
Abstract

A patient is severely injured by a medical error while you are on call. You feel responsible and experience shame, guilt, anger and numbness. You begin to second-guess your clinical skills, knowledge base, and even your ability to be a physician. You withdraw from your colleagues and your mood sinks, and the care of your current patients suffers. A month later, you do not feel much better, and you feel worse when you see a patient who reminds you of the one who was injured. You may ultimately choose to leave medicine.
This situation exemplifies the second victim phenomenon, the suffering of the caregiver in the face of a patient adverse event. 1 This experience, which may affect up to half of all healthcare workers during their careers and lead to depression, anxiety, post-traumatic stress disorder (PTSD), or in the worst cases, suicide, is intimately tied to healthcare’s epidemic of provider burnout. Burnout, a syndrome of emotional exhaustion, depersonalization, loss of meaning in one’s work, and feelings of ineffectiveness, is associated with high physician, nurse, and staff turnover and decreased quality of care. 2 Rates of burnout are disturbingly high and increasing: in 2011, 45.5% of physicians met criteria for burnout, and by 2014, this number had climbed to 54.4%. 2 This is not just a phenomenon of physicians: 34% of hospital nurses and 37% of nursing home nurses met criteria for burnout in 2014. 3
The healthcare community has begun to acknowledge this problem. Bodenheimer et al. proposed expanding healthcare’s Triple Aim – enhancing patient experience, improving population health, reducing costs – to a Quadruple Aim by adding the goal of improving the work life of doctors, nurses, and other healthcare providers. 3 Hospitals are taking steps in this direction by implementing workflow process changes, encouraging healthy behaviors, and offering psychological support to all healthcare workers who reach out to hospital-based programs. But the last phrase includes an important caveat: providers who reach out. The proportion is small.
At the Johns Hopkins Hospital, the Resilience in Stressful Events (RISE) program 4 was created in 2011 to help healthcare workers deal with the psychological effects of stressful patient-related events. However, use of this otherwise helpful program has been modest – only about eight calls per month. When compared to the number of patients harmed by healthcare, estimated to be approximately ten percent of hospitalized patients, this number seems very small. Other hospitals have developed similar programs – the University of Missouri Health Care’s forYou program is a prime example – and these programs report tangible benefits. But this is not enough: we should be able help all wounded providers and eliminate barriers to the seamless provision of psychological support.
Psychological first aid (PFA) may be the answer. Originally developed in the 1950s and used primarily in developing countries after crisis events, PFA is easily adapted and applied to hospital settings. The World Health Organization (WHO)’s 2011 Guide for Field Workers describes it as “humane, supportive, and practical help to support fellow human beings [immediately after] suffering serious crisis events”. 5 It is an evidence-informed approach with the goal of promoting an environment with five essential elements – (1) safety, (2) self- and community-efficacy, (3) calming, (4) connectedness, and (5) hope – all of which have received empirical support as restoring social and behavioral functioning. 6
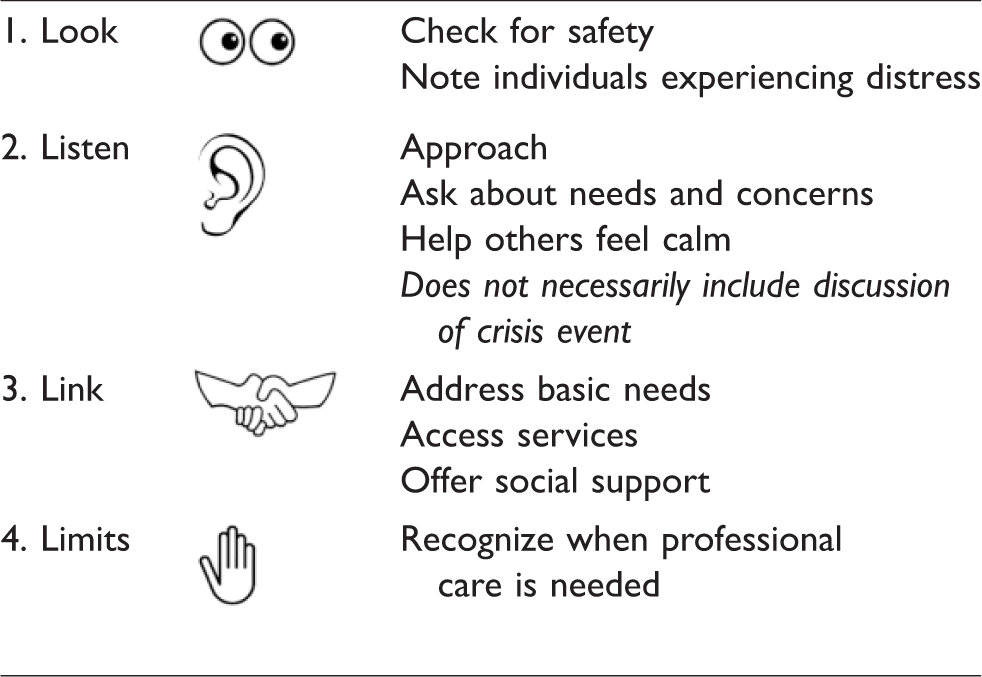
The WHO’s core action principles of PFA are simple: (1) look – check for safety and note individuals experiencing distress reactions, (2) listen – approach those individuals, ask about needs and concerns, and help them feel calm (unlike psychological debriefing, this does not necessarily include discussion of the crisis event) (3) link – address basic needs, access services, offer social support, and (4) know PFA’s limits and recognize when professional care is needed 5 (see Table 1). This last point is notable: PFA is not a replacement for professional care. Everly et al. wrote in a 2014 article about PFA training at the Johns Hopkins Bloomberg School of Public Health, “PFA is to the practice of psychotherapy as physical first aid is to the practice of medicine”. 7
The core action principles of psychological first aid.
PFA is supported by disaster mental health experts as an “acute intervention of choice”, 8 and despite our title comparing PFA to CPR (which we make to indicate that all healthcare workers can, and should, be trained), we conceptualize it as more similar to a rapid response, necessary to prevent more severe downstream effects of an acute decompensation. There has been rapid uptake of the methodology due to the proven efficacy of its components, although the overall model awaits a definitive trial. In 1991, the International Federation of the Red Cross and Red Crescent Societies selected PFA as the best form of psychological support for developing countries. In 2004, the American Red Cross (ARC) endorsed PFA and now requires PFA training for all of its disaster relief workers. Remarkably, at least 50% of all ARC volunteers have received training. The published WHO guidelines for providing PFA during Ebola outbreaks recommend that it be used in preference to both psychological debriefing, and multiple-session psychological interventions for stress-related incidents. The National Center for Post-Traumatic Stress Disorder and National Child Traumatic Stress Network also promote its use and have created a free PFA app for mobile devices. 9
We believe that training healthcare workers in PFA would be a simple, efficient, and cost-effective approach to help address healthcare’s burden of second victims and burnout. PFA is readily adapted for use in the hospital, and we suggest using it as an on-the-floor adjunct to ongoing staff assistance programs and professional counseling. Use in ambulatory settings where there are fewer supporting resources may be even more beneficial. Our vision is for PFA to be the CPR/rapid response for mental health crises, so that all healthcare workers have the tools to address their colleagues’ basic needs for emotional support. However, it is important to note that PFA is meant for acute events that contribute to the development of burnout; addressing burnout more broadly will require comprehensive systemic change to hospital culture, work/life balance in practice and in training, administrative and documentation burden, and financial pressures on providers among other things.
PFA trainings lasting 4 to 6 hours have been shown to increase knowledge of PFA delivery, self-efficacy in using PFA, and confidence in resiliency. 7 We suggest that medical schools, nursing schools, and residency programs implement PFA training in their core curricula and that clinical leaders support its application on the wards and clinics with both colleagues and patients. Similar to CPR trainings, anyone in trained in PFA can lead classes so long as they have support from the institution and clinical leaders (who could introduce or publicize the classes). Trainings are publically available throughout the country, and we suggest that a few individuals at each institution attend a formal training and spearhead the development of institution-specific trainings. This could, for example, be a residency quality improvement project or a project within the institution’s staff assistance or quality improvement departments. Given PFA’s status as an evidence informed but not yet evidence-based intervention, it is important that early adopters monitor its effectiveness and adjust training, resources, and best practices accordingly. Evaluation should include numbers of calls and rates of PFA use, changes in scales to measure psychological well-being, burnout, provider comfort discussing psychological needs, utilization of mental health services, and rates of provider turnover and student drop-out. Some of these metrics could be incorporated into rotation evaluations completed by trainees.
As doctors, nurses, and other healthcare professionals, we are accustomed to helping our patients, but we are less accustomed to helping each other. Approaching distressed colleagues must become the norm rather than the exception; broad training in PFA will facilitate this by encouraging awareness of colleagues’ emotions and reducing barriers to getting help. On-the-ground PFA coupled with existing staff assistance programs, professional counseling, and workflow process changes will bring us closer to achieving Bodenheimer’s fourth aim – improving the work life of healthcare professionals, thereby decreasing burnout and perhaps even beginning to address the specter of physician suicide.
Reimagine the first scenario.
A medical error occurs while you’re on call. Your patient is severely injured. You feel responsible, second-guessing your clinical skills, knowledge base, and suitability to be a physician. Your PFA-trained colleague notices your withdrawal and approaches you, offering his support. You may confide in him or you may not, but either way, he puts you in contact with your hospital’s assistance services immediately. You’re less likely to develop depression, anxiety, or PTSD, and you’re able to rebuild your confidence and return to patient care.
Psychological first aid isn’t magic. It won’t stop the burnout epidemic on its own, but it will give us tools and training to nudge each other towards seeking help when we need it.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.