
Abstract
Background:
Migraine affects 9.3% of Latin Americans but remains underdiagnosed and undertreated across the region.
Objective:
To examine migraine care inequities across Argentina, Brazil, Chile, Colombia, Peru, and Mexico and propose evidence-based recommendations.
Methods:
We synthesized epidemiological data, healthcare system analyses, and professional society reports to compare treatment access, medical education, and care delivery models across countries. Data sources included PubMed, SciELO, WHO reports, and ASOLAC documents. The search strategy was conducted by authors from each country and covered the period 2015–2025.
Results:
Despite high healthcare coverage (91.5–99.6%), significant care gaps exist. Neurologist-to-population ratios are critically low (1:47,000–58,000), with specialists concentrated in urban areas. Medical education provides minimal headache training (2–4 h of undergraduate training). Triptan usage varies dramatically from 0.14% (Mexican emergency departments) to 23% (Peruvian neurologists). Anti-CGRP medications remain restricted only to private healthcare. Only 2.6% of eligible Brazilian patients receive preventive therapy. Rural patients face wait times of 3–5 years for specialty care, compared with immediate access in the urban private sector. Emergency department utilization remains high, with 179,618 migraine-related visits in Mexico (2013–2022).
Conclusions:
Despite strong healthcare coverage, migraine care requires systematic reform. Priority interventions include expanding triptan access in public systems, standardizing medical education, developing telemedicine networks, and coordinating health promotion to distinguish primary from secondary headaches. When adapted to national contexts, these strategies could substantially improve diagnosis and outcomes over the medium term.
This is a visual representation of the abstract.
Keywords
Introduction
Migraine remains one of the leading causes of disability worldwide, ranking second in years lived with disability (YLDs) according to the Global Burden of Disease Study 2019. Since GBD does not estimate any deaths from headache disorders, DALYs (Disability-Adjusted Life Years) are equivalent to YLDs for headache disorders. 1 It has a significant impact on the quality of life, especially among women and younger people. In Latin America, the burden of migraine is worsened by deep-rooted socioeconomic inequalities, division within healthcare systems, and limited training of medical practitioners. 2
The study design explicitly realized a narrative review synthesizing epidemiological data, healthcare system analyses, and professional society reports, using as data sources included PubMed/MEDLINE, SciELO (Scientific Electronic Library Online), WHO, and PAHO (Pan American Health Organization) reports, ASOLAC documents and member surveys, national health ministry databases, and professional society documentation. Our search strategy covered the period 2015–2025 and the languages Spanish, Portuguese, English, and French. The search terms: “migraine,” “migraña,” “enxaqueca,” “cefalea,” “headache,” “Latin America,” “healthcare access,” “treatment,” “epidemiology,” and Country-specific terms combined with treatment and healthcare delivery terms. The inclusion criteria were (a) Published studies on migraine prevalence, treatment, or healthcare access, (b) Reports from health ministries and professional organizations, (c) Data from Argentina, Brazil, Chile, Colombia, Mexico, and Peru, and (d) Publications in Spanish, Portuguese, English, or French. The exclusion criteria were (a) Studies focused solely on pediatric populations, (b) Case reports and small case series, (c) Studies without clear methodology, (d) non-peer-reviewed sources (except official government and professional society reports). The data synthesis described how country-level experts collected and verified data, with disagreements resolved through consensus discussion. This expanded methodology follows SANRA (Scale for the Assessment of Narrative Review Articles) guidelines for narrative reviews and provides readers with sufficient detail to evaluate the robustness of our synthesis (Table 1).
Data sources and languages for migraine care in Latin America research.

Systematic Review Period: 2015–2025.
(a) Primary languages: Spanish and Portuguese (official languages in studied countries).
(b) English included for international publications and comparative studies.
(c) French included for WHO/PAHO documents (official UN language).
(d) Search terms adapted to each language and regional terminology variations.
(e) Countries included: Argentina, Brazil, Chile, Colombia, Mexico, Peru.
This paper reviews the current state of migraine care in six Latin American countries: Argentina, Brazil, Chile, Colombia, Peru, and Mexico. For each country, it identifies structural and clinical challenges. It proposes strategies to improve diagnosis, expand access to treatment, and enhance physician education, with the ultimate goal of improving outcomes for individuals living with migraine (Table 2–7 and Figure 1).

Migraine care in Latin America: regional analysis healthcare coverage and neurologist density by country (2015–2025).
Regional burden: migraine prevalence across six Latin American countries.
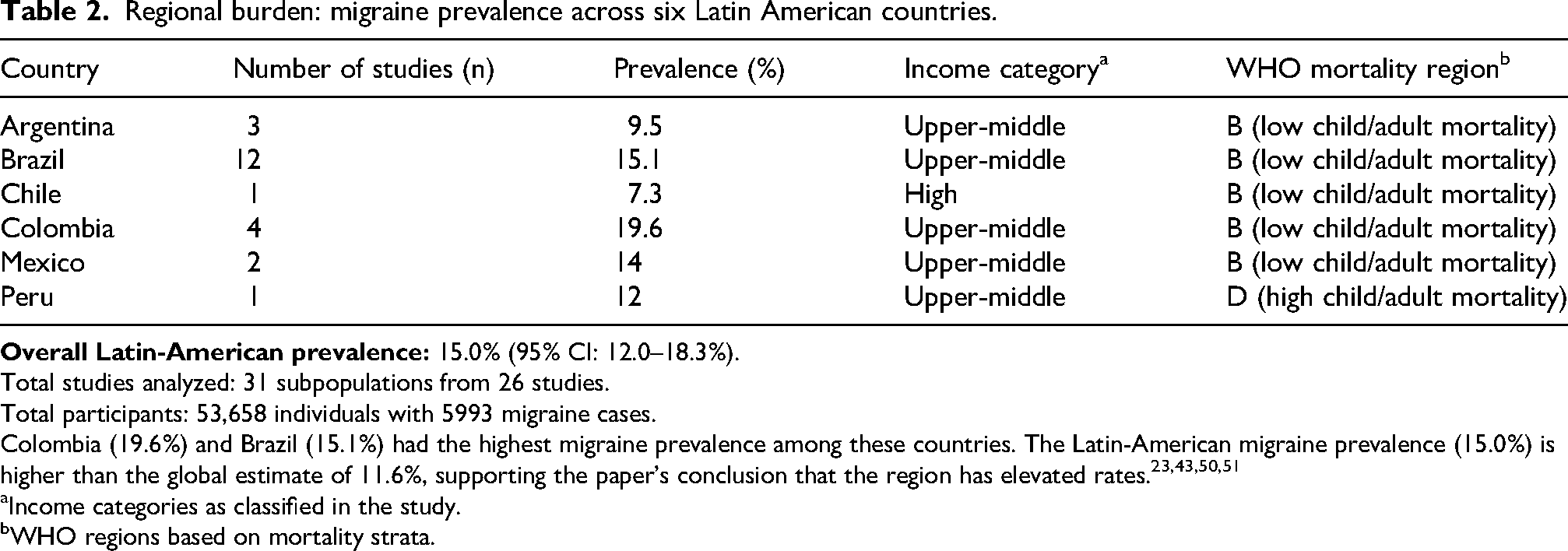
Total studies analyzed: 31 subpopulations from 26 studies.
Total participants: 53,658 individuals with 5993 migraine cases.
Colombia (19.6%) and Brazil (15.1%) had the highest migraine prevalence among these countries. The Latin-American migraine prevalence (15.0%) is higher than the global estimate of 11.6%, supporting the paper's conclusion that the region has elevated rates.23,43,50,51
Income categories as classified in the study.
WHO regions based on mortality strata.
Neurologist-to-population ratios highlighting workforce constraints in migraine care across Latin America

Abbreviations: SUS = Sistema Único de Saúde (Brazil); FONASA = Fondo Nacional de Salud (Chile); SGSSS = Sistema General de Seguridad Social en Salud (Colombia); SIS = Seguro Integral de Salud (Peru); EsSalud = Seguro Social de Salud (Peru); IMSS = Instituto Mexicano del Seguro Social (Mexico); ISSSTE = Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (Mexico).
Treatment utilization patterns: documenting the evidence-practice gap.

Abbreviations: GBD = global burden of disease; ED = emergency department; CGRP = calcitonin gene-related peptide. Utilisation metrics differ by country and data source.
Disproportion between migraine burden and formal headache training in medical education.

Abbreviations: SBCe = Sociedade Brasileira de Cefaleia (Brazilian Headache Society); ABRACES = Associação Brasileira de Cefaleia e Enxaqueca; ACEFALCH = Asociación Chilena de Cefalea y Dolor Craneofacial; AMCEMIG = Asociación Mexicana para el Estudio de la Migraña y Cefalea; ASOPECE = Asociación Peruana de Cefalea; IHS = International Headache Society.
Treatment accessibility: comparing public and private healthcare sectors.

Abbreviations: NSAIDs = nonsteroidal anti-inflammatory drugs.
System-level indicators of access, utilization, and treatment failure in migraine care.

Data availability varied by country and indicator; absence of data does not imply absence of the problem.
Country-specific overviews
Argentina
General practitioners provide migraine care. Access to neurologists and advanced treatments is limited to urban and privately insured populations. Triptan use remains low, and medical education varies. The Red Latinoamericana de Cefaleas (RedALCeF) aims to improve education and develop regional guidelines for headache management.
Migraine constitutes a major public health challenge in Argentina, affecting 9.5% of the adult population, with marked gender differences. Women present a prevalence of 14% compared to 5% in men, translating to approximately 4.3 million Argentinians who experience this condition. Chronic migraine, the most disabling form, affects 1.5% of the population and is frequently associated with excessive analgesic consumption. 3
The country's genetic, socioeconomic, and climatic heterogeneity generates considerable disparities in regional prevalence, underscoring the need for tailored health policies adapted to each local context. 4
The Argentine health system provides multiple access points for managing migraine through three main sectors. The public sector offers free care in national, provincial, and municipal hospitals, ensuring universal access. Social security includes union-based health plans, the National Institute of Social Services for Retirees and Pensioners, and provincial health insurance programs, all of which are funded through labor contributions. The private sector encompasses prepaid medicine and private insurance. 5 According to the 2022 census, 60.9% of the population has some form of social or prepaid coverage, 35.8% rely solely on public health services, and 3.3% access specific government programs. This fragmented system presents unique challenges for comprehensive migraine management. 6
Despite universal coverage, considerable disparities in access to specialized care persist. The main obstacles include notable geographic differences, with many headache specialists concentrated in large urban areas, which limits access for rural communities and smaller cities. Long wait times for specialized appointments and inconsistent quality of care across various sectors worsen these challenges. This issue is aggravated by the absence of standardized protocols and the limited number of headache specialty centers, which are not evenly distributed across the country. 4
Evidence-based treatments for migraine face substantial access barriers. Triptans, considered a first-line treatment for acute migraine, have variable availability depending on the health sector, with more limited access in the public sector and relatively high costs that impact therapeutic adherence. New anti-CGRP medications, such as erenumab and fremanezumab, are limited in availability due to their high costs and limited coverage by public and private insurers. Gepants, including rimegepant and atogepant, encounter similar limitations, confining these innovative treatments to sectors with greater economic capacity. 5
Education on headaches in Argentine medical schools receives inadequate attention, given their rate and complexity. In undergraduate training, students get only a few hours of dedicated headache education, with the subject being covered indirectly in other parts of the curriculum. During postgraduate education, neurology residency programs in Buenos Aires include specific rotations in headache clinics at leading hospitals. However, specialized headache training elsewhere in the country is limited and requires more standardization and expansion. Although headache fellowship programs exist, they still lack official recognition from educational authorities. 6
The Argentine Neurological Society, through its headache working group, develops specific programs to strengthen care for patients with migraine. These include clinical practice guidelines tailored to the Argentine context, taking into account local availability of medications and diagnostic resources, as well as disseminating their findings. 7 In 2024, the creation of a dedicated headache research laboratory within the Mercedes and Martín Ferreyra Medical Research Institute was authorized, signifying a notable step forward in developing national research capacity and sharing its findings. Additionally, partnerships have been established with international organizations, such as the International Headache Society, to develop educational programs and facilitate scientific exchange.
Brazil
Migraine places a significant public health burden in Brazil, being the leading cause of outpatient neurology visits. Its one-year prevalence is estimated at 15.1%, unequally impacting women, those with higher education but lower income, and individuals who do not exercise regularly. Economic impacts stem from decreased productivity, absenteeism, and reduced social engagement. GBD 2019 data show that Brazil’s age-standardized incidence rates surpass the global average.8–10 Worldwide, migraine ranks second in years lived with disability (DALYs) and first among people under 50, making it Brazil's second most common and most disabling non-communicable disease. 11
Brazil’s universal Sistema Único de Saúde (SUS) operates a tiered model, with primary care serving as the entry point and secondary services providing referrals to specialized services, such as neurology, with a neurologist ratio of 1:47,000.
Despite coverage, migraine treatment is hampered by low public awareness, uneven distribution of professionals, and inconsistent medication supply. From 2009 to 2018, SUS recorded 59,615 migraine hospitalizations (BRL 19.37 million) and 300,162 outpatient procedures (BRL 17.09 million), representing increases of 242% and 314%, respectively. 12 Workforce shortages and the urban concentration of specialists leave general practitioners managing the majority of cases.
Headache disorders are not included in Brazil’s National Health Survey (PNS), so many public-health policies overlook them. Nevertheless, the Brazilian Headache Society (SBCe) has led education efforts, conducted nationwide surveys, and integrated headache medicine into the curriculum. Besides, the Brazilian Association of Cluster Headache and Migraine (ABRACES) has advanced advocacy efforts.12,13 Over 80% of people with migraine experience disability, yet underdiagnosis and undertreatment persist. 11 A 2011 survey found that over 90% of those needing preventive therapy were untreated; in metropolitan regions, nearly 30% receive no prophylaxis. 12 Approximately 5.5 million Brazilians (9.5 million, including probable cases) would likely require preventive care, yet only 7.7% of high-disability patients (MIDAS > 10) receive any prophylaxis, and only 2.6% receive it appropriately.14,15 Tertiary centers report that 31.8% of patients have failed 3 or more preventive regimens. Geographic, economic, and social factors—medication supply gaps, rural-urban disparities, and stigma—exacerbate these challenges.14,15
Triptans are approved but confined mainly to private care. In SUS, acute management relies on nonspecific analgesics (dipyrone, paracetamol, NSAIDs), whose availability varies. 16 Preventive options in SUS are limited to valproate, amitriptyline, and propranolol in select regions; other effective therapies, such as topiramate, venlafaxine, onabotulinumtoxinA, anti-CGRP monoclonal antibodies, and anesthetic nerve blocks, are accessible only privately.17,18 Fragmented availability underlies the persistent treatment gap, and systematic monitoring of outcomes is scarce.
Patients widely use non-pharmacological measures, including acupuncture, mindfulness, and physiotherapy. A Brazilian RCT in a low-income community found multidisciplinary interventions equally effective for primary headache management, underscoring their cost-effectiveness and community potential. 19
Medical schools often provide insufficient migraine education, contributing to underdiagnosis and suboptimal care. Neurology residency programs offer more training in headache management, but the annual output of specialists remains inadequate. SBCe and ABRACES lead continuing education and research efforts; however, there is no formal certification for headaches. 20
In 2019, SBCe and ABRACES organized a seminar in Brasília that culminated in the Brasília Declaration, which integrated headache disorders into public health agendas. In 2024, SBCe's Committee on Public, Institutional, and Advocacy Policies reactivated the Working Group on Migraine/Headache, enhancing interinstitutional collaboration. Proposals to CONITEC include updating topiramate indications, incorporating onabotulinumtoxinA for chronic migraine, approving triptans for acute care, and developing comprehensive clinical protocols.20–22
The “Maio Bordô” campaign is Brazil’s flagship initiative for migraine awareness. In 2025, government buildings were lit and displayed messaging nationwide to reduce stigma and encourage early diagnosis and care.
Despite universal healthcare, Brazil still faces significant gaps in migraine care: high disease burden, poor management, unequal access to modern therapies, and a lack of specialized policies. However, ongoing advocacy, research, and adapted treatment strategies provide a clear path forward. Coordinated policy implementation, educational improvements, and broader access to evidence-based treatment are crucial to closing these gaps.17–22
Chile
The prevalence of primary headache disorders in Chile is 39.7%, with migraine affecting 7.3%, tension-type headache (TTH) 24.3%, and chronic headache 2.6% of the population. 23 Specialist care is available in major cities, where neurologists are more readily accessible. Triptans are available but not widely used in clinical practice. The Chilean Headache Society emphasizes ongoing education and residency training, supported by International Headache Society (IHS) programs. However, access to specialized care in rural areas remains a major challenge.
The Chilean healthcare system is organized into three main groups: FONASA (Fondo Nacional de Salud, public insurance), ISAPRES (private insurers), and DIPRECA and CAPREDENA (insurance programs for military and police forces). Each entity provides the primary financial support for care in private clinics and healthcare centers. Approximately 82% of the population is insured through FONASA. 24 Patients seek care based on their insurance type. FONASA beneficiaries access primary healthcare centers located near their homes, where general practitioners or family physicians provide initial care. These professionals may refer patients to secondary-level centers where neurologists are available, although not necessarily headache specialists. 25 However, there are no specific timelines for these referrals in Chile, which can result in delays of several years. FONASA patients are exempt from paying for consultations.
Most specialists are concentrated in the capital, Santiago. However, the Chilean Ministry of Health has programs to send general neurologists to various regions across the country. In the Chilean healthcare system, patients can choose to receive treatment at any private facility, regardless of their insurance coverage. However, this option is often expensive and restricts access, leading to inequities. Additionally, most specialists work within the private sector, making it more common to find neurologists specializing in headache disorders there. 26
Patients with ISAPRE coverage, as well as those enrolled in FONASA, can consult neurologists directly with a co-payment, potentially enabling quicker, more direct access to specialized care. Most specialists are concentrated in Santiago, the capital, although the Chilean Ministry of Health has implemented programs to deploy general neurologists to various regions across the country. In the Chilean healthcare system, patients can choose to receive treatment at any private facility regardless of their insurance coverage. However, this option is often expensive and restricts access, leading to significant healthcare inequities. Additionally, most specialists work within the private sector, making it more common to find neurologists specializing in headache disorders in private practice. 26 Specific medications for migraine are generally not fully covered by the public healthcare system, leading to substantial out-of-pocket expenses for patients and further restricting treatment access. In some cases, supplemental private insurance (available at additional cost) may provide better reimbursement for certain migraine medications. 27
There is an apparent shortage of headache specialists in Chile, creating a critical need to improve general practitioners’ training, expand coverage with well-trained healthcare professionals, and ensure the availability of both preventive and acute migraine treatments. Greater awareness and understanding by public authorities and society at large are also crucial for improving migraine care. 25
Several preventive treatment options are available in Chile for managing migraine. Both nonspecific preventive therapies and newer CGRP-targeted treatments are accessible, including erenumab and rimegepant. OnabotulinumtoxinA has been used in Chile for years; this medication was first registered with the Health Registry in 1994 under its trademark name. 26
For the management of acute headache episodes, three triptans are available in Chile: eletriptan, naratriptan, and rizatriptan, as well as rimegepant. A wide range of NSAIDs is also accessible for treating acute migraine attacks. 26 Various non-pharmacological treatments, including acupuncture, meditation centers, mindfulness training, and yoga, have become more popular in recent years as complementary approaches to migraine management.
Headache disorders receive limited and inadequate attention during undergraduate medical education in Chile. Similarly, postgraduate neurology training programs at various Chilean universities offer only limited theoretical instruction on this subject, as the focus tends to be on “neurohospitalism.” 27 Very few training centers in Chile provide dedicated headache rotations during neurology residency. Currently, there are no formal postgraduate programs or diploma courses specifically focused on headache disorders. 27
In August 2024, the Chilean Association for Headache and Craniofacial Pain (ACEFALCH) was established. In April 2025, the inaugural ACEFALCH Congress took place, featuring a wide range of headache topics and strong attendance from over 300 professionals. 28 At the annual national congress, jointly hosted by psychiatry and neurosurgery under the SONEPSYN (Sociedad de Neurología, Psiquiatría y Neurocirugía) society, a dedicated headache module has been well-received. Additionally, the SONEPSYN group has been offering an annual headache module in various cities across Chile, which has also received positive feedback from attendees. 29 ACEFALCH aims to unify the study and clinical management of headache disorders in Chile, positively influencing public health policies and enhancing access to medications. The organization also supports and educates patient groups, such as the Chilean “Club de la Migraña,” thereby increasing societal awareness and engagement. 30
Colombia
Colombia has a prevalence of primary headache disorders of 42.7%, migraine 19.6%, chronic headache 8.6%, and tension-type headache 33.6%. Colombia had the highest prevalence of migraine and TTH in Latin America, according to Pacheco-Barrios et al. 23
Despite over 99.6% healthcare coverage, access to specialists remains limited (1 neurologist per 58,000 adults). 31 Triptans are prescribed to only 4% of patients, and neurologists account for just 5.6% of migraine prescriptions. The Colombian Neurology Association has responded with updated guidelines, awareness campaigns, and learning activities for healthcare professionals.
In Colombia, the health system is organized under the General Social Security System (SGSSS), which includes two regimes: contributory and subsidized. The contributory system covers both self-employed workers and employees, while the subsidized system supports low-income individuals and is funded by the state. Currently, the SGSSS has a coverage rate of about 99.6% the total population. 32 However, obstacles persist in ensuring equitable access to and quality of care across regions and socioeconomic groups. Health services are organized into three levels of care, forming a hierarchy to optimize resources. The medical primary level attention is the first contact point for individuals experiencing migraine symptoms, usually involving consultations with general practitioners in outpatient settings. At the secondary and tertiary levels, patients are seen by neurologists and other specialists in outpatient clinics, emergency departments, and hospitals. According to Rubio et al., the first line of care for patients with migraine is provided by a general practitioner in 82.6% of cases, by a neurologist in 8.9%, and by an emergency specialist in 5.7%. 33 Outpatient infusion rooms for status migrainosus cases have been established and are attended by neurologists and general physicians. 34 The limited distribution may account for the low proportion of individuals with migraine who access specialized care, with rates of 8.9% among those enrolled in health insurance programs and 4.9% in the general population.35,36
Although primary care offers greater accessibility, significant barriers remain at this level, especially regarding the clinical approach. A review revealed that most Colombian medical schools allocate 2 to 4 h to headache education, and 6.9% of primary care physicians consistently apply the ICHD-3 diagnostic criteria when evaluating patients with migraine. 37
The implementation of evidence-based treatments in the country faces major obstacles. Although oral medications are available, 92.9% of prescriptions are written by general practitioners, with only 49% following established management guidelines. Approximately 5.6% of drugs are prescribed by neurologists.38–40 The most common treatments for acute attacks include NSAIDs (46.6%), acetaminophen (43.8%), and ergotamine/caffeine (35.1%), while the most used preventive medications are flunarizine (16.3%), valproic acid (9.4%), propranolol (9.3%), and amitriptyline (8.5%). 38 The use of targeted therapies remains limited, with only 4% of patients receiving triptans at baseline. 35 OnabotulinumtoxinA saw increased use between 2018 and 2020 (15%), while galcanezumab was used by 0.2% of physicians. 10 Access barriers are primarily due to health system restrictions resulting from the high cost of medications and inadequate training for primary care physicians.
Colombia has 14 neurology residency programs, which graduate approximately 60 neurologists each year. While this improves access to specialized headache care, significant gaps remain because residency curricula do not typically require training in common, high-prevalence disorders, such as headache. 39
Nevertheless, because of educational campaigns led by the Colombian Neurology Association, headache has become the third most popular subspecialty among neurology residents in the country. 40
The Colombian Neurology Association (ACN) leads initiatives to improve care for patients with migraine through its headache committee. It organizes the National Neurology Congress and the Colombian Headache Symposium to update neurologists on advances in diagnosis and treatment. It serves as a consulting body for the Ministry of Health and the drug-approving agency INVIMA. It has published treatment guidelines based on consensus methodology and evidence for the management of migraine.40–42 In 2023 and 2024, the ACN conducted community education initiatives, “The Two Faces of Migraine” and “Migraine Journey,” utilizing social media. Despite these efforts, migraine still carries a social stigma that hampers the implementation of better patient care.
Mexico
In Mexico, migraine is a major public health concern, especially among women. According to the Ministry of Health, from 2013 to 2022, there were 179,618 emergency visits for migraine, accounting for 14–19% of all headache-related cases, with women accounting for 78% of these visits. 43 These numbers align with global trends showing an increase in migraine prevalence among people aged 15–39 years from 1990 to 2021.13,44–46
The ratio of Neurologists’ attendance to the population is 1: ∼72,000. The Mexican healthcare system includes several subsystems. The Ministry of Health provides public care for people who are not formally employed. Employees in the formal economy are covered by the Mexican Social Security Institute (IMSS). Meanwhile, government workers receive services through the Institute of Social Security and Services for State Workers (ISSSTE). Military personnel and PEMEX employees are protected by their own institutions. The private sector also plays a key role, with more citizens gaining access to care through insurance providers like AXA, GNP, Monterrey, and BBVA. Additionally, pharmacy-based clinics offering affordable consultations are becoming more common, serving as a first point of contact for patients with headaches.
Despite various healthcare options, inequities continue in the quality and continuity of care. Migraine is often underdiagnosed and undertreated. Use of triptans remains very low, reported in just 0.14% of emergency visits for migraine, 45 and access to newer treatments like anti-CGRP monoclonal antibodies is limited, probably due to cost and structural obstacles. Obstacles to optimal care include limited infrastructure, fragmented access, and inadequate training among general practitioners in current diagnostic and treatment protocols.
Deficiencies in education are also clear. Although headache disorders are part of medical curricula, they are often only briefly covered in general neurology or neuroscience courses. Many physicians receive little or no formal training in detecting and handling primary headache disorders, which leads to underuse of evidence-based treatments and overdependence on symptomatic medications.
Mexico is currently collaborating with the International Headache Society (IHS) on a joint review to develop a regional strategy to improve migraine care. This endeavor spotlights the country’s dedication to aligning local priorities with global best practices.
To address these challenges, the Mexican Association for the Study of Migraine and Headache (AMCEMIG) has launched several initiatives. It works with international organizations, such as the IHS, to improve medical education. This includes a headache management course introduced in 2023, in partnership with the Universidad Autónoma de San Luis Potosí. The association also promotes responsible prescribing practices and contributes to scientific literature.46–48 Additionally, it supports continuing medical education through diploma programs and outreach efforts aimed at physicians in pharmacy-based clinics. By raising awareness and advocating for better clinical care, AMCEMIG plays a key role in improving the diagnosis and treatment of migraine in Mexico, despite ongoing social and institutional challenges that hinder recognizing migraine as a national health priority.
Peru
Underdiagnosis and misclassification are common because general practitioners often lack adequate training. Access to neurologists is limited, and the use of triptans is low. National treatment protocols have not yet been put in place. The Peruvian Neurological Society is calling for improved training and the development of standardized protocols.
According to GBD studies, migraine causes substantial disability worldwide, particularly among women aged 15–49 years. 8 Migraine prevalence seems to have increased notably from 1990 to 2024,49,50 Migraine constitutes a major public health challenge in Peru, according to recently published data regarding the growing burden of this disease.51–55
Healthcare services in Peru are categorized into three sectors: public, military, and private. According to the 2024 Household Survey conducted by the National Institute of Statistics and Informatics of Perú, 91.5% of the country's population had health insurance. The rate was higher in rural areas (93.6%) compared to urban areas (90.5%). By type, 64.5% have Integral Health Insurance (SIS), 22.6% have Social Security (EsSalud), and 4.4% have private insurance. 56
Of the 100 people with illnesses in Peru, 33% seek medical care. Of this group, 39% visit a pharmacy or drugstore, while 35% go to Ministry of Health (MINSA) facilities. 14% use Social Health Insurance (EsSalud), and 11% visit a private practice. 57 According to the Peruvian Medical Association, the 700 registered neurologists nationwide are insufficient to meet the demand for care for over 32 million residents, who are mostly concentrated in the capital city. 45 Requesting a prescription from untrained pharmacy staff is an inappropriate but common practice among migraine patients in Peru. 58
Evidence-based migraine treatments face significant challenges in Perú. Triptans are not included in the Pharmacological National List but are available in pharmacies. High patient costs create a major barrier to practical implementation. Currently, we do not have access to monoclonal antibodies or ditans. Recently, Rimegepant has entered the market, but it is only affordable in private practices due to its high price. A survey of Peruvian neurologists revealed that 27% prescribe NSAIDs for migraine, 23% use Triptans as monotherapy, 14% combine Triptans with other analgesics, 14% prescribe ergotamine, and 7% give opioids. Additionally, 88% reported that they were unaware that using opioids for migraine headaches is not considered best practice. 59
There are no officially recognized programs for headache subspecialty in the country. An average of 4 h of headache-related topics is covered in pre-med training. There is no formal headache training during the Neurological Residency. Neurologists interested in headache care often travel abroad for rotations at specialized centres. 58 The Peruvian Society of Neurology has a headache chapter that organizes an annual two-day headache conference, featuring both international and national professors.
In 2025, the Peruvian Headache Association (ASOPECE), in partnership with the International Headache Society (IHS) and the University of Piura, launched a 6-month Diplomate Programme in Headache and Facial Pain. This initiative aims to enhance medical knowledge at the primary care level through regional courses.
Despite the significant impact of headaches and migraine, they are often overlooked by both healthcare professionals and the public. Currently, Peru lacks a dedicated headache patient association, emphasizing the need for advocacy.
To address the educational gap in headache care, ASOPECE is focusing on academic improvement through its Diplomate program. Meanwhile, AcefaPeru aims to empower neurologists and researchers with annual International Congresses. By encouraging young neurologists to specialize in headaches, we hope to foster expertise and improve patient care.
Insufficient education among medical students and practitioners, along with a lack of appropriate medications, hinders effective management. ASOLAC is committed to increasing the number of headache specialists in Peru to elevate healthcare management and treatment for patients.
Common challenges
Across the six countries analyzed, several recurrent barriers to effective migraine care were consistently documented (Figure 2, Tables 3–7). First, evidence-based acute and preventive treatments remain underutilized across healthcare settings. Triptan prescription rates ranged from 0.14% of migraine-related emergency department visits in Mexico to 23% among Peruvian neurologists, while CGRP-targeted therapies were largely restricted to private healthcare or absent from national formularies.

Challenges in diagnosing and treating headaches in Latin America.
Second, the limited availability of neurologists and headache specialists was observed throughout the region. Neurologist-to-population ratios ranged from approximately 1:29,000 to 1:72,000, with specialists predominantly concentrated in capital cities and major urban centers, resulting in restricted access for rural and underserved populations.
Third, formal medical education in headache disorders was consistently limited. Undergraduate and postgraduate training programs across countries typically allocate only 2–4 h to headache medicine, despite migraine representing a leading cause of disability.
Fourth, fragmented healthcare systems characterized by parallel public and private sectors contributed to marked inequities in access to diagnosis and treatment. Patients relying on public systems frequently experienced prolonged waiting times for specialist care and restricted formularies, whereas privately insured patients had more immediate access to specialists and migraine-specific therapies.
Finally, migraine continued to be under-recognized as a disabling neurological condition, with persistent social stigma and low prioritization in public health planning reported across multiple countries.
Discussion
This narrative review highlights a consistent regional paradox in migraine care across Latin America: despite high levels of formal healthcare coverage, access to timely diagnosis and evidence-based treatment remains highly unequal. The findings summarized in the Results and Common Challenges sections indicate that migraine continues to be underdiagnosed and undertreated, leading to preventable disability, excessive emergency department utilization, and substantial socioeconomic burden.
Although a regional perspective is adopted, the observed patterns do not imply homogeneity across countries. Health-system organization, financing mechanisms, workforce distribution, and pharmaceutical policies vary widely among Argentina, Brazil, Chile, Colombia, Mexico, and Peru. Accordingly, the disparities identified should be interpreted as shared challenges with distinct national expressions rather than uniform system failures, and any proposed strategies require contextual adaptation.
One of the most influential contributors to inequitable migraine care is the geographic concentration of neurologists and headache specialists in capital cities and major urban centers. This pattern reflects long-standing structural factors, including centralized medical education, limited specialist posts in rural areas, and economic incentives favoring private urban practice. Consequently, rural and peri-urban populations experience prolonged delays in specialist access, increasing the risk of misdiagnosis, inappropriate treatment, and progression to chronic migraine.
Economic stratification further reinforces inequity. Across all reviewed countries, a two-tiered model persists in which patients with private insurance or greater financial means can access triptans, CGRP-targeted therapies, onabotulinumtoxinA, and specialist consultations, while those dependent on public systems are largely limited to nonspecific analgesics and restricted preventive options. This disparity highlights the distinction between healthcare coverage and effective therapeutic access.
A consistent finding across countries is the mismatch between migraine burden and formal medical education. With migraine affecting a substantial proportion of the adult population, the limited curricular exposure to headache medicine has cascading consequences, including low diagnostic confidence in primary care, poor adherence to evidence-based guidelines, and unnecessary referral pressure on specialist services.
Despite these challenges, several opportunities for improvement are evident. All six countries possess healthcare infrastructures capable of supporting targeted reforms. Professional societies have demonstrated increasing leadership in education, advocacy, and guideline development, often in collaboration with international organizations. In parallel, the expansion of telemedicine following the COVID-19 pandemic offers a pragmatic mechanism to reduce geographic inequities and extend specialist expertise to underserved regions.
Overall, the findings suggest that meaningful improvements in migraine care do not require entirely new systems, but rather the strategic realignment of existing resources through education, service organization, and equitable access to evidence-based therapies.
Conclusion
This narrative review demonstrates that near-universal healthcare coverage in Latin America has not translated into equitable migraine care. Persistent structural barriers—including workforce shortages, geographic maldistribution of specialists, insufficient medical education, economic stratification of treatment access, and limited availability of migraine-specific therapies—continue to leave millions of individuals without effective diagnosis and management despite formal insurance coverage.
As a narrative synthesis, this analysis has inherent limitations. Data availability and quality vary substantially across countries, and many estimates rely on heterogeneous sources, including epidemiological studies, administrative databases, and professional society reports. The descriptive nature of the review precludes causal inference, and rapid policy evolution means that some barriers may have been partially addressed since the publication of the source data. Nonetheless, the convergence of findings across diverse national contexts supports the robustness of the identified patterns.
Despite these constraints, the review highlights clear opportunities for progress. Expanding access to essential acute and preventive treatments, strengthening headache education at undergraduate and postgraduate levels, leveraging telemedicine to reach underserved populations, and elevating migraine within national non-communicable disease agendas represent realistic and impactful strategies. Achieving meaningful improvement will sustain collaboration among governments, professional societies, academic institutions, patient organizations, and international partners. Given migraine substantial's contribution to disability and lost productivity, such investments have the potential to generate significant returns in population health, economic performance, and social well-being across the region.
Public health relevance
Migraine remains underdiagnosed and undertreated across Latin America.
Specialist care is concentrated in urban areas, with rural waits up to five years.
Triptan and anti-CGRP access is limited mainly to the private sector in most countries.
Medical schools offer only 2–4 h of headache education on average.
Regional telemedicine and unified advocacy could bridge major care gaps.
Footnotes
Acknowledgements
The authors would like to sincerely thank the International Headache Society (IHS) for its trust and support in the development of this study. We also acknowledge the Latin American Headache Association (ASOLAC) for its leadership in promoting collaboration, education, and research in headache medicine across the region. We thank all national neurological societies and contributors who provided data, reports, and expert input that made this regional synthesis possible, including the Argentine Neurological Society, Brazilian Headache Society (SBCe), ABRACES, Chilean Association for Headache and Craniofacial Pain (ACEFALCH), Colombian Neurology Association, Mexican Association for the Study of Migraine and Headache (AMCEMIG), and Peruvian Headache Association (ASOPECE). Finally, we thank Claude AI (Anthropic) for assistance with document organization and formatting during the revision process.
ORCID iDs
Ethical considerations
This study is a narrative review based on previously published data, institutional reports, and publicly available sources. It did not involve direct interaction with human participants, patient data collection, or identifiable personal information. Therefore, formal ethical approval was not required in accordance with institutional and international guidelines.
Consent to participate
Not applicable. This study did not involve human participants or primary data collection.
Consent for publication
All authors have reviewed and approved the final version of the manuscript and agree to its submission and publication in Cephalalgia Reports if accepted.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: María-Karina Velez-Jimenez: Speaker AbbVie- Allergan, Abbott, Pfizer, Weser Pharma. Pablo Schubaroff: Speaker AbbVie- Allergan, Pfizer, Novartis, Teva. Marco Lisicki: Speaker/Advisor: AbbVie- Allergan, Pfizer, Teva, Novartis. Mario F.P. Péres: Abbvie, Eli Lilly, Eurofarma, Libbs, Lundbeck, Novartis, Pfizer, Sanofi, Teva. Ivy Liger: Speaker, Teva. Joe Muñoz: Speaker and medical advisory services, Pfizer, AbbVie, Abbott, Novartis. Yessika Rojas-Villegas: No disclosures. Raúl Juliet: Speaker AbbVie - Pfizer-Axon. María José López: Speaker AbbVie and Pfizer. Ernesto Bancalari: Former R&D Director GSK/ Speaker Pfizer. María Teresa Reyes: Speaker, Pfizer, Adium. Ildefonso Rodriguez-Leyva: Speaker Abbvie- Allergan, Pfizer.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.