
Abstract
Background
While research has established the negative impact of medical errors or adverse events on healthcare providers, few organizations have evaluated support programs for second victims. Thus, we examined satisfaction with a peer support program to provide lessons learned from early implementation.
Methods
Participants (N = 466) were recruited from seven neonatal intensive care units affiliated with a large, pediatric hospital. Following implementation of a peer support program, a mixed-method online survey assessed program satisfaction at 12 month follow-up (n = 250, 54%).
Results
Most participants were female (n = 243, 97%), white (n = 239, 96%), and nurses (n = 180, 72%), with an average age of 40.80 (SD = 11.89) years. Ninety-three (37%) participants observed or were directly involved in an error or adverse event during the preceding six months. Thirty-six (14%) received support from someone within the neonatal intensive care unit, and 16 (16%) had spoken with a peer supporter after the event. All users reported benefit from the interaction. However, most participants were unaware of the program or had not utilized it.
Conclusion
Findings suggested that peer support programs are likely to be viewed favorably by second victims. Healthcare providers who accessed the program felt it was a valuable resource and helped them return to work effectively after an error or adverse event. Better communication is needed during early implementation of any peer support program to increase awareness and use of this resource among healthcare providers.
Introduction
Despite organizational efforts to improve patient safety, medical errors are inevitable in today’s complex healthcare environment. 1 These errors may be due to faulty systems, processes, or conditions, and can range from near misses to errors that result in devastating patient injuries or death. 2 Regardless of the cause and scope of the error, there is increasing recognition that healthcare providers who are involved in such events can become second victims and experience a range of adverse effects. For example, second victims have reported sleep disturbances, anxiety, depression, or even suicidal ideation.3–5 They may also experience significant guilt and decreased professional confidence, which may lead to absenteeism and turnover. 6
The prevalence of second victims among healthcare professionals has been reported to range from 10.4% to 43.3%.6–11 This is concerning because healthcare providers who are distressed are at an increased risk of making additional errors, which can be costly for organizations and negatively affect patient care.6–13 Turnover can result in significant costs for organizations due to hiring and training needs, as well as decreased productivity. 14 Considering that insufficient support has been linked to higher distress and turnover intentions in second victims, it is important that support resources are accessible to healthcare providers following a medical error.6,8,15–17
While many types of support may be valuable, research suggests that second victims prefer to receive support from peers when coping with a traumatic experience.6,18–21 In addition to providing emotional support, peer support programs can benefit all employees by creating a positive shift in workplace culture over time. 22 Prior studies have shown that most healthcare providers feel second victim support programs are beneficial.8,23However, additional research with a variety of professions is needed to fully capture healthcare provider outcomes and satisfaction with peer support programs.
Although errors can occur in any hospital unit, healthcare providers in the neonatal intensive care unit (NICU) may be especially sensitive to the second victim phenomenon given the fragile patient population. 24 Thus, utilizing a mixed-method approach, our aim was to assess healthcare provider satisfaction with a second victim program during early implementation in local NICUs affiliated with a large pediatric hospital.24,25 We hypothesized that the peer support program would be perceived as beneficial for second victims, and findings would also inform the implementation and evaluation of similar programs. As peer support programs grow nationally, lessons learned from early adopters can optimize efforts to quantify the impact of these programs on second victims and healthcare organizations alike.
Methods
Procedure and participants
Data are from a longitudinal survey administered as part of an ongoing, quality improvement initiative to evaluate the impact of a peer support program for second victims.8,24,25 As a quality improvement initiative, which involved anonymous surveys and posed minimal risk to participants, the Institutional Review Board determined this project was exempt from review. Participants were recruited from seven NICUs affiliated with a large, quaternary-care, pediatric hospital during the first 12 months of second victim program implementation. Six of the NICUs are physically located within community birthing hospitals and one is located on the main campus of the pediatric institution. The program was initially launched in several other units within the institution and refined for two years prior to conducting the current evaluation study in the NICUs. All employees working in the NICU were eligible for recruitment, regardless of their profession or employment status (i.e. full-time or part-time). An initial survey was created and disseminated online in July 2015 to 1115 healthcare providers using Research Electronic Data Capture (REDCap). 26 Nurses, physicians, nurse practitioners, respiratory therapist, pharmacists, patient care assistants, lactation consultants, dieticians, and therapists were all invited to participate in the study. Non-clinical staff, such as unit clerks and unit managers, were also included.
During the next year, the NICU sites then implemented a peer support program comprised of a multidisciplinary team of healthcare providers and modeled from a similar program at the University of Missouri Health Care System (MU Health Care). 6 First, all healthcare providers learned to identify and provide initial support to second victims. Then, a select group of volunteers and healthcare providers, who were recommended by NICU managers, received more comprehensive peer support training.
The 466 healthcare providers who participated in the initial survey were invited to complete a 12-month follow-up survey on REDCap in July 2016. 26 To encourage participation, managers from each of the seven NICU sites emailed their units prior to survey dissemination, survey reminders were sent to non-completers via REDCap, and incentives were offered to the highest participating units (e.g. pizza party, gift card raffle). The portal to complete surveys remained open for 6–8 weeks. This manuscript focuses on cross-sectional data from the 12 month follow-up. Only participants who responded to at least one quantitative or qualitative item regarding program satisfaction were included in this study.
Measures
Demographic and quantitative satisfaction data
Participants provided demographic information and rated their involvement and satisfaction with the program. Participants responded “yes” or “no” regarding whether they had experienced an error or adverse event during the past six months, whether they received support from anyone within the NICU or a peer supporter after the event, and whether they had referred a coworker to the program. Participants who experienced an event and spoke with a peer supporter rated how much they benefitted from this interaction on a scale from 1 (not at all) to 4 (a lot) and reported whether they required additional support outside of the department. The same scale was used to rate how much the NICU benefitted overall from the program.
Qualitative satisfaction data
Two open-ended questions assessed participant satisfaction with the program. Participants voluntarily provided written responses, with no maximum word count. The questions were: (Q1) “How did the program support you in returning to work after a traumatic event or experience?” (Q2) “Please provide any other feedback or recommendations for improving the program.”
Data analyses
Analyses were conducted using SPSS Version 24. 27 Descriptive statistics and frequencies are provided for primary variables of interest regarding participant involvement and satisfaction with the program. Independent samples t-tests (two-tailed; α = .05) compared program satisfaction for participants who did and did not experience an error or adverse event during the past six months. Effect sizes are presented for significant dichotomous (Cramer’s V) and continuous (Cohen’s d) outcomes.
Thematic content analysis of the qualitative data produced themes regarding participant satisfaction with the program and recommendations for improvement. 28 Three team members (CAG, AMW, JMM) independently read participant responses to the first open-ended question to get a sense of the data. Next, they clustered responses that portrayed similar themes and began generating codes. The team discussed the rationale for each theme, reviewed direct quotes, and revised codes/themes until they reached both consensus and saturation (i.e. until no new themes emerged). Exemplary quotes were extracted to represent each theme. This process was repeated for the second question. Findings for each question are in narrative form, including major themes and quotes from participants.
Results
Participant demographics
The overall response rate for the baseline survey was 466/1115 (42%). Only participants who completed the baseline survey (i.e. 466 individuals) received the 12-month follow-up survey, which assessed satisfaction with the second victim program. Of those 466 healthcare providers who received the follow-up survey, 250 completed at least one satisfaction measure (overall response rate was 250/1115, which is 22.4%). For the current analyses, the response rate was 250/466, which is 54%.
Most participants were female (n = 243, 97%) and white (n = 239, 96%), with an average age of 40.80 (SD = 11.89) years. The majority were registered nurses or licensed practical nurses (n = 180, 72%; Table 1). Healthcare providers who completed the follow-up survey did not significantly differ in sex, race, or years worked in the NICU from those who did not. However, participants were significantly older (M = 40.80, SD = 11.89) than nonparticipants (M = 37.72, SD = 11.74); t=–2.80, p=.005, d = 0.26.
Quantitative results
Fifty-nine (23.6%) of the 250 participants observed an unanticipated adverse patient event, medical error, patient-related injury, or near miss event during the preceding six months, and 34 (13.6%) were directly involved in one. The 93 (37%) participants who had experienced an event (i.e. observed or involved) did not significantly differ in terms of age, race, sex, or years in the NICU compared to those who had not (Table 2). However, participants who worked full-time (vs. part-time) were more likely to have experienced an event χ2 (1, n = 250) = 9.11, p = .003, V = 0.19.
Professions of healthcare providers in the NICU.
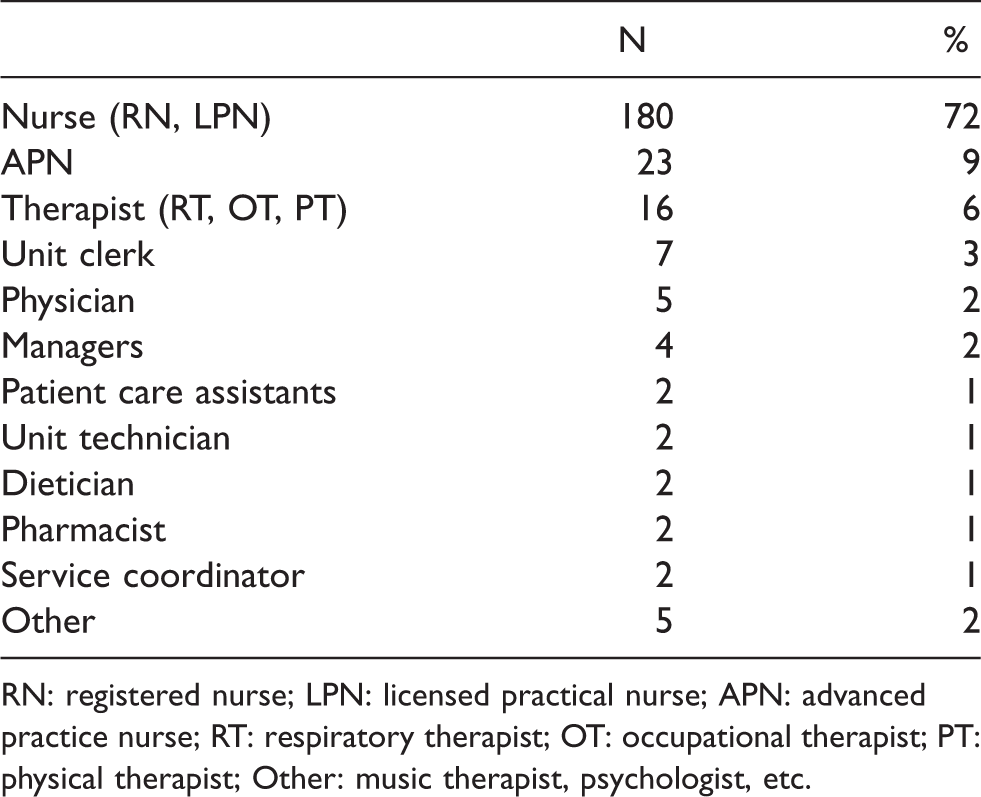
RN: registered nurse; LPN: licensed practical nurse; APN: advanced practice nurse; RT: respiratory therapist; OT: occupational therapist; PT: physical therapist; Other: music therapist, psychologist, etc.
Comparison of demographic characteristics of healthcare providers who did and did not experience an error or adverse event in the NICU.
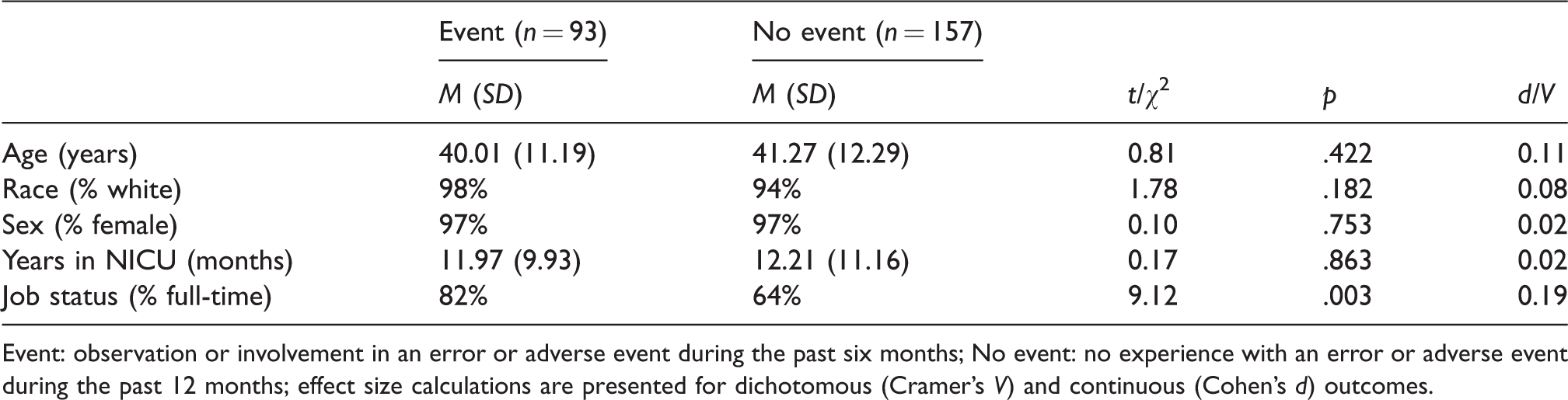
Event: observation or involvement in an error or adverse event during the past six months; No event: no experience with an error or adverse event during the past 12 months; effect size calculations are presented for dichotomous (Cramer’s V) and continuous (Cohen’s d) outcomes.
Of the 93 participants who had experienced an event during the preceding six months, 36 (38.7%) received support from someone within the NICU and 16 (17.2%) had spoken with a peer supporter after the event. Each reported benefit from this interaction, with two (12.5%) reporting a little benefit, nine (56.3%) reporting moderate benefit, and five (31.3%) reporting that they benefitted a lot. Only one person (6.3%) required additional support from outside the department (i.e. referral to pastoral care, employee assistance program, social work, behavioral health). Additionally, 20 (8.0%) of the 250 participants had referred a coworker to a peer supporter. A majority of participants (n = 183, 73.2%) indicated that the NICU benefitted at least a little from the second victim peer support program (Figure 1). Program satisfaction between participants who had experienced an error or adverse event (i.e. observed or involved; M = 2.22, SD = 0.95) and those who had not (M = 2.01, SD = 0.79) was similar, t = –1.72, p = .09.
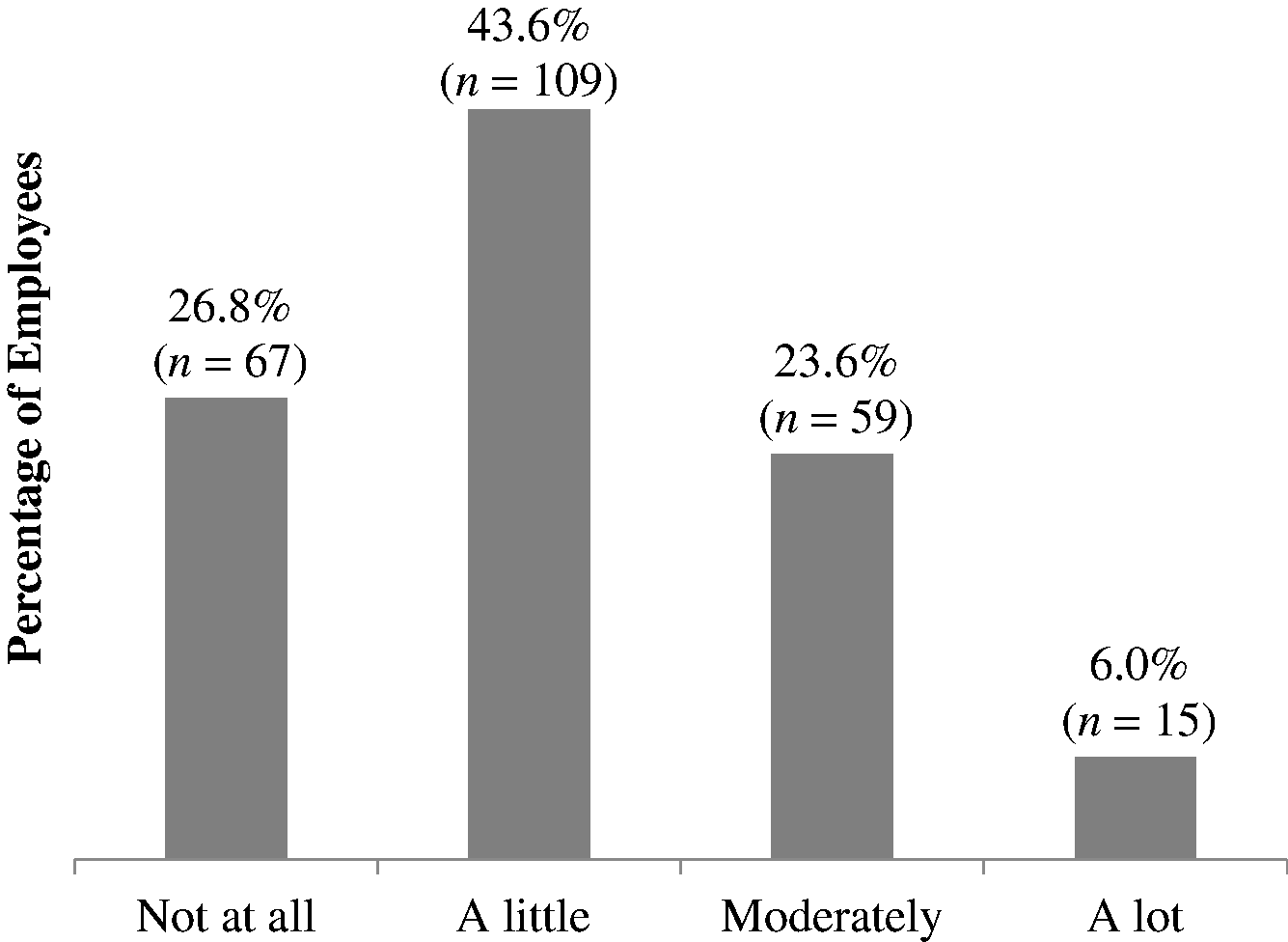
Healthcare provider report of how much the NICU has benefitted from implementation of a second victim program to support second victims (n = 250).
Q1 – Qualitative themes: Program support in returning to work
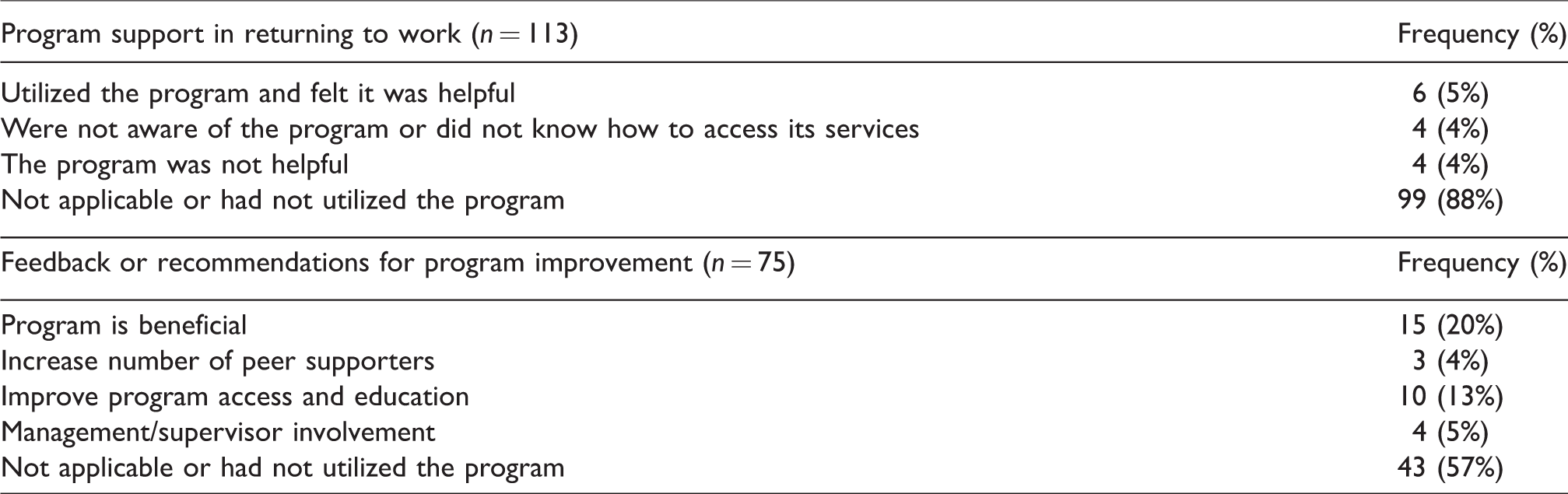
One hundred and thirteen participants described their experience with the second victim program in response to Q1. Although some participants reported that the program helped them return to the NICU following an error or adverse event, many others had not yet utilized the program or did not find it accessible. Outlined below are the four themes that emerged, and Table 3 lists frequencies for each theme.
Common qualitative themes identified regarding program support (Q1) and feedback or recommendations for program improvement (Q2).
Utilized the program and felt it was helpful
A small number of healthcare providers (n = 6) used the program and found it was a helpful resource. One provider reported that the program served as a way to access outside services, whereas others indicated that simply having the program in place gave them peace of mind. Managers reported that the program improved their ability to lead their team effectively. It helped as it led me to further counseling. Helped me feel that I was not alone in my concerns. Supported the team that reports to me, re-enforces trust in (hospital) and me as a leader.
Not aware of the program or did not know how to access services
During the few months following program implementation, some healthcare providers (n = 4) were unaware of its existence or did not know how to access services. …I have heard about it through these surveys, and I am aware it exists, however, I am not sure that we (staff members) have the tools easily accessible to access it if needed.
Program was not helpful
A few employees reported the program was not useful (n = 4). Two did not specify why. The other two explained that the program had not altered the workplace culture and that they were often required to return to work immediately after difficult situations. Witnessing day after day the death of infants and not even having time to take off or being able to attend a funeral is not helpful and created nurse burnout.
Not applicable or did not utilize the program
Of identified themes, the largest number of responders (n = 99) reported that the question was “not applicable” or that they had not used the program. These participants had likely not experienced a traumatic event since program implementation, and thus had no need to access the program.
Q2 – Qualitative themes: Recommendations for program improvement
A total of 75 participants responded to Q2 regarding recommendations for improvement. Some simply reported that the program was beneficial and supported them after a traumatic experience, while others provided specific suggestions for improvement. Outlined below are the themes for Q2, and Table 3 lists frequencies for each theme.
Program is already beneficial
Some participants (n = 15) felt that the program was already beneficial and did not offer advice for improvement. A few participants (n = 4) noted that the program was beneficial after experiencing an error or adverse event, whereas others (n = 3) reported benefitting from just knowing the program was available should they need it. My co-worker recently spoke to someone with the second victim team and said it was very helpful. If I were involved in a serious event, I would appreciate the help from this program. Something that no one ever wants to need, but I think it is great that a program has been put in place.
Increase number of peer supporters
Although peer supporters from various units, departments, disciplines, and shifts were trained, a few participants (n = 3) reported a need for more trained peer supporters, especially in the off-site NICUs. We need to have more people as peer supporters. Need to get more off-site employees to be peer supporters.
Improve program access and education
Although marketing efforts for the second victim peer support program were initiated in 2013, participants (n = 10) felt that the program would benefit from increased advertisement. They reported a need for more information among frontline staff. Make it more widely publicized with examples of how the program can help. I do not believe that I have received any information about this program.
Increase management/supervisor involvement
Another theme was the importance of manager buy-in. A few participants (n = 4) felt that supervisors should activate the program when an event occurs as frontline staff are often too preoccupied. It’s great to have this program available. I think continually reminding people of your presence is important because it’s probably not at the top of our minds after an adverse event. Managers should also remind staff frequently of the availability. After events, the management team should reach out to associates, initiate the process.
Not applicable or had not utilized the program
The remaining survey participants (n = 43) reported that they had not utilized the program or “not applicable.” Again, it is likely that many providers had not yet experienced an error or adverse event that required peer support. Haven’t had to utilize this service, but would if I needed to.
Discussion
After a medical error or adverse event, healthcare providers (or second victims) often report experiencing significant distress (e.g. anxiety, depression, burnout) and a desire for coworker support.6,11,19–21,23,25,29 This mixed-method study is one of the first to assess utilization and satisfaction with a program to support second victims.6–8,23,30 As these programs grow nationally, it is important to share lessons learned from early adopters and recommendations to optimize impact. Some participants (n = 34) revealed that they had been directly involved in an error or adverse event, yet only 6% utilized the program. This low access rate may be reflective of hesitancy to participate in a new program or because peer support had not yet been ingrained in the unit culture. Despite the level of engagement, early adopters did report satisfaction with the support received, and 8% of survey participants had referred peers to the program. Further, there were no differences in program satisfaction between those who did and did not experience an error or adverse event, suggesting that healthcare providers perceived some benefit merely from program existence regardless of their personal need for services. These findings provide additional support for the utility of peer support programs. Although survey data revealed that most early adopters felt that the NICU benefitted at least a little from the program, qualitative themes indicated areas for improvement.
Consistent with our hypothesis and previous quantitative research,6,8,20,21,23,25 early adopters cited that the peer support program was valuable. Specifically, healthcare providers noted that the program helped them return to work after an event, enabled them to be a more effective leader, and served as a liaison for additional resources and support (e.g. formal counseling). Although our study and past research suggests that peer support is desired and potentially useful for helping healthcare providers cope with adverse events, few organizations have established a formal support program and reported evidence of its impact.6–8,23,30 As programs grow nationally, our findings provide early evidence of the perceived benefits of a second victim peer support program and suggestions for developing and implementing these programs effectively.
Despite general satisfaction with the program, qualitative data revealed several key themes regarding areas for improvement. For example, given the interim analysis and relatively brief period between program implementation and the satisfaction survey, nearly two-thirds of participants had not experienced an event requiring utilization of the program. Given the low incidence of such problems, additional research is needed to examine the impact of the program over a longer period of time. Importantly, most participants reported that they were unaware of the program’s existence or were unsure how to access the program. These findings suggest that ongoing communication or active outreach from the second victim team is critically needed. Healthcare providers recommended distributing additional educational materials to improve program awareness for frontline staff. Participants also reported a need for more peer supporters as well as improving manager buy-in and support of the program. Training sessions for managers or web-based materials may be helpful. Examining interim effectiveness and reach of second victim programs is essential during early implementation to ensure that healthcare providers have adequate access. Notably, culture change may also take time following implementation as work environments may have different histories of being punitive or supportive to providers involved in errors. In order to promote the efficacy of these programs, institutions must ensure that second victims feel safe and not stigmatized when accessing resources.
While our findings are an important first step in evaluating satisfaction with a peer support program, there are several limitations. First, to maintain anonymity, participants self-reported whether they had experienced an adverse event. Data regarding the type of event (e.g. medication error, death) and severity were not obtained. Future studies should delineate the characteristics of adverse events to determine subtypes that might contribute to variability in outcomes or use of services. Standardized measures (i.e. anxiety, depression, burnout) to identify specific benefits of second victim peer support programs and objective data regarding turnover and absenteeism are also recommended. 28 Given the brevity of many participants’ responses to open-ended survey questions, qualitative interviews may elicit more detailed information. Response bias should also be considered due to survey response rates. Most participants were nurses despite efforts to include physicians and ancillary staff (i.e. therapists, dieticians, etc.). This is not surprising given that nurses comprise a substantial portion of hospital staff. However, future research should incorporate a wider variety of healthcare providers as their experiences with medical errors and adverse events are likely distinct. Furthermore, longitudinal research is needed to temporally characterize the impact of errors or adverse events on healthcare providers and to determine whether the effects of a peer support program endure. As part of the current project, we plan to continue following healthcare providers to determine if these efforts improve long-term satisfaction and outcomes.
Conclusion
While program evaluations are inherently challenging for such low incidence occurrences, opportunities for improvement were identified and implemented early. Findings suggest that second victim peer support programs are likely to be viewed favorably and can provide much needed assistance to healthcare providers after traumatic events. However, given that most healthcare providers had not yet utilized the program, additional work is needed to ensure that programs are both accessible and effective across organizations.
Footnotes
Acknowledgement
Portions of this research have been presented at the National Patient Safety Foundation 2017 Annual Meeting.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by intramural funding from the Nationwide Children’s Hospital.