
Abstract
Background:
Metatarsus adductus is a congenital forefoot deformity associated with pathologies including proximal fifth metatarsal fractures. The aim of this study is to assess the presence of metatarsus adductus and alignment in patients with proximal fifth metatarsal fractures. We hypothesize that there is an increased incidence of metatarsus adductus in patients with proximal fifth metatarsal fractures.
Methods:
A retrospective analysis was performed of patients who were treated for fifth metatarsal fractures from 2022 to 2024. Radiographic measurements including metatarsus adductus angle (MAA), lateral Meary angle, fracture zone, and foot alignment were recorded for each fracture.
Results:
Forty-nine patients were included. Patients with a zone 1 fracture had an average MAA of 14.2°. Of these patients, 10% had a cavus and 18% had a planus midfoot. Patients with a zone 2 fracture had an average MAA of 19.9°. Of these patients, none were cavus and 4% were planus. Patients with a zone 3 fracture had an average MAA of 26.8°. Four percent of patients had a cavus midfoot, whereas 4% had planus. Patients with a dancer’s fracture had an average MAA of 15°. Of these patients, 8% were cavus and 4% were planus. A significant difference (P < .001) was detected between the average MAA of zone 1 vs zone 3 fractures and between zone 3 and dancer’s fractures, suggesting an association between increasing metatarsus adductus severity and more proximal diaphyseal fracture location.
Conclusion:
Cavovarus deformity was infrequent in our cohort, whereas most patients had some degree of metatarsus adductus. Twenty-two percent in zone 1 and 6% in zone 2 were mild metatarsus adductus. Six percent in zone 2 and zone 3 were moderate, whereas 10% in zone 3 were severe. The authors recommend assessing for the presence of metatarsus adductus in patients with fifth metatarsal fractures, particularly zone 2 and 3, although further study in larger cohorts is needed to confirm these findings.
Level of Evidence:
Level IV, retrospective case series.
Introduction
Metatarsus adductus is a congenital isolated forefoot deformity of the tarsometatarsal joints that results in soft tissue contractures and foot remodeling. It is characterized by medial deviation of the metatarsals, adduction of the forefoot, and plantarflexion of the first ray.1–4 It is the most prevalent congenital foot disorder in newborns with an incidence rate ranging between 1 and 3 cases per 1000 births and a frequency of occurrence ranging from 0.1% to 12%.1-6 The metatarsus adductus angle (MAA) as measured on weightbearing radiographs has been shown to have excellent diagnostic reliability.7,8 Domínguez and Munuera 8 describe standard measuring techniques for metatarsus adductus using the fourth metatarsocuboid joints and have reported high intraobserver reliability with these methods. Angles measuring >15° are typically indicative of mild metatarsus adductus, angles measuring between 20° and 25° are classified as moderate, and severe metatarsus adductus measures >25°. 9
Metatarsus adductus deformity is theorized to be caused by osseous abnormality, abnormal muscle attachment, or high intrauterine pressure resulting in abnormal foot position. However, an exact etiology of metatarsus adductus is unknown.1-3,5,6,10 Metatarsus adductus can result in numerous pathologies including hallux valgus, skew foot, hammer toes, in-toeing, increased medial tibial torsion, recurrent fifth metatarsal fractures, and trouble with fitting into shoes.1,4-6,10
Proximal fifth metatarsal fractures often necessitate surgical intervention for treatment because of high nonunion and failure rates with nonoperative treatment. There are 3 well-defined zones of fifth metatarsal fractures. 12 Additionally, some patients may sustain a long spiral fracture in the distal metaphyseal region, which is considered a dancer’s fracture. 12 This can be a costly and highly debilitating endeavor for patients.11-13 Cavus foot deformity and varus hindfoot alignment have been implicated as risk factors contributing to fifth metatarsal fractures.10,11,13 One study identified a significant association between metatarsus adductus and zone 3 fifth metatarsal fractures. 14 Theodorou et al 15 found that metatarsus adductus was common among patients with metatarsal stress fractures and hypothesized that it is due to increased mechanical load across the lateral aspect of the foot.
The aim of our study was to evaluate the presence of metatarsus adductus and cavus foot deformity in patients with proximal fifth metatarsal fractures. We hypothesize that there is an increased incidence of metatarsus adductus in patients with proximal fifth metatarsal fractures regardless of location of fracture.
Methods
This retrospective review was conducted following Institutional Review Board approval. All patients treated by the senior author who had a diagnosis of fifth metatarsal fracture from 2022 to 2024 were queried using International Classification of Diseases, Tenth Revision (ICD-10). Patients who had multiple fractures, prior foot deformity surgery (hallux valgus, progressive collapsing foot deformity, etc), or incomplete imaging (nonweightbearing or lacking sufficient views) were excluded. Of the 74 patients identified in the database query, 49 patients and 49 feet were included.
Patients with fifth metatarsal fractures were assessed for the age, sex, fracture side, and fracture location. Fractures were radiographically classified according to the zone of injury. MAA (Figures 1-2) and lateral Meary angle (LMA) (Figure 3) of the affected foot were measured on anterior-posterior and lateral weightbearing radiographs of the foot, respectively. The metatarsus adductus angle was measured in the same technique described by Domínguez and Munuera, 8 which has been found to have high intraobserver reliability. Radiographic measurements were made using standard techniques (Figures 1-3). 8 These were then categorized as cavus (greater than 4° cavus), planus (greater than 4° planus), or neutral (between 4° cavus and 4° planus). 9 The severity of metatarsus adductus deformity was compared within each fracture type. All fracture classification and measurements were performed by a fellowship-trained foot and ankle surgeon.
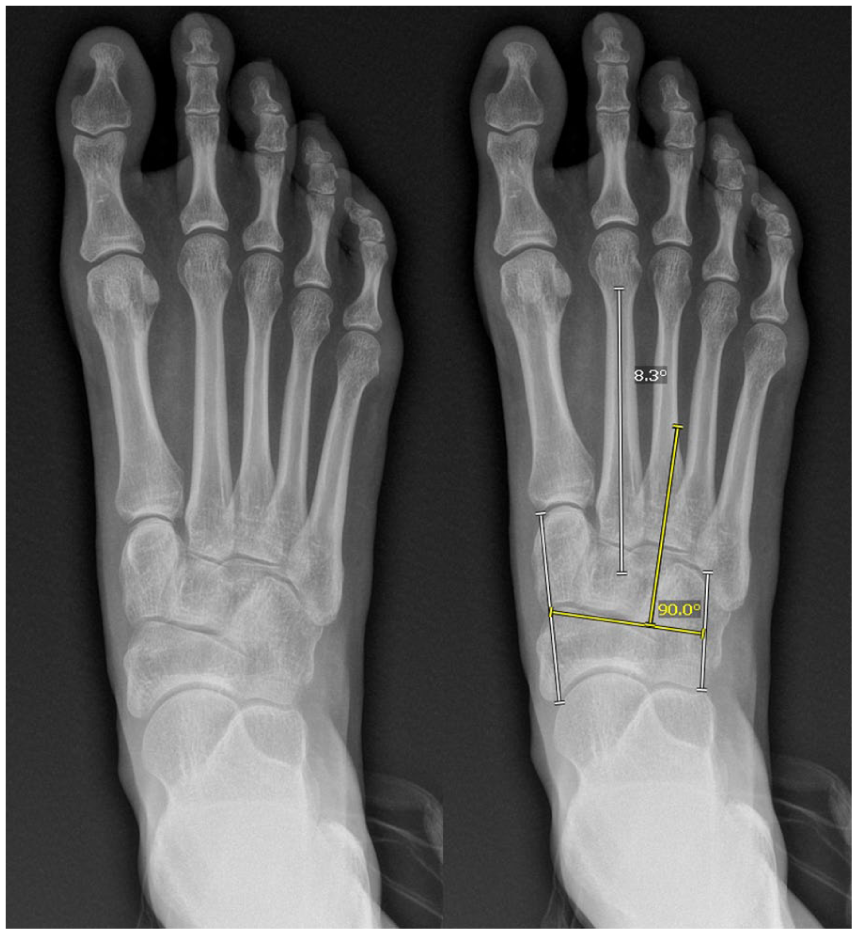
Patient with normal anatomy (left, metatarsus adductus angle [MAA] 8.3°).

Patient with severe metatarsus adductus (right, metatarsus adductus angle [MAA] 27.4°).
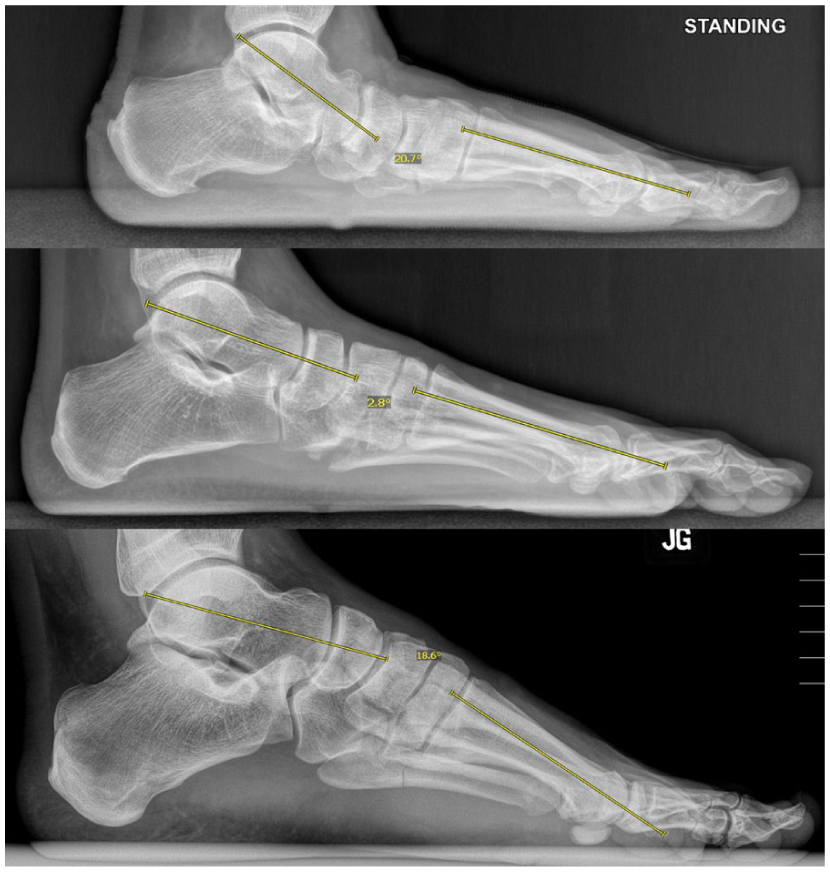
Patient with planus foot (top, lateral Meary angle [LMA] 20.7° of planus), neutral foot (middle, LMA 2.8°), cavus foot (bottom, LMA 18.6° of cavus).
Given the 4 zones and unequal sample sizes of each group, an analysis of variance was performed and a Tukey-Kramer post hoc analysis was used to identify variation between groups. Figure 4 identifies the average MAA within each fracture group.
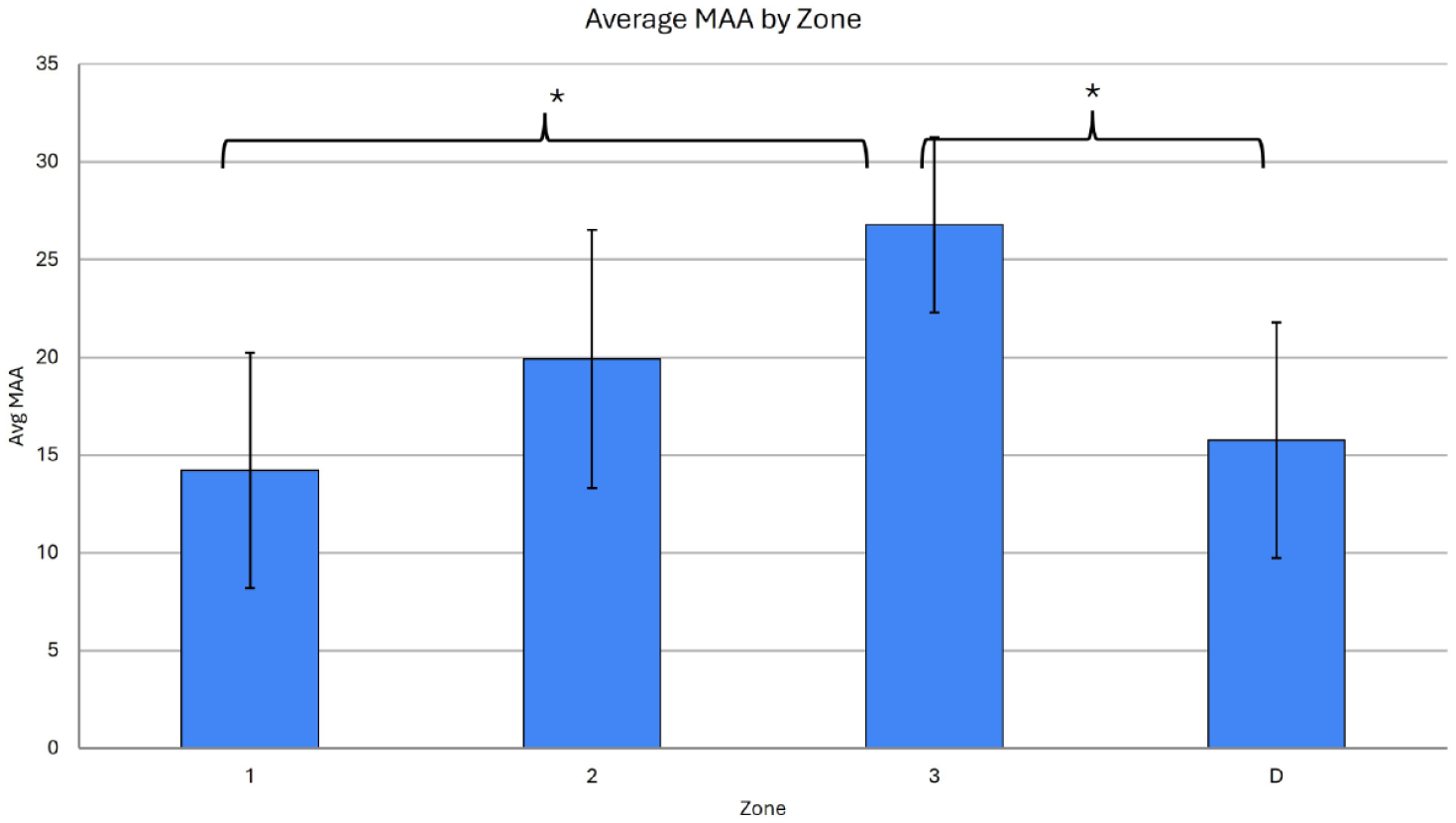
Average metatarsus adductus angle (MAA) by zone. The asterisks denote significant differences between zone 1 vs 3 and zone 3 vs distal.
Results
A total of 49 patients were included. Twenty-two had zone 1 fractures, 8 had zone 2 fractures, 8 had zone 3 fractures, and 11 had dancer’s fractures (Table 1). Patients with a zone 1 fracture had an average MAA of 14.2° (95% CI 12.8-15.6). Ten percent of these patients had a cavus midfoot, and 18% had a planus midfoot. Patients with a zone 2 fracture had an average MAA of 19.9° (95% CI 18.6-21.5). None had cavus, but 4% had planus deformity. Patients with a zone 3 fracture had an average MAA of 26.8° (95% CI 25.7-27.9). Four percent of patients had a cavus midfoot, whereas 4% had planus. Patients with a dancer’s fracture had an average MAA of 15° (95% CI 13.7-16.3). Of these patients, 8% were cavus and 4% were planus (Tables 2 and 3). The majority of zone 1 and distal metatarsal fractures had normal or mild metatarsus adductus angles with a single outlier with severe metatarsus adductus in zone 1. On the contrary, all zone 3 fractures had moderate or severe metatarsus adductus deformities. Analysis of variance and a Tukey-Kramer post hoc test showed a significant difference (P < .001) between the average MAA of zone 1 vs zone 3 fractures and between zone 3 and dancer’s fractures (Figure 4). Shapiro-Wilks test showed normal distribution of both metatarsus adductus angle as well as lateral Meary angle.
Age and Number of Patients With Each Type of Fracture.

Average Metatarsus Adductus Angle per Zone.
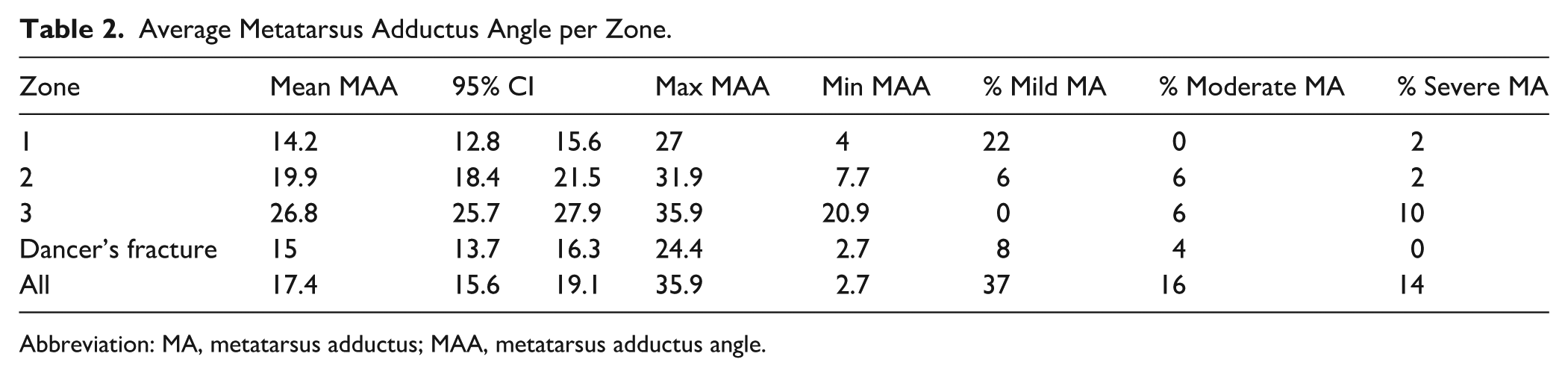
Abbreviation: MA, metatarsus adductus; MAA, metatarsus adductus angle.
Typical Foot Alignment and Its Association With Fracture Zone.

Abbreviation: NA, not applicable.
Discussion
Fifth metatarsal fractures are one of the most common foot and ankle injuries and the most common metatarsal injury.12,14 Clinically, fractures must be dealt with in an accurate and timely manner as a result of the high prevalence of nonunion in this fracture because of vascular watershed limiting perfusion. 13 The association of these fractures with lateral column overload is well recognized, but typically discussed in the setting of cavovarus deformity. Treatment and prognosis for these fractures are determined by the zone in which the fracture has occurred. One biomechanical study theorizes that repetitive activities leading to repetitive inversion may predispose patients to stress fractures at the fifth metatarsal. 16 It is reasonable to theorize that based on this study, one explanation for stress fractures in the setting of metatarsus adductus is that metatarsus adductus places the foot in an inverted position, which would increase the lateral column pressures.
Zone 1 fractures, identified by injuries to the metatarsal tuberosity, are classified as pseudo-Jones fractures or avulsion fractures from the lateral band of the plantar fascia. Conservative treatment approaches, such as early functional therapy, are recommended. In our cohort, these fractures were associated with primarily mild metatarsus deformity. Twenty-two percent of patients with this fracture had mild metatarsus adductus and 2% had severe deformity. All of these patients were treated nonoperatively with immobilization in a postoperative shoe.
Zone 2 fractures, characterized by fracture of the metaphyseal-diaphyseal junction extending to the fourth-fifth intermetatarsal joint, are labeled as Jones fractures. These fractures are caused by substantial adduction force on the foot often seen in athletic injuries or foot deformities.11-14 These fractures have a higher nonunion rate of 15% to 30%, 13 thus making treatment approaches more controversial. Both conservative and surgical treatments can be employed based on the surgeon’s assessment of patient expectations, degree of displacement, and probability of nonunion.12,17 In our cohort, all patients with zone 2 fractures had mild or moderate metatarsus adductus. All of these patients were treated nonoperatively with immobilization in a postoperative shoe. In patients with metatarsus adductus, a lateral-posted heel wedge was prescribed to be used in the postoperative shoe during initial immobilization. None of the patients required conversion to surgical treatment and none have had recurrent fractures. Patients with metatarsus adductus were encouraged to obtain custom inserts following healing.
Zone 3 fractures, identified as injury localized in the diaphyseal region, have a characteristically high nonunion rate. These fractures are often associated with repetitive microtrauma to the location of injury, antecedent pain, and low-energy mechanisms of injury. They are frequently diagnosed as stress fractures, suggesting a mechanical cause for fracture from a baseline deformity. These injuries often require surgical treatment, as conservative methods can involve up to 20 weeks of immobilization and still result in nonunion. Even following appropriate open reduction internal fixation, recurrent fracture or peri-implant fracture may still occur. In our cohort, all patients were treated nonoperatively in a postoperative shoe. All patients had metatarsus adductus and all were prescribed lateral-posted heel wedges to be used in the postoperative shoe.
One patient presented with a recurrent fracture after her previous stress fracture was treated with nonoperative treatment. As the patient was reluctant to proceed with surgery, we opted instead for custom shoe inserts to accommodate for the metatarsus adductus deformity. The patient was allowed to weightbear as tolerated in a supportive sneaker with the insert and her fracture fully healed both symptomatically and radiographically with nonoperative treatment. No patients returned with recurrence of their zone 3 fracture.
Additionally, we found that cavovarus deformity was very infrequently present in our cohort. Seventy percent of patients with zone 1 fractures and all patients with zone 2 and 3 fractures had either neutral or planus alignment of the midfoot. In contrast, most patients had some degree of metatarsus adductus deformity. In zone 1 fractures, 22% had mild metatarsus adductus and 0% had moderate. In zone 2 fractures, 6% had mild metatarsus adductus and 6% had moderate. In zone 3 fractures, 6% had moderate metatarsus adductus and 10% had severe. Although cavovarus alignment remains a risk factor for fifth metatarsal fractures, metatarsus adductus is notably more prevalent in this study.
Theodorou et al 15 found a strong association between metatarsus adductus and lateral metatarsal stress fractures specifically located in the proximal and mid-diaphyseal regions of the fourth and fifth metatarsals. Their study found that most patients with lateral metatarsal stress fractures had either moderate or severe metatarsus adductus. 18 In contrast, our study did not look at fourth metatarsal fractures, but found a similar association between moderate to severe metatarsus adductus and fifth metatarsal fractures. Yoho et al 19 found a statistically significant difference in mean MAA between subjects with Jones fractures and controls similar to our study. They also used the same manner for measurement of MAA and found high reliability with this method.
This study is limited by its small sample size, all of whom were treated by a single surgeon, which may reduce the generalizability of the findings and statistical power. Each subgroup was also small in size, with only 8 patients for zone 2 and zone 3. This analysis utilized analysis of variance, which assumes normally distributed data and homogeneity of variance across groups. As group sample sizes were unequal, the Tukey-Kramer correction was applied to account for this in the post hoc pairwise comparisons. Another limitation is that we did not perform a prior power analysis. Additionally, it is possible that there was a bias toward patients with more severe or long-standing symptoms because these patients were all seen by an operative, orthopaedic foot and ankle surgeon in a tertiary referral center. Our exclusionary criteria may bias toward healthier patients or less deformed patients. Additionally, our patients were treated nonoperatively, so our outcomes may not be generalizable to surgical cases. The outcomes are observational only. There may be a role for surgical intervention, so further research would be required to identify cases where surgery may benefit in the setting of metatarsus adductus. Lastly, severe cavovarus deformity affects the anterior-posterior projection of the foot, which may lead to falsely elevated MAA measurements. 15
Our findings suggest a strong and previously underestimated association between metatarsus adductus and fifth metatarsal fracture. The literature typically associates cavovarus foot deformity with the fractures, as lateral column overload puts additional stress to an already avascular area of the bone. Although all our patients healed with nonoperative intervention, this treatment may not be appropriate for all patients with fifth metatarsal fractures, such as high-level athletes with recurrent zone 3 fractures.
The authors recommend considering the presence of metatarsus adductus in patients with fifth metatarsal fractures, particularly zone 2 and 3, in addition to cavovarus deformity. Although the choice of surgical vs conservative treatment must be made with the patient factors in mind (activity level, comorbidities, return to play, recurrent fracture, etc), acknowledging the presence of deformity is necessary in holistic treatment.
Based on our study, clinicians may want to consider deformity in association with fifth metatarsal fractures. In patients who prefer conservative treatment or are poor surgical candidates, immediate immobilization with lateral offloading may be a consideration for nonoperative treatment. Our study demonstrated healing in nonoperatively treated patients, but this finding was observational only. In patients who undergo surgical treatment who have metatarsus adductus, clinicians can consider lateral offloading through custom inserts to potentially decrease risk for nonunion and refracture. Finally, for the patient who sustains recurrent fracture recalcitrant to surgical management and offloading, correction of the metatarsus adductus may be considered. This would be in line with cavovarus correction for chronic ankle sprains. As such, given the extensive nature of the procedure, it should only be considered for recalcitrant cases.
Conclusion
There is a strong association between proximal fifth metatarsal fractures and lateral column overload of the foot. Although cavovarus deformity is typically implicated, we have found that metatarsus adductus was more frequently observed than cavovarus deformity among patients in this cohort. Moreover, although zone 1 and 2 fractures are associated with mild and moderate deformity, zone 3 fractures are associated with moderate or severe metatarsus adductus. We recommend consideration of lateral column offloading to the treatment of fifth metatarsal fractures. Based on the observational findings of this series, we recommend consideration of lateral column offloading in the treatment of fifth metatarsal fractures; in this cohort, lateral-posted heel wedges were used for initial immobilization and custom inserts were prescribed following healing in patients with metatarsus adductus.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261453078 – Supplemental material for Metatarsus Adductus Association With Fifth Metatarsal Fractures: Radiographic Analysis
Supplemental material, sj-pdf-1-fao-10.1177_24730114261453078 for Metatarsus Adductus Association With Fifth Metatarsal Fractures: Radiographic Analysis by Caitlin Curtis Crocker, Delaney Lagrew, Chris Lamprecht, Alex Barnett and Miqi Wang in Foot & Ankle Orthopaedics
Footnotes
Ethical Considerations
IRB was obtained at the University of Florida.
Consent to Participate
Informed consent was obtained at the University of Florida.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Caitlin Curtis Crocker, MD, reports that her husband is sales representative for Exactech/Skeletal Dynamics/ Conventus Orthopaedics (unrelated to this project). Miqi Wang, MD, reports Conventus Orthopaedics Inc, consulting; AAOS, committee member; Restor3D, research support; Exactech, consulting. ICMJE forms for all authors are available online.
Data Availability Statement
Data is available for review upon request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.