
Abstract
Introduction
Dislocated intraocular lenses are commonly encountered in ophthalmic practice. Some studies have reported a prevalence ranging from 0.05% to 3% following cataract surgeries in patients aged over 40 years.1,2 Intraocular lens dislocation most commonly occurs in the setting of complex prior surgery, pseudoexfoliation syndrome, or trauma, although apparently spontaneous dislocations are also common.3–9 Observation may be a suitable initial management strategy, especially in cases of tolerable visual symptoms. However, more advanced cases have been associated with higher rates of cystoid macular edema (CME), uveitis–glaucoma–hyphema syndrome, corneal endothelial loss, vitreous hemorrhage, and other complications.3,10 In addition, a dislocated or decentered intraocular lens may cause visual symptoms that might not be adequately captured by Snellen visual acuity (VA) measurements, including glare, halos, shadows, postural VA fluctuations, or monocular diplopia, all of which impair activities of daily living.
Surgical management options for these patients include intraocular lens removal with correction of aphakia using contact lenses, intraocular lens exchange, or lens refixation/repositioning. 11 Aphakia is generally the least attractive option, especially in elderly patients. Intraocular lens exchange is a viable option, especially in specific circumstances or with certain intraocular lens designs; however, it may be associated with longer operating times, additional patient costs, and a higher risk of corneal complications due to the additional surgical manipulation required both for removing the intraocular lens and inserting another lens with an appropriate fixation method, particularly in eyes with preexisting corneal endothelial insufficiency.
The anterior incisions and anterior chamber “traffic” associated with intraocular lens exchange increase the risk of endothelial cell loss. 10 Certain techniques, such as bisecting the intraocular lens before removal, may mitigate the exacerbation of corneal endothelial loss. These concerns are especially relevant in eyes with marginal corneal endothelial function, anterior synechiae, or previous glaucoma surgery, including the presence of a glaucoma drainage device.
Scleral suture fixation for intraocular lens repositioning has been described for several decades and is best suited for 3-piece intraocular lenses, although repositioning techniques for several other intraocular lens types have also been reported.11,12 Successful scleral suture fixation requires a haptic design that either has holes, a notch at the haptic–optic junction, or increased distal haptic thickness to avoid the haptic from slipping out of the suture loop. Consequently, some intraocular lens designs have traditionally been unsuitable for scleral suture-based repositioning techniques.
The present study reports intraocular lens refixation in 3 cases with intraocular lens designs that have not been manageable with scleral suture fixation and would otherwise require intraocular lens exchange.
Methods
Three consecutive cases of dislocated intraocular lenses with haptic designs lacking eyelets, notches, or reverse-tapered haptics were encountered. Comprehensive preoperative and postoperative ophthalmic examinations included best-corrected visual acuity (BCVA), intraocular pressure measurement, slitlamp examination, and dilated fundus examination. All cases were performed by a single surgeon at a single institution and involved intraocular lens refixation using scleral sutures with a modified surgical technique. Each case also had extenuating factors that favored avoidance of intraocular lens exchange, including prior Descemet stripping automated endothelial keratoplasty, pseudoexfoliation glaucoma with corneal edema and a capsular tension ring, and a desire to preserve the optical benefits of an extended-depth-of-focus intraocular lens. These factors motivated rescue and refixation of the existing intraocular lens rather than exchange with a new lens.
Surgical Technique
The procedure was initiated with a standard 23-gauge 3-port pars plana vitrectomy. A core vitrectomy was performed, and a preexisting posterior vitreous detachment was confirmed or induced. The vitreous was then trimmed back to the vitreous base. The conjunctiva was opened at the 2 o’clock and 8 o’clock meridians, and limbal-based partial-thickness triangular scleral flaps were fashioned, with the base positioned 1 mm posterior to the limbus and the apex extending 4 mm posterior to the limbus. The dislocated intraocular lens was retrieved and brought to the anterior vitreous. While grasping the dislocated intraocular lens with 23-gauge forceps, a 9-0 polypropylene suture prethreaded through a 27-gauge needle was passed through the partial-thickness scleral flap 3 mm posterior to the limbus. The threaded needle was pierced through the base of the haptic (Figure 1A). The suture was grasped using the 23-gauge forceps (Figure 1B) and transferred using a “handshake” maneuver to a second 25-gauge forceps inserted through a separate scleral stab incision within the partial-thickness scleral flap, located 1 mm anterior to the needle insertion site (Figure 1C).
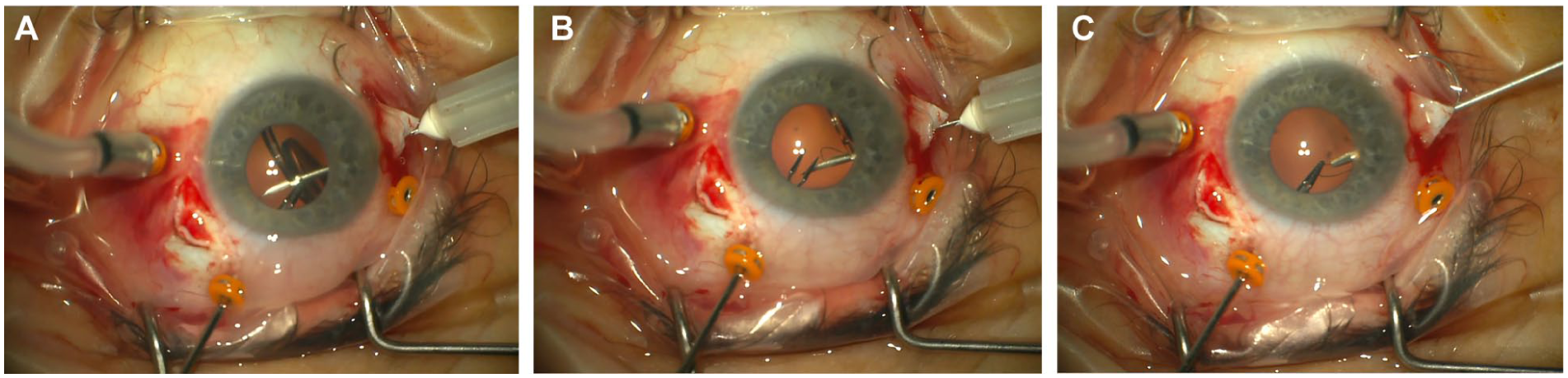
Surgical steps demonstrating the modified scleral fixation technique for a dislocated ASPIRA-style intraocular lens. (A) A prethreaded needle pierces the flat portion of the haptic. (B) After haptic penetration, the suture is grasped from the prethreaded needle using the first intraocular forceps. (C) A second intraocular forceps, introduced through a sclerotomy adjacent to the original needle entry site, grasps the suture from the first forceps and externalizes both suture ends.
These steps were repeated on the other side of the eye to secure the other haptic. The externalized suture ends were then tied, with the suture tension adjusted to ensure appropriate centration of the intraocular lens. The conjunctiva was closed using 6-0 plain gut sutures, while the scleral flaps were left unsutured.
Case Descriptions
Case 1
A 78-year-old woman presented with vision loss after she was hit by a tennis ball. BCVA was eccentric viewing at 2 feet, intraocular pressure was normal, and the intraocular lens was dislocated inferiorly. The intraocular lens was an ASPIRA lens (Human Optics), a 1-piece acrylic intraocular lens without haptic holes and having a constant haptic width. As the lens was designed to provide enhanced depth of focus, the patient was motivated to avoid intraocular lens exchange.
At postoperative month 3, uncorrected BCVA was 20/20. At the most recent follow-up examination, 26 months postoperatively, uncorrected VA remained 20/20 without astigmatism. The patient used +1.50 diopter reading glasses to achieve J1 near vision. The intraocular lens remained well centered without any tilt.
Case 2 (See Supplemental Video File)
A 74-year-old woman with pseudoexfoliation glaucoma presented with spontaneous loss of vision in her right eye. VA was 20/150, and intraocular pressure was 41 mm Hg despite treatment with latanoprost and prior placement of an iStent at the time of cataract extraction. Microcystic corneal edema was present. The intraocular lens was mobile and demonstrated endocapsular subluxation with a capsular tension ring in the residual capsular bag. Intraoperatively, the intraocular lens was identified as an ASPIRA-style lens (as in Case 1). The lens bag complex was removed to expose the intraocular lens, and scleral fixation was performed using the technique described above. The capsular tension ring was retrieved by grasping one end with 23-gauge forceps and removing it through the trocar during withdrawal.
At 5 months after intraocular lens repositioning, uncorrected VA had improved to 20/25, which represented the patient’s baseline VA before the dislocation, as she had not required glasses previously. Uncorrected near vision was J2. No apparent intraocular lens tilt was observed. As intraocular pressure remained elevated despite maximal medical therapy, the patient subsequently underwent implantation of a glaucoma device (Baerveldt). Two months after Baerveldt placement, the glaucoma consultant recorded a VA of 20/30, with an intraocular pressure of 12 mm Hg.
Case 3 (See Supplemental Video File)
A 77-year-old woman with pseudoexfoliation glaucoma presented with loss of vision in her right eye shortly after undergoing back surgery and subsequent physical therapy. Preoperative VA was counting fingers, and intraocular pressure was normal. The intraocular lens was dislocated posteriorly and was identified as an Akreos MI60 lens (Bausch + Lomb), characterized by 4 short haptic protrusions without haptic holes. Two diametrically opposite haptic tabs were pierced using the technique described above, allowing scleral refixation of the intraocular lens. Postoperatively, the intraocular lens was well centered without evidence of tilt. At 3 months, uncorrected VA improved to 20/25. The patient had not required glasses preoperatively, and no postoperative astigmatism was noted.
Conclusions
This case series demonstrates a modification of the standard scleral suture technique for rescuing dislocated intraocular lenses that have traditionally not been considered amenable to rescue procedures. Each of these cases had extenuating circumstances that made repositioning a more favorable option than intraocular lens exchange.
Scleral suture fixation for intraocular lens refixation has been well described and is most widely used with 3-piece intraocular lens designs.9,12 Previously, variations in this technique have been described for other intraocular lens types, such as 1-piece acrylic lenses (SN60-style; Alcon), Akreos-style intraocular lenses with holes in the 4 short haptics (Bausch + Lomb), Symfony-style intraocular lenses with notches at the haptic–optic junction (Tecnis), plate-haptic intraocular lenses, intraocular lenses with holes at the haptic–optic junction, and Crystalens models with large T-shaped haptics (Bausch + Lomb). These modifications have relied on threading sutures through the holes, looping sutures around proximal haptic notches, or placing the loop at the thinner portions of haptic segments to secure the suture to the haptic before scleral fixation. In contrast, dislocated intraocular lenses lacking these haptic designs have historically required intraocular lens exchange for surgical management.
The key modification in this technique involves piercing a portion of the haptic with a polypropylene-threaded needle and retrieving the suture with a second forceps through a sclerotomy adjacent to the insertion point of the needle to allow scleral suture fixation. The “handshake” technique has previously been reported for 1-piece intraocular lenses in which the suture is passed through the holes in a plate haptic or through openings at the optic–haptic junction. 13 A similar handshake technique has also been reported to rescue dislocated Akreos intraocular lenses using 4-point scleral fixation. 14
A similar technique has previously been described in which an intraocular lens punch, such as a Kelly punch, was used to create holes in haptics without preexisting holes. 15 However, this approach is not a closed-system maneuver, as it necessitates the creation of a corneal incision to introduce the punch instrument and additional manipulation within the anterior chamber. These steps may be avoided with the piercing-lasso technique described in the present study.
This management approach does not require the implantation of another intraocular lens, which may be particularly important for patients who have previously paid for a premium intraocular lens, as was the case for 2 patients in this series. In the authors’ experience, this technique may provide a more cost-effective and less invasive procedure alternative to intraocular lens exchange. However, shorter operation duration was not observed in a head-to-head randomized controlled trial of repositioning vs intraocular lens exchange performed by a single surgeon in a tertiary care hospital. 21
Other benefits of intraocular lens rescue include smaller changes to astigmatism, less trauma to the cornea, and faster recovery to BCVA.10,16 A less invasive procedure may also help avoid substantial worsening of other preexisting conditions, such as compromised corneal endothelium, anterior synechia, or glaucoma, which would likely be exacerbated by intraocular lens exchange.17–19 One retrospective study reported higher rates of vitreoretinal complications, including retinal detachment, choroidal effusion, and secondary epiretinal membranes, after intraocular lens exchange compared with refixation. 20 Iris chafing leading to CME and the so-called “new” uveitis–glaucoma–hyphema syndrome have been described following both intraocular lens repositioning and exchange, as well as after primary cataract surgery. These complications are more likely to occur when the intraocular lens is tilted or if the patient has taken tamsulosin.17,19,21 In addition, 1 meta-analysis demonstrated a lower incidence of CME following intraocular lens repositioning compared with intraocular lens exchange. 22
Another study evaluating sutureless intrascleral fixation techniques, including both intraocular lens rescue and exchange cases, demonstrated a postoperative redislocation rate of 17%. 23 In comparison, the present authors’ published experience with redislocation after scleral fixation of more standard intraocular lenses was approximately 6%, although this has not been recently tabulated. 8 More studies with longer follow-up are required to further assess these differences.
In conclusion, this modification of the scleral fixation technique provides an additional option for individualized management of intraocular lens dislocations in eyes with haptic designs that have traditionally not been amenable to rescue procedures. In selected cases, this approach might preserve the advantages of the existing intraoperative lens and avoid exacerbation of preexisting ocular conditions.
Supplemental Material
Supplemental Material
Footnotes
Ethical Considerations
Institutional ethical approval was not required for this report of 3 individual cases.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.