
Abstract
Introduction
Trigeminal neuralgia may be secondary to an underlying condition. Clinical findings alone are not sufficient to distinguish primary neuralgia from secondary neuralgia. Failing to recognize a cancer diagnosis can result in missed opportunities. We present two cases of trigeminal neuralgia that were initially thought to be idiopathic but turned out to be secondary to an ear, nose, and throat (ENT) cancer.
Objective
Raise awareness among clinicians to examine the entire trigeminal nerve along with its entire course, not just where it emerges from the Cerebellopontine angle.
Conclusion
This article emphasizes the importance of examining the extracranial portion of the trigeminal nerve, particularly in cases of clinical atypia and the absence of neurovascular compression.
This is a visual representation of the abstract.
Introduction
Trigeminal neuralgia is a chronic pain condition that most commonly affects individuals over the age of 50. It is characterized by sudden, severe neuralgic pain in the distribution of the trigeminal nerve, often triggered by everyday actions such as light facial touch, speaking, or chewing.
Trigeminal neuralgia can be classified as classical, when caused by a neurovascular conflict; secondary, when related to an underlying condition; or idiopathic, when no underlying cause or neurovascular conflict is identified. 1
When trigeminal neuralgia is suspected, magnetic resonance imaging (MRI) focused on the trigeminal nerve pathway is mandatory to exclude secondary causes and to assess for possible neurovascular conflict. 2
However, in clinical practice, the evaluation often focuses mainly on the intracranial segment and the nerve's point of emergence, while the distal portions of the trigeminal nerve may be overlooked. This study is reported in accordance with the CARE (CAse REports) guidelines for case reports.
In this case report, we present two patients who were initially diagnosed with idiopathic trigeminal neuralgia, based on clinical features and MRI findings showing no neurovascular conflict or underlying pathology. The first patient was referred with a diagnosis of idiopathic trigeminal neuralgia with background pain; however, given the atypical presentation and the subsequent emergence of clinical abnormalities, the diagnosis was revised to secondary trigeminal neuralgia following a reevaluation of the imaging studies. The second patient was referred with a diagnosis of idiopathic paroxysmal trigeminal neuralgia but given the change in clinical features over the course of the disease, the diagnosis was revised to trigeminal neuropathy, which led to the diagnosis of a space-occupying lesion.
Case
The first case involves a 65-year-old man with a medical history of ischemic heart disease treated with aspirin and type II diabetes mellitus managed with metformin. He was referred to our Pain Center for right-sided trigeminal neuralgia that was resistant to carbamazepine.
Nine months before this consultation, the patient began experiencing facial pain that gradually worsened over time. He described the pain as a persistent burning sensation punctuated by brief, paroxysmal, electric shock–like episodes lasting only a few seconds with no clinical abnormalities noted during the referring physician's examination. The pain was confined to the right maxillary (V2) and mandibular (V3) territories. These characteristics led to the diagnosis of idiopathic trigeminal neuralgia with concomitant continuous pain (group 13.1.1.3.2 of the International Classification of Headache Disorders, 3rd edition [ICHD-3]). In the time between the patient's initial consultation with the referring physician and their visit to our Pain Center, the clinical examination has changed. It revealed no sensory deficit; however, marked right-sided labiomental allodynia was present for 2 months, with a trigger zone located in the center of the right temporalis muscle that reliably reproduced the electric shock–like pain in the V3 distribution. The pain significantly disrupted his sleep, with frequent nocturnal attacks, and led to an unintended weight loss of 10 kg.
An initial MRI focused on the trigeminal nerve pathway was reported as normal, with no evidence of neurovascular conflict (Figure 1).
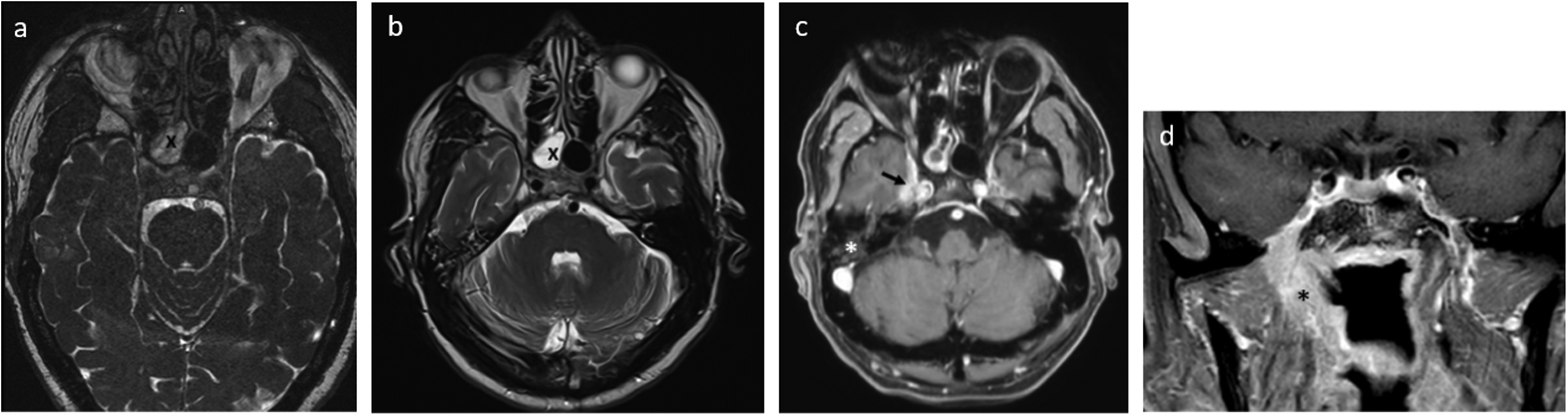
(a–b) First brain magnetic resonance imaging (MRI). Thick slices. (c–d) Follow-up brain MRI with contrast-enhanced sequences along with the course of the right trigeminal nerve. (a) Axial T2 CISS, nasopharyngeal mass with hypointense signal (the mass is indicated by a black cross). (b) Axial T2 TSE, nasopharyngeal mass with hyperintense signal (the mass is indicated by a black cross). (c) Axial T1 gadolinium-enhanced image showing hyperintensity of the nasopharynx and contrast enhancement with encasement of the right maxillary nerve in its cisternal segment (black arrow) and right serous otitis (white asterisk). (d) Coronal T1 gadolinium-enhanced image showing encasement of the right mandibular nerve (black asterisk).
Over time, the patient's pain evolved, becoming continuous and particularly severe at night, while remaining unresponsive to carbamazepine.
Given several atypical features—notably the progressive worsening of continuous pain, the onset of allodynia and the loss of its initial electric shock–like quality—a careful rereview of the imaging was undertaken. This revealed an asymmetry of signal intensity in the nasopharynx, raising suspicion of an underlying expansile process. In light of these findings, a second high-resolution MRI and a facial CT scan were subsequently requested.
In the meantime, several therapeutic options were explored. These included lacosamide and amitriptyline, both of which were poorly tolerated, clonazepam, which proved ineffective, an infraorbital nerve block performed via an intraoral approach without benefit, and pregabalin, which was also ineffective. Among all treatments attempted, only oxycodone, an opioid analgesic, led to a noticeable reduction in pain intensity.
Reassessment with facial MRI (Figure 1) demonstrated soft tissue infiltration of the right nasopharynx extending into the parapharyngeal space, with associated seromucous otitis. Additional findings included osteosclerotic bone infiltration involving the right pterygoid process, the right greater wing of the sphenoid, and the lateral portion of the clivus. There was also widening of the foramen ovale, the pterygoid nerve canal, and the pterygopalatine fissure. Finally, perineural spread was observed along with the right V2, V3, XII, and vidian nerves. Overall, the clinical presentation and imaging findings were concordant with the nerve territories responsible for the patient's symptoms.
A biopsy confirmed the diagnosis of a T4N1Mx squamous cell carcinoma. The staging workup showed possible liver metastases. The patient is currently undergoing immunochemotherapy.
The second case involves an 82-year-old man with a history of left internal carotid artery stenosis, discovered after retinal ischemia, which left him with partial blindness in one eye. He was on aspirin, blood pressure medication, and cholesterol-lowering drugs.
He was referred to our Pain Center for the assessment of persistent trigeminal neuralgia affecting the left maxillary (V2) region. Multiple treatments had failed, including carbamazepine, gabapentin, pregabalin, and tramadol.
His pain started about a year before the consultation and gradually worsened, affecting his left upper lip, cheek, and the side of his nose. At first, the pain was typical of trigeminal neuralgia—brief electric shock–like bursts several times a day, without constant background pain, which led to the diagnosis of idiopathic trigeminal neuralgia, purely paroxysmal (group 13.1.1.3.1 of the ICHD-3). By the time, he was seen at the clinic, the pain had changed. He described it as a continuous burning sensation, with sudden flare-ups lasting 1–2 h. He no longer experienced the electric shock sensations.
On examination, there was no specific trigger zone, but a widespread sensitivity to normally nonpainful stimuli (allodynia) in the painful area, along with reduced sensation throughout the entire maxillary nerve distribution. Changes in pain characteristics led to a revision of the diagnosis to maxillary neuropathy.
The first MRI focusing on the trigeminal nerve was reported as normal, with no sign of neurovascular conflict (Figure 2). However, since the pain had evolved into a neuropathic type—suggesting nerve damage—a second look at the MRI was done. This revealed an asymmetry in the signal near the cavernous sinus. After consulting with radiologists, a mass was identified behind the left maxillary sinus, extending into the pterygopalatine fissure and foramen rotundum, and invading the cavernous sinus. There was also a slight contrast enhancement of the maxillary nerve in that area. A follow-up facial MRI was then requested. In the meantime, the patient found significant pain relief with duloxetine and lacosamide (200 mg daily).
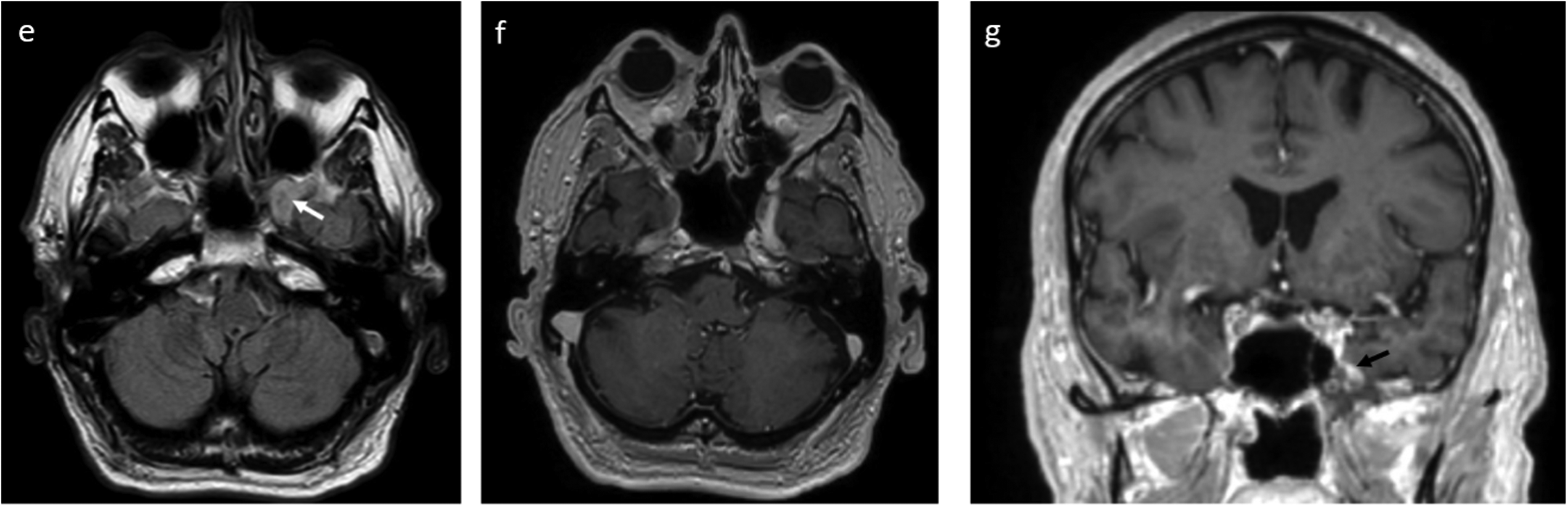
Diagnostic brain magnetic resonance imaging (MRI) with contrast-enhanced sequences focused on the trigeminal nerve. (a) Axial T2 FLAIR image showing a mildly hyperintense mass posterior to the left maxillary sinus (white arrow). (b) Axial T1 gadolinium-enhanced image demonstrating enhancement in the region of the left cavernous sinus. (c) Coronal T1-gadolinium-enhanced image showing enhancement of the cavernous sinus (black arrow), adjacent to the sphenoid sinus.
A follow-up MRI showed an infiltrating lesion at the base of the skull, centered on the left maxillary nerve, with extension into the nearby cavernous sinus. A biopsy of the mass revealed a mucinous adenocarcinoma of intestinal type. Radiotherapy was started; initially, the tumor continued to grow, causing the pain to spread to the ophthalmic nerve territory, but it eventually responded well to treatment.
Five years after diagnosis, the patient remains stable, with residual neuropathic pain well controlled by lacosamide (250 mg daily) and repeated nerve blocks of the supra- and infraorbital nerves.
Discussion
Trigeminal neuralgia is most often caused by a neurovascular conflict, but it's crucial to rule out secondary causes before assuming it's idiopathic. An MRI focusing on the trigeminal nerve pathway is usually done at diagnosis to look for any underlying issues. Most secondary causes involve intracranial lesions such as meningiomas, schwannomas, multiple sclerosis, or brainstem ischemia.
Consequently, clinicians involved in patient care tend to focus on the intracranial segment of the trigeminal nerve, often neglecting a thorough analysis of the extracranial portion of the nerve. An MRI centered on the cerebellopontine angle and intracranial trigeminal nerve pathway may fail to detect ENT lesions (ear, nose, and throat) or perineural tumor invasion.
In the two cases we presented, the initial normal MRI reading delayed the cancer diagnosis, showing how important it is to question the diagnosis if anything seems unusual—especially when there is no sign of neurovascular conflict and when clinical abnormalities arise. For the first patient, resistance to carbamazepine despite proper administration, a persistent burning sensation from the onset of the condition, the occurrence of nocturnal attacks and the progressive onset of an allodynia suggest underlying causes. For the second patient, clinical abnormalities emerged during follow-up as clinical characteristics changed.
Perineural tumor invasion is a recognized pathway of cancer dissemination along with nerves, causing neuropathic pain that can mimic trigeminal neuralgia or involve other cranial nerves like the glossopharyngeal nerve. 3
In summary, these cases highlight how essential it is to regularly revisit the diagnosis, to reconsider it whenever there are atypical clinical signs, and to repeat imaging if needed, so as not to miss a serious underlying condition that requires prompt specialized care.
Clinical implications
The importance of not overlooking the evaluation of the extracranial course of the nerve when investigating secondary causes of trigeminal neuralgia. Persistent or atypical facial pain should prompt repeat imaging and thorough evaluation to rule out underlying oncologic causes.
Footnotes
Consent to participate
Both patients gave their written consent for the writing and publishing of this paper.
Consent for publication
Authors agree to publish with Cephalalgia Reports, if the manuscript is accepted.
Author contributions
Antoine Bender contributed to conceptualization, data curation, formal analysis, investigation, visualization, writing—original draft, and writing—review & editing. Francis Veillon contributed to data curation and formal analysis. Amélie Albisetti contributed to writing—review & editing. Eric Salvat contributed to project administration, validation, and writing—review & editing. Mirela Muresan contributed to conceptualization, project administration, supervision, validation, and writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Université de Strasbourg.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are derived from patient medical records.