
Abstract
Background:
Varus-type ankle osteoarthritis (OA) is often managed conservatively; however, surgical intervention is required in some patients. Identifying factors associated with transition to surgery may help optimize treatment timing.
Methods:
This retrospective study included 53 ankles in 45 patients with Takakura-Tanaka stage ≥3a varus ankle OA who newly initiated conservative treatment with lateral wedge insoles. Patients were classified into nonsurgery or surgery groups based on treatment choice. Multivariate logistic regression was performed using 12 clinical and radiographic variables, including Self-Administered Foot Evaluation Questionnaire (SAFE-Q) subscales and weightbearing radiographic parameters.
Results:
At baseline, lower pain-related SAFE-Q scores (odds ratio [OR], 0.854; 95% CI, 0.738-0.989; P = .035) and greater talar tilt in the tibial plafond–talar dome angle (TTW) (OR, 1.506; 95% CI, 1.025-2.214; P = .037) were, in multivariable logistic regression, independently associated with surgical selection. The cutoff values for predicting surgery were ≤68 for pain-related SAFE-Q and ≥5° for TTW. With the numbers available, no significant difference could be detected in radiographic parameters at the final assessment. Neither group showed significant longitudinal changes in SAFE-Q or radiographic parameters with the numbers available. Pain-related SAFE-Q scores at the final assessment were significantly better in the nonsurgery than surgery groups.
Conclusion:
Baseline pain-related impairments and TTW deformities were associated with subsequent surgical selection in patients with advanced varus ankle OA.
Level of Evidence:
Level III, retrospective comparative cohort study.

Keywords
Introduction
Ankle osteoarthritis (OA) occurs in approximately 6% of the population. 1 The functional disability and diminished quality of life associated with end-stage ankle OA are comparable to those associated with end-stage hip or knee OA.2,3 The etiology of ankle OA includes intra-articular fractures, and varus ankle OA without prior trauma or general disorders is rare. Although the etiology of varus ankle OA remains to be fully determined, the Japanese lifestyle, that is, people sitting cross-legged or with legs tucked under their bodies, has been implicated because the prevalence of varus ankle OA in Japan is higher than that in other countries. 4 The management of varus-type ankle OA typically begins with conservative measures, including lateral wedge insoles (LWIs), intra-articular injections, and nonsteroidal anti-inflammatory drugs. For patients who fail to respond to such nonoperative treatments, surgical options are considered based on age, activity level, and severity of the deformity. Depending on these factors, procedures, such as supramalleolar osteotomy, ankle arthrodesis, or total ankle arthroplasty, may be performed. In the early stages of varus ankle OA, the varus deformity at the ankle joint is compensated by valgus inclination at the subtalar joint.5,6 LWIs have been used to treat patients with varus ankle OA and have been shown to reduce medial ankle compartment loading. 7 Therefore, most patients respond favorably to conservative treatment. In contrast, patients with Takakura-Tanaka classification stage ≥3a are more likely to require surgical intervention. In cases of pronounced talar tilt, the progression of deformity during the natural course of the disease has been reported. 8 Continuing ineffective conservative treatment under such circumstances may delay timely surgical management, imposing a substantial burden on patients and resulting in adverse socioeconomic consequences. This underscores the importance of understanding the clinical backgrounds of patients likely to require surgery. Previous reports have indicated that patients are more likely to select surgery for musculoskeletal disorders when experiencing higher levels of symptoms or dysfunction and have positive perceptions of surgical suitability and expectations. 9
Based on this evidence, we hypothesized that pain, pain-related functional impairment, and the degree of deformity observed on imaging studies are key factors influencing the background of patients opting for surgical treatment. We aimed to investigate predictive factors in the clinical background of patients with varus-type ankle OA at stage ≥3a who newly initiated conservative treatment with LWI, focusing on whether they subsequently transitioned to surgery or continued nonoperative management.
Methods
Ethical Approval Statements
This study was approved by the local institutional review board (research number: 3472).
Study Population
A total of 82 ankles from 66 consecutive patients who were newly prescribed LWI for varus-type ankle OA from 2013 to 2023 were included in this retrospective study. After excluding cases with <12 months of follow-up (8 ankles of 5 patients) and those with a history of surgery, valgus-type ankle OA, or general disorders such as rheumatoid arthritis or Charcot neuroarthropathy (10 ankles of 10 patients), a cohort of patients with primary varus-type ankle OA was identified (64 ankles in 51 patients). Furthermore, early-stage cases, up to stage 2 according to the Takakura-Tanaka classification,4,10 were excluded (11 ankles of 6 patients). Consequently, 53 ankles of 45 patients were included in this study (Figure 1). No missing data were imputed, and only complete cases were analyzed.

Flow diagram of participant selection.
For conservative treatment, LWI, nonsteroidal anti-inflammatory drugs, and intra-articular injections were administered in appropriate combinations in each case. Patients who opted for surgery were assigned to the surgery group, whereas those who did not were assigned to the nonsurgery group. In the multivariate logistic regression analysis, the surgery group was set as the dependent variable, and 12 covariates were included: age; body mass index (BMI); the Self-Administered Foot Evaluation Questionnaire (SAFE-Q), which consists of 5 subscales11,12; and 5 parameters obtained from weightbearing radiographs of the ankle. The angles between the tibial shaft and articular surface of the tibial plafond on anteroposterior and lateral views (TAS and TLS), the tibial shaft and medial malleolus (TMM), the articular surface of the tibial plafond and talar dome (TTW), and the angles between the tibial shaft and talar dome (TTS) were measured using weightbearing ankle radiographs (Figure 2). Varus-type OA was defined as a TTS of <90°.

Radiographic assessment parameters on weightbearing ankle radiographs. (A) The angles between the tibial shaft and the articular surface of the tibial plafond on anteroposterior view (TAS), and the articular surfaces of the tibial plafond and talar dome (TTW) were measured. (B) The angles between the tibial shaft and the medial malleolus (TMM), and the tibial shaft and talar dome were measured. (C) The angle between the tibial shaft and articular surface of the tibial plafond on lateral view (TLS) was measured.
The nonsurgery group was evaluated at the initial visit and final follow-up (mean 45.6 ± 29.6 [range 12-109] months after initial visit), whereas the surgery group was evaluated at the initial visit and immediately before surgical intervention (mean 23.4 ± 28.4 [range 2-98] months after initial visit). The following 4 sets of comparisons were performed: (1) between the baseline and final assessment in the nonsurgery group, (2) between the baseline and final assessment in the surgery group, (3) between the nonsurgery and surgery groups at baseline, and (4) between the 2 groups at final assessment.
Statistical Analysis
The sample size in this study was smaller than that required to compare means between the 2 groups, with a power of 0.80 and an alpha error of 0.05. This study was designed as an exploratory, hypothesis-generating analysis. Multivariate analysis was performed using logistic regression with a stepwise selection procedure to identify predictors of surgery and estimate their odds ratios (ORs). The initial candidate variables included age, BMI, SAFE-Q, and 5 parameters derived from weightbearing ankle radiographs, and ORs with 95% CIs were reported for variables retained in the final model. Statistical significance was set at a P value <.05. The sensitivity and specificity of the receiver operating characteristic curve and the area under the curve were calculated for significant variables using multivariate logistic regression. The cutoff value was calculated based on sensitivity and specificity. Homogeneity of variances was assessed using the F test following confirmation of normality of continuous variables using the Shapiro-Wilk test. Student t tests were applied when variances were equal; otherwise, Welch t tests were used. Because 4 sets of comparisons were performed simultaneously across multiple SAFE-Q subscales and radiographic parameters, no correction for multiple comparisons was applied, and therefore all P values should be interpreted with caution. All analyses were performed using SPSS, version 26.0 (IBM Corp).
Results
Overall, 45 patients (53 ankles) were included in the study: 28 patients (33 ankles) in the nonsurgery group and 17 patients (20 ankles) in the surgery group (ankle arthrodesis, 4 ankles; total ankle arthroplasty, 11 ankles; and supramalleolar osteotomy, 5 ankles). Patient demographics and baseline characteristics are summarized in Tables 1 and 2.
Baseline Demographics of All Included Cases (53 Ankles/45 Patients). a

Abbreviations: SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAS, tibial anterior surface angle; TLS, tibial lateral surface angle; TMM, tibial medial malleolus angle; TTS, tibial talar surface angle; TTW, talar tilt of weightbearing.
Male: 9 ankles / 7 patients, female: 44 ankles / 38 patients.
Characteristics and Outcome Measures of the 2 Study Groups.

Abbreviations: SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAS, tibial anterior surface angle; TLS, tibial lateral surface angle; TMM, tibial medial malleolus angle; TTS, tibial talar surface angle; TTW, talar tilt of weightbearing.
At baseline, TTW was significantly greater in the surgery group than in the nonsurgery group (P = .02, 95% CI, –5.219 to –0.469). No significant between-group differences were observed with the numbers available in the pain-related SAFE-Q subscale at baseline (P = .28).
In multivariate analysis, the pain-related subscale of the SAFE-Q at baseline was associated with a lower likelihood of surgical intervention, whereas TTW on radiographic assessment at baseline was associated with a higher likelihood of surgical intervention. Higher pain-related subscale of SAFE-Q was significantly associated with a lower likelihood of surgery (OR, 0.854; 95% CI, 0.738-0.989; P = .035), whereas greater TTW was associated with an increased likelihood of surgery (OR, 1.506; 95% CI, 1.025-2.214; P = .037) (Tables 3-5). Multicollinearity was assessed using variance inflation factors, all of which were below the commonly accepted threshold. Model fit was confirmed using the Hosmer-Lemeshow goodness-of-fit test, indicating that the logistic regression model was adequately specified and not overfitted. The cutoff values for the pain-related subscale of the SAFE-Q and TTW for surgery were 68° and 5.0° at baseline, respectively (Figures 3 and 4).
Variables Retained in the Final Stepwise Logistic Regression Model.

These variable were retained in the final model but did not achieve statistical significance.
Abbreviations: OR, odds ratio; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TTW, talar tilt of weightbearing.
Variables Removed During Stepwise Selection at Baseline.
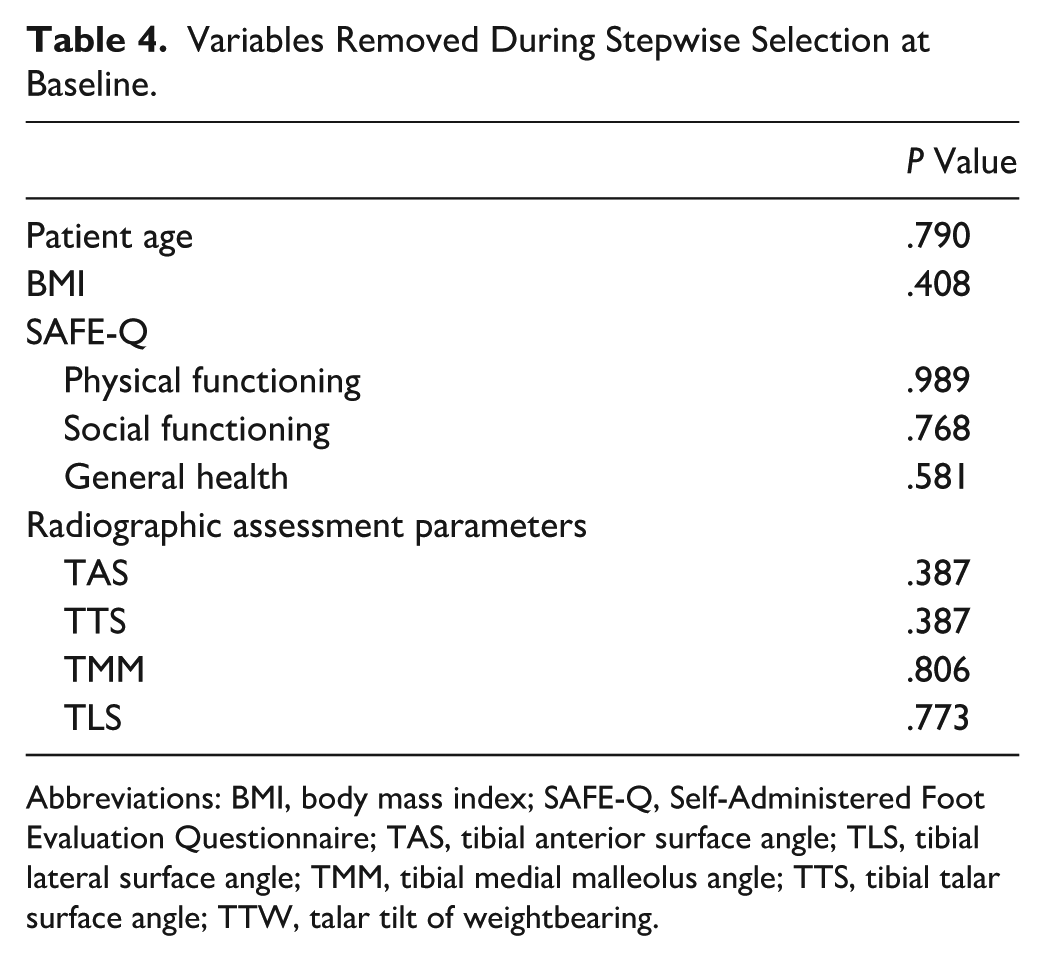
Abbreviations: BMI, body mass index; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAS, tibial anterior surface angle; TLS, tibial lateral surface angle; TMM, tibial medial malleolus angle; TTS, tibial talar surface angle; TTW, talar tilt of weightbearing.
Variables Removed During Stepwise Selection at Final Assessment.
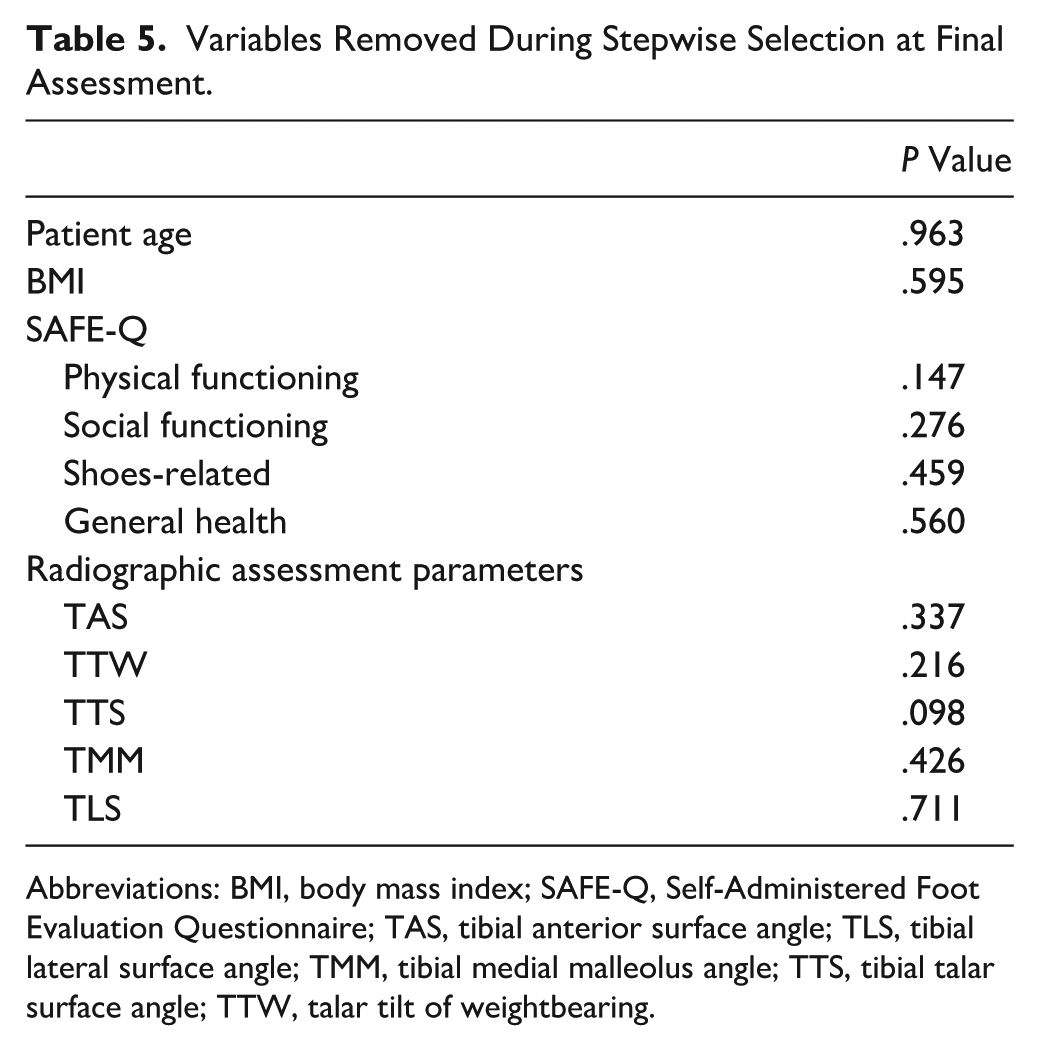
Abbreviations: BMI, body mass index; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAS, tibial anterior surface angle; TLS, tibial lateral surface angle; TMM, tibial medial malleolus angle; TTS, tibial talar surface angle; TTW, talar tilt of weightbearing.

Receiver operating characteristic curve analysis of Pain-related subscale scores of the Self-Administered Foot Evaluation Questionnaire at baseline for surgical intervention. The optimal cutoff value was 68.0, with corresponding sensitivity (0.889) and specificity (0.391). The area under the curve was 0.603 (95% CI, 0.423-0.782).

Receiver operating characteristic curve analysis of talar tilt of weightbearing at baseline for surgical intervention. The optimal cutoff value was 5.0, with corresponding sensitivity (0.700) and specificity (0.667). The area under the curve was 0.6917 (95% CI, 0.5408-0.8426).
In the surgery group, with the numbers available, no significant longitudinal changes were observed between baseline and final assessments in any SAFE-Q subscale or radiographic parameter (Table 6).
Within-Group Changes From Baseline to Final Assessment With 95% CIs.

Abbreviations: MD, mean difference; SAFE-Q, Self-Administered Foot Evaluation Questionnaire; TAS, tibial anterior surface angle; TLS, tibial lateral surface angle; TMM, tibial medial malleolus angle; TTS, tibial talar surface angle; TTW, talar tilt of weightbearing.
Similarly, in the nonsurgery group, with the numbers available, no significant changes were detected between baseline and final assessments across SAFE-Q subscales or radiographic parameters.
At the final assessment, the pain-related SAFE-Q subscale was significantly higher in the nonsurgery group than in the surgery group (P < .01, 95% CI, 7.064-27.341). No significant between-group differences were observed with the numbers available in radiographic parameters at the final assessment (Table 2). Of note, 1 patient in the nonsurgery group demonstrated marked radiographic progression, with a final TTW of 28°, compared with a cohort baseline maximum of 13°; this value did not materially alter the within-group or between-group analyses.
Discussion
This study included patients who were likely to opt for surgery. At baseline, patients with a pain-related SAFE-Q score of ≤68 or those presenting with varus deformity of the ankle characterized by a TTW of ≥5° were more likely to choose surgery. In addition, the OR for TTW was 1.506, indicating that each 1° increase in talar tilt was associated with approximately a 50% increase in the likelihood of undergoing surgery. This provides a clinically intuitive measure that may assist clinicians in counseling patients regarding the progression of varus ankle OA.
In patients with varus ankle OA, the talus becomes varus and rotates internally as the ankle joint progresses. To compensate for this deformity, the calcaneus undergoes valgus and external rotation of the subtalar joint. The breakdown of this compensatory function is caused by OA progression, and the hindfoot shows varus deformity.5,6
Regardless of the severity of ankle OA, an initial trial with conservative treatment is recommended to assess the therapeutic potential. Although multiple nonoperative modalities may be combined to alleviate symptoms, supporting evidence remains limited and is often of low methodologic quality. Intra-articular HA injections are typically well tolerated and provide rapid improvements in pain, stiffness, function, and patient satisfaction while reducing the need for analgesics. 13 However, these injections are not reimbursed by Japan’s national health insurance system. In contrast, intra-articular corticosteroid injections offer short-term symptomatic relief lasting 4-8 weeks; however, given their potentially deleterious effects on joint cartilage, current evidence suggests restricting their use to persistent pain in advanced-stage OA, with no more than 3 to 4 injections per year. 14
The aim of orthotic treatment is to reduce pain by maintaining proper alignment, thereby decreasing the mechanical load on the ankle. From a biomechanical standpoint, LWI can reduce plantar pressure on the medial forefoot and hindfoot, 7 whereas their clinical success can be predicted with >80% sensitivity based on mechanical axis deviation measured on full weight-bearing long-standing radiographs. 15 To date, only 1 clinical trial has evaluated the long-term effects of LWI, reporting no adverse impact on hip or ankle joint space width over 36 months, although the authors reported no clinically meaningful benefits. 16
LWI is generally indicated in the early stages of ankle OA when varus deformity has not yet progressed severely and compensatory motion at the subtalar joint is preserved.
In end-stage disease, this compensatory mechanism often collapses, potentially exacerbating the calcaneal varus alignment. Nevertheless, even among patients with end-stage ankle OA, those with mild or absent subtalar joint degeneration may retain sufficient compensatory capacity to maintain neutral hindfoot alignment. 17 Therefore, LWI may be effective for this subset of patients. Accordingly, herein, LWI was applied to end-stage cases. Although conservative treatment did not result in significant improvements from baseline to the final assessment with the numbers available, the pain-related domain of the SAFE-Q at the final assessment was significantly better in the non-surgery group (68.8 ± 15.8) than the surgery group (51.6 ± 11.1). No minimum clinically important difference (MCID) has been established for the SAFE-Q pain subscale in the existing literature. However, the MCIDs reported for PROMIS Pain Interference range from 3 to 25 points (median = 8.9), 18 and calculated MCID values for VAS pain range from 1.8 to 5.2 points. 19 Given these reference values, the 17-point difference observed between the 2 groups in our study is likely to represent a clinically meaningful difference. Insights into other weightbearing joints may further contextualize these findings. Patients with musculoskeletal disorders, particularly those affecting the hip and knee, are more likely to opt for surgery when experiencing greater symptom severity or functional impairment, coupled with favorable perceptions of surgical suitability and expected outcomes. Additional factors, including age, overall health status, race, financial circumstances, professional and nonprofessional communication, and sources of information also influence decision making, although their impact on the likelihood of preferring surgery appears less consistent. 9
In hip osteoarthritis, the effectiveness of a consensus-based decision tool with uniform criteria for hip replacement surgery has been reported, incorporating age, flexion, internal rotation, Hip Disability and Osteoarthritis Outcome Score, quality of life, and Kellgren-Lawrence classification as key determinants. 20
To date, no reports have addressed decision making in ankle OA. However, our study demonstrated that baseline pain and TTW are novel, clinically relevant predictors. To our knowledge, this is the first study to highlight these parameters as key considerations in subsequent surgical selection for ankle OA.
This study had some limitations. First, the conservative treatment in this study was not standardized; the combination of intra-articular injections, LWI, pharmacologic therapy, and physiotherapy was determined by patient preference and the clinical discretion of the treating physician. This heterogeneity represents a central limitation, as it may influence both treatment response and the subsequent transition to surgery. Therefore, the findings should be interpreted with caution, particularly regarding the causal interpretation of predictors associated with surgical selection. Second, this study did not account for patient-level factors such as medical comorbidities, socioeconomic circumstances, occupation, or family structure, which may influence treatment selection and outcomes. These variables were not systematically collected in our data set and, therefore, could not be incorporated into the analysis. Third, the relatively small sample size is a limitation; however, it reflects the rarity of such cases and underscores the importance of reporting detailed clinical outcomes to guide future investigations. Fourth, in this study, the radiographic parameters (TAS, TLS, TMM, TTW, and TTS) were performed once by a single surgeon, and no further analysis of interobserver or intraobserver reliability was conducted. Their accuracy and reproducibility are generally lower than those of 3D imaging modalities. However, these indices are widely used and well-established in clinical practice. 8 Finally, the prevalence of stage 3a arthritis differed substantially between the nonsurgical and surgical groups, which may represent a potential source of confounding. Future studies should incorporate stratified or stage-adjusted analyses to account for this imbalance.
To our knowledge, this is the first study to report the surgical preferences in patients with advanced ankle OA. These findings may help clinicians determine the appropriate timing for transitioning from conservative to surgical treatment.
Conclusion
In patients with advanced varus ankle OA who initiated conservative treatment, lower pain-related SAFE-Q scores, and greater TTW at baseline were independently associated with the subsequent selection of surgical intervention. These findings suggest that pain-related impairments and tibiotalar alignment may serve as clinically relevant indicators linked to the likelihood of transitioning to surgery. Although these parameters were associated with surgical selection in this cohort, they should not be interpreted as validated thresholds for determining the timing or expected benefit of conservative management.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114261454964 – Supplemental material for Pain-Related Impairment and Talar Tilt as Predictors of Surgical Decision Making in Advanced Varus Ankle Osteoarthritis
Supplemental material, sj-pdf-1-fao-10.1177_24730114261454964 for Pain-Related Impairment and Talar Tilt as Predictors of Surgical Decision Making in Advanced Varus Ankle Osteoarthritis by Hiroaki Kurokawa, Akira Taniguchi, Chika Nakaniwa, Norihiro Tsujimoto, Yoshiyuki Kamatani, Yinghao Li, Nan Mei, Takuma Miyamoto, Yasuhito Tanaka and Kenji Kawamura in Foot & Ankle Orthopaedics
Footnotes
ORCID iDs
Ethical Considerations
This study was approved by the local institutional review board (research number: 3472).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.