
Abstract
Background
Burning mouth syndrome (BMS) is an orofacial pain syndrome where patients have chronic pain without a clear underlying lesion or cause. This can significantly impair patients’ quality of life, and no definitive treatments exist at this time.
Case
The case presented here describes a case of BMS with symptom resolution after starting galcanezumab. The patient was a 60-year-old female with recently diagnosed systemic lupus erythematosus and Sjögren’s disease who was first seen by neurology for chronic migraine, but on subsequent visit noted a burning sensation of her tongue as well as extremity paresthesias. The orofacial pain was found to be consistent with BMS based on International Classification of Headache Disorders 3rd Edition (ICHD-3) criteria after workup for this and her other symptoms. The migraine was first treated with metoprolol, but when this was unsuccessful, she was switched to galcanezumab. After starting this, the BMS symptoms resolved, and on continued follow up it was noted that when she delayed receiving galcanezumab the symptoms did return until she took the medicine again.
Conclusion
This case expands our understanding of BMS by demonstrating a potential relationship between migraine and BMS. This relationship can help us understand the pathophysiology and potentially reveal new treatment options for this syndrome.
This is a visual representation of the abstract.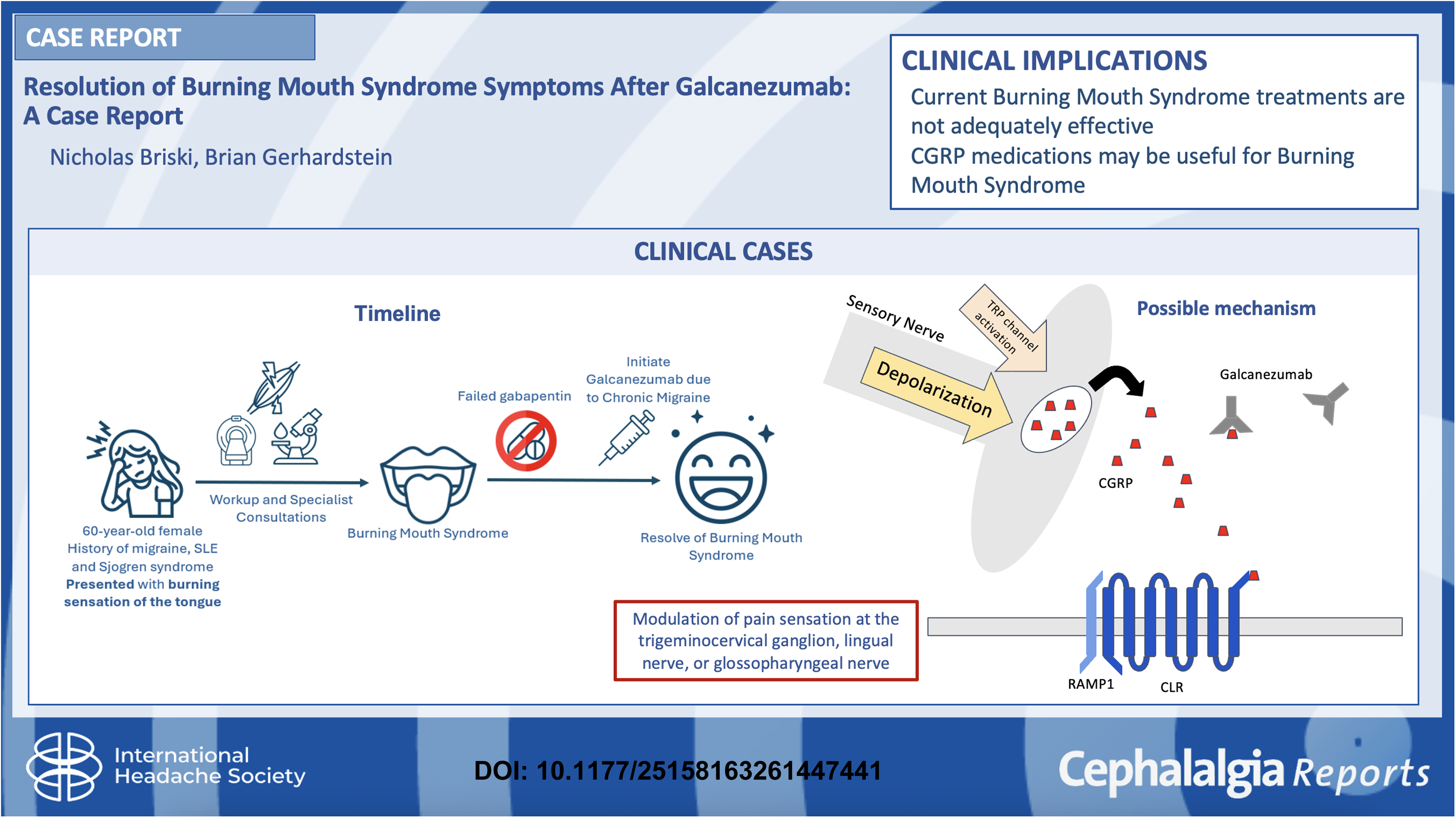
Introduction
Burning mouth syndrome (BMS) is a pain disorder characterized by severe chronic orofacial pain. As defined by the International Classification of Orofacial Pain from 2020, it is “idiopathic orofacial pain with intraoral burning or dysesthesia recurring daily for more than 2 hours per day and more than 3 months, without any identifiable causative lesions” and may occur with or without sensory changes. 1 Though the ICHD-3 criteria require the pain to be described as burning, recent proposals suggest that broader descriptors of dysesthetic symptoms should be included in the future. 2 The descriptions of pain can vary, but commonly “burning” in quality, lasts for years, and involves the tongue and soft palate. The exact etiologies and mechanisms are still under investigation, but prior studies show involvement of the lingual nerve, chorda tympani, and glossopharyngeal nerve. 3 The worldwide prevalence of BMS is 1.73% of the general population with the greatest prevalence in females over the age of 50 and in European countries. 4
Especially since this is often a diagnosis made by excluding other disorders, requiring additional testing and specialist evaluations, it poses a significant cost to both the patient and healthcare system. Further, the chronicity of these intrusive symptoms and the relatively low efficacy of current treatments can deteriorate the patient's quality of life, as evidenced by increased rates of depression, decreased appetite, and mood changes. 5
Though there is no definitive cure for BMS, many treatments are used to ameliorate symptoms. A recent meta-analysis assessed the use of available treatments, which fall into categories of anticonvulsants, antidepressants, phytomedicines, saliva substitutes, laser therapy, transcranial magnetic stimulation, oral devices, and cognitive behavioral therapy. 6 The analysis had limitations such as studies with small sample sizes and limited data on prolonged treatment courses, and though some were effective at reducing symptoms partially none of the treatments studied achieved the target of 50% pain remission. Among the more effective long-term treatments included clonazepam, cognitive behavioral therapy, and topical capsaicin, as well as phytomedicines for short-term pain symptoms. Others, such as trazodone, hypericum perforatum, alpha lipoic acid were either minimally effective or limited by side effects. Additionally, as additional treatments are explored our understanding of the underlying disease process grows. For example, the efficacy of cognitive therapy for BMS suggests that there may also be underlying psychological factors affecting the disease course. 7
Galcanezumab is a monoclonal antibody targeting calcitonin gene-related peptide (CGRP) and is used in the treatment of chronic migraine headache. 8 CGRP is a molecule released at the trigeminocervical complex, which is believed to modulate the sensation of pain in migraine headache. Galcanezumab is dosed as a monthly subcutaneous injection, and though it is typically tolerated very well the most common adverse effects include injection site symptoms and sinusitis. While it is primarily used for treatment of chronic migraine, there is also some evidence for its efficacy with episodic cluster headache through the same CGRP mechanism. 8 This case report seeks to describe a case where starting galcanezumab was temporally associated to resolution of BMS, suggesting an underlying connection between migraine and BMS and new possibilities for treatments to investigate.
The CARE case report guidelines checklist was utilized in the writing of this report to ensure adequate information and organization throughout the report. 9
Case presentation
A 60-year-old female patient with a history of chronic migraine, gastroesophageal reflux disease (GERD), systemic lupus, and Sjögren’s disease seen in the general neurology clinic for numbness and paresthesias in her legs as well as a burning sensation of her tongue. The tongue burning started 6 months prior to presentation, near the same time that she was diagnosed with lupus and had transitioned from prednisone to hydroxychloroquine. Regarding her history of migraine, she was recently seen in headache subspecialty clinic and had tried metoprolol for prevention, which was unsuccessful.
The pain involved the whole tongue, occurring in daily episodes lasting hours at a time without any identified trigger, and with mild improvement after taking ibuprofen, acetaminophen, and diazepam but no improvement with gabapentin. The pain was not worsening over time, not temporally associated with her typical migraine, and there was no change in the sense of taste. No oral or mucosal abnormalities were identified on physical exam, and no evidence of deficits with cranial nerves, motor strength, sensation, coordination, or gait. The leg numbness and paresthesias were a separate complaint; this symptom had started many years prior to this presentation, involving both legs in a distal, symmetric pattern following a “glove and stocking” distribution. It was not typically painful and improved with ambulation. She was already taking gabapentin 200 mg three times daily. The patient initially agreed to try increasing her gabapentin dose to 300 mg three times daily, and workup was obtained both for these symptoms and others that she noted.
For the sensory symptoms in the mouth and legs, labs and EMG were completed. Serology including Complete Blood Count Comprehensive Metabolic Panel, C-reacrive protein, B12, folate, and urinalysis were unremarkable. Electromyography with nerve condition study showed mild decrease in amplitude of the right superficial peroneal nerve but otherwise no evidence of large fiber neuropathy, denervation, myositis, or myopathy. Recent magnetic resonance imaging (MRI) from 6 months before presentation showed mild scattered Fluid-Attenuated Inversion Recovery (FLAIR) hyperintensities likely consistent with microvascular disease or migraine, as well as empty sella turcica. She was also seen by neuro-ophthalmology because of blurring of vision, which showed no evidence of papilledema, optic nerve dysfunction, or other evidence of idiopathic intracranial hypertension. She continued to follow up with rheumatology for her recently diagnosed Lupus and Sjögren’s disease, though the burning sensation persisted despite other medication adjustments such as resuming oral steroid temporarily, stopping azathioprine, and starting methotrexate with folic acid.
The patient was then seen in a headache clinic again. By that time, the patient had independently stopped taking gabapentin for her neuropathy due to lack of therapeutic effect. Initially the plan was to try atogepant but it was not approved by insurance, so instead galcanezumab was tried. After starting monthly galcanezumab 120 mg subcutaneous injections, the headaches improved in both severity and frequency and the burning tongue sensation completely resolved and had not recurred in over 1 year since starting. On subsequent follow up, she reported that when she was delayed in taking galcanezumab the BMS symptoms returned temporarily until she took the next dose. The patient was satisfied with her galcanezumab and symptom control and has experienced no adverse effects; the patient provided informed consent for this case to be published.
Conclusion
This case helps demonstrate a possible therapeutic effect of CGRP medications for BMS. Especially when current literature shows limited efficacy of most current treatments, this case can suggest new treatments to explore for BMS with the potential for dramatic improvement of symptoms. Additionally, this case may also imply association between the mechanisms for migraine and BMS, bolstering our understanding of both diseases. Though a clear causative relationship or mechanistic link is yet to be revealed, this is supported by recent literature showing increased incidence of BMS in patients diagnosed with migraine. 10
Despite the promising outcome shown here, as with many case reports there are some limitations associated. Many conditions can cause oral pain, so to diagnose BMS these secondary causes should be excluded as much as possible. Overall, the patient's oral pain was found to be consistent with BMS based on ICHD-3 criteria and evaluation and exclusion of secondary causes. 11 Episodes occurred daily and lasted for at least 2 hours each over the preceding 6 months, and pain was described as burning and throughout the oral mucosa. Visual examination by multiple specialists showed no mucosal lesions, xerostomia, or evidence of infection. While the patient did have other conditions that can give oral pain, including GERD, Sjögren’s, and systemic lupus erythematosus, the burning pain persisted after each of these were treated appropriately. Though other diagnostics also have their limitations, such as EMG which would not show all kinds of neuropathy and was not focused on the facial innervation, the other testing such as serology and the pattern of pain suggested against these other secondary causes like nutritional deficiencies. Overall, though this patient did have other risk factors for oralfacial pain, the clinical course and workup suggests that those were less likely the main cause of her persistent oral dysesthesia, so with pain that fits ICHD-3 criteria this was considered consistent with BMS.
Another potential confounder is that with the natural course of the disease it is possible she would have improved spontaneously regardless of the addition of galcanezumab. However, with the timing of the resolution of symptoms closely related to initiating the medicine and recurrence when galcanezumab was delayed, this seems less likely to be a coincidence.
Future studies could continue to investigate new treatments for BMS and the relationship between migraine and BMS. For example, a clinical trial or other similar study could investigate the effect of galcanezumab or other CGRP medications on BMS. Additionally, this could be expanded to other medications that are effective for migraine to find other classes of medication that may be effective. Further, by studying the underlying pathophysiology of these diseases we can understand the mechanisms and potentially find new therapeutic targets. In this way, better treatments can be found for BMS, improving quality of life and potentially saving on healthcare costs for patients with this syndrome.
Key findings
Galcanezumab, prescribed for this patient's chronic migraine, also resolved this patient's BMS.
Since current BMS treatments are often ineffective, this case suggests CGRP inhibitors, which have not previously been investigated BMS, could outperform existing therapies.
This highlights a potential for new research and possibly treatments for BMS.
Footnotes
Ethical considerations
The information provided does not contain any personally identifiable health information and no experimental interventions were performed, so this research publication does not pose significant risk to the patient and additional ethical approval was not required.
Consent to participate
The patient provided consent for this case report to be written and submitted for publication.
Consent for publication
The authors of this article agree to publish with Cephalgia Reports if the manuscript is accepted.
Authors’ contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.