
Abstract
Introduction
Age-related macular degeneration (AMD) is one of the leading causes of irreversible blindness in the United States, affecting an estimated 15 million people older than 40 years of age. 1 Risk factors include age, genetics, smoking, and systemic vascular conditions. 2 Hypoxia, oxidative stress, autophagy, and chronic local inflammation have been implicated in the development of AMD. 3 Given the vision-threatening consequences of AMD, the identification and treatment of its modifiable risk factors are highly relevant. 4
Sleep is a key modifiable lifestyle factor, influencing both physiologic and psychologic health. 5 Obstructive sleep apnea, a disorder characterized by recurrent upper airway obstruction during sleep, contributes to systemic hypoxia, oxidative stress, and vascular dysregulation. Sleep disorders are increasingly recognized for their systemic adverse effects, including cardiovascular, 6 metabolic, and neurovascular health, which also contribute to neuroinflammatory and neurodegenerative conditions such as Alzheimer disease.7–9
Studies have suggested links between sleep disorders and ocular diseases such as cataract, primary open-angle glaucoma, and AMD. 10 Despite growing interest in the systemic consequences of poor sleep, its potential role in ocular health—particularly in relation to AMD—remains poorly understood. Emerging evidence has linked obstructive sleep apnea with retinal disease, including diabetic retinopathy (DR) and central serous chorioretinopathy, but its association with AMD remains underexplored. 10 In this study, we aimed to elucidate the impact of obstructive sleep apnea on AMD incidence through a population-based approach. We also studied the potential effect of obstructive sleep apnea in different AMD subtype distribution, sex, age of onset, and intravitreal (IVT) treatment patterns.
Methods
This retrospective cross-sectional study was conducted using the Epic electronic health record (EHR) system at the University of Miami from January 1, 2020, to July 30, 2025. All data were de-identified before extraction and analysis. The institutional review board approved the study, which adhered to the tenets of the Declaration of Helsinki.
Eligible patients were aged 50 years or older and had International Classification of Diseases (ICD)–coded diagnoses of AMD or obstructive sleep apnea. Patients with DR or retinal vein occlusion were excluded when analyzing IVT injections to minimize confounding by other retinal vascular pathologies.
Patients were divided into 2 groups: those with and those without obstructive sleep apnea. Patients with AMD, including all subtypes as defined by the Epic database, were identified in each group. Patients were then stratified into mutually exclusive categories (exudative, nonexudative, or both) and further categorized into advanced disease stages, defined as exudative AMD with inactive scar and advanced nonexudative AMD with subfoveal involvement.
The primary outcome of the study was the prevalence of AMD among patients with and without obstructive sleep apnea. Secondary outcomes included AMD subtype distribution, progression to end-stage disease, sex and age distribution among patients with AMD stratified by obstructive sleep apnea status, and IVT injection use.
Age was extracted in categorical bands (50–65, 65–80, 80–100, and ≥100 years). For continuous analysis, bin midpoints (57.5, 72.5, 90, and 100 years) were applied and expanded by frequency counts to approximate mean and median ages. Sex distribution and AMD subtype classification were directly obtained from the EHR.
Statistical Analysis
Comparisons of prevalence, AMD involvement, and IVT injections between groups were performed using Fisher exact test. Chi-square tests were applied to evaluate categorical variables, including age-band distributions. Approximate mean and median ages were compared using the Mann-Whitney U test. Logistic regression was performed to assess sex as a predictor of obstructive sleep apnea status among patients with AMD, with odds ratios (ORs) and 95% CIs reported. All analyses used 2-sided significance testing with a threshold of P < .05. Statistical analyses were conducted using Python (version 3.10) with the SciPy and Statsmodels libraries.
Results
A total of 43 846 individuals with a diagnosis of obstructive sleep apnea and 2 371 245 individuals without obstructive sleep apnea (control group) aged 50 years or older were included in the study. The prevalence of AMD was significantly higher in the group with obstructive sleep apnea compared with the control group (1.996% vs 1.023%; OR, 1.97; P < .001) (Table 1).
Prevalence and Age of Patients With AMD by Obstructive Sleep Apnea Status.

Abbreviation: AMD, age-related macular degeneration.
The mean age (approximate, based on age-band midpoints) was 80.8 years in the group with obstructive sleep apnea and 84.9 years in the control group (P < .001). The median age was 90 years in both groups, which is an approximation based on categorical age bins rather than the actual median age (Figure 1). Patients with nonexudative AMD and obstructive sleep apnea were statistically significantly younger compared with the control patients (P < .001).
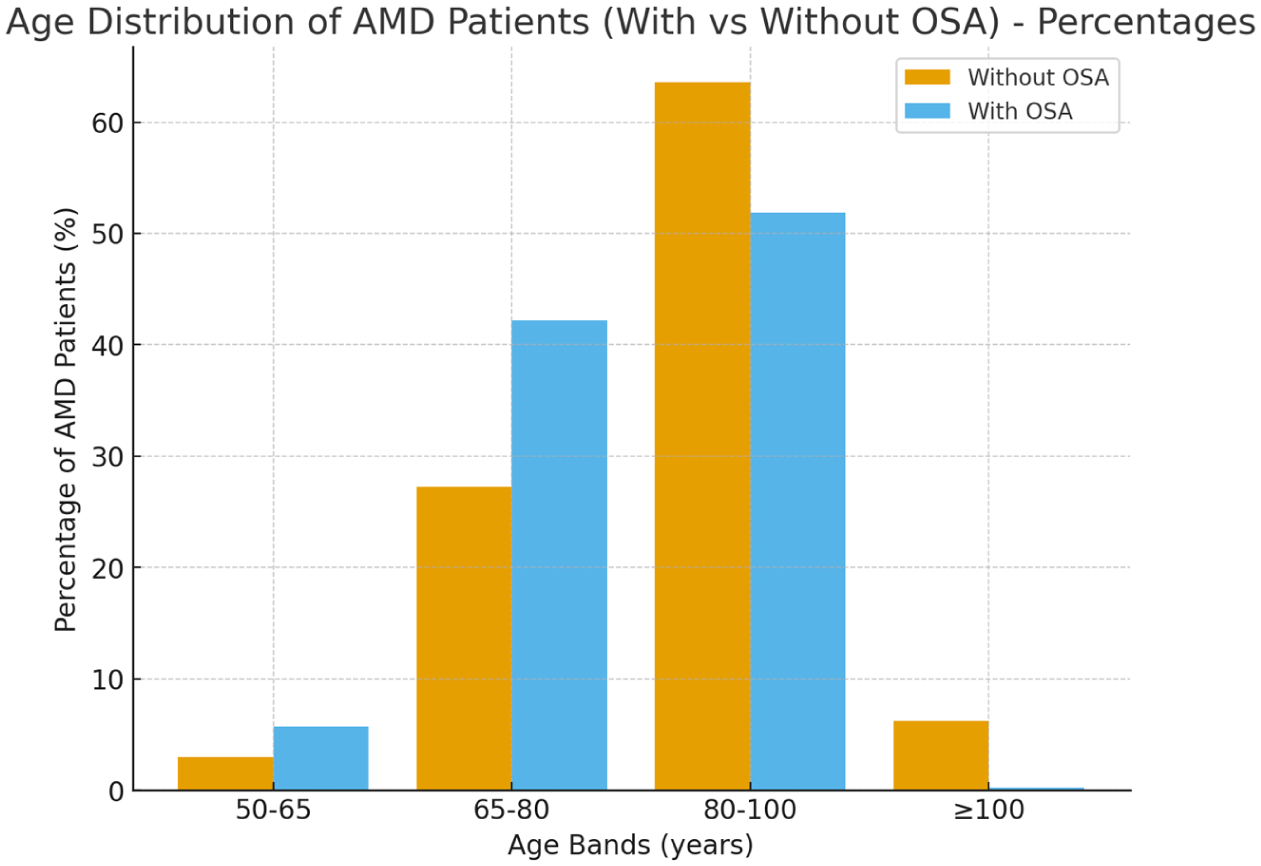
Age distribution of patients with age-related macular degeneration (AMD) with and without obstructive sleep apnea, expressed as percentages within each group. Bars represent the proportion of patients falling into age bands 50 to 65, 65 to 80, 80 to 100, and older than 100 years. Patients without obstructive sleep apnea are shown in orange, and patients with obstructive sleep apnea are shown in blue.
When stratifying patients with AMD by sex, significant disparities were observed between the group with obstructive sleep apnea and the control group. Men comprised 56.2% of patients with AMD in the group with obstructive sleep apnea, compared with 40.5% men in the control group (P < .0001).
Compared with control patients, both exudative and nonexudative AMD were more common among patients with obstructive sleep apnea. Exudative AMD occurred in 0.9% of patients with obstructive sleep apnea vs 0.5% of control patients (OR, 1.71; P < .001), while nonexudative AMD occurred in 1.1% of patients with obstructive sleep apnea vs 0.8% in control patients (OR, 1.47; P < .001). When subcategorized into mutually exclusive groups (nonexudative only, exudative only, or both), distribution differences remained significant (P < .001) (Table 1).
Rates of exudative end-stage AMD (inactive scar formation) did not differ significantly between patients with obstructive sleep apnea and the control group (11.3% vs 8.7%; OR, 1.34; P = .098). However, nonexudative end-stage AMD (subfoveal involvement) was significantly less common in the group with obstructive sleep apnea compared with the control group (7.7% vs 13.8%; OR, 0.52; P < .001) (Table 2).
End-Stage AMD Outcomes by Obstructive Sleep Apnea Status.

Abbreviation: AMD, age-related macular degeneration.
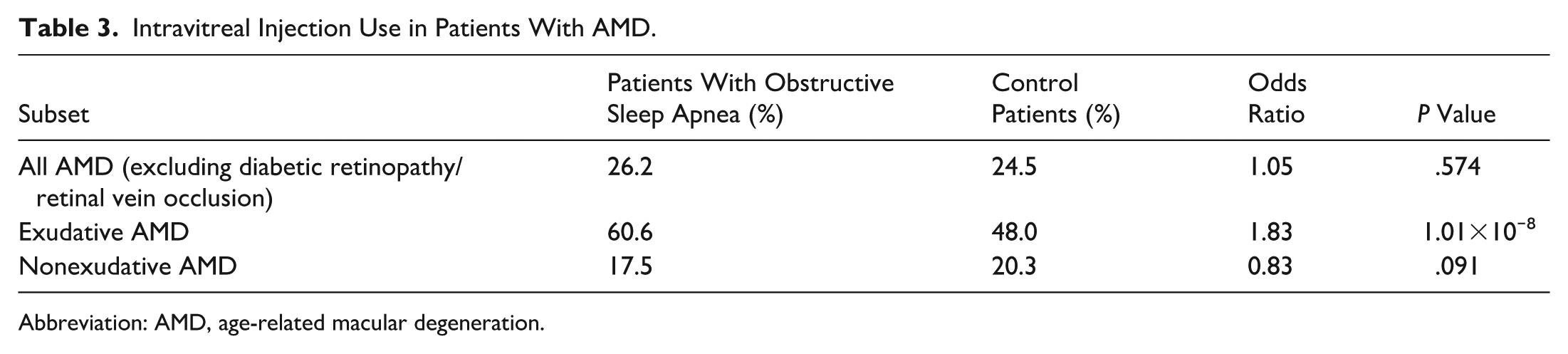
Patients with exudative AMD and obstructive sleep apnea received IVT injections significantly more frequently compared with control patients (60.6% vs 48.0%; OR, 1.83; P < .001) (Table 3).
Intravitreal Injection Use in Patients With AMD.
Abbreviation: AMD, age-related macular degeneration.
Conclusions
Obstructive sleep apnea is a systemic disorder characterized by recurrent upper airway obstruction during sleep, resulting in intermittent hypoxia and sleep fragmentation. These physiologic disturbances have been implicated in widespread vascular and metabolic dysfunction, and the potential ocular consequences have increasingly become an area of clinical and scientific interest. In this large, retrospective analysis, we identified a higher prevalence of AMD among patients with obstructive sleep apnea compared with control patients, supporting the hypothesis that obstructive sleep apnea is associated with altered macular health and may contribute to AMD expression.
Our findings align with multiple epidemiologic studies demonstrating increased AMD risk in individuals with obstructive sleep apnea. 11 A Taiwanese cohort reported a 1.36-fold increased risk among patients with obstructive sleep apnea, 12 while long-term follow-up in the UK Biobank and the Canadian Longitudinal Study on Aging each showed a risk ratio of 1.39. 13 Similarly, a UK National Health Service database analysis found a rate ratio of 1.44 for AMD among those patients with obstructive sleep apnea. 14 More recently, analysis of TriNetX Health Research Network showed that patients with obstructive sleep apnea were 2.64 times more likely to develop nonexudative AMD and 2.48 times more likely to develop exudative AMD; in addition, they were also 2.85 times more likely to require IVT antivascular endothelial growth factor therapy. 15 Untreated obstructive sleep apnea, confirmed by polysomnography, was associated with an even higher likelihood of both AMD and treatment burden. 15 Although our effect sizes were more modest, the consistency of direction across studies reinforces the robustness of this association.
Among patients with AMD, men represented a greater proportion in the cohort with obstructive sleep apnea relative to controls (56.2% vs 40.5%). Because the total sex distribution of both source populations was not extracted, this proportional difference cannot be interpreted as a sex-specific AMD risk. However, this male predominance is consistent with trends described in other datasets, including the TriNetX-based study that reported a higher proportion of men among patients with AMD with obstructive sleep apnea compared with the control group. 15 These findings should therefore be interpreted descriptively.
Our dataset also provides additional clinically relevant observations. Patients with obstructive sleep apnea appeared to present with AMD at a younger age than those without. Although causal inference is limited by our study design, chronic intermittent hypoxia and oxidative stress may accelerate phenotypic expression among susceptible individuals. Interestingly, although overall likelihood of nonexudative AMD was higher in patients with obstructive sleep apnea, fewer individuals in the cohort had nonexudative end-stage disease. This discrepancy may reflect competing systemic mortality or earlier conversion to exudative disease.
Our analysis of IVT injection administration showed significantly more frequent injections among patients with exudative AMD and obstructive sleep apnea compared with controls. The overall proportion of patients with exudative AMD receiving IVT injections was lower in our study (60.6% in patients with obstructive sleep apnea vs 48.0% in control patients) and the previously published EHR-based study, 15 compared with 78% reported in the literature. 16 Although patients with DR, retinal vein occlusion, and nonexudative AMD were excluded from injection analyses to reduce attribution bias, these exclusions are unlikely to explain the magnitude of under-representation. Therefore, the lower observed treatment rate is attributable primarily to EHR coding and ascertainment limitations rather than true undertreatment.
Multiple biologic mechanisms have been proposed to explain the association between obstructive sleep apnea and AMD. Intermittent hypoxia induces oxidative stress, mitochondrial dysfunction, and inflammatory cascades, which promote retinal microglial activation and neuronal injury.12,16 Hypoxia-driven apoptosis of retinal ganglion cells has been linked to thinning of the retinal nerve fiber layer. 12 Furthermore, nocturnal oxygen desaturation has been specifically associated with increased risk of neovascular AMD. 11 At the choroidal level, obstructive sleep apnea–related hypoxia and hypercapnia may alter vascular tone, permeability, and perfusion dynamics, contributing to retinal pigment epithelium (RPE) dysfunction. Given the essential role of the RPE in photoreceptor metabolism and immune homeostasis, oxidative vulnerability of RPE cells is a plausible mechanistic bridge between obstructive sleep apnea and progression of AMD.11,12
Several limitations of this study must be acknowledged. The retrospective design and reliance on ICD coding introduce potential diagnostic misclassification. Key AMD-related covariates, including smoking status, hypertension, vascular disease, and nutritional or genetic risk factors, were unavailable, and residual confounding cannot be excluded. Finally, obstructive sleep apnea treatment status (eg, adherence to continuous positive airway pressure treatment) was not captured, which prevents the evaluation of whether treatment modifies AMD risk or outcomes.
Despite these constraints, the large sample size, statistically consistent findings, and alignment with previous epidemiologic studies strengthen the validity of our results. Collectively, these observations underscore the relevance of sleep-disordered breathing within ophthalmic care and highlight the importance of interdisciplinary patient management. To our knowledge, this is the first single-center EHR analysis to describe earlier onset of AMD and a lower frequency of nonexudative end-stage AMD in patients with obstructive sleep apnea.
In conclusion, AMD was approximately twice as prevalent among patients with obstructive sleep apnea compared with those without. These findings support targeted ophthalmologic evaluation in individuals diagnosed with sleep apnea to facilitate earlier detection of macular disease and timely therapeutic intervention, which could result in decreased treatment burden and better long-term visual outcomes. 17 Prospective longitudinal studies are needed to determine whether treatment of obstructive sleep apnea alters AMD incidence, progression, or conversion to advanced disease.
Footnotes
Acknowledgements
The authors thank the staff of the Bascom Palmer Eye Institute for their assistance in data collection and statistical analysis.
Ethical Considerations
This study adhered to the tenets of the Declaration of Helsinki and received approval from the institutional review board (IRB) of the University of Miami.
Consent to Participate
Because this retrospective study used de-identified patient data, the requirement for individual patient consent was waived by the IRB.
Funding
The research was supported by Research to Prevent Blindness Unrestricted Grant GR004596-1 (institutional).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon request.