
Abstract
Aim
There is a growing recognition of the need for sex-specific approaches in primary headache disorders. Research on sex differences in cluster headache (CH) is quite limited, and examining this data across different populations is crucial for understanding genetic and sociocultural differences. We aimed to investigate sex differences in clinical features, acute treatment responses, and the burden of CH in Türkiye.
Methods
This multicenter cross-sectional study was conducted between January and June 2024 and involved patients with CH from tertiary healthcare centers, who met the International Classification of Headache Disorders (ICHD-3) criteria. Patients with cluster-like secondary headache conditions were not included. Sociodemographic data, clinical characteristics, acute treatment responses, and the burden of CH were assessed using a semi-structured questionnaire. Statistical comparisons were done between male and female patients.
Results
A total of 318 patients (244 males, 76.7%), with a mean age of 45.0 ± 10.9 years, were included. Previous misdiagnosis rates were significantly higher in females (71.6%) compared to males (50.8%) (p = 0.002). While the frequency and duration of cluster bouts were similar in both sexes, compared to males, females were more likely to experience headache attacks lasting longer than 2 h (44.3% vs. 60.8%; p < 0.013) and more frequently experience agitation during the attacks (66% vs. 79.7%; p = 0.025). The presence of autonomic symptoms also varied by sex; males reported higher rates of conjunctival injection (52.5% vs. 35.1%; p = 0.009) and facial sweating (37.3% vs. 17.6%; p = 0.002). Males showed a higher therapeutic benefit from subcutaneous sumatriptan (91.7% vs. 66.7%; p = 0.002). Both sexes reported a negative impact of CH on daily life in the previous year, with a mean of 18.3 days in males and 22.5 days in females.
Conclusion
Several sex differences were observed in patients with CH: attack duration was longer, agitation during the attacks, and misdiagnosis were more frequent. On the other hand, autonomic features such as conjunctival injection and facial sweating tended to accompany CH attacks more often in males, who responded better to subcutaneous triptan than females. These findings highlight the necessity of investigating the underlying mechanisms of sex-specific differences in future research, as well as the careful consideration of these factors in diagnostic and treatment planning.
This is a visual representation of the abstract.
Introduction
Cluster headache (CH) represents one of the most excruciating forms of primary headache disorders, classified under “trigeminal autonomic cephalalgias.” 1 While historically considered a predominantly male disease, recent studies reported that CH is not exclusively male and male predominance has been decreased progressively over decades. 2 This trend has been later confirmed by both Western and Eastern studies.3–7 In males, CH tends to appear in a classic pattern with a higher frequency of episodic CH, while in females, a chronic course is often more common.8–10 A Danish study showed that the peak timing of diurnal variation of attacks also differs between males and females, with a delayed timing of approximately 1 h compared to males. 11 Females may experience more prominent autonomic symptoms compared to males, which can increase the disability. 10 However, the pain intensity, duration, and associated symptoms such as nausea, photophobia, and phonophobia are reported to be equally severe, if not more so, in females from Western populations.8,10,11 Attack duration and associated symptoms showed sex-related differences in several Asian studies,12,13 while clinical features of CH were similar in both sexes in another study from Korea. 14
In recent years, there has been growing recognition of the need for sex-specific approaches to primary headache disorders. So far, related studies have mainly focused on migraine,15,16 and studies from different geographical regions that primarily examined sex-related differences in CH reported heterogeneous results.8,10,14 Evaluation of sex differences may provide new insights into the pathophysiology and individualized management of CH. Detailed assessments evaluating differences across all aspects of this headache disorder, including treatment responses and personal burden, were lacking in the present data. Therefore, we aimed to investigate sex-related differences in clinical features, treatment responses, and burden of CH in Türkiye.
Methods
This cross-sectional multicenter study was conducted between January and June 2024, in accordance with the STROBE statement. All five of the participant centers were headache outpatient clinics of tertiary healthcare centers or private offices of headache specialists. We recruited patients with CH diagnosed by headache specialists according to ICHD-3 criteria, 1 who gave written informed consent. All patients had brain magnetic resonance imaging, and cluster-like secondary headache conditions were not included. Patients who were not willing to participate and with unstable medical or psychiatric diseases that would not allow them to answer the survey, such as being hospitalized at the time, were excluded. Patient recruitment was performed in two steps. First, medical records from the participating centers were reviewed. Second, patients were invited to participate in the study and answer a semi-structured survey administered either through face-to-face interviews during outpatient visits or via phone interviews conducted by the authors. The survey included questions on sociodemographic characteristics, detailed clinical features, responses to acute pharmacological and non-pharmacological therapies, and burden-related information (Supplemental Appendix 1). Treatment responses were also verified, and any missing data were completed by reviewing medical records during interviews.
The sample size depended on data availability without a priori calculation. Subgroups, subject to statistical comparison, consisted of male and female patients with CH.
Statistical analysis
Statistical comparisons were conducted between male and female patients with CH. The Shapiro–Wilk test was used to assess the normality of the data, and all hypothesis tests were two-tailed. Categorical data were analyzed using the chi-square (χ2) test or Fisher's exact test, and the independent samples t-test or Mann–Whitney U test was used for continuous variables, where applicable. For the statistical analysis, we used Statistical Package for the Social Sciences (SPSS) for Windows, version 21.0, and p < 0.05 was considered statistically significant.
Results
A total of 318 patients with a mean age of 45.0 ± 10.9 years were included; 244 (76.7%) were male; 338 patients did not answer phone calls or refused to participate in the study, 14 patients had cluster-like secondary headache, and none of them had an unstable medical condition, not allowing patient recruitment. The mean age at onset of CH was 29.1 ± 11.9 years, and the mean age at diagnosis of CH was 34.7 ± 11.1 years, with an earlier onset in female patients. The time to diagnosis was similar for both sexes. However, a significantly higher rate of previous incorrect diagnoses was observed in female patients, with 53 out of 74 (71.6%) receiving a wrong diagnosis compared to 124 out of 244 males (50.8%) (p < 0.002). The most common misdiagnosis was migraine, recorded in 69.4% of male patients and 71.7% of female patients. Although the duration of cluster bouts and number of daily attacks were similar in both sexes, 45 out of 74 female patients (60.8%) reported attacks lasting 2 h or more, compared to 108 out of 244 males (44.3%), showing statistical significance (p < 0.013).
When autonomic symptom frequencies were analyzed, conjunctival injection was reported by 128 males (52.5%) and 26 females (35.1%), demonstrating a significant difference (p = 0.009). Likewise, forehead and facial sweating occurred in 91 males (37.3%) and 12 females (17.6%), also showing a significant difference (p = 0.002). However, agitation during CH attacks was more frequently reported by females (59 patients, 79.7%) than males (161 patients, 66%), showing a significant difference (p = 0.025). The occurrence of other autonomic symptoms did not differ between males and females.
The majority of the patients reported a negative impact on daily life, with a remarkable absenteeism from work. Comparison of demographic and clinical characteristics, burden of CH between the female and male patients was given in detail in Table 1, and clinical features showing significant sex differences were presented in Figure 1.

Clinical features showing sex differences in cluster headache.
Demographic and clinical characteristics, burden of CH in the female and male patients.

Bold values represent statistical significance (for p values <0.05, which is a generally accepted threshold value for statistical significance).CH: cluster headache; IQR: interquartile range; mo: month; NRS: numeric rating scale; Tx: treatment.
Chi-square or Mann–Whitney U test where appropriate.
Thirty-six (36) females and 161 males used alcohol.
Regarding treatment, more males (100 out of 109 users, 91.7%) reported benefiting from subcutaneous sumatriptan injections for treating attacks compared to females (18 out of 27 users, 66.7%) (p = 0.002). No significant sex-related differences were found in the usefulness of oxygen therapy, oral triptans, ergotamine, non-steroidal anti-inflammatory drugs (NSAIDs), and sphenopalatine ganglion block as abortive therapies. Patients had undergone other procedures to treat the CH attack, but the rates of benefit from these non-pharmacological procedures or managements were also similar in both sexes (Table 2).
Responses to abortive pharmacological and non-pharmacological treatments or procedures.
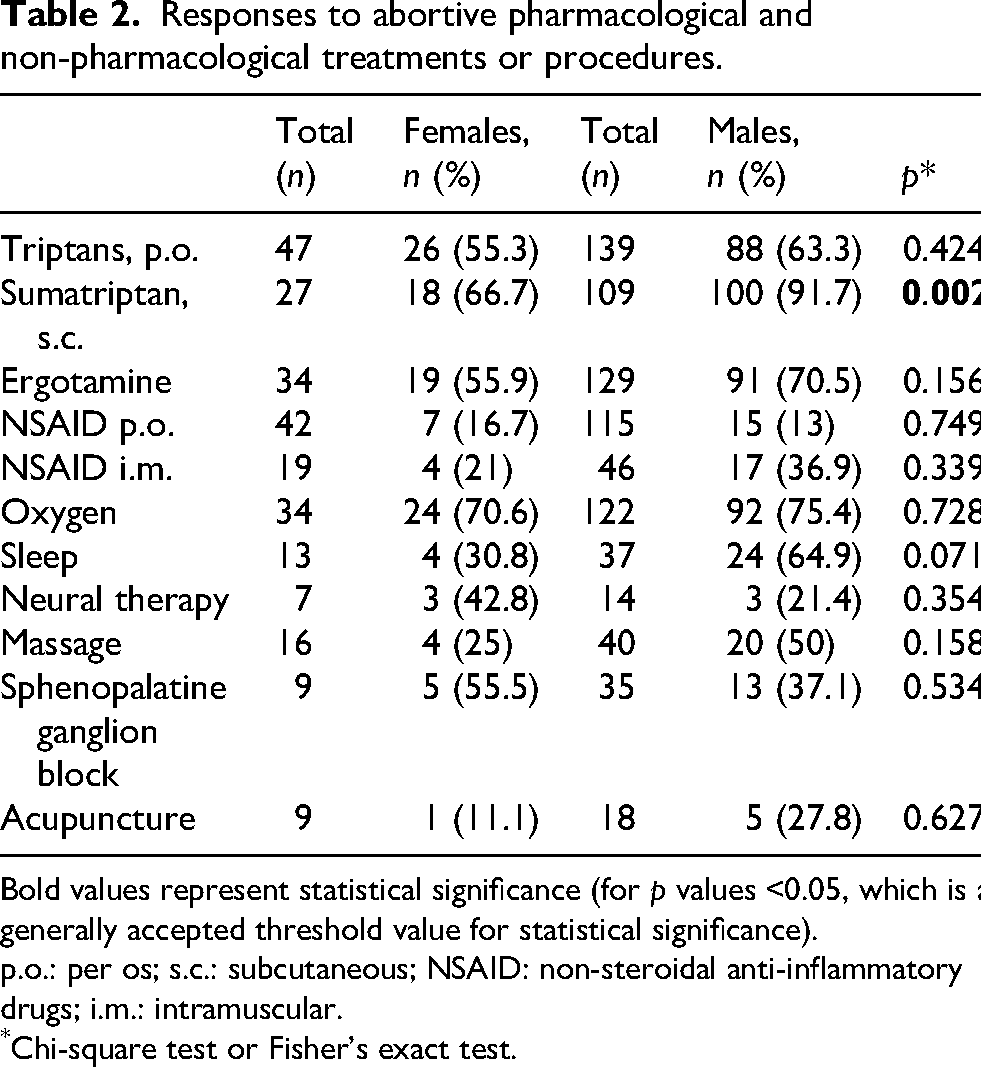
Bold values represent statistical significance (for p values <0.05, which is a generally accepted threshold value for statistical significance).p.o.: per os; s.c.: subcutaneous; NSAID: non-steroidal anti-inflammatory drugs; i.m.: intramuscular.
Chi-square test or Fisher's exact test.
Discussion
This study revealed some sex-related important clinical differences in the clinical profiles, abortive treatment effectiveness, and disability of CH patients. Attack duration was longer, and agitation during attacks was more frequent in female patients. On the other hand, conjunctival injection and facial sweating tended to accompany CH attacks more often in males, who responded significantly better to subcutaneous triptan than females. Other clinical features were similar in both sexes. The onset of CH was significantly earlier in female patients, and misdiagnosis was experienced more often by females compared to males, as expected by the recognition of CH as a male headache disorder. Our results also suggested that the perception of the burden of CH was similar in both sexes.
Diagnostic delay in females is a major concern in CH as reported earlier,11,17 although some of the recent studies have not found an association between female sex and diagnostic delay.18,19 The perception of CH as a males-only disorder was suggested to be the underlying reason for the under-recognition of this condition among females. Nevertheless, the sex ratio decreased over the decades, from 5–7:1 in the 1970s to 2:1 in the 1990s, in the Western population,20,21 while male predominance remained striking in Asia.13,22 In this study, males constituted 76.7% of the participants, reflecting a ratio of 3.3:1. However, this ratio cannot be generalized to reflect the prevalence of the disease, as most centers were tertiary clinics. Most of the females had been misdiagnosed, which was significantly more often than it was for male patients, similar to the results of previous studies.11,23 Several studies showed that females are more likely to develop CH at two different ages, namely during the earlier and older stages of their lives.8,9,14 While females experienced their first CH attack at a younger age than males in several studies8,12,24; consistent with our findings, mean age at onset did not differ between males and females in other previous reports.10,11,14,17,25,26
Several clinical aspects of CH were questioned in this study, and a few of them showed sex differences. More females reported CH attacks lasting longer than 2 h in comparison to male patients. The average duration of attacks was longer than 1 h in previous studies11,12,14,26; two of them12,26 reported longer duration of attacks in females compared to males, in line with our findings. A survey study from the US 8 also reported that females had more attacks per day in comparison to males. However, we found that the number of daily attacks was similar in both sexes. Most of our patients experienced CH bouts lasting longer than one month, with similar rates in both sexes. Duration of cluster bouts did not show sex differences in previous studies.14,17,26 Only one study observed extended bouts lasting 12 weeks or longer significantly more often in females compared to males. 8
The rates of chronic CH also vary across studies.10–12,14,26 We found that chronic CH was more frequent in females compared to males and similar to a study from Denmark 11 reporting that more than one-third of the patients were diagnosed with chronic CH, with a female predominance. It is important to note that these high rates may be related to the referral bias of patients with chronic CH to tertiary headache centers. A very low prevalence of chronic CH has been reported in Asian series12,14 suggesting that population-specific characteristics may also influence the presentation of CH.
Furthermore, several triggering factors have been identified in CH. Alcohol was mostly evaluated in the studies aiming to assess sex-related differences in triggers. While some studies reported that alcohol provokes a CH attack in males more frequently than in females,8,10,11 other studies,18,27 including this one, could not find a significant difference between males and females with CH.
In this study, we also evaluated sex-related differences in the presence of cranial autonomic symptoms and the sense of restlessness or agitation that accompanies headaches. The most frequently observed autonomic symptoms were lacrimation and nasal congestion, which occurred with similar frequencies in both sexes. Conjunctival injection and facial sweating were accompanying CH attacks significantly more often in male patients in comparison to females. Several studies also reported that males were more likely to experience conjunctival injection,11,12,24 lacrimation,8,28 facial and forehead sweating14,24; while nasal congestion, 26 ptosis,10,11,24,26 and eyelid edema11,12,24 were predominant in females. However, in this study, more females reported agitation during attacks compared to males, showing a significant difference, similar to a previous report. 11 Restlessness was also more frequent in females than in males in a recent study. 10 Furthermore, we have evaluated the rates of accompanying migrainous symptoms such as photophobia, nausea, and vomiting. These remained comparable in both sexes, although females experienced them slightly more frequently. Another study from our country also showed no significant sex-related difference in migrainous symptoms that accompanied CH. 28 However, a previous survey study from the US 8 reported that females experienced migrainous symptoms more frequently than males, with a significant difference observed in nausea.
Sex-related differences in responses to abortive and preventive therapies were also previously evaluated, and two large prospective cohort studies could not reveal any difference in treatment responses.12,27 Another study also reported no statistically significant difference between triptan responses of both sexes. 14 However, these two of these studies, one from Taiwan and the other from Korea, could not assess the effectiveness of subcutaneous sumatriptan as this form of triptan was unavailable in either country. In this study, we found that male patients respond significantly better to injectable sumatriptan than females, confirming the findings of a single previous study. 8 Nevertheless, the number of females using subcutaneous sumatriptan was lower than that of male patients, which may act as a confounding factor when interpreting these data. This difference in subcutaneous sumatriptan response may suggest some differences in the pathophysiology and clinical picture of CH attacks in females, potentially involving additional mechanisms. Future studies should carefully focus on acute treatment responses while also considering sex differences, and it may be beneficial to explore the use of gepants and other options in CH. As a limitation, due to the cross-sectional nature of this study and the lack of standardized follow-ups, as well as the significant variability in prophylactic options, combinations, used dosages, durations, and approaches, we did not consider it appropriate to include prophylactic treatments in our sex-related assessment.
Importantly, CH also has a significant impact on quality of life, causing disability and economic and job-related issues, 8 as well as increasing the risk of suicide, as previously highlighted in a review study. 29 Our findings also support the negative impact of CH on working, family, and social life, which were more frequently reported by females in comparison to males, although the differences were not statistically significant. Moreover, the rates of female patients expressing suicidal thoughts were also numerically higher than those of male patients.
Strengths and limitations
While the retrospective nature of our study and certain other limitations, such as recall bias from patients and the reliance on patients' reporting past treatment responses that were not monitored during direct follow-up, are weaknesses. Almost half of the patients either did not answer phone calls or refused to participate in the study. This could also affect the generalizability of the findings, despite our sample size being relatively large. Another limitation of this study was its cross-sectional design, which relied on the availability of data without a prior calculation of the number of participants required from both sexes. However, the strength lies in our large sample size and the involvement of headache specialists. We did not use any specific measures to assess treatment responses. On the other hand, medical records were checked in order to minimize the risk of recall bias.
Furthermore, since conducting the study in headache centers may indicate a problematic patient group that is more difficult to diagnose and treat, the findings may not reflect the general population. Selection bias constitutes a limitation to the generalizability of the study. In every case, a detailed sex comparison from Türkiye is noteworthy due to its geographical location as a bridge, considering the differences in sex-related data from Asia and Europe in patients with CH. Therefore, our study is significant because it is broad and multi-centric.
Conclusion
This study demonstrated several sex-related disparities in patients with CH. The duration of the attacks was significantly longer, and agitation during the attacks was more frequent in female patients than in males. Furthermore, misdiagnosis and absenteeism due to CH were more prevalent in female patients in comparison to male patients. However, autonomic manifestations, such as conjunctival injection and facial sweating, appeared more frequently in males than in females during CH attacks. Female patients, with a modest sample size, exhibited a lower response rate to subcutaneous sumatriptan compared to males. Further studies from different geographical regions are needed to illuminate sex-related associations in CH.
Clinical implications
Several sex differences are present in patients with CH according to the findings of this study.
Attack duration was longer, agitations during the attacks and misdiagnosis were more frequent in female patients compared to males.
Autonomic features such as conjunctival injection and facial sweating tended to accompany CH attacks more often in males.
Male patients responded better to subcutaneous sumatriptan than females.
Further studies from different geographical regions are needed to illuminate sex-related associations in CH, as well as the careful consideration of these factors in diagnostic and treatment planning.
Supplemental Material
sj-docx-1-rep-10.1177_25158163261462937 - Supplemental material for Sex differences in cluster headache, treatment insights, and burden of disease in Türkiye: A multi-center cross-sectional study
Supplemental material, sj-docx-1-rep-10.1177_25158163261462937 for Sex differences in cluster headache, treatment insights, and burden of disease in Türkiye: A multi-center cross-sectional study by Esme Ekizoğlu, Pınar Yalınay Dikmen, Mustafa Ertaş, Edis Hacılar, Elif Ilgaz Aydınlar, Elif Kocasoy Orhan, Ferda Selçuk, Aynur Özge, Ayşenur Şahin, Tuba Erdogan Soyukibar and Betül Baykan in Cephalalgia Reports
Footnotes
Acknowledgements
The authors want to thank the Global Migraine and Pain Society for their support. EH used Gemini and Canva AIs to create different parts of the figure, which were then merged in PowerPoint.
Ethical considerations
The study received approval from the institutional ethics committee of Acıbadem University (2024-2/92).
Consent to participate
The participants provided written informed consent to participate.
Consent for publication
The authors agree to publish with Cephalalgia Reports if the manuscript is accepted.
Author contributions
EE: Design of study, acquisition and interpretation of data, drafting, and revising the manuscript. PYD and ME: Design of study, acquisition and interpretation of data, and revising the manuscript. EH: Acquisition and interpretation of data. EIA: Design of study, acquisition of data, and revision of the manuscript. EKO, FS, AÖ, AŞ, and TES: Acquisition of data and revising the manuscript. BB: Design of study, acquisition and interpretation of data, drafting, and revising the manuscript. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: EE has served as a lecturer for Pfizer and Neutec for the last 5 years. PYD, ME, EH, EIA, EKO, FS, AŞ, TES, and BB have no conflicts of interest. AÖ: has served as a lecturer for AbbVie, Lilly, Abdi İbrahim, Neutec, İlko, Ali Raif, and Orzax for the last 5 years. She is currently the president of the Global Migraine and Pain Society and a Board Member of IHS since 2019.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.