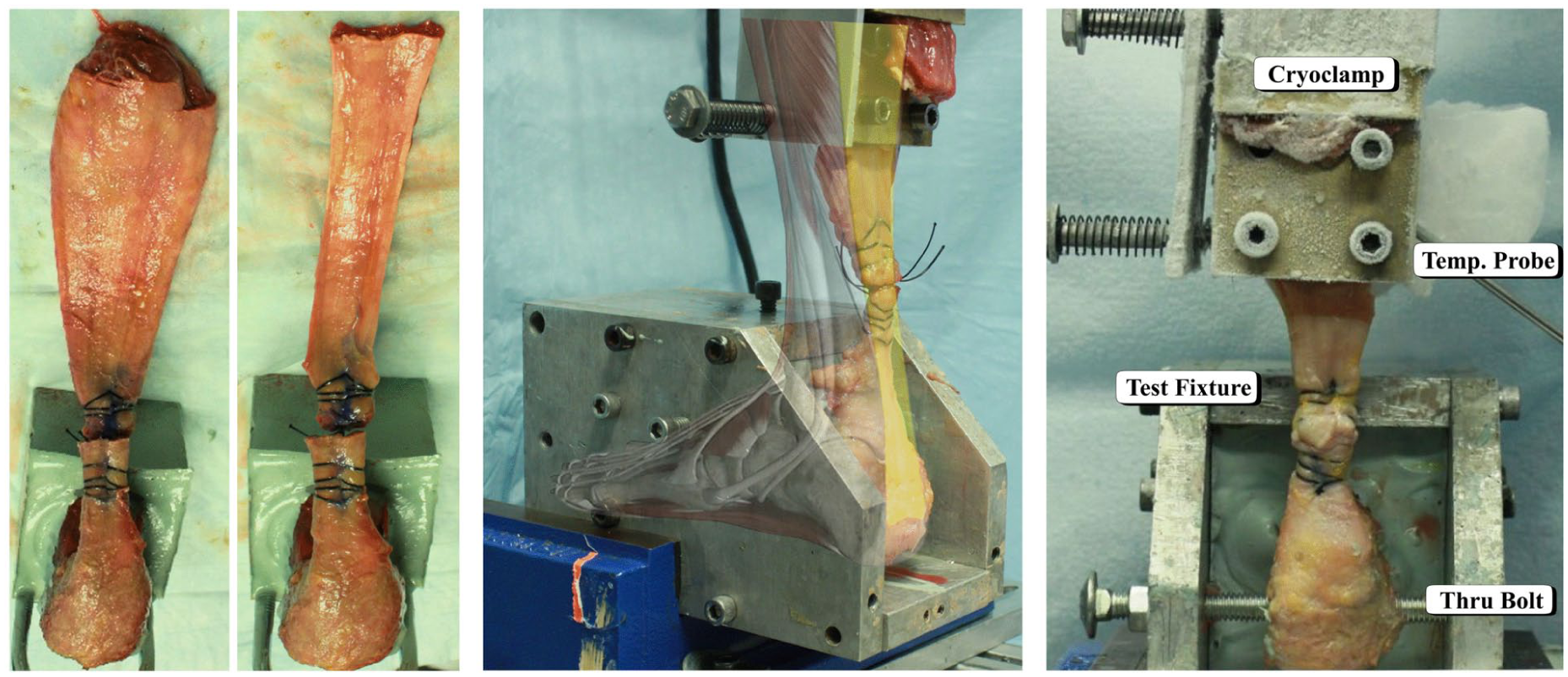
Illustration of specimen dissection, debulking, and biomechanical test setup using fixtures and cryoclamp.
Biomechanical Testing
Biomechanical evaluation was established using previously published protocols.7,16,17,21 -23 All specimens followed a standardized testing protocol consisting of 3 discrete phases: preconditioning, cyclic loading, and load-to-failure testing. Testing was performed on a servohydraulic testing machine (MTS Bionix; MTS Systems) equipped with a 5-kN loading cell.
All samples underwent a preconditioning phase of cyclic loading from 20 to 100 N for 10 cycles at 0.5 Hz. Thereafter, each specimen was subjected to constant-amplitude cyclic loading under force control at a frequency of 1 Hz for 1000 cycles. The force bounds were set between 20 N (valley load) and 100 N (peak load). Peak-to-peak elongation (mm) was defined as the average of the maximum and minimum displacements across the last 3 cycles, providing an estimate of steady-state elongation. Cyclic elongation (mm) was defined as the difference in displacement between the first and last cycle peaks (including preconditioning), as measured by crosshead displacement. Survival was recorded as a binary outcome denoting whether the construct completed all 1000 cycles. Based on previous benchmarks, failure was defined by elongation greater than 10 mm or failing at loads below 300 N.2,7 -10
After cyclic loading, the samples underwent a monotonic ramp-to-failure at 25.4 mm/s. Stiffness (N/mm) was calculated as the slope of the linear portion of the load-to-displacement curve (Figure 5). The failure load (N) was defined as the peak load sustained at the onset of failure.
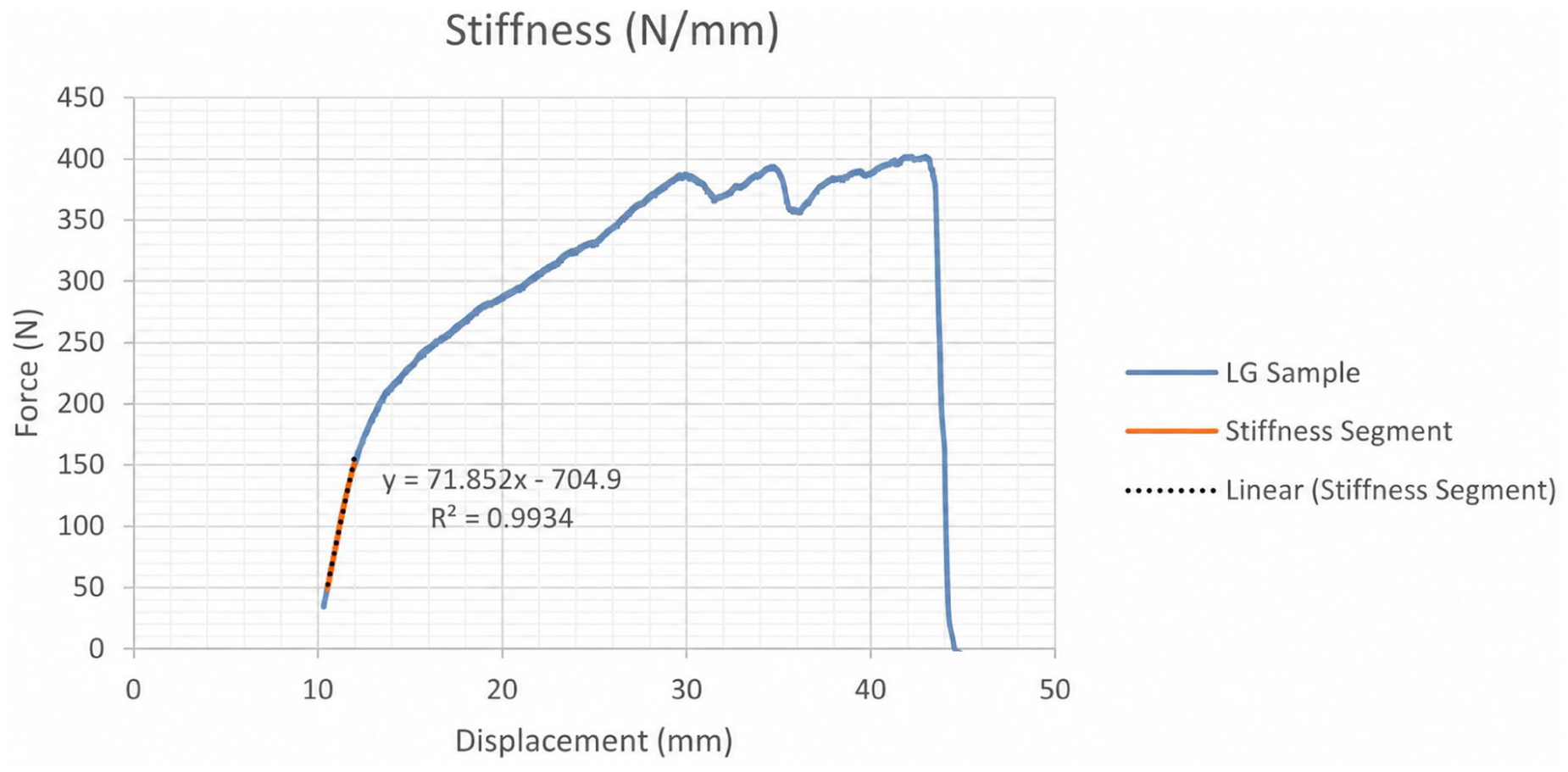
Example using a locking whip stitch gift box LG sample illustrating the computation of stiffness (N/mm).
Failure modes were categorized into 3 conditions: (1) tissue-related failures described samples that failed by suture pull-through in a cheese-wiring effect through the tendon; (2) suture-related failures described samples that failed as a result of the knot slipping or the suture breaking; (3) combined failures described samples that had a significant amount of pull-through followed by suture break.
Suture Weight (Burden) Testing
After testing was completed, the suture used for each repair was removed from the tissue and weighed as a measure of suture material burden. The weight (g) of each repair was recorded and averaged across each group.
Statistical Analysis
Using mean and variance data from prior studies of similar scope,7,17,21 -23 a large effect size (f = 0.8) was used for an a priori power analysis (G*Power 3.1). Assuming normal distribution, a 1-way analysis of variance design, with a significance threshold of .05, powered the study at the 0.86 level with a total sample size of 21 (7 samples per group). Using 10 samples per group allows for any possible tissue rejection, or unforeseen failures while retaining approximate study power.
The Shapiro-Wilk tests for normality were performed on the data set and found to significantly deviate from normality. Therefore, nonparametric statistical analysis was performed. The Kruskal-Wallis analysis with Bonferroni correction was also used to analyze the biomechanical parameters measured for 3 suture configurations. The parameters included peak-to-peak displacement, cyclic elongation, stiffness, and failure load. The prespecified primary outcome was failure load. Cyclic elongation, stiffness, survival, failure mode, and suture weight were prespecified secondary outcomes. Data are presented as median and IQR.
Results
Donor Demographics
The average age of cadaveric donors was 72 years (range: 49-87 years; 8 male and 12 female). No statistical differences for age, height, weight, or BMI between groups were found.
No statistical differences were found between the length, width, and thickness of AT specimens. The average and SD for length was 29.8 ± 5.5 mm, for width was 16 ± 3.5 mm, and for thickness was 6.9 ± 1.9 mm.
All mechanical data are summarized in Table 1.
Data Summary of Results. a
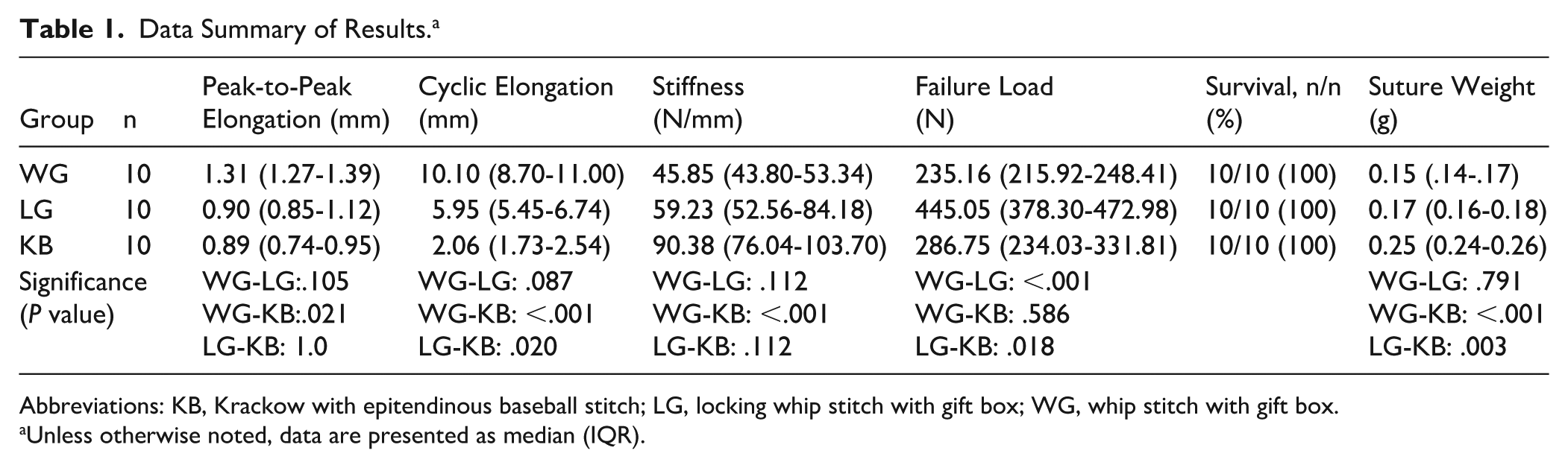
Abbreviations: KB, Krackow with epitendinous baseball stitch; LG, locking whip stitch with gift box; WG, whip stitch with gift box.
Unless otherwise noted, data are presented as median (IQR).
Cyclic Loading
KB (0.89 mm) achieved the lowest peak-to-peak elongation, which was significantly lower than WG (1.31 mm, P = .021), but not significant when compared to LG (0.90 mm, P = 1.0).
For cyclic elongation, WG (10.10 mm, P < .001) and LG (5.95 mm, P = .020) both demonstrated significantly higher elongation compared with KB (2.06 mm) (Figure 6A).
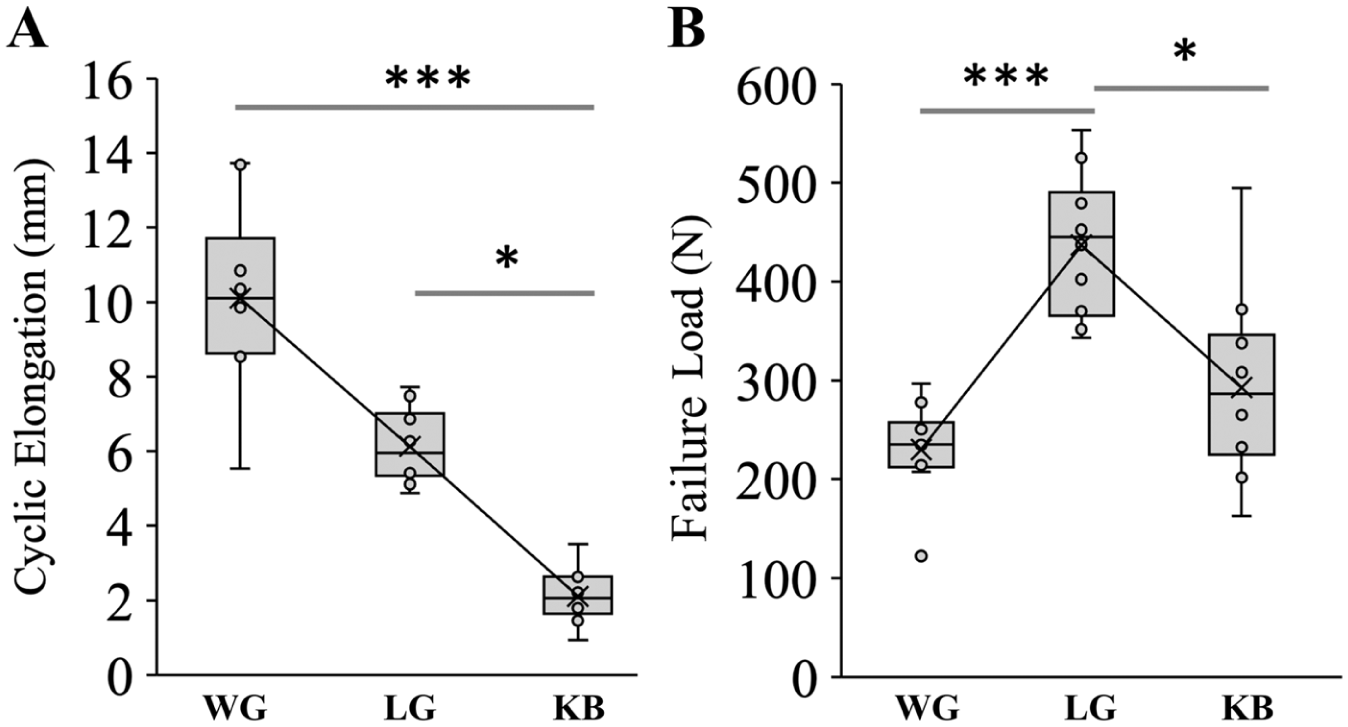
Box plots of (A) cyclic elongation (in millimeters; mm) and (B) failure load (in newtons; N). KB, Krackow with epitendinous baseball stitch; LG, locking whip stitch with gift box; WG, whip stitch with gift box.
Stiffness and Load-to-Failure
Both locking techniques demonstrated higher stiffness compared to the standard whip stitch technique. KB (90.38 N/mm) demonstrated significantly higher stiffness compared to WG (45.85 N/mm; P < .001). LG (59.23 N/mm) did not differ significantly from either group.
LG (445.05 N) achieved the highest failure load and was significantly greater than both WG (235.16 N, P < .001) and KB (286.75 N, P = .018) (Figure 6B).
Failure Mode
All samples in WG failed by tissue pull-through, whereas the LG was split 40/60 between tissue pull-through and combined failures, and the KB was split 40/60 between tissue and suture failures (Table 2). Representative images of failures from each group are shown in Figure 7.
Summary of Failure Mode Data.

Abbreviations: KB, Krackow with epitendinous baseball stitch; LG, locking whip stitch with gift box; WG, whip stitch with gift box.
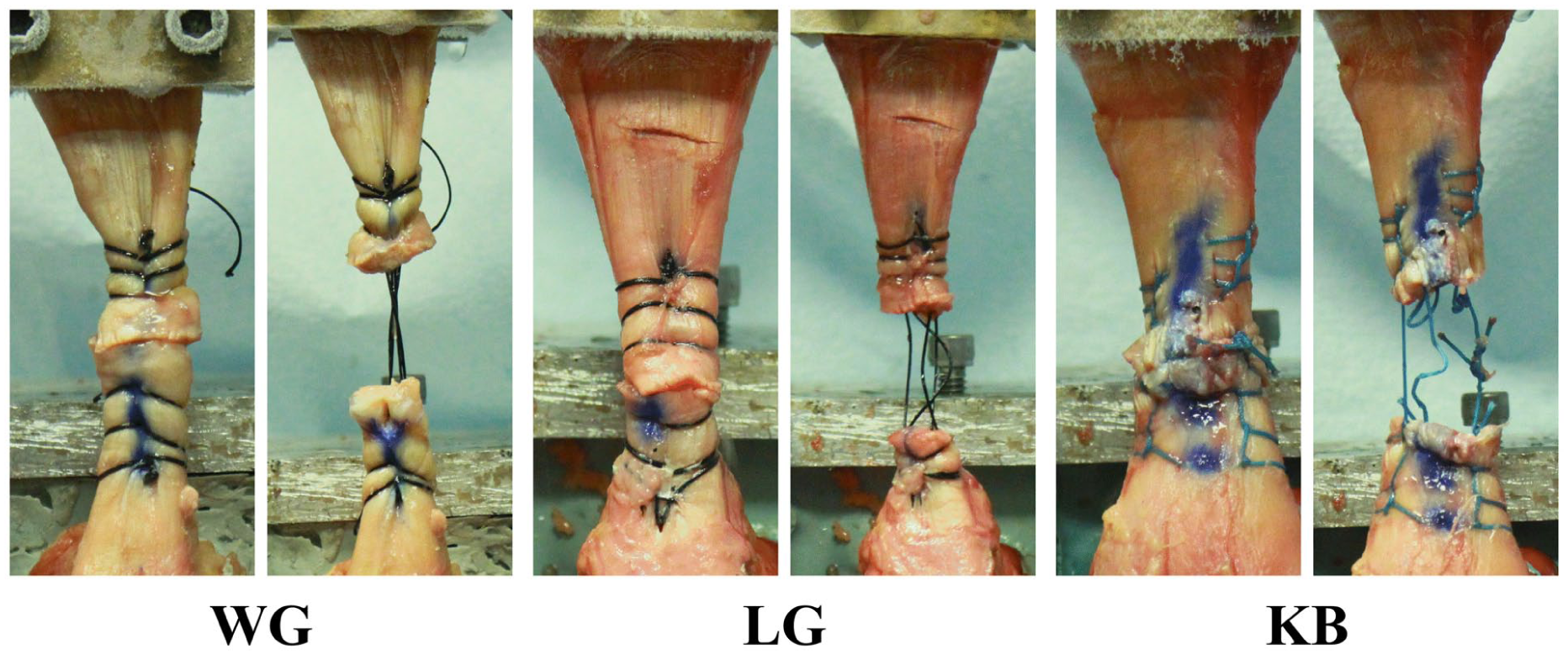
Representative images of failure mode for each group. KB, Krackow with epitendinous baseball stitch; LG, locking whip stitch with gift box; WG, whip stitch with gift box.
Suture Weight
KB (0.25 ± 0.018 g) had the highest suture weight, followed by LG (0.17 ± 0.020 g) and then WG (0.16 ± 0.021 g). Pairwise comparisons showed a significantly greater suture weight for KB compared with both WG (P < .001) and LG (P = .003).
Discussion
The primary outcome of this investigation revealed that the locking stitch techniques LG and KB demonstrated a significant improvement in overall biomechanical performance compared with the nonlocking WG method. The LG achieved significantly higher loads surpassing the minimum benchmark failure threshold of 300 N. Although the failure load for KB fell below the 300 N threshold, it did achieve significantly lower elongation. Both the KB and LG maintained cyclic displacements below the maximum failure threshold of 10 mm. Importantly, this 10-mm threshold should be interpreted as a biomechanical testing benchmark derived from prior literature rather than a clinical threshold that directly defines revision risk. The clinical relevance of gapping vs failure load is central to postoperative management. Excessive elongation beyond 10 mm compromises push-off and functional recovery.7,9 Constructs that resist excessive displacement, such as KB, may better preserve tendon length and justify cautious early motion. It should be noted that in this model, cyclic elongation represents the direct measure of gap formation under loading conditions, whereas failure load reflects the reserve strength of the construct after cyclic loading. In contrast, higher failure load, as seen with LG, may protect against unexpected overload during rehabilitation or premature weight bearing.13,17 The WG underperformed across all biomechanical metrics tested. Specifically, it demonstrated the lowest stiffness, the greatest elongation, and the poorest failure load capacity. These outcomes reinforce previous literature that locking stitch configurations are preferred for high load-bearing tendon repairs.12,18,24 -26
The weakness of these simplified nonlocking stitch techniques for midsubstance AT repairs is related to the fact that fixation depends solely on suture-tendon purchase and quality of the tissue. Nonlocking whip stitches are popular because they reduce needle passes and save time, but biomechanically they concentrate applied tensile force along the central axis of the tendon, which can result in increased elongation and tissue pull-through, termed “cheese-wiring” in previous literature.14,16 The WG test group was established to investigate whether adding a gift box augment to a nonlocking stitch could enhance biomechanical performance and reduce pull-through. Given the results in this study, that was not the case.
Labib et al 8 first described the gift box in 2009, and it has since become a widely trusted technique to improve biomechanical performance of midsubstance AT repairs. This technique moves the knots away from the tendon junction to limit elongation and adds sutures through the core of the tendon to increase failure load. They compared the Krackow alone to Krackow with a gift box and found that the Krackow gift box more than doubled failure load over a Krackow alone (168 N vs 81 N). Direct comparison of these values to the present study is limited by differences in failure definitions, as Labib et al reported load at 1 cm of gap formation, whereas the present study reports ultimate load at catastrophic construct failure, a later biomechanical endpoint that would be expected to yield higher values. Despite these differences in failure metrics, both studies demonstrated similar directional trends. The LG represented a similar technique as it uses a gift box stitch in addition to the locking whip stitch. This locking whip stitch method allows the load to be distributed better across the tissue while minimizing needle perforations and increasing failure load. 26
In a cadaveric midsubstance AT repair study by Meeks et al, 27 the authors found that a Krackow stitch with flat suture tape significantly increased failure load over round suture (352 N and 289 N, respectively), which was the type of suture tested in this study. 27 The KB group in this study (292 N) achieved similar load results to the round suture.
One important factor is the difference in the number of strands crossing the repair site: the gift box configuration in WG and LG creates 4 suture strands across the defect, whereas the KB core repair had only 2 strands crossing the repair site. This structural difference likely contributed to the prevalence of suture-related failures in KB (Figure 6) and may explain why KB did not achieve peak failure load commensurate with its greater suture burden (higher total suture weight).
Despite having fewer crossing strands, the KB achieved the greatest stiffness and least cyclic elongation of all 3 groups. This is likely attributable to the epitendinous augmentation which may function as a circumferential sleeve that reinforces the tendon interface.11,15 Because WG and LG were intentionally tested without augmentation to evaluate the baseline performance of gift box–based repairs, this effect cannot be isolated experimentally. However, previous literature supports the role of epitendinous reinforcement on reducing gap formation and elongation under cyclic loads,11,13,15 which was consistent in our study.
Conversely, the increased number of needle passes and total suture material required for the KB construct may introduce stress risers within the tendon.13,14 This may explain why the KB did not achieve failure load as high as LG. Furthermore, the clinical implications of increased nonabsorbable foreign material has been shown to cause inflammatory reaction in some patients.28,29 There appears to be a point of diminishing return with increased suture burden 30 as the KB improved construct stability (reduced elongation) but did not yield a proportional increase in ultimate strength relative to LG.
Van Dyke et al 31 conducted a cadaveric midsubstance AT repair study with similar loading protocol and showed that a Krackow gift box significantly improved biomechanics over a Bunnell stitch. The Bunnell is a nonlocking suture technique, akin to a whip stitch, that is popular because of its relatively simpler and more efficient technique. The Krackow gift box in their study achieved failure load (373 N), stiffness (47.5 N/mm), and elongation (5.8 mm) similar to the LG group in this study (load 436 N, stiffness 66.3 N/mm, elongation 6.1 mm).
Carmont et al 7 also tested a Bunnell technique with 4 strands of suture (compared to 2 strands in this current study and Van Dyke’s study 31 ) and achieved a failure load of 465 N, but experienced substantially higher elongation of 17.4 mm, highlighting the biomechanical disadvantages of nonlocking suture techniques.
Midsubstance AT repairs rely entirely on suture to achieve suture-tendon purchase for approximation and optimal repair. Thus, it is important to evaluate current advancements by comparing clinically relevant biomechanical properties. Future studies using a factorial design could evaluate whether combining LG with epitendinous augmentation would produce a construct with advantages in gap resistance and failure load.
Limitations
This study is not without limitations. The use of the time-zero cadaveric model does not capture the full scope of in vivo biological healing. The absence of inflammatory response, scar formation, and remodeling limits direct translation of biomechanical findings to long-term in vivo performance. Additionally, the advanced donor age (72 years) might not represent a typical patient population for midsubstance AT repairs.
In this experimental environment, ruptures and repair techniques were standardized, but clinically relevant factors such as nature of the injury, surgeon experience, suture material, and knot tying can alter construct performance. The simulated rupture in this model was created with a transverse scalpel incision, which differs from the irregular, often longitudinally split “ponytail” fiber pattern characteristic of AT ruptures. This distinction may affect suture purchase and the degree to which a locking mechanism is biomechanically required. The nature of a uniaxial testing machine also means that loads exerted on specimens do not fully represent multidirectional stresses, including torsion and shear, that the AT experiences during gait. Cyclic testing at 20-100 N simulates very small loads that might be experienced during nonweighted flexion and extension of the AT. This only represents a small fraction of the full 2-3 kN forces that the AT experiences in vivo during more rigorous activities like walking. Although time-zero findings are valuable, clinical research is necessary to determine long-term outcomes in patients. After data collection, the observed data violated normality assumptions, and the analysis was therefore appropriately performed using the Kruskal-Wallis test. Although the a priori analysis provided a reasonable basis for initial sample size estimation, the analysis of variance–based a priori power analysis does not directly correspond to the Kruskal-Wallis and was not intended as a post hoc validation. Beyond technical variables, other clinically relevant considerations include operative time, suture cost, and biological effects of additional suture material. In the present study, suture burden was estimated by way of suture weight. Additionally, the locking techniques evaluated in this study require an open surgical approach that may disrupt local tendon perfusion to a greater extent than minimally invasive or percutaneous methods; this biological consideration is not captured in the time-zero cadaveric model.
The LG and WG test groups did not include an epitendinous suture to investigate whether the gift box alone could achieve sufficient biomechanical performance without adding extra suture burden. Future studies may compare the effects of using additional epitendinous suture.
This study compared 3 prespecified repair constructs as they may be applied clinically and was not designed to isolate the independent contribution of each technical element. As a result, the observed differences in cyclic elongation, stiffness, and failure load reflect overall construct-level performance. The independent effects of locking configuration, gift box augmentation, number of strands crossing the repair site, and epitendinous augmentation cannot be determined from these data.
Conclusion
Among the 3 constructs tested, locking configurations demonstrated superior biomechanical performance compared with the nonlocking whip stitch technique. The locking whip stitch gift box (LG) achieved the highest failure load, whereas the Krackow with epitendinous baseball stitch (KB) minimized cyclic elongation.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261450946 – Supplemental material for Locking Stitch Techniques Demonstrate Improved Biomechanical Performance in Cadaveric Midsubstance Achilles Tendon Repair
Supplemental material, sj-pdf-1-fao-10.1177_24730114261450946 for Locking Stitch Techniques Demonstrate Improved Biomechanical Performance in Cadaveric Midsubstance Achilles Tendon Repair by D. Trey Remaley, Eric M. Cohen, Conrad Stoy, Jon Raso, Stephen Fernicola and Miguel A. Diaz in Foot & Ankle Orthopaedics
Footnotes
Acknowledgements
This study was funded by Winter Innovations, Inc, and supported by the National Science Foundation under grant no. 2304269.
Ethical Considerations
IRB was not required—a cadaveric study, where no patient information was used. Donors were procured by the United Tissue Network (UTN).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Winter Innovations, Inc, and supported by the National Science Foundation under grant no. 2304269.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D. Trey Remaley, DO, is a paid consultant for Arthrex. Miguel A. Diaz, MS, reports research grant from Winter Innovations, Inc. (paid directly to institution). Disclosure forms for all authors are available online.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author,
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.