
Abstract
Aim
To examine the association between digital screen exposure patterns, lifestyle behaviors, and headache complaints among healthcare students across the Middle East and North Africa (MENA) region.
Methods
This multinational cross-sectional study was conducted between November 2024 and April 2025 among 2904 healthcare students from 11 MENA countries. Data were collected using a structured, self-administered online questionnaire assessing sociodemographic characteristics, digital screen use patterns, environmental factors, lifestyle behaviors, and self-reported headache occurring during or shortly after screen exposure. Univariable analyses were performed to explore associations, followed by multivariable logistic regression to identify independent factors associated with headache occurrence.
Results
Headache during or immediately following digital screen exposure was reported by 78.6% of participants. Prolonged daily screen use (particularly ≥7 h/day) and continuous screen use without breaks for more than two hours were significantly associated with headache complaints (p < 0.001). Frequent caffeine consumption during screen use, inadequate hydration, variable sleep duration, and higher perceived stress levels were also significantly associated with headache occurrence. Female sex and a family history of migraine were additionally associated with increased likelihood of reporting headache with screen use. In multivariable analysis, prolonged screen duration and absence of regular breaks remained independently associated with headache after adjustment for relevant demographic and lifestyle factors.
Conclusion
Headache complaints related to digital screen exposure were highly prevalent among healthcare students across the MENA region. Prolonged and uninterrupted screen use, along with modifiable lifestyle behaviors, were significantly associated with headache occurrence. Although causality cannot be established, these findings underscore the importance of preventive awareness, ergonomic education, and behavioral interventions within academic institutions. Longitudinal studies are warranted to clarify temporal relationships and evaluate targeted prevention strategies.
This is a visual representation of the abstract.
Background
The widespread integration of digital technologies into daily life has substantially increased exposure to digital screens. Activities such as watching movies, reading books or newspapers, shopping for clothes or groceries, booking vacations, registering for courses, applying for jobs, and scheduling doctor appointments can all be done with just a tap. 1 For healthcare students, in particular, the use of digital screens is crucial for their daily learning activities, continuous medical education, and exams. They commonly use various types of digital screens, including desktops, laptops, tablets, and mobile phones. 2 Numerous studies have demonstrated correlations between increased screen time and negative effects on weight, mental health, and sleep.3,4 However, the relationship between digital screen exposure and headache remains incompletely understood. The International Classification of Headache Disorders, third edition (ICHD-3), does not currently include a specific diagnostic entity for headache associated with screen use. The operational definition for this study was therefore based on existing literature, referring to headaches occurring during or immediately after screen use, which may overlap with or act as a trigger for established primary headache disorders such as migraine or tension-type headache. 3 Digital media may influence headache occurrence through both direct and indirect mechanisms. Direct mechanisms include prolonged exposure to high-intensity screen light, computer vision syndrome (digital eye strain), specific device ergonomics, and engagement with stimulating digital content, all of which may trigger or exacerbate headache symptoms. Indirectly, the timing and duration of screen use can disrupt circadian rhythms and sleep quality, contribute to mental fatigue or psychological stress, and promote sedentary behavior, all of which may interact to increase headache susceptibility.5–9
Continuous screen use without adequate breaks appears to be a key factor associated with headache. 10 Taken together, this evidence suggests a link between digital screens exposure and headache in young adults and highlights potential vulnerability of healthcare trainees. Addressing screen-related behavioral factors (e.g., ergonomics, screen time management) and stress in this population could be important for reducing headache burden and improving students’ quality of life. In our study, we hypothesized that specific patterns of digital screen use—including duration, timing, and environmental/ergonomic factors—as well as related behavioral patterns would show significant associations with the occurrence, frequency, and characteristics of headache complaints among healthcare students in the Middle East and North Africa (MENA) region. Our study aims to examine the relationship between digital device usage patterns, lifestyle factors and headache complaints among healthcare students in the MENA region. Specifically, we sought to identify demographic, lifestyle, and behavioral factors— including duration, frequency, and type of device use—that are associated with their headache complaints. By investigating these associations across students from diverse cultural and educational contexts within the MENA region, we aim to generate evidence that can guide preventive strategies and targeted interventions, ultimately supporting both health and academic performance in future healthcare professionals.
Methods
Study design
The current study is a cross-sectional, multinational investigation conducted among healthcare students using a descriptive correlational methodology. The study adheres to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) and utilized the STROBE reporting guidelines to ensure precision and accuracy in reporting.11,12
Study setting and participants
From November 2024 to April 2025, a cohort of 2904 undergraduate healthcare students was recruited via an online survey from medical schools in 11 countries within the MENA region. Participants were recruited through Microsoft Teams groups, announcements in medical classes, flyers posted in common areas of the medical school, email invitations sent through the faculty's mailing list, and social media platforms associated with the medical faculties. Eligible participants were healthcare students (medicine, nursing, pharmacy, dentistry, and allied health sciences) enrolled in universities across the MENA region at the time of the study. Inclusion criteria were: age ≥18 years; current enrollment in a healthcare-related degree program; using different types of digital screens on daily basis; and able to complete the survey. Healthcare students were selected because their academic activities typically involve extensive digital screen exposure through online learning platforms, electronic medical resources, and prolonged study periods, making them a relevant population for investigating screen-related symptoms. Exclusion criteria were: (1) a prior formal diagnosis of chronic primary headache disorders (e.g., chronic migraine or chronic tension-type headache); (2) regular medical follow-up or pharmacological treatment for such disorders; and (3) history of neurological disorders that could influence headache patterns. This included any diagnosed secondary headache disorders (e.g., post-traumatic headache, idiopathic intracranial hypertension, postmeningitis headache) or neurological diseases known to affect headache presentation such as brain tumors, vascular malformations, central nervous system infections, epilepsy, demyelinating diseases, hydrocephalus, or neurodegenerative disorders. The survey included students from various academic years, allowing for a diverse range of perspectives based on their progression through medical education. Each participant received a written explanation of the study's purpose and provided digital informed consent before data collection. The study emphasized anonymity, voluntary participation, and the right to withdraw at any time. Confidentiality was maintained, and responses were anonymous, with no identifying data collected. The study adhered to the ethical principles outlined in the latest version of the Declaration of Helsinki (2013).
No formal a priori statistical power calculation was reported for this study. The target sample size was determined based on the maximum number of eligible participants reachable through our recruitment strategy across 11 MENA countries, informed by prior studies of similar design and scope.5–8 The final sample of 2904 participants is substantially larger than most comparable studies, and given the prevalence of the primary outcome, was expected to provide adequate statistical precision and power to detect moderate associations in multivariable models.
Data collection instrument
Data were collected using a structured, self-administered electronic (online) questionnaire developed by the authors after an extensive review of relevant, Up-To-Date literature.3,5–7 The instrument was designed to assess digital screen use patterns, lifestyle factors, and self-reported headache complaints among healthcare students. The final questionnaire consisted of four main sections:
Part I: sociodemographic and health characteristics
This section collected information on participants’ age, sex, academic program and year, nationality, marital status, smoking status, and relevant medical history.
Part II: lifestyle and behavioral factors
This section assessed lifestyle habits that may influence headache complaints and screen exposure symptoms, including sleep duration and regularity, physical activity, caffeine consumption, perceived stress during screen use, and hydration practices.
Part III: digital screen use patterns and environmental factors
This section assessed various aspects of digital screen exposure, including types of devices used, duration and frequency of daily screen use, years of exposure, break-taking behavior, environmental conditions (lighting, noise, and seating), and primary purposes of screen use.
Part IV: headache complaints and characteristics
This section evaluated participants’ self-reported headache symptoms, including frequency, duration, intensity, laterality, associated symptoms, and functional impact. Participants were asked whether they experienced headache during or shortly after digital screen use using standardized self-report questions (e.g., “Do you notice headache while using screens?” and “Do your headaches worsen after screen use?”). For the purposes of this study, headache attributed to screen exposure was operationally defined as any self-reported headache occurring during or immediately after digital screen exposure, reflecting a perceived temporal association rather than a formal ICHD-3 diagnosis. This pragmatic definition was informed by previous literature describing associations between screen exposure and headache symptoms in student and young adult populations, including studies addressing screen time, online learning, and digital eye strain, and was used to capture symptom occurrence in real-life educational settings.3,5,6,8,10 As headache related to screen use is not currently classified as a distinct entity in the International Classification of Headache Disorders (ICHD-3), we acknowledge that this operational definition does not establish causation or clinical attribution and should be interpreted as a self-reported exposure-related symptom pattern rather than a distinct headache diagnosis.
The questionnaire was designed as a symptom-reporting tool rather than a diagnostic instrument, and it was reviewed by a multidisciplinary panel of seven experts in neurology, pharmacology, medical education, dentistry, and nursing to assess clarity, relevance, and face validity. Based on their feedback, ambiguous items were clarified, redundant questions were removed, and illustrative examples were added where appropriate.
The instrument was pilot tested on 110 healthcare students who were excluded from the final analysis. Internal consistency was assessed using Cronbach's alpha, demonstrating acceptable to good reliability for the main domains: headache characteristics (α = 0.81), screen use patterns (α = 0.84), and behavioral and environmental factors (α = 0.79). The pilot phase also evaluated feasibility, comprehensibility, and completion time, leading to minor revisions such as reordering items for logical flow, simplifying wording, and adding optional response categories. Following pilot testing, the questionnaire was programmed with built-in eligibility checks and branching logic to ensure appropriate survey flow and minimize incomplete responses. As a result, no missing data were recorded in the final dataset. The complete questionnaire is provided in Supplementary File S1.
Ethical approval
Ethical approval was granted by the Research Ethics Committee at the National Institute of cancer, Cairo University (IRB: EB2411-504-067-193) in November 2024.
Statistical analysis
Data were managed and analyzed using IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized using means and standard deviations (SD) for approximately normally distributed data and medians with interquartile ranges (IQR) for skewed distributions. Categorical variables were presented as frequencies and percentages. Normality of continuous variables was assessed using the Shapiro–Wilk test and visual inspection of histograms and Q–Q plots. Group comparisons were performed using the independent samples t test for normally distributed variables and the Mann–Whitney U test for non-normally distributed variables. Associations between categorical variables were examined using the chi-square (χ2) test or Fisher's exact test, as appropriate.
The primary outcome variable was self-reported headache during or after digital screen use (yes/no). Participants were categorized into two groups according to the primary outcome variable: those reporting headache during or immediately after digital screen exposure and those reporting no such headache. Group comparisons were subsequently performed to explore differences in demographic, lifestyle, and screen exposure characteristics between these two groups. Univariable analyses were first conducted to explore associations between potential predictors and headache complaints. Variables showing statistical significance in univariable analysis (p < 0.10) and those considered clinically relevant based on previous literature were subsequently included in a multivariable logistic regression model. The multivariable model was used to identify independent factors associated with headache complaints, including demographic characteristics, screen use patterns, and lifestyle factors. Adjusted odds ratios (aORs) with 95% confidence intervals (CIs) were reported. Multicollinearity was assessed using variance inflation factors (VIF), with values < 5 considered acceptable. Model fit was evaluated using the Hosmer–Lemeshow goodness-of-fit test. All statistical tests were two-tailed, and a p-value < 0.05 was considered statistically significant.
Results
Demographic and health-related characteristics of the participants:
A total of 2904 healthcare students participated in our study. The study population was predominantly female (71.3%), with a mean age of 21 ± 1.6 years. Participants represented a wide geographical distribution across the MENA region, with the largest proportion from Egypt (28.5%), followed by Yemen (15.4%) and Syria (12.1%). Most respondents were single undergraduate students enrolled across various healthcare disciplines. A very small number of participants reported being widowed (n = 9, 0.3%). Although uncommon in this age group, this may reflect sociocultural variations across participating countries in the MENA region. Given the extremely small proportion, this category had no meaningful influence on subsequent analyses. Table 1 summarizes main sociodemographic characteristics of study participants.
Demographic and health-related characteristics of study participants (n = 2904).
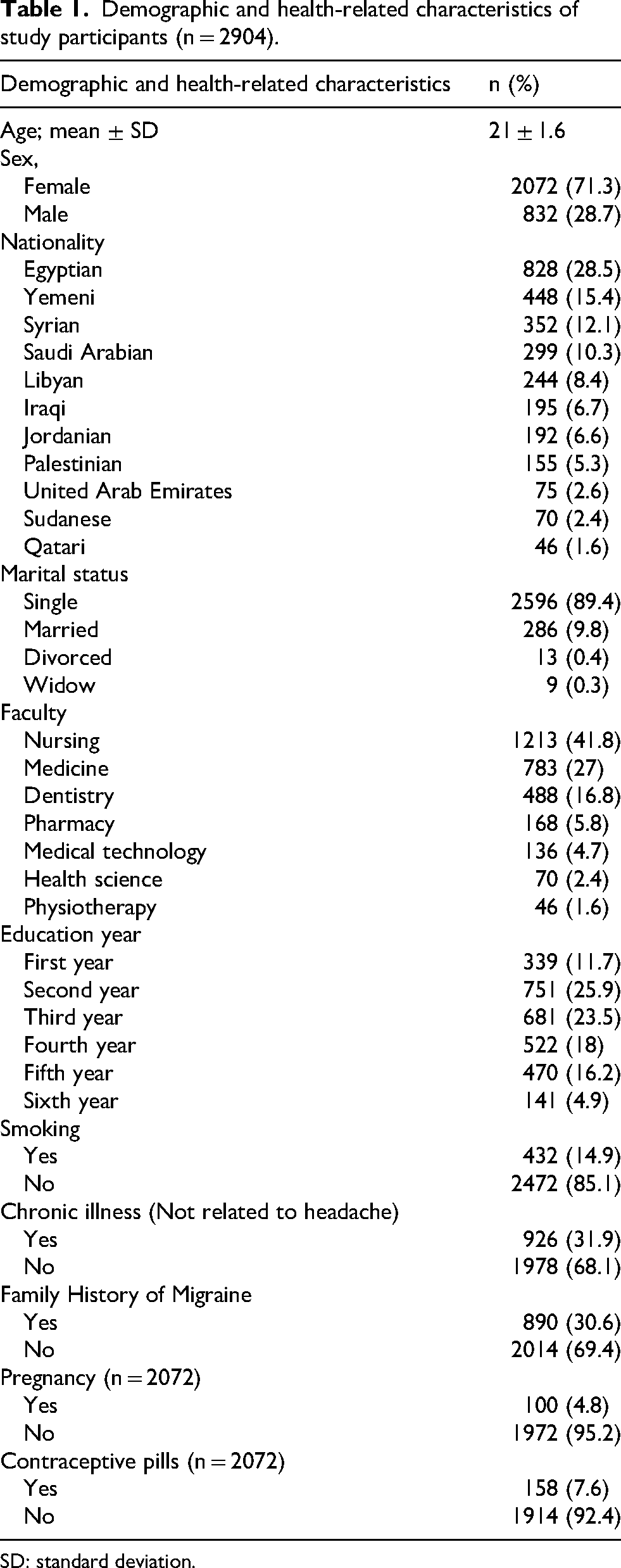
SD: standard deviation.
Lifestyle habits among study participants
Regarding lifestyle behaviors, the most commonly reported sleep duration was 6–8 h per night (36.5%), while 43.3% of participants reported sleeping less than six hours. Physical activity levels varied, with 38.3% engaging in exercise a few times per week. Approximately one-third of students reported daily caffeine consumption during screen use, and moderate perceived stress during screen exposure was reported by the majority of participants. Table 2 shows lifestyle habits among study participants regarding sleep, physical activity, hydration, caffeine usage and stress.
Lifestyle habits among study participants (n = 2904).

Digital screen usage among study participants
Most participants reported long-term exposure to digital screens, with over half indicating more than six years of use. Smartphones were the most commonly used device (89.5%), followed by laptops (54.8%). Daily screen exposure was substantial, with more than 40% reporting ≥7 h of use per day. Continuous screen use without breaks for more than two hours was reported by 43% of students. Digital screen usage patterns and associated behaviors are detailed in Table 3.
Digital screen usage and environmental factors among study participants (n = 2904).

Headache complaints related to digital screen use
Headache during or immediately following digital screen exposure was reported by 2282 participants (78.6%). Among participants reporting headache presumed to be associated with screen use, most episodes occurred occasionally (1–3 times per month) or weekly. Headache duration varied considerably, with approximately one-third lasting between 30 min and 1 h and another third lasting 1–4 h. Pain characteristics were heterogeneous, with throbbing or pulsating quality reported by 39.4% of participants. Table 4 summarizes some of characteristics of headache presumed to be attributed to digital screen use.
Characteristics of headache attributed to digital screen use (n = 2282).
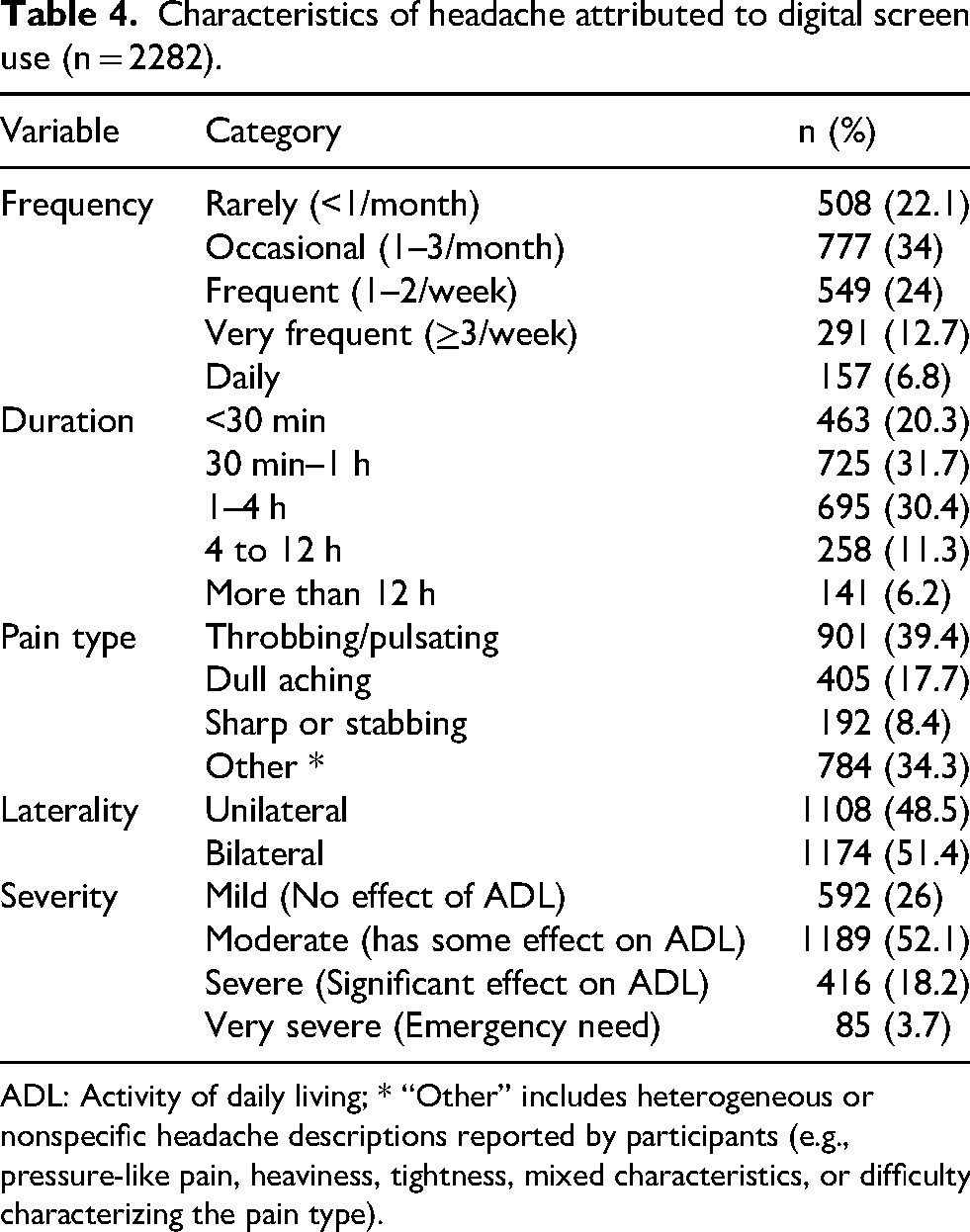
ADL: Activity of daily living; * “Other” includes heterogeneous or nonspecific headache descriptions reported by participants (e.g., pressure-like pain, heaviness, tightness, mixed characteristics, or difficulty characterizing the pain type).
The reported headache characteristics represent participants’ symptom descriptions rather than clinical diagnoses. Although some features (e.g., throbbing quality, unilateral pain, and longer duration) overlap with typical migraine or tension-type headache patterns, the questionnaire did not apply formal ICHD-3 diagnostic criteria.
In those who experienced headache with screen use, they attributed their headache with screen use to many factors shown in Figure 1.

Self-reported factors perceived by participants as contributing to headache during or after digital screen use (n = 2282).
Association of demographic and lifestyle factors and occurrence of headache
To explore potential determinants of headache occurrence, demographic, lifestyle, and behavioral factors were compared between participants reporting headache during or after screen use and those who did not report such headaches. Table 5 summarizes the association between demographic and lifestyle factors and headache occurrence.
Association between demographic and lifestyle factors and headache occurrence (n = 2904).
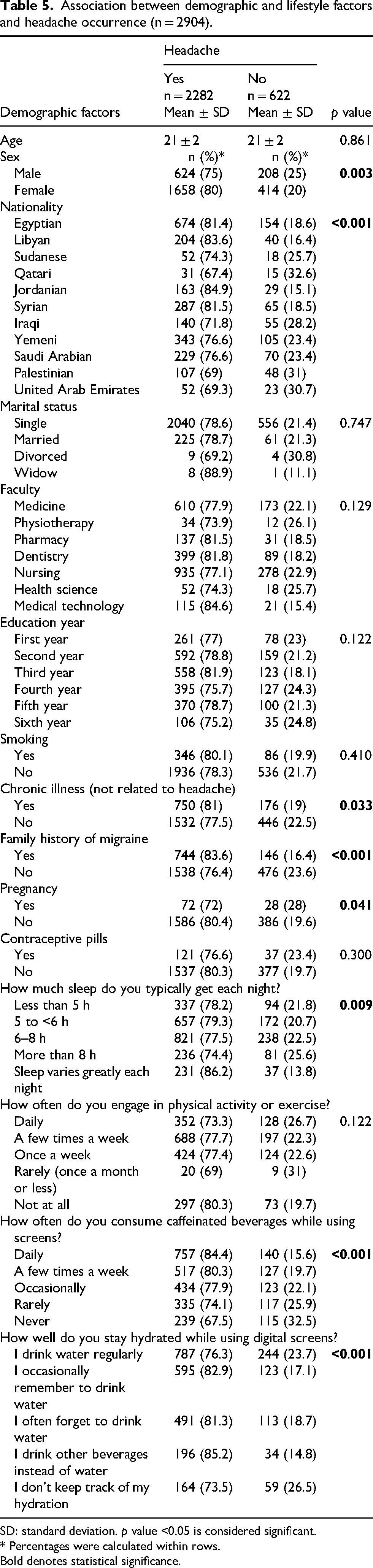
SD: standard deviation. p value <0.05 is considered significant.
* Percentages were calculated within rows.
Bold denotes statistical significance.
Association between digital screen usage and environmental factors and occurrence of headache
Several screen-related factors showed significant relationships with headache complaints, particularly longer daily screen duration, prolonged continuous screen use without breaks, and certain environmental conditions. Table 6 presents the comparison between participants reporting headache and those without headache across different digital screen exposure patterns and environmental characteristics.
Association between digital screen usage and headache occurrence (n = 2904).
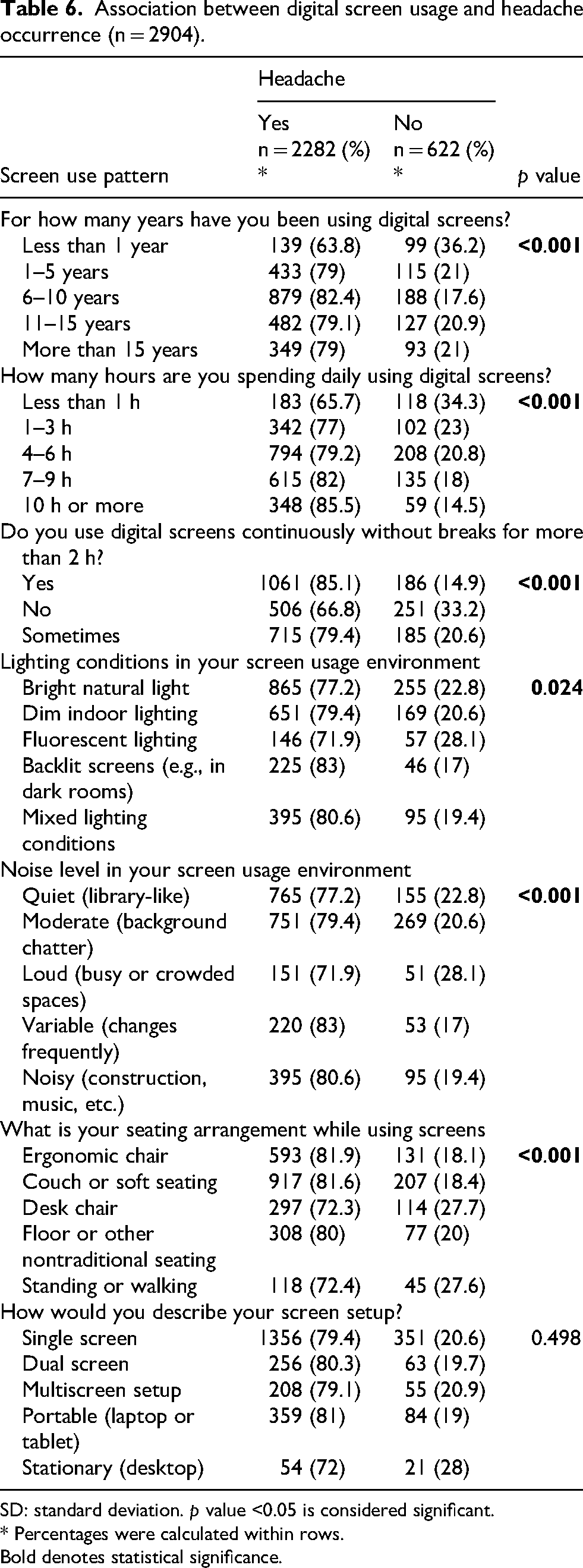
SD: standard deviation. p value <0.05 is considered significant.
* Percentages were calculated within rows.
Bold denotes statistical significance.
Discussion
In this large multinational cohort of 2904 healthcare students across 11 MENA countries, we observed a notably high prevalence of self-reported headache occurring during or shortly after digital screen exposure (78.6%). Headache complaints demonstrated significant associations with prolonged daily screen time, particularly among students reporting ≥7 h of use. Continuous screen exposure without breaks for more than two hours was strongly associated with headache occurrence, highlighting the importance of exposure patterns rather than screen use alone. Lifestyle factors also showed meaningful relationships: frequent caffeine consumption during screen use, suboptimal hydration practices, variable sleep patterns, and higher perceived stress levels were significantly associated with headache complaints. Collectively, these findings suggest that both digital exposure intensity and modifiable behavioral factors contribute to headache burden among healthcare students in the region.
Our findings are consistent with emerging international evidence linking screen exposure to headache in student populations. A cross-sectional study from Nepal reported high headache prevalence among medical students, with significant associations with prolonged study-related screen use. 5 Similarly, research from Bangladesh demonstrated that increased screen time was independently associated with both migraine and tension-type headache among university students. 6 In Italy, Romozzi and colleagues reported a high burden of primary headaches among medical students, with screen exposure and academic stress identified as contributing factors. 7 Studies conducted in Saudi Arabia during the COVID-19 pandemic also showed increased headache complaints associated with online learning and prolonged digital exposure.1,8 Furthermore, data from Jordan revealed a high prevalence of computer vision syndrome among medical students, frequently accompanied by headache symptoms. 10 Taken together, these studies suggest that prolonged digital screen exposure has been associated with headache and related symptoms in student populations across different geographical and educational contexts. However, the methodologies and specific outcomes assessed across these studies vary considerably. Therefore, the available evidence should be interpreted as broadly supportive of a possible association rather than as directly comparable findings.
Although causality cannot be inferred from our cross-sectional design, several plausible mechanisms may explain the observed associations. Prolonged screen use can induce digital eye strain, characterized by ocular discomfort, blurred vision, and headache, likely mediated by sustained accommodation, reduced blink rate, and tear film instability. 9 Exposure to high-intensity blue-enriched light may contribute to photic stimulation and central sensitization pathways implicated in headache pathophysiology. 13 Additionally, extended screen use—particularly during evening hours—may disrupt circadian rhythms and sleep architecture, thereby increasing headache susceptibility. 14 Musculoskeletal tension represents another relevant pathway. Poor posture, suboptimal seating arrangements, and sustained cervical flexion during device use may provoke pericranial muscle tension and cervicogenic components that exacerbate headache. 15 These mechanisms likely interact rather than operate independently, suggesting a multifactorial relationship between screen exposure and headache complaints. It is important to note that the headache characteristics reported in this study should not be interpreted as diagnostic classifications of migraine or tension-type headache. Because the questionnaire did not apply formal ICHD-3 criteria, the observed symptom patterns likely reflect heterogeneous headache complaints. In some participants, digital screen exposure may act as a trigger for underlying primary headache disorders, while in others the symptoms may reflect nonspecific screen-related discomfort such as digital eye strain or musculoskeletal tension.
A notable observation in our cohort was that female sex was associated with higher odds of reporting headache with screen use compared to males. This finding aligns with existing literature that suggests hormonal differences and other biological factors may contribute to the increased prevalence of headache among women. 16 Additionally, a family history of migraine was associated with higher odds of reporting headache during screen use. This observation may reflect increased susceptibility among individuals predisposed to primary headache disorders, particularly migraine. 17 Because the questionnaire did not apply formal diagnostic criteria, it is possible that some participants with migraine experienced screen exposure as a triggering factor rather than representing a distinct headache entity. Understanding these familial patterns can help in identifying at-risk individuals and implementing preventative strategies. However, the observed association should be interpreted cautiously, as digital screen exposure may act as a trigger for underlying headache disorders rather than representing a unique headache phenotype.
Importantly, our findings highlight modifiable behavioral factors that may mitigate headache risk. Students who reported regular breaks during screen use had significantly lower headache prevalence compared to those with prolonged uninterrupted exposure. This supports ergonomic recommendations such as structured microbreaks and the 20-20-20 rule. 18 Hydration practices also emerged as relevant; inadequate water intake during prolonged screen use was associated with higher headache reporting. Caffeine consumption, particularly daily intake during screen sessions, was similarly associated with headache occurrence, potentially reflecting both triggering and withdrawal phenomena. Perceived stress during digital engagement further amplified headache complaints, underscoring the interaction between psychological strain and somatic symptoms.19,20 These observations suggest that behavioral adjustments may represent practical, low-cost interventions for reducing headache burden in academic settings.
The high prevalence observed in this multinational cohort has important public health implications for educational institutions. Healthcare students represent a population with intensive academic screen exposure, and unaddressed headache burden may negatively affect concentration, productivity, and quality of life. Universities and training institutions should consider integrating preventive guidance into student wellness programs, including structured recommendations on screen-time management, ergonomic positioning, hydration awareness, and stress reduction strategies. Ergonomic education could be incorporated into early academic orientation sessions, particularly as digital learning platforms continue to expand globally. Given the modifiable nature of several identified factors, targeted preventive interventions may be both feasible and impactful.
This study represents one of the largest multinational investigations examining digital screen exposure and headache among healthcare students in the MENA region, with a diverse sample spanning 11 countries. The standardized survey instrument demonstrated acceptable reliability and allowed for comprehensive assessment of exposure patterns and lifestyle behaviors. However, several limitations should be considered when interpreting the findings of this study. First, the cross-sectional design precludes causal inference; therefore, the observed relationships between digital screen exposure and headache complaints should be interpreted as associations rather than cause–effect relationships. Second, the study population consisted exclusively of healthcare students. Although this group was intentionally selected because of their intensive academic screen exposure, the findings may not be fully generalizable to students from other academic disciplines or to the general young adult population. Future studies including comparative student populations from other faculties, such as engineering or computer science programs, could help determine whether the observed headache prevalence reflects a broader trend among young adults or is specific to healthcare training environments. In addition, the number of participants varied across participating countries, with a higher proportion of respondents from Egypt. This imbalance likely reflects differences in recruitment feasibility and institutional participation and may limit the generalizability of country-specific interpretations. Third, the study relied on self-reported data collected through an online questionnaire. Self-reported measures of both digital screen exposure and headache symptoms are susceptible to recall bias, reporting inaccuracies, and subjective interpretation. Although the questionnaire underwent expert review, pilot testing, and demonstrated acceptable internal consistency reliability, these procedures assess the coherence of questionnaire items rather than the objective accuracy of participants’ responses. Furthermore, recruitment through mailing lists and social media platforms may have introduced volunteer bias, as students experiencing headache symptoms or with greater interest in the topic may have been more likely to participate, potentially influencing prevalence estimates. Future studies incorporating probability-based sampling strategies and objective exposure monitoring—such as digital usage logs—may help improve measurement validity. Fourth, the questionnaire was designed to assess self-reported headache complaints temporally associated with screen exposure rather than to establish clinical diagnoses of specific primary headache disorders. Because formal ICHD-3 diagnostic criteria were not applied and validated headache diagnostic instruments were not used, some participants may have had undiagnosed primary headache disorders in which digital screen exposure acted as a trigger. Consequently, the reported headache characteristics should be interpreted as symptom descriptions rather than diagnostic classifications. Finally, several potentially relevant factors were not evaluated. These include detailed contextual aspects of screen exposure (such as content type, timing of use, and specific digital tasks), psychiatric comorbidities such as anxiety or depression, and standardized measures of headache-related disability. Future research incorporating more comprehensive behavioral, psychological, and clinical assessments may help further clarify the mechanisms linking digital screen exposure and headache symptoms.
Conclusion
In this large multinational study of healthcare students across the MENA region, headache complaints during or shortly after digital screen exposure were highly prevalent and were significantly associated with prolonged and uninterrupted screen use, as well as modifiable lifestyle factors including caffeine intake, hydration practices, sleep variability, and perceived stress. While causal relationships cannot be established due to the cross-sectional design, the findings suggest that patterns of digital engagement and related behavioral factors may play an important role in headache occurrence among young adults in academically intensive settings. These results underscore the need for increased awareness, preventive guidance, and ergonomics-focused education within universities. Future longitudinal and interventional studies are warranted to clarify temporal relationships and evaluate strategies aimed at reducing screen-related headache burden in student populations.
Article highlights
In this 11-country MENA study (n = 2904 students), 78.6% reported headache during or after screen exposure.
Screen use ≥7 h/day and continuous use >2 h without breaks independently increased headache odds.
Caffeine, poor hydration, variable sleep, and high stress were significantly associated with screen-related headache.
Female sex and family migraine history increased reporting likelihood.
Findings suggest modifiable behavioral and ergonomic targets for prevention in academic settings.
Supplemental Material
sj-docx-1-rep-10.1177_25158163261453877 - Supplemental material for Digital screen exposure, lifestyle behaviors, and headache complaints among healthcare students: A multinational study from the MENA region
Supplemental material, sj-docx-1-rep-10.1177_25158163261453877 for Digital screen exposure, lifestyle behaviors, and headache complaints among healthcare students: A multinational study from the MENA region by Ahmed Dahshan, Marwa Ibrahim Mahfouz Khalil, Mohamed Mahmoud Elsaieed, Sameer A Alkubati, Saleh Zaghir Mohammed Alhetar, Nada Ab. Hweissa, Malak Khalel, Zainalabideen Yasser Jumaa, Nadia Mohamed Ibrahim Wahba, Dalia Abdelfatah, Fatima Hallaj, Ebtehal S Doma, Basma Salameh, Fuad Taleb, Ahmed Awad Osman Mohammed, Alaeldeen Hakim Mohamed Hakim, Merghani Abdallah Hussain Abdallah, Alaa Ahmed Shalan, Taliaa M Al-Yafeai, Olaa Abdalslam Ibraheem and Diana Khedr in Cephalalgia Reports
Footnotes
List of abbreviations
Acknowledgments
The authors acknowledge the use of artificial intelligence (AI) tools specifically chat GPT plus solely for drafting assistance and language corrections. These tools were utilized to enhance clarity, grammar, and overall readability of the manuscript while ensuring that all scientific content, data interpretation, and intellectual contributions remain the original work of the authors. The integrity and authenticity of the research are fully maintained.
ORCID iDs
Ethical considerations
Ethical approval was granted by the Research Ethics Committee at the National Institute of cancer, Cairo University (IRB: EB2411-504-067-193) in November 2024. The study emphasized anonymity, voluntary participation, and the right to withdraw at any time. Confidentiality was maintained, and responses were anonymous, with no identifying data collected. The study adhered to the ethical principles outlined in the latest version of the Declaration of Helsinki (2013).
Consent to participate
Each participant received a digital written explanation of the study's purpose and provided digital informed consent before data collection.
Consent for publication
All authors agree for publication in Cephalalgia Reports.
Author contributions
AD, MIMK, MME, and DA contributed to the conceptualization and design of the study. Methodology was developed by AD, DA, MIMK, and MME. Questionnaire development and validation were performed by AD, MIMK, DA, and ESD. Data collection and coordination were undertaken by MME, SAA, SZMA, NAH, MK, ZYJ, NMIW, FH, BS, FT, AAOM, AHMH, MAHA, AAS, TMA-Y, OAI, and DK. Statistical analysis was performed by DA, AD, and MME, while data interpretation was carried out by AD, MIMK, DA, and NMIW. The manuscript was drafted by AD, MIMK, and DA and all authors contributed to critical revision of the manuscript. Supervision was provided by AD and MIMK and project administration was managed by AD and MME. All authors approved the final manuscript and agreed to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.