
Abstract
Introduction:
Substance use disorder (SUD) is a significant cause of morbidity and mortality among perinatal people. Integrated perinatal SUD treatment programs (SUD, obstetrics, mental health, and other services) show promising improvements in SUD and perinatal outcomes. This study describes the redesign of an integrated perinatal SUD treatment program that partnered with a community-based recovery housing facility to integrate clinical and social services and evaluated the impact of this redesign on several indices of treatment retention.
Methods:
This retrospective cohort study used health record data from 164 perinatal people aged 18+ years admitted to an integrated intensive outpatient SUD treatment program in Baltimore, Maryland, between March 8, 2021, and June 11, 2025. Negative binomial regression was used to examine the association between the program redesign and length of treatment, and logistic regression was used to examine associations between program redesign and retention (until delivery and at 30-, 60-, and 90-days postpartum).
Results:
Perinatal people admitted post-redesign had a 108% increase in length of treatment compared to people admitted pre-redesign (adjusted incidence rate ratios [aIRR] 2.08, 95% CI: 1.40, 3.10). People admitted post-redesign had greater odds of treatment retention until delivery (aOR 3.53, 95% CI: 1.39, 8.95); and greater odds of treatment retention at 30-, 60-, and 90-day postpartum compared to people admitted pre-redesign (adjusted odds ratio [aOR] 6.58, 95% CI: 2.52, 17.16; aOR 9.87, 95% CI: 3.47, 28.07; and aOR 5.50, 95% CI: 1.98, 15.27, respectively).
Discussion:
The study illustrates the benefits of creating community partnerships to deliver integrated clinical and social services to perinatal people with severe forms of SUD.
Introduction
Substance use disorder (SUD) is a significant cause of morbidity and mortality among perinatal people in the United States. In Maryland, substance use overdose was the leading cause of death among perinatal people from 2011 to 2020. 1 Untreated perinatal SUD increases risks for preterm delivery, low birth weight, admission to the neonatal intensive care unit, and stillbirth.2,3 Simultaneously, pregnancy offers a unique opportunity to initiate SUD treatment as perinatal people report heightened concerns for the baby’s welfare and more readiness to reduce substance use. 4
SUD treatment during pregnancy, including the use of medications for opioid use disorder (MOUD), is the most effective method to decrease substance use and adverse perinatal events,5,6 with good outcomes strongly associated with pre- and post-delivery retention. 7 The most effective SUD treatment programs for perinatal people are accessible and responsive to health equity—defined as the absence of unfair differences in health among social groups. 8 These programs utilize an interdisciplinary approach that integrates mental health services, obstetric care, and pediatric care. They also address barriers to SUD treatment such as stigma, discrimination, housing, transportation, legal assistance, and the need for co-location with their children, all while emphasizing trauma-informed and gender-responsive care.5,9,10
Despite strong evidence supporting SUD treatment, including MOUD, only half of pregnant people with opioid use disorder (OUD) in treatment receive MOUD. 11 There are significant racial and ethnic disparities in access to MOUD, rooted in structural and social drivers. 12 Black women are less likely to receive MOUD compared to White women. 12 Additionally, perinatal people with SUDs often experience high rates of co-occurring mental health conditions like depression, anxiety, and post-traumatic stress disorder, and have a history of trauma.13–15 If left untreated, these mental health issues can lead to worsened substance use outcomes, poor treatment retention, and worsened quality of life.13,16
The Comprehensive Addiction and Pregnancy (CAP) program, located at the Johns Hopkins Bayview Medical Center (JHBMC) in east Baltimore, Maryland, is nationally recognized for its interdisciplinary approach to treating perinatal people with SUDs for five decades. 17 CAP played a pivotal role in the evaluation of the efficacy and safety of perinatal methadone and buprenorphine for OUD.18,19 Historically, CAP offered SUD treatment (MOUD with Residential [ASAM 3.1], Intensive Outpatient [IOP; ASAM 2], and Outpatient [OP: ASAM 1] levels of care), Obstetrics/Gynecology (OB/GYN), pediatric care, psychiatric care, and registered nursing support. Prior to the COVID-19 pandemic, the residential level of care was closed and replaced with domiciliary services co-located within a two-floor facility on the medical center campus and delivered through a reduced staffing model. During the COVID-19 pandemic, the domiciliary unit had a capacity of eight patients, did not allow accommodations for children and visitors, and was typically at less than 50% bed occupancy.
During the COVID-19 pandemic, several factors drove the medical center to further redesign CAP’s integrated programming: (1) Long-term financial revenue downturn linked to a decline in the patient census; (2) Prevention of program revenue increases from updates in Maryland’s Health Services Cost Review Commission; (3) Consequent unsustainability of expenses for hospital-based housing and staffing for OB/GYN, pediatric, and other ancillary providers; and (4) Loss of federal grant funding. To maintain program continuity, IOP and OP services were incorporated within an Opioid Treatment Program (OTP) located in the same building, and the domiciliary unit was closed. Perinatal and pediatric services were moved to a nearby Federally Qualified Health Center not owned by the medical center (though higher-risk medical procedures, e.g., deliveries, occurred at the medical center hospital).
Concurrent with this disaggregation of services and reduction in staffing, CAP worked with the Medical Center to create a Memorandum of Understanding with a community-based Christian faith-based facility, Helping Up Mission (HUM), to provide safe housing, transportation, and other social services for perinatal residents who wished to enroll in CAP. 20 In the spirit of distributive justice, the aim of this partnership was to retain an integration of clinical and social services that were no longer on the medical campus and move social services into a setting that was established and more clearly a part of the local community. This also allowed access to more services than were available through the medical center, given the reimbursement model of capitated costs. The fully redesigned CAP began operation on March 1, 2023. The purpose of this study is to examine the impact of this CAP redesign on SUD treatment retention pre- and post-delivery among perinatal people receiving integrated SUD treatment through CAP. The CAP redesign addressed health equity by implementing a multi-faceted and integrated approach that addressed clinical and social drivers of health within a community-academic partnership. This partnership prioritized the needs of perinatal people with SUD, improved accessibility of critical services, and decreased the risk for fragmentation of care.
Methods
Study sample and data collection
The sample for this observational, retrospective cohort study comes from the CAP program. We extracted data from the paper health records of 227 perinatal people aged 18 years and older who were enrolled at CAP between March 8, 2021, and June 11, 2025. After exclusion for reasons detailed below, our final analytical sample was 164 perinatal people (Fig. 1).

Flow diagram of sample.
Data were extracted between July 2025 and October 2025 by three trained researchers (LM, TC, EJ) and entered into the institution’s Research Electronic Data Capture (REDCap) system using a standardized data collection format. 21 One researcher collected data from each chart (LM), and another researcher independently verified 33% of chart entries (TC or EJ). There were no discrepancies. The Johns Hopkins Medicine Institutional Review Board (protocol IRB00468404) approved this study.
Primary treatment settings and service integration
CAP
The current program model offers SUD treatment (with MOUD) at the JHBMC Addiction Treatment Services OTP that includes IOP and OP levels of care, offering modules on parental education, stress and anger management, relapse prevention, and other issues relevant to the treatment of perinatal people with SUDs. An interdisciplinary team of psychiatrists, psychologists, counselors, and advanced practice providers offers trauma-informed SUD care. IOP level of care includes a minimum of nine structured hours of weekly counseling/education for substance use for people needing more support than standard outpatient care but no housing. 22
HUM
HUM is a long-term community-based facility for people with SUD and unstable housing that has been in existence since 1885. It is in east Baltimore, approximately three miles from JHBMC. The women’s facility was opened in 2022 in a new building specifically designed for women and children. Despite a faith-based orientation, people of all beliefs are welcome. Perinatal people are provided safe and secure housing pre-delivery and can remain post-delivery with their child for up to 1 year. HUM does not provide SUD treatment or other health care services, they offer wrap-around social services. HUM staff are trained to utilize trauma-informed care techniques, and the facility offers access to several social services like job training and job-seeking skills, spiritual development (e.g., pastoral counseling, peer recovery support), social outings, and educational offerings. HUM operates a highly structured living environment that requires residents to adhere to facility rules (e.g., curfews and an initial period that restricts opportunities to leave the facility), completion of daily chores and other responsibilities, and attendance at scheduled in-house classes that are coordinated around other health care and social activities. Adherence to the facility rules results in more privileges within HUM.20,23
Integration of services post-redesign
Integrated service delivery was achieved using several approaches. Communication across disciplines was facilitated through a weekly meeting that included CAP, HUM, OB/GYN, and pediatrics staff. This meeting was supplemented by weekly medical rounds at CAP attended by clinical and administrative staff and weekly counseling supervision. Taken together, these meetings integrated care through ongoing development of the treatment plan, addressing emergent medical and psychiatric concerns, adjusting SUD or other treatment medications, intensifying (or reducing) the schedule of individual and group counseling services, coordinating referrals to outside social service agencies, and managing other issues relevant to the comprehensive care of patients. In addition to providing safe and secure housing, HUM provided and coordinated transportation to and from CAP, OB/GYN, and pediatric care, and delivered other social services and skills development programs at their facility to meet a wide range of patient needs and interests.
Measures
Exposure
The main exposure of interest was whether the pregnant person was enrolled in CAP after the redesign took effect on March 1, 2023. All people admitted to CAP before March 1, 2023, were assigned a zero (pre-redesign), and those admitted on or after March 1, 2023, were assigned a one (post-redesign). Table 1 presents a side-by-side comparison of services offered pre- and post-redesign. Those whose treatment crossed the pre- and post-redesign periods (n = 15) were removed from the analytical sample because they experienced aspects of both the pre-redesign and post-redesign programs. All persons in this analysis were unique. No one was included in the sample more than once, and no one was in both the pre- and post-redesign. We only included the most recent admission if someone was admitted more than once during their pregnancy.
Services Offered, Their Location, and Whether They Changed During Pre- and Post-Redesign Phases

SUD, substance use disorder; MOUD, medications for opioid use disorder; CAP, Comprehensive Addiction and Pregnancy program; JHBMC, Johns Hopkins Bayview Medical Center; FQHC, Federally Qualified Health Center; ASAM, American Society of Addiction Medicine.
Outcomes
Five outcomes of interest were examined: (1) total length of treatment in days (count), (2) treatment retention until delivery (yes/no), (3) treatment retention at 30-days postpartum (yes/no), (4) treatment retention at 60-days postpartum (yes/no), and (5) treatment retention at 90-days postpartum (yes/no).
For the length of treatment analysis, people who were still engaged in treatment and missing a discharge date at the time of data extraction (n = 7) were excluded from the analytical sample because the length of treatment could not be calculated without a discharge date. Of note, patients could be discharged from treatment due to a variety of reasons: completion of treatment, transfer to another treatment program, or patient-directed discharge. Additionally, if CAP patients become completely disengaged from treatment for 30 consecutive days, they are administratively discharged. Those who were admitted to CAP postpartum (n = 31) were removed from the analytical sample, as several variables (e.g., treatment retention until delivery) could not be calculated for this subgroup. Those whose length of treatment was less than or equal to 3 days (n = 17) were also removed from the analytical sample due to insufficient time to develop a treatment plan for engagement.
Covariates
Age (years), race and ethnicity (Black or person of color, non-Latinx White), educational attainment (less than high school, high school or higher), psychiatric diagnosis (yes/no), past 30-day nicotine use (no use, non-daily use, daily use), OUD (yes/no), stimulant use disorder (yes/no), sedative use disorder (yes/no), cannabis use disorder (yes/no), alcohol use disorder (yes/no), comorbid SUDs (e.g., two or more SUD diagnoses (yes/no)), gestational age at admission (weeks), unhoused at admission (yes/no), previous substance use treatment (yes/no), admission after Maryland House Bill 833 (yes/no), and admission during the COVID-19 pandemic state of emergency in Maryland (yes/no) were included as covariates in the final adjusted models.
The Maryland House Bill 833 “Parents in Substance Use Disorder Treatment—Children in Need of Assistance and Treatment Facilities” took effect on October 1, 2024. 24 This bill allows the children of parents who are receiving treatment for SUDs at a residential treatment program to stay with their parent for the duration of their parent’s treatment in circumstances when this is the best option for the child, 24 and impacted 7 of 64 patients in the post-design cohort. The COVID-19 pandemic state of emergency in Maryland ended on July 1, 2021, 25 and impacted 17 of 100 patients in the pre-design cohort. Collinearity was checked and ruled out between these two variables and the redesign phase. Employment status and marital status were not included in the adjusted regression models because most of the sample was unemployed and single.
Statistical analysis
Due to low levels of missingness on study variables (0.6 − 2.4%), we used complete case analysis, where records with missing values were excluded from the regression models. Descriptive analyses of demographics, outcome variables, and other covariates by redesign phase were performed using chi-square for categorical variables, Fisher’s exact test for categorical variables with small cell sizes, independent two-sample t-tests for normally distributed continuous variables, and Wilcoxon rank-sum test for continuous variables that are not normally distributed.
We used unadjusted and adjusted negative binomial regression analysis to calculate incidence rate ratios (IRR) to estimate associations between redesign phase and length of treatment because this count variable was overdispersed and right-skewed. 26
We used unadjusted and adjusted logistic regression analysis to calculate odds ratios (OR) to estimate associations between redesign phase and treatment retention until delivery and treatment retention at 30-, 60-, and 90-day postpartum (each outcome examined separately). We considered p values <0.05 statistically significant, and all tests were two-tailed. All analyses were conducted using Stata 18.0. 27
Results
Table 2 shows descriptive statistics of the study variables by redesign phase. The mean age of our sample was 30 years (SD = 5.1). Participants were primarily non-Latinx White (59.1%), unemployed (93%), and single and never married (87%). Most of our sample had a psychiatric diagnosis (92%), an OUD(76%), and comorbid SUDs (63%). The most common combination of SUDs among people who had comorbid SUDs was OUD and stimulant use disorder (82%). Among people who were admitted with an OUD, 94% received MOUD while at CAP (31% buprenorphine, 69% methadone). There were no differences in most of the demographic, social, and clinical variables between people admitted pre-redesign compared to post-redesign. Those who were admitted during the pre-redesign phase had a significantly higher gestational age compared to people admitted post-redesign (23.0 vs. 19.9 weeks, respectively, p value = 0.023). Additionally, people admitted pre-redesign had a lower proportion of sedative use disorders and cannabis use disorders compared to people admitted post-redesign (sedative: 4.0% vs. 17.2%, p value = 0.010; cannabis: 11.0% vs. 26.6%, p value = 0.010).
Sample Characteristics of Pregnant People Admitted to the Comprehensive Addiction & Pregnancy (CAP) Program by Redesign Phase
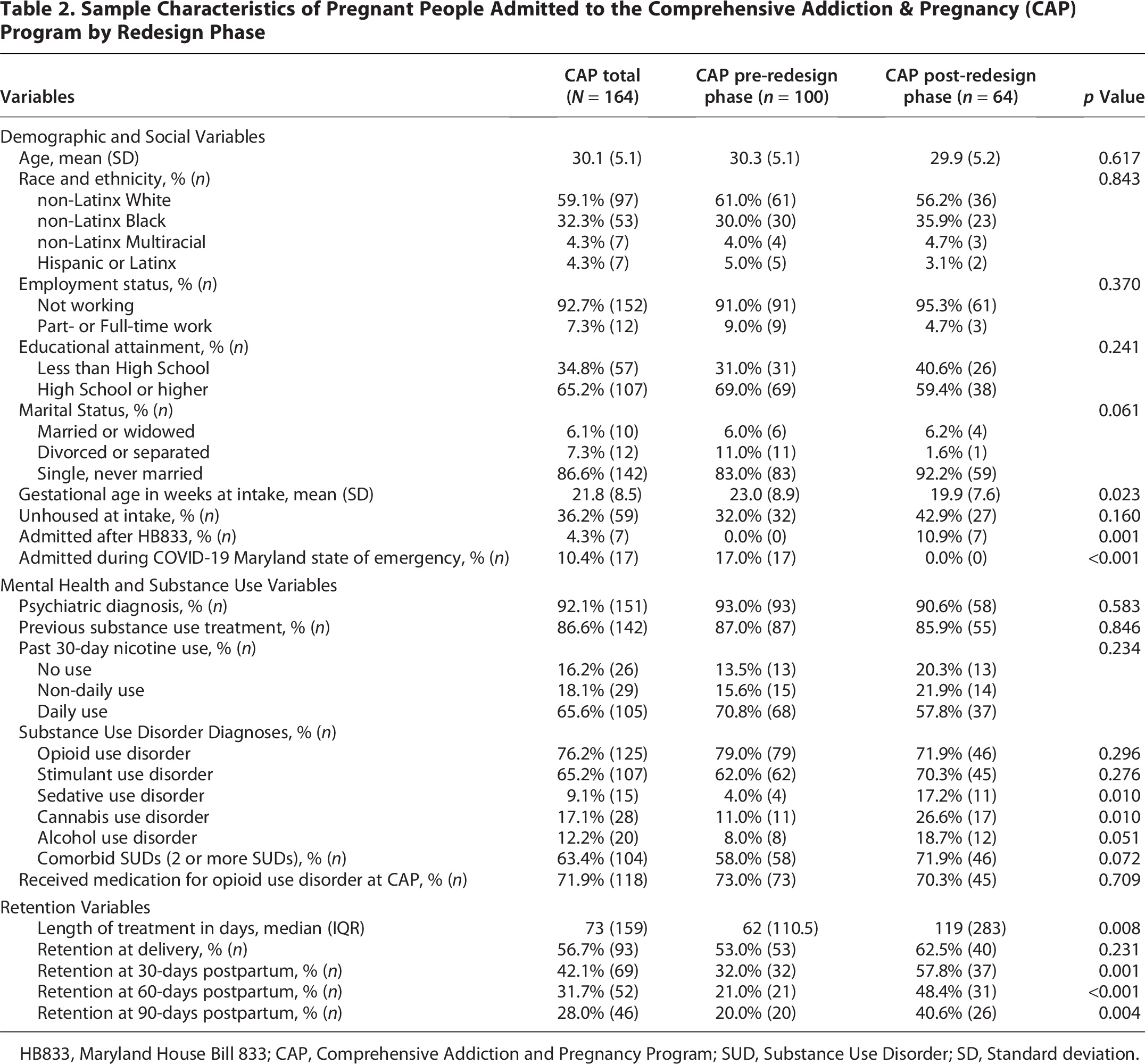
HB833, Maryland House Bill 833; CAP, Comprehensive Addiction and Pregnancy Program; SUD, Substance Use Disorder; SD, Standard deviation.
Table 3 shows unadjusted and adjusted negative binomial regression model results for length of treatment. In the adjusted regression model, pregnant people admitted during the post-redesign phase had a 108% increase in length of treatment days compared to pregnant people admitted pre-redesign (adjusted IRR [aIRR] 2.08, 95% CI: 1.40, 3.10). Figure 2 shows the predicted marginal count of days of treatment by redesign phase, adjusting for all covariates in the adjusted model. The predicted pre- plus post-delivery length of treatment for people admitted pre-redesign was 104 days and 217 days for people admitted post-redesign, a difference of 113 days.
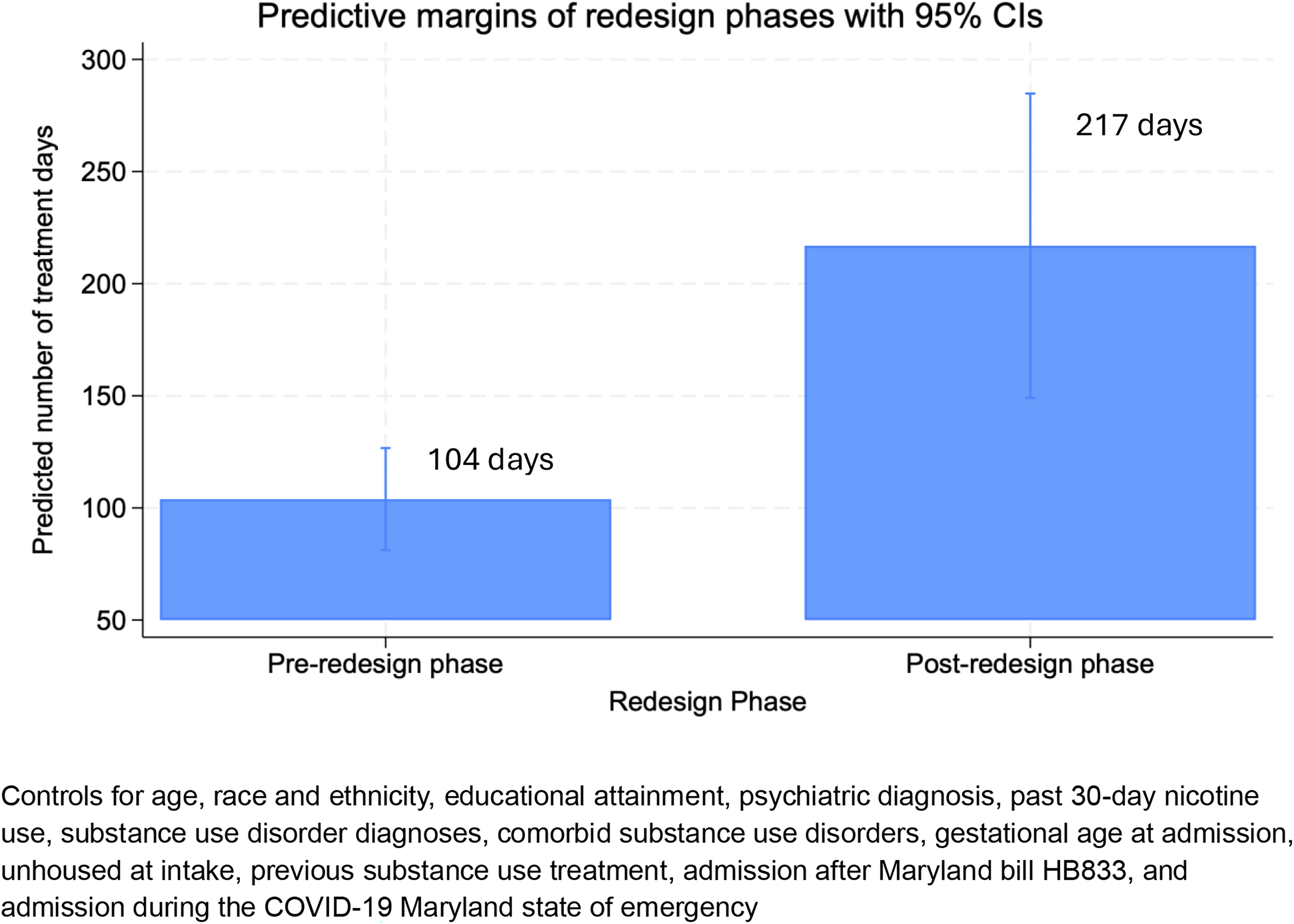
Predictive margins (n = 153).
Negative Binomial Regression Between CAP Redesign Phase and Length of Treatment

aPeople still engaged in treatment and missing a discharge date (n = 7) were excluded from the analytical sample.
bBlack or Person of Color includes people who identify as Black or African American (n = 53), Multiracial (n = 7), and Hispanic/Latinx (n = 7).
***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05.
HB833, Maryland House Bill 833; CAP, Comprehensive Addiction and Pregnancy Program; SUD, Substance Use Disorder.
Table 4 shows unadjusted and adjusted logistic regression model results for treatment retention until delivery. In the final adjusted model, the odds of staying in treatment until delivery were 3.53 times higher for pregnant people admitted post-redesign compared to pregnant people admitted pre-redesign (adjusted OR [aOR] 3.53, 95% CI: 1.39, 8.95).
Logistic Regression between CAP Redesign Phase and Retention Until Delivery

aBlack or Person of Color includes people who identify as Black or African American (n = 53), Multiracial (n = 7), and Hispanic/Latinx (n = 7).
***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05.
HB833, Maryland House Bill 833; CAP, Comprehensive Addiction and Pregnancy Program; SUD, Substance Use Disorder.
Table 5 shows unadjusted and adjusted logistic regression model results for treatment retention at 30-, 60-, and 90-days postpartum. In the final adjusted regression models, there was a significant difference in treatment retention at 30-, 60-, and 90-days postpartum between those admitted pre-design compared to those admitted post-redesign. Compared to people admitted pre-redesign, the odds of staying in treatment until 30 days postpartum were 6.58 times higher for people admitted post-redesign (aOR 6.58, 95% CI: 2.52, 17.16); the odds of staying in treatment until 60 days postpartum were 9.87 times higher for people admitted post-redesign (aOR 9.87, 95% CI: 3.47, 28.07); and the odds of staying in treatment until 90 days postpartum were 5.50 times higher for people admitted post-redesign (aOR 5.50, 95% CI: 1.98, 15.27).
Logistic Regression Between CAP Redesign Phase and Retention at 30-, 60-, and 90-Days Postpartum

aBlack or Person of Color includes people who identify as Black or African American (n = 53), Multiracial (n = 7), and Hispanic/Latinx (n = 7).
***p ≤ 0.001, **p ≤ 0.01, *p ≤ 0.05.
HB833, Maryland House Bill 833; CAP, Comprehensive Addiction and Pregnancy Program; SUD, Substance Use Disorder.
Discussion
The present study offered an opportunity for CAP to evaluate the benefits of partnering with a community-based facility (HUM) in efforts to retain and improve an integrated care approach for the treatment of perinatal people with severe forms of SUD. Following the dismantling of co-located care at CAP, HUM offered critical social services that may have resulted in improved SUD treatment retention. Results demonstrated that SUD treatment length increased by 108% for perinatal people admitted post-CAP redesign, and that they had markedly higher odds of treatment retention at delivery, 30-, 60-, and 90 days postpartum compared to those admitted pre-redesign.
Promoting postpartum retention is important because this period is a particularly vulnerable time for return to drug use, treatment attrition, and overdose among people who have SUDs.28,29 Longer treatment retention is associated with better long-term substance use outcomes, including decreased substance use30–32 and improved birth outcomes like reductions in preterm birth, low birthweight, neonatal mortality, and infant hospitalization stays.2,30 Our findings align with prior studies that have found integrated treatment programs are associated with a longer length of treatment compared to non-integrated programs that do not include services such as prenatal and pediatric care, 33 and demonstrate the success that can be achieved when an integrated program is partnered with a community organization. A key program detail that HUM provided after the redesign was that postpartum people were able to receive housing with their infant for up to one year after delivery. Prior to the redesign, the domiciliary unit did not allow children to reside with their parent, requiring postpartum people who continued to need housing services to find their own housing to continue at CAP, transfer to another SUD treatment program that offered housing services, or discontinue SUD treatment.
The CAP redesign highlights the potential implications of serving the underserved through a thoughtful reduction of traditional medical center resources and intentional inclusion of community members as an active partner in the transformation. This redesign represents the element of distributive justice, a core principle of health equity. The partnership with HUM maintained the legacy of coordinated SUD treatment, mental health, prenatal care, and pediatric care, while leveraging community-informed recovery services, amplifying solutions for transportation, unstable housing, and other critical social barriers to perinatal health. The trauma-informed and non-judgmental approach utilized by CAP and HUM providers likely reduced stigma and established stronger relationships between patients and providers. While spurred partially but financial circumstances, this partnership represents a significant step toward reimagining perinatal care by prioritizing health equity through integrated clinical and social services within a community-academic partnership and achieving a quality of care that neither the academic institution nor the community members could achieve independently. This partnership can serve as a blueprint for future perinatal SUD treatment programs to sustain and potentially augment SUD treatment and recovery services in an uncertain financial climate.
These support services were delivered within HUM’s highly structured living environment that required adherence to facility rules and restricted freedom of movement outside the facility during the initial phase of residency. Although factors associated with promoting good retention under these circumstances are not well understood, it is important to recognize the protective role that the perinatal period may have on substance use, 34 offering a window of time to capitalize on enhanced motivation. Future research might focus on understanding and examining barriers and facilitators for postpartum treatment retention, including novel community-informed methods and patient perspectives about programming.
Limitations and strengths
Our study sample came from one perinatal SUD program in Baltimore, Maryland, in partnership with a unique community-based program, and results may not generalize to other cities, treatment populations, or settings. We utilized an observational, retrospective cohort design, and causality cannot be inferred. There is also the potential for unmeasured confounders that explain the relationship between the CAP redesign and improved treatment retention. Due to data limitations, we could not examine other treatment outcomes, such as level of treatment engagement, substance use, or birth outcomes. Finally, we lacked measures to determine which components of the CAP redesign accounted for the improved retention outcomes.
Among the many study strengths include a moderately large sample of perinatal people receiving high-intensity SUD treatment, a creative integration of community-based clinical and social services, and a sound evaluation approach that accounted for multiple possible confounding variables. The study was conducted in an urban city that has experienced a large burden of overdose deaths in recent years.35,36 Study findings may generate new approaches for integrating services when co-located health care is neither possible nor feasible.
Conclusions
This observational study showed that the CAP redesign, which created a novel partnership with a community-based residential facility, was associated with improved SUD treatment retention pre- and post-delivery. These promising findings were achieved following the unfortunate dismantling of previously co-located services. Instead of eliminating or reducing services, CAP identified impending gaps in recovery services and maintained core SUD treatment at the Medical Center, filled these openings with a new community partner, and ultimately expanded the scope of integrated services offered to its patients. Our results add to a growing literature supporting the benefits of comprehensive and integrative care as best practices for the treatment of perinatal people with SUD.
Authors’ Contributions
L.A.M.: Conceptualization; methodology; formal analysis; writing-original draft. M.K.: Conceptualization; writing—review and editing; and supervision. J.D.E.: Conceptualization; writing—review and editing; E.C.S.: Writing—review and editing; H.A.T.: Writing—review and editing; D.G.A.—Conceptualization; writing—review and editing; and supervision.
Footnotes
Acknowledgments
The authors would like to thank Dana Madden, Eunyeong Joo, and Towanda Carr for their help with data verification and data procurement. They are also grateful to Helping Up Mission and the Addiction Treatment Service and Comprehensive Addiction and Pregnancy staff for all their work.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding Information
This work was supported by the