
Abstract
Background:
Migraine is a leading cause of disability in India and Sri Lanka but remains underdiagnosed and undertreated. Both countries, with their differing healthcare systems, provide an important regional perspective on migraine care.
Methods:
We utilized a combination of structured search as well as relevant literature screening to identify studies and practice standards on migraine care in India and Sri Lanka, from year 2000 to July 2025 with emphasis on large clinical studies, multicentric studies, and randomized controlled trials following PRISMA guidelines.
Results:
India's care delivery of migraine is via a large network of public and private sector hospitals, with three strata of physicians working at primary, secondary and tertiary care centres, and primary physicians are the first point of contact for patients. Additionally, private practitioners see sizeable proportion of patients with free referral to public sector at all levels. Subsidized medications are available all over the country with options for private medical insurance as well as government medical insurance for selected cases. Sri Lanka on the other hand has universal healthcare system that provides free, publicly funded care to all citizens, financed through general taxation, complemented by a growing private sector. While a larger number of medications are available in India, newer therapies are challenged with high costs and lack of insurance coverage for many. Newer medications are currently not available in Sri Lanka. Similarly, headache research is widespread in India but suffers from the lack of institute support whereas it is in a nascent stage in Sri Lanka.
Conclusion:
India and Sri Lanka present striking differences in care of migraine and research opportunities. While therapeutic advances and research have progressed in India, universal health coverage is a challenge. Sri Lanka needs to incentivise research while bringing in newer antimigraine therapies to optimize patient outcomes.
This is a visual representation of the abstract.
Keywords
Introduction
Migraine imposes a substantial burden on individuals and society. According to Global Burden of Disease (GBD) data, migraine is one of the most disabling neurological conditions worldwide. 1 It is, in fact, the most disabling neurological condition among children, adolescents, and women of child-bearing age.2,3 Reflecting global trends, migraine is also highly prevalent in the Indian subcontinent, contributing substantially to the overall burden of neurological diseases in the region.
A hospital-based study from North India confirmed the high prevalence of primary headache disorders, with migraine being the most common presentation, highlighting the significant patient load in routine neurology practice. 4 The GBD trends for migraine indicate a higher incidence of migraine in India but comparable prevalence, however, disease morbidity was higher in Sri Lanka. 5 This highlights the need for healthcare reforms and prioritizing healthcare research in the region.
Migraine not only impairs a person's quality of life (QOL) but also contributes substantially to the loss of productivity due to absenteeism as well as presenteeism, making it a major public health challenge even for high-income countries.6,7 Despite its widespread impact, migraine continues to be underdiagnosed and undertreated, often overshadowed by other health priorities. In India, the large population base, socio-economic disparities, and inequality of healthcare access challenge the existing health infrastructure. On the other hand, Sri Lanka offers universal health coverage for its population, however, recent economic and political challenges have affected the delivery of health services including migraine care.
There is a paucity of literature regarding the existing standards of care in the Indian subcontinent. This review aims to provide an overview of migraine care in the Indian subcontinent, with an emphasis on India and Sri Lanka. The objective of this review is to discuss the existing standards of migraine care in India and Sri Lanka, with emphasis on service delivery, pharmacological and non-pharmacological approaches, barriers to care, and future directions.
Methods
We aimed to present an updated evidence-based narrative review focusing on the healthcare scenarios of both India and Sri Lanka. An adaptive design incorporating structured search questions focusing on various outcomes for collecting evidence for migraine care in India and Sri Lanka was used as well as database search was used to collect relevant reports and information from different health agencies of both countries and international organizations such as the World Health Organization and the World Bank. This study is reported in accordance with the PRISMA guidelines for systematic review. We followed the principles of PRISMA and searched databases like (PubMed, Scopus, and Embase) for identifying studies on migraine care in both the countries. Structured searches were conducted using MeSH term ‘migraine’, ‘migraine disorders’, ‘management’, ‘treatment’, ‘prophylaxis’, ‘CGRP antagonist’, ‘abortive’, ‘analgesics’, ‘alternative medication’, ‘Yoga’, and ‘headache clinics’ with use of Boolean operators OR and AND in different combinations. Results were screened for India and Sri Lanka, and the search was limited from 2000 till July 2025. The title search for India was independently conducted by two blinded reviewers (SR and VS), and the full text reviews were conducted by both authors independently, and disagreements were resolved by a third author (KC).
Literature on migraine care from Sri Lanka, identified using the same search criteria, were screened and added to the tables where suitable. Due to the paucity of data, a narrative synthesis was used to summarise information on Sri Lanka. Where relevant, anecdotal evidence based on the authors’ clinical and professional experiences was used, particularly in areas where published data were limited.
Inclusion and exclusion criteria
Inclusion criteria
We included multicentric studies, randomized controlled trials (RCTs), observational studies, reviews, case series with more than 20 subjects, and practice-based reports wherever necessary to the provided context. Studies published in English, conducted in India and Sri Lanka, involving adult or paediatric populations with migraine, and addressing management, treatment, or healthcare delivery, barriers and future directions in migraine care were included in the study. Randomized control trials performed in India and Sri Lanka or trials in which either of these countries were a part were also included.
Exclusion criteria
Case reports, single-patient studies, studies not directly related to migraine care, and studies outside India or Sri Lanka were excluded.
Results
Due to the differences in the health care systems and the availability of literature, migraine care in the two counties is discussed separately.
Status of migraine care in India
Search process
For India, we retrieved records from three databases (PubMed: 478 records, Scopus: 260 records, and Embase: 834 records), totaling 1572 records. After removing duplicates and ineligible records, we performed a full-text review of 96 articles, out of which 47 studies met our final inclusion criteria and were included for the purpose of this review along with two national guidelines from ICMR and IMA (Figure 1).
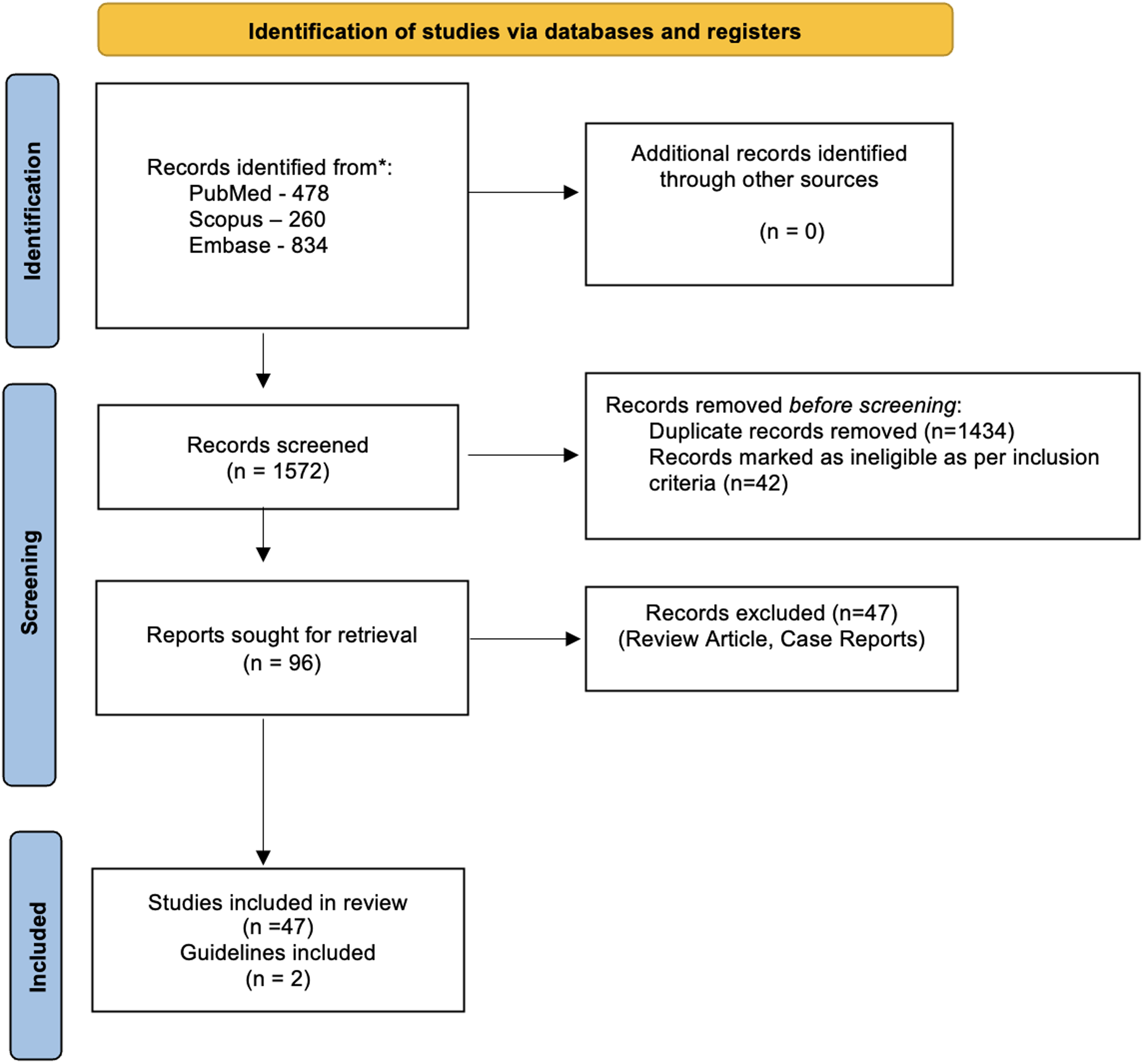
PRISMA Flow Diagram showing schematic representation of the selection process and inclusion of the studies.
Demographic data
Migraine has a varied prevalence across the country, with studies reporting a broad range of prevalence. A recent epidemiological study from the national capital region showed a one-year prevalence of 26.3% for migraine, with a female dominance. 8 In comparison, a door-to-door prevalence study in Karnataka (South India) also yielded similar results with a prevalence of 25.2%. 9 A cross-sectional study in eastern India reported a prevalence of 14.1%, and similar cross-sectional studies reveal similar rates of prevalence in various convenience sampling. 10 Women, that too in the economically active group bear the burden of disability in most cases.11–13 According to 2021 statistics, India ranks first in the world with 8,096,330.9 disability-adjusted life years (DALYs) (95% UI: 10,157,454.4–18,217,286.6). 14 Evidence from various studies has reported a one-year prevalence of migraine in India as high as 25%, compared to the global prevalence of 14.7%.9,15 There is no available data on pediatric migraine in India.
Organization of health services for migraine
The Indian medical system produces the largest number of doctors in the world annually. 16 India has managed to exceed the doctor-to-population recommendation ratio with 1:834 against the recommended ratio of 1:1000. 17 However, there is a large variance in the ratio from rural to urban regions. The healthcare system has a well-distributed system of public sector hospitals aided by private sector hospitals offering different levels of care. Neurologists as well as general practitioners provide migraine treatment in both public and private healthcare facilities. Public healthcare organization is a three-tiered system with physicians in public sector hospitals at primary, secondary, and tertiary or referral centres. 18 Primary practitioners form the first point of contact for headache patients. Referral of headache patients is usually to tertiary care centres where internal medicine and neurology departments cater to headache and migraine management. However, dedicated headache clinics are less common and are limited to bigger towns and cities. Primary care practitioners also lack specialized training in headache medicine and refer patients to higher centres. A 2023 paper cited a total of 612 hospitals—321 (52.45%) government-run and 291 (47.55%) private medical colleges. Several regional All India Institute of Medical Sciences (AIIMS), state health universities, institutes of national importance, and prominent state medical colleges cater to referred headache patients 19 (Figure 2). Despite this, there is a large unmet need for more structured headache services and specialized care pathways all over the country. 20

Map of India showing various prominent public sector tertiary care hospitals in India with facilities for Headache management.
Barriers to care
Several misconceptions surround headache. Patients often believe that migraine is not a neurological disorder but rather caused by lifestyle, eyesight, or psychosomatic stress. Financial barriers preventing adequate therapy, absence of medical insurance, and lack of awareness of headache as a chronic condition requiring prophylactic and abortive medications are all patient-related barriers. Low education level and lack of access to imaging are other factors that are barriers to effective migraine care. 21 There are also instances of gender biases in pain perception and healthcare-seeking behaviour, due to which women, who suffer from migraine at a disproportionate rate, frequently experience delays in diagnosis. 5 Furthermore, neither public nor private insurance programs have adequate reimbursement guidelines for headache medicine and cutting-edge therapies like anti-CGRP monoclonal antibodies and other targeted therapies for migraine. A telephone-based follow-up of headache patients showed that only 126 out of 214 patients were given prophylactic medications even for chronic migraine casess. 22 Several patients also do not visit the general practitioner or neurologist at the first instance and rather visit psychiatrists or practitioners of alternative medicine for their complaints. Yet, there is a broad framework of antimigraine medications available in the Indian pharmaceutical market including newer therapies that are used by a significant proportion of affording population (Figure 3).
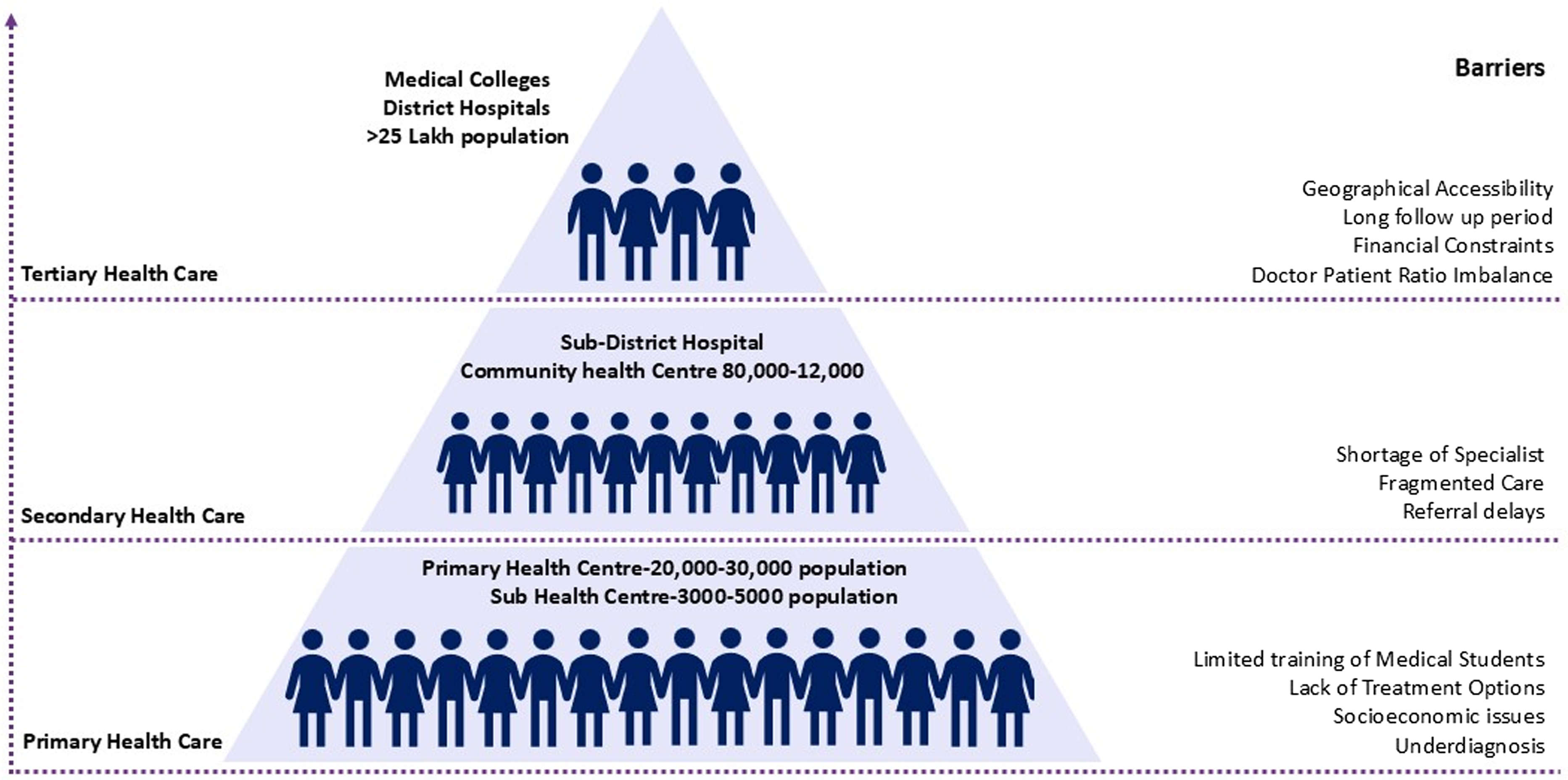
Levels of healthcare organization and barriers and access to healthcare in India.
Symptomatic or abortive therapies for migraine
Several analgesics in the Indian markets have established efficacy in migraine. Naproxen-domperidone combination is one of the most common combination analgesics used as abortive therapies for an acute attack. 23 Paracetamol, ergotamine, and caffeine are other drugs used for stopping acute attacks. Triptans, including rizatriptan, sumatriptan, almotriptan, and zolmitriptan, have an established safety profile compared to analgesics..24,25 A review by Thangaraju et al. on Indian drug information sources highlights that non-steroidal anti-inflammatory drugs (NSAIDs), paracetamol, triptans, and ergot derivatives are consistently referred to as available acute treatment options, underscoring their prominence in regular clinical practice. 26
Recently, dispersible analgesics and parenteral routes of administration have also been shown to be useful. A randomized crossover trial demonstrated 82% of patients experiencing a reduction in pain score by four points, or to zero, at 20 min using timolol eye drops as compared to placebo 27 (Figure 4) (Table 1 lists all evidence-based migraine treatments available in India).
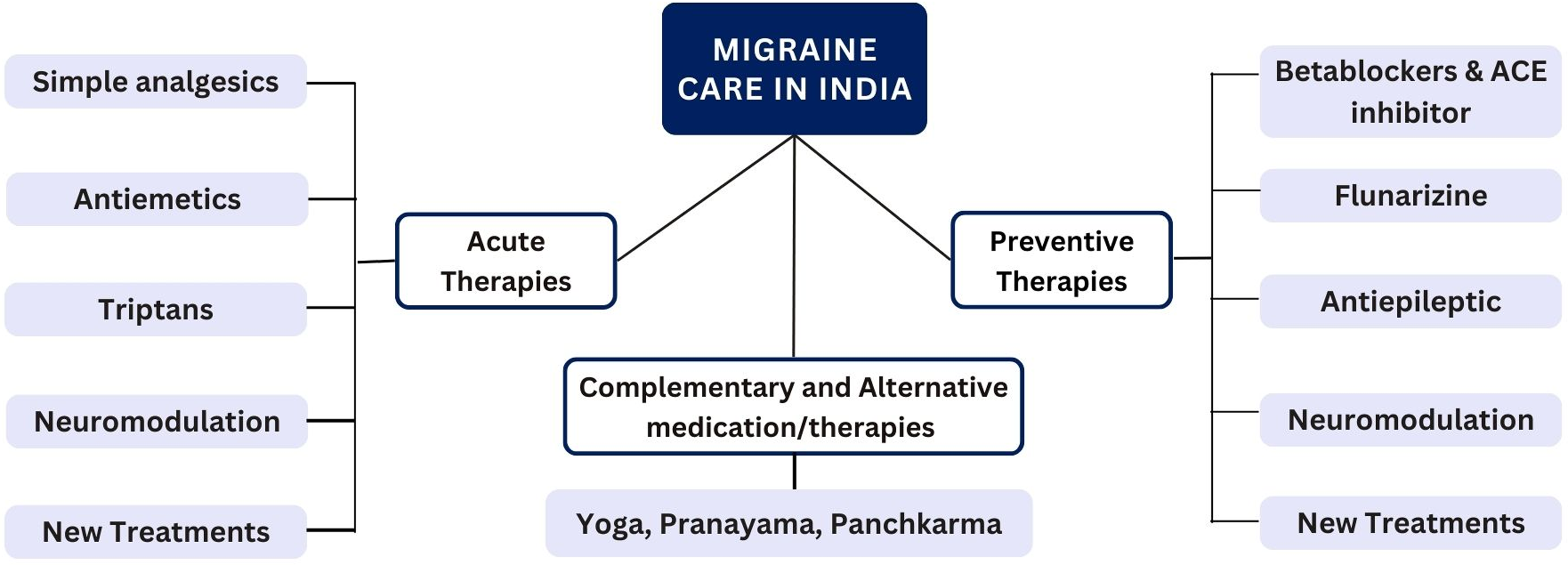
Summary of the various modes of migraine treatment practised in India.
Table listing all evidence-based migraine treatments available in India.

Prophylactic therapy for migraine
Among prophylactic agents, topiramate, propranolol, divalproate, amitriptyline, sodium valproate, and flunarizine are some commonly used preventive medications in India.28,29 Propranolol and cyproheptadine were found to be equally effective in preventing migraine in early double-blind Indian study, with both showing good tolerability profiles. 30 Topiramate and propranolol have also demonstrated significant efficacy in paediatric and adult patients in various Indian studies,31–33 while propranolol was comparable in efficacy and better tolerated in long-term follow-up than topiramate.32,34–36 Despite having distinct adverse effect profiles, divalproate and amitriptyline demonstrated similar effects, as supported by a study which showed that both divalproate extended-release and amitriptyline resulted in comparable efficacy in improving headache by 74.7% and 62%, respectively. 37 Flunarizine has also been studied for vestibular migraine and has been shown to improve vertigo and migraine symptoms. 38 A prospective interventional study found that flunarizine therapy (10 mg daily for 2 months) in 31 vestibular migraine patients significantly reduced headache frequency (p = .001), headache duration (p = .001), vertigo frequency (p = .001), vertigo duration (p = .001), and vertigo intensity (p = .009), with no significant changes in cervical or ocular vestibular evoked myogenic potentials (p > .05). 39
Even with multiple options for prophylactic therapies, utilization remains low, even for chronic migraine. Beta-blockers have been reported to be used in 28.9%, followed by tricyclic antidepressants in 24.3% of a cohort of headache patients. The latest therapies in migraine, which is the anti-CGRP therapy including erenumab and rimegepant are also available in India, although they’re not used widely due to high cost and restricted availability. However, several global studies have included India that establish the role of these agents in the Indian population. The EMPOwER study, a large multinational RCT that included India, confirmed the efficacy and safety of erenumab for the prevention of episodic migraine in which erenumab significantly reduced monthly migraine days (MMDs) compared with placebo (–4.days with erenumab 70 mg, −4.8 days with erenumab 140 mg, vs. −3.1 days with placebo at week 12). 40 Similarly, a recent indirect comparative analysis found that patients on erenumab achieved a greater reduction in MMDs at 12 weeks (−0.90, p = .042), making it more effective than rimegepant at preventing migraine, underscoring the importance of CGRP-targeted monoclonal antibodies in the development of future migraine treatment protocols in India (Figure 4) (Table 2 lists and summarize randomized clinical trials in pharmacological interventions from India).
Summarizing randomized clinical trials in pharmacological interventions from India.

MMD = monthly migraine days.
Newer technology and devices:
Cephaly, an electronic trigeminal nerve stimulator and Nerivio, a remote electrical neuromodulation device has been permitted for use in India. However, there is no large-scale data for their usage or efficacy. Device technology like repetitive transcranial magnetic stimulation (rTMS) have now been studied to prevent migraine. A randomized sham control study utilizing high-rate transcranial magnetic stimulation found significant improvement in headache frequency (78.7 vs. 33.3%, p = .0001) and reported VAS scores (76.6 vs. 27.1% p = .0001). 45 In Indian patients with acute migraine, buccal prochlorperazine was found to be both effective and well-tolerated, providing a useful substitute in outpatient settings. 46
There have also been many studies on the use of transcranial magnetic stimulation in migraine form various parts of India. A randomized trial showed that in chronic migraine, rTMS, both by itself and in conjunction with amitriptyline, demonstrated >50% reduction in headache days at 2 months (69% vs. 29.3%; p < .001) and 3 months (76.2% vs. 31.7%; p < .001). A recent study compared topiramate monotherapy to combination treatments with greater occipital nerve block (GONB) in chronic migraine patients, finding that combination treatments (topiramate with GONB using lidocaine with or without steroids) significantly reduced monthly migraine days (−9.6 and −10.1 vs. −7.3 days, p = .003 and p < .001) and achieved ≥50% reduction in headache days in a greater proportion of patients (71.4% and 62.4% vs. 39%, p = .004 and p = .034) in 3 months 44 (Figure 4).
Interventional approaches such as greater occipital nerve (GON) block have been validated in India in a randomized double-blind placebo-controlled trial, showing four-weekly GON blockade with 2% lidocaine significantly reduced mean headache (−4.2 days) and migraine days (−4.7 days) compared to placebo in chronic migraine patients 47 (Table 3 lists and summarizes some recent randomized clinical trials in non-pharmacological interventions in migraine from India).
Summarizing randomized clinical trials in non-pharmacological interventions from India.

MMD = monthly migraine days.
Lifestyle changes and alternative medications
India is a country with vast history dating back thousands of years. Traditional health practices remain an integral part of life and when compared to conventional NSAID treatment. Ayurveda and yoga have also shown improvements in headache frequency, intensity, and QOL. 52 A randomized study from North India including 160 patients with episodic migraine showed that yoga as an add-on therapy for migraine reduced headache frequency (−3.53, p < .0001), headache intensity (−1.31, p = .0004), HIT score (−8.0, p < .0001), MIDAS score (−7.85, p < .0001), and pill count (−2.28, p < .0003).. 20 A notable decrease in average VAS score, headache frequency, and MIDAS questionnaire was found in an exploratory study investigating the efficacy of fMRI-guided rTMS, sustained at the one-month follow-up. 53 Other novel approaches include α-Lipoic Acid (ALA) as an adjunctive therapy that has also demonstrated biochemical and clinical improvement and is one of the other innovative strategies. A recent RCT for migraine prophylaxis in adolescents suggested that adding ALA to flunarizine significantly reduced migraine frequency (−7.7 days), with an improved responder rate (80% vs. 33.3%) in the flunarizine-only group (p = .001) 54 (Figure 4 and Table 3).
Guidelines on migraine:
The International Headache Society (IHS) has released global consensus recommendations for acute and preventive migraine treatment, which provide a valuable framework for standardizing care in the Indian subcontinent and bridging local guideline gaps.55,56 The Indian Council of Medical Research (ICMR) Standard Treatment Workflow (STW) for headache disorders, released in October 2019, provides evidence-based guidelines for headaches including management of migraine, standardized diagnostic and treatment protocols tailored to the Indian healthcare system and outlining a flowchart for evaluation and treatment of headaches, starting with identifying the type of headache (e.g., continuous, migraine, tension, or cluster) and red flags (e.g., sudden severe onset, fever, neurological signs) that warrant urgent imaging (CT/MRI) or referral to tertiary care center. At primary care level, management includes analgesics, antiemetics, lifestyle changes, and prophylaxis (e.g., propranolol, flunarizine for migraine >2/month); district hospitals handle atypical cases with amitriptyline or indomethacin, while tertiary care centres address major causes like subarachnoid haemorrhage, cerebral venous thrombosis, or tumours via anticoagulation, surgery, or antibiotics. Follow-up emphasizes blood pressure control, antiepileptics, prophylaxis tapering, and admission/discharge criteria for severe or unresponsive cases. 57
Similarly, the Indian Medical Association (IMA) headache guidelines, as outlined in the Headache Management Booklet (Version 1.1, July 2024), offer practical recommendations for migraine prophylaxis, including the use of beta-blockers, tricyclic antidepressants, and lifestyle modifications, with a focus on patient education and cost-effective therapies for the abortive treatment algorithm for migraine starting with paracetamol 1000 mg; if ineffective, use NSAIDs (naproxen 250/500 mg, ibuprofen 400 mg, or aspirin 1000 mg) with antiemetics (domperidone or metoclopramide 10 mg). For persistent symptoms, try oral triptans (e.g., sumatriptan 100 mg, rizatriptan 10 mg), nasal sprays (zolmitriptan 5 mg, sumatriptan 20 mg), or subcutaneous sumatriptan 6 mg; if no control, switch triptans or combine with naproxen, and refer to a headache specialist. If still uncontrolled, consider oral lasmiditan 50–100 mg and refer to a specialist or tertiary care centre. 58
Utilization and costs:
India is home to affordable healthcare with the national insurance scheme called Ayushman Bharat Pradhan Mantri Jan Arogya Yojana (AB-PMJAY), launched in 2018 as a key policy towards universal health coverage. The insurance is a guarantor against many serious and life-threatening conditions and antimigraine therapy unfortunately does not come under its umbrella. Personal health insurance is not universal and is limited to either the rich and affording or government employees of some predesignated standing. Hence, medications like CGRP antagonists, botulinum toxin, and other newer migraine medications have not found a wider audience.
Migraine education and the way forward
There is a noticeable lack of structured migraine education within Indian medical training programs, with a few structured programs in undergraduate or postgraduate training. Headache is often underrepresented in neurology training, leading to a lack of proficiency among general practitioners. Dedicated CME programs and headache workshops are increasing, supported by the Indian Academy of Neurology (IAN). However, certification programs for headache specialists are still lacking.
Advocacy and initiatives:
Several hospitals conduct annual migraine days and workshops are held by certain hospitals, a national body for education and training in headaches and migraine is still lacking. However, physicians in many tier-1 and tier-2 cities are now skilled in management of migraine and usage of therapies like the ditans and botulinum toxin is now evolving. The headache subsection of Indian Academy of Neurology (IAN) is a recognized body that regularly conducts webinars, conferences and training programs in migraine. A range of antimigraine therapy is available in India but analysis of Indian pharmacopoeia showed some inconsistencies and insufficient information about migraine medications. The findings highlight the need for improved professional and public education. 26 There are also some significant differences in the accessibility of necessary migraine drugs between nations, and a global IHS survey revealed that India continues to lack access to more advanced treatments, highlighting the need for policy-level interventions. 59 Overall, there is a large growing body of evidence to support research and innovation in India, but the population is vast and catering to the same needs to be encouraged at multiple levels or healthcare and executive organization.
Status of migraine care in Sri Lanka
Demographic data
Sri Lanka is an island nation with a population of 22.9 million. 60 It is a lower middle-income country currently recovering from a deep economic crisis which had a significant impact on its health system.60,61 The gross domestic product (GDP) of Sri Lanka in 2024 was 98.96 billion USD and the current health expenditure as a percentage of GDP is around 4.36%.62,63 Although this is substantially lower than the global average of 9.89%, it remains higher than both the South Asian average (3.26%) and the average among lower-middle-income countries (3.89%) 62 (Figure 5).
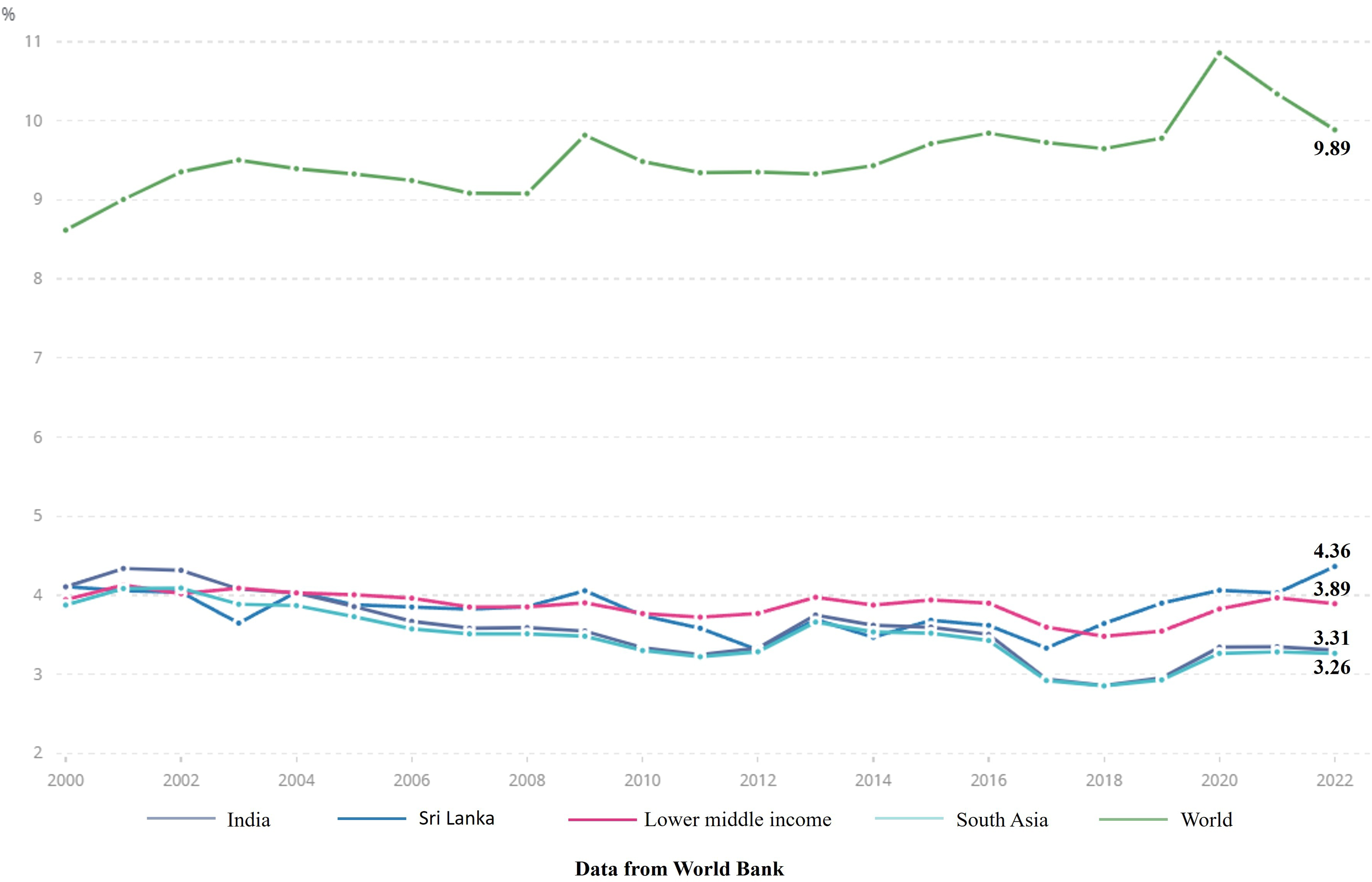
Health expenditure as a percentage of gross domestic product (GDP).
Analysis of GBD data shows that in Sri Lanka, an estimated 3.7 million migraine cases were reported in 2021, a 36.8% increase since 1990. 5 The crude incidence of migraine in Sri Lanka has risen by 16.8% from 1990 to reach 280,000 cases per annum in 2021. 5 The age-standardised incidence rate has increased only slightly, from 1285.6 to 1290.9 cases per 100,000, while the age-standardised prevalence rate rose from 15638.5 to 15890.5 cases per 100,000. 5 There was also a slight increase in the age-standardised years of life lost due to migraine, from 588.2 thousand to 592.2 thousand patient-years in Sri Lanka. 5
Despite the impact of migraine, precise national estimates remain limited. The only population-based epidemiological study on migraine in Sri Lanka was conducted among approximately 1850 individuals aged 20–59 years in the predominantly urban district of Gampaha. 64 This study found a crude period prevalence of migraine of 10.4% (95% CI: 9.0–11.8) and a standardised period prevalence of 9.0% (95% CI: 9.0–9.1). Several small-scale cross-sectional studies have examined migraine epidemiology in specific populations. In one study of 680 schoolchildren aged 12–15 years from the rural and suburban district of Polonnaruwa, the prevalence of migraine was at 7.8%. 65 Among Sri Lankan undergraduates, three descriptive studies have reported prevalence rates ranging from 7.5% to 25%.66–68
Organization of services and workforce development
Sri Lanka operates a universal, free public healthcare system, initiated in the 1930s, complemented by a growing private sector. The public system delivers 50% of outpatient care and 95% of inpatient services. 69 The private sector, largely concentrated in urban and suburban areas, contributes primarily to outpatient care. 69 While multiple medical systems are practised (Western, Ayurvedic, Unani, Siddha, and Homoeopathy), Western medicine predominates in both sectors. The country maintains an extensive health facility network, with a healthcare unit typically within 1.4 km of any residence, and free government Western-medicine services accessible within 4.8 km. Specialised provisions also exist for the armed forces and police, ensuring broad geographic coverage and multiple points of access. 69
Migraine care is generally provided by non-specialist doctors as well as specialists in neurology and general medicine in outpatient settings across both public and private sectors. Dedicated headache specialists are not available in Sri Lanka; complex or refractory cases are usually referred to general neurology specialists. Neurologists are present in most districts, with higher concentrations in densely populated and urbanised regions. Major hospitals in select districts, particularly Colombo, Kandy, Galle, and Jaffna, have dedicated headache clinics. In other hospitals, patients with migraine are typically managed within general neurology or general medical clinics. Advanced diagnostic services, such as magnetic resonance imaging, are available only in major cities.
Barriers to care
Despite the well-structured healthcare delivery system detailed above, several barriers to migraine care prevail. From a patient perspective, headache related health – seeking behaviour is somewhat restricted by cultural beliefs. This occurs when headache is not identified as a symptom, but as an expected result of social or personal struggles. This is more so in rural populations who have limited access to headache education and specialist care. Anecdotally, many patients referred to our services have endured migraine for years without receiving an accurate diagnosis and have been treated incorrectly for conditions such as vision problems, sinusitis, dental pain, tension type headache or hypertension. Even among those who were correctly diagnosed, most had only been offered simple analgesics, despite clear indications for preventive therapy.
Sri Lanka does unfortunately suffer from a shortage of trained physicians and according to government statistics there were 42 neurologists in the government service in 2022 which translates to approximately 0.33 neurologists per 100,000 population. 69 This is a stark contrast to 7.1 neurologists per 100,000 in high income countries, and even the global average of 3.1 neurologists per 100,000 people. 70 Consequently, there is reduced availability of neurologists to provide dedicated migraine care, especially in rural communities, as well as a diminished capacity to train other healthcare professionals in the principles of effective migraine management.
At present, treatment options for patients with migraine, especially those who suffer with the chronic form remain suboptimal. While newer treatment options such as CGRP monoclonal antibodies, gepants, ditans and neuromodulation devices are not available in Sri Lanka, the limited availability of standard treatments such as Onabotulinum toxin A and triptans creates challenges for prescribers and disadvantages migraine patients. Furthermore, the widespread availability of acute analgesics throughout the country acts as a double-edged sword due to less stringent prescribing policies. Unrestricted over the counter purchase of pain relief medications leads to increasing incidence of medication overuse headaches, a known barrier to effective migraine management.
The paucity of data on migraine in Sri Lanka including epidemiological and demographic data is a significant challenge for healthcare planning and advocacy for improved resources for migraine care in Sri Lanka. Limited institutional support for researchers, including insufficient funding, lack of protected research time, and avoidable logistical obstacles, has been a challenge for the development of a robust research culture within the medical community that motivates researchers. 71
The absence of patient and professional organizations related to migraine has significantly limited efforts to advocate for enhanced support and funding for the development of comprehensive migraine services and research.
Availability and use of evidence-based treatments
In Sri Lanka, the public healthcare system provides a range of acute and preventive migraine treatments within the essential medicines framework. 72 The availability of various forms of migraine therapies in Sri Lanka is detailed in Table 4. Commonly used acute agents include NSAIDs, simple analgesics such as paracetamol, and, in certain settings, combination analgesics. Preventive therapy typically relies on low-cost treatments. These medicines are generally accessible in secondary and tertiary care institutions, though stock-outs and variable prescribing practices may occur. Comprehensive national-level utilisation data, such as prescription claims or patient registry information, are currently unavailable, limiting evaluation of real-world treatment coverage and adherence.
Availability of acute and preventive migraine treatments in Sri Lanka

FR = fully reimbursed, GSL = general sales list, off the shelf, N = No, NR = not reimbursed, P = Pharmacy only, without prescription, PoM = prescription only medicine, Y = Yes.
In the private sector, a broader spectrum of medications may be accessible, however, such access is concentrated in urban and semi-urban areas, and affordability remains a major barrier, particularly for chronic preventive use. Over-the-counter availability of some analgesics without prescription oversight may contribute to medication overuse headache in certain patient populations, although no published local studies have quantified this risk.
Specific treatments such as novel anti-CGRP agents and neuromodulatory device therapies are currently unavailable in either sector. Onabotulinum toxin A is available in the state sector, however the availability can be unpredictable resulting in treatment disruptions.
The global practice recommendations of the International Headache Society have established essential as well as optimal treatments to facilitate policy changes for migraine care.56,73 However, in the 2022 revision of Sri Lanka's National Essential Medicines List, several drugs historically used in migraine management were removed compared to the 2013 version (Table 5).72,74 Although this is in contrast to the global practice recommendations of the International Headache Society, these changes likely reflect national efforts to rationalise the list in line with cost-effectiveness priorities and severe procurement constraints during the recent economic crisis.
Comparison of acute and preventive migraine medications listed in the national list of essential medications in 2013 and 2022.

Y = listed; N = not listed.
Other treatments
Despite Western medicine being well established and accessible across the island, complementary/alternative medicine is also utilised for migraine management. According to a World Health Organization (WHO) review conducted between 2015 and 2019, traditional medicine systems were reported to have catered to up to 75% of the population especially in rural areas. 75 Four traditional medicine systems: Ayurveda, Desheeya Chikitsa (indigenous medicine), Siddha, and Unani are recognised in Sri Lanka. 76 Treatment options utilised in each system are summarised in Table 6. Traditional systems offer highly personalised and often holistic care and are culturally trusted. Ayurvedic practices are the most well documented amongst the traditional systems, however, standardization is variable and is often practitioner dependant. Ayurveda is by far the most widely practiced and is part of the national health service under the purview of the Ministry of Indigenous Medicine.
Traditional medical systems for migraine management in Sri Lanka.

Colombo is home to the Ayurveda National Hospital of Sri Lanka; additionally, many privately owned clinics, and wellness retreats are distributed throughout the country. Although the Ayurveda National Hospital offers free services, all other expenses such as outpatient medications are borne by patients, with no targeted reimbursement strategies apart from personal health insurance.
Education in migraine
The Association of Sri Lankan Neurologists (ASN), established in 2007 is the primary professional organisation for neurology in Sri Lanka, and is the epicentre of education in migraine. 77 The ASN conducts annual academic meetings to promote neurology education and research in Sri Lanka. By maintaining close links with many similar international organisations including the World Federation of Neurology (WFN), the Association of British Neurologists (ABN) and the International Headache Society (IHS) the ASN regularly hosts international experts to their annual meeting, which invariably includes a dedicated session for headache disorders. Furthermore, the ASN conducts regional meetings and regular one day ‘Neurology Updates’ which offer CME for neurology trainees. Over the course of a calendar year at least one ‘Neurology Update’ is dedicated to Headache education.
Migraine education begins formally in medical school where undergraduate students are introduced to the pathophysiological basis of migraine and given a brief overview of the principles of management. Headache is one of the major topics included in the structured 3-year training programme in neurology laid out by the Postgraduate Institute of Medicine (PGIM) in conjunction with the ASN, with emphasis on migraine management. The programme includes a year of training overseas, most often in the UK, during which neurology trainees can expand their experience and gain exposure to newer treatment options that are not yet accessible in Sri Lanka.
Although there are no associations dedicated to headache at national level at present, the ASN encourages all members to obtain membership of the International Headache Society (IHS), and similar regional organisations. The ASN also offers travel grants for their members to attend and present at international headache conferences and seminars.
Advocacy and initiatives
Initiatives to improve the public awareness of the burden of migraine in Sri Lanka have been scarce. Only a handful of activities have been undertaken in the last 10 years, and these were carried out mostly by the ASN or its individual members.
The ASN provides information for patients on common neurological conditions though the Patient Education page of their official website. This page contains a section on Migraine with generic information on migraine with a two-page document which can be downloaded and has been shared though social medial platforms. 78 This information is available in the two official languages; Sinhala and Tamil, and also in English.
Several feature articles on migraine have been published in the mainstream newspapers, however, only about 10 articles have been published in the last 10 years. These include discussions with eminent neurologists from Sri Lanka or abroad,79–87 or articles written by journalists.88,89 Although only 31% of the population is able to read and write English language, 90 most of these articles are in English, and only a few were published in the two official languages of the country. To date, no regional or national public awareness campaigns on migraine have been conducted in Sri Lanka.
There are no migraine charities or patient organizations that are active in Sri Lanka. While the ASN is involved in promoting migraine care, Sri Lanka does not have a dedicated association for headache disorders.
Many patients continue to carry out their day-to-day activities and attend work while experiencing severe migraine attacks and are not offered suitable work adjustments. 91 The national occupational safety and health policy of Sri Lanka primarily focuses on work-related injuries and diseases, with minimal emphasis on adapting the work environment to individual needs, which is a barrier for migraine patients in receiving appropriate support within the workplace. 92
Due to the cost, newer migraine medications such as CGRP monoclonal antibodies or gepants are unlikely to be included in the national essential medications list, however, less costly medications such as triptans are undoubtedly necessary for migraine care. Sumatriptan was listed in the national list of essential medicines of Sri Lanka 2013–2014 edition, 74 however, none of the triptans are included in the national list of essential medicines published in 2022. 72 This underscores the lack of policy-level support for migraine care, representing a significant barrier to the development and improvement of services for patients living with migraine.
Future directions for migraine care in India and Sri Lanka
Optimizing access to drugs and bringing anti-CGRP therapy under national insurance coverage in India will help the large population base of patients suffering due to migraine-associated disability. Technology can help incorporating digital health tools monitoring stress and exercise goals in order to maintain healthy lifestyles and reduce stress. There is space for building regional registries in headache in all areas of India to generate data and study the disease patterns and evolution. Increased participation is required from academic bodies need to emphasize on collaborative research and develop databases and generate evidence that caters to the Indian population.
For Sri Lanka, universal health coverage and a manageable population are advantages, but several challenges remain. Future efforts should focus on expanding access to evidence-based therapies, and the development of dedicated headache clinics in major hospitals and district-level centres. Research and development of technology need to be prioritized and incentivized with financial support from policy-makers to keep abreast of global standards and establishing a national association for the study and advancement of headache medicine is an important next step to advocate for such policy changes.
Leveraging digital health tools such as telemedicine consultations, mobile headache diaries, and artificial intelligence–based diagnostic tools may help overcome geographic and infrastructural barriers, ensuring more equitable and efficient migraine care in both India and Sri Lanka, as well as other countries in the region. However, with health system which typically have outdated systems and administrative processes that discourage innovation, the successful implementation of such changes would require strong political and institutional commitment alongside substantial financial investment and advocacy from both the medical community and patient organizations in the region.
Finally, collaborative efforts of these two adjacent nations as well as other countries of the Indian subcontinent are a way forward to develop regional research and practice standards for this condition which significantly affects the economically productive population.
Conclusion
Migraine care in India and Sri Lanka is a constantly evolving landscape. Despite recent advances in the treatment of migraine, access to newer therapeutic options remains limited in the region, which places migraine patients in the region at a disadvantage. Cost of these treatments remains a major barrier to optimal migraine care in the region, and policy changes are needed to improve affordability and ensure equitable access to these treatments for the wider population.
While there have been significant strides in both nations in terms of research and practice, there is space to generate regional research, international collaboration and intersectoral convergence to further improve the QOL of people suffering from migraine in these two countries and across the region.
Article highlights
Migraine is not yet treated seriously despite being a disabling condition in the economically productive age group
Several strides in research and evidence-based practice in India, and universal free health coverage in Sri Lanka are innate strengths of both nations.
Widespread use of alternative medications with several quality publications supporting its use in reducing migraine burden. Pioneering research on utility of nerve blocks and yoga in India.
Footnotes
Abbreviations
Consent for publishing
The authors agree to publish the review with Cephalalgia Reports.
Author contributions
The title search for Indian subsection was independently conducted by VS and SR, full text reviews were conducted by VS and SR independently, and disagreements were resolved by KC, original draft was written by VS. Verification of clinical trials were done by AK and KC. Literature search and original draft of Sri Lankan subsection was done by AR, DW and PA, review and editing done by PA and BS. Final editing and redrafting of combined manuscript was done by SR and PA. All authors have reviewed and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data sets comprised in this study are available from the corresponding author and can be shared upon request.