
Abstract
Introduction
communication errors between medical personnel are known to be a leading source of adverse events (AEs). The implementation of teamwork training together with the use of a standardized handoff bundle has previously shown to reduce the number of AEs. However, the applicability of this program in spanish-speaker countries remains unclear.
Objective
to assess whether the exploratory implementation of I-PASS bundle in an Argentine pediatric hospital is associated with a reduction in the rate of AEs.
Methods
Design: an exploratory, uncontrolled, pre-post study.
Population and sample: medical records (MR), medical prescriptions, and physician reports were reviewed in two clinical wards of the "Hospital General de Niños Pedro de Elizalde".
Intervention: I-PASS Spanish version, an standardized handoff bundle consists in: a mnemonics, an introductory workshop, a written handoff tool, simulation sessions, and structured observations with feedback.
Results
we reviewed 264 MR. Preventable AEs decreased by 62.8% between pre-intervention and post-intervention period (12.1 vs 4.5 AEs/100 admissions; IC95: 0.010; 0.142; [p = 0.025]). Adherence to the use of quality handoff key elements increased significantly, from 25% to 61% in post-intervention period (p = 0.0001). Handoff duration did not change significantly (5.5 ± 0.2 vs 5.3 ± 0.3 minutes per patient [p = 0.59]).
Conclusion
Implementation of an I-PASS Spanish version was associated with a significant reduction in the rate of AEs and with improvements in handoff quality; without changes in duration.
Introduction
Patient safety is an important healthcare quality domain and its assurance represents a priority for health care systems. In clinical care settings, effectiveness of communication is essential and should be considered as an interactive process. 1 Communication problems have long been noted as a major contributing factor to sentinel events.2,3
Perhaps the most relevant moment for inter-professional communication in daily clinical practice interactions is the handoff of patient care between providers. Handoffs refers to the process of transferring role and responsibility for providing care from one person to another, thus insuring continuity of care. 4 Patients can experience transitions in their care up to 15 times during a five-day period of hospitalization, and physicians may participate in as much as 3,000 individual patient’s handoffs per month. 5 Residents and fellows involved in patient care have reported that one of the main potential causes of adverse events (AEs) are issues related to handoffs. 6
Furthermore, several studies have shown that an effective and standardized communication between caregivers at the moment of handoff is fundamental for patient safety since it anticipates and limits possible errors.4,7–12 The Joint Commission has recently established standardized transmission of information as a patient safety goal. Consequently, it advocates organizations to implement “a standardized approach to handoff communications, including an opportunity to ask and respond to questions”. 13
The implementation of a teamwork training (TeamSTEPPS) together with a structured handoff tool known as I-PASS, has previously shown to decrease the number of medical errors and AEs.14–17 I-PASS was developed in tertiary academic medical centers in the United States and has only been studied so far in that setting. Therefore, its effectiveness in locations that speak different languages, have different availability of resources (e.g. lack of electronic medical records), belong to low and middle-income countries, and are immersed in a different safety culture, remains unclear.
Therefore, our study is intended to evaluate the impact of an intervention to improve communication by implementing handoff standardization among pediatric residents. Since an adequate communication between medical professionals is one of the pillars to consider for improving healthcare quality.
Our objective is to assess whether the implementation of the I-PASS Handoff bundle in an argentine pediatric hospital is associated with a reduction in the rate of AEs and to evaluate its impact on time consumption during handoffs and incidence of medical prescriptions errors (MPE).
Methods
Study design
We conducted an exploratory, uncontrolled, pre-post study; between July 2017 and January 2018, in two wards of Pedro de Elizalde Children's General Hospital (HGNPE) in Buenos Aires, Argentina. Wards were composed of 44 clinical and surgical pediatric hospital beds. At baseline, none of the two wards had a standardized handoff program
The investigators obtained written consent from the subjects who participated and contributed to the study data.
Population
First to third year pediatric internal medicine residents during their terms of provision of care to patients in the selected wards.
Intervention
The I-PASS bundle consists in: an oral mnemonic, an introductory workshop, a teamwork training based in TeamSTEPPS, a printed handoff document, simulation exercises, faculty development, structured observation and feedback, and an I-PASS campaign.
The I-PASS oral mnemonic stands for: I) Illness severity, P) Patient summary, A) Action list, S) Situation awareness and contingency plans, S) Synthesis by the receiver.
TeamSTEPPS is a systematic approach, developed by the Department of Defense (DoD) and the Agency for Healthcare Research and Quality (AHRQ), that aims to integrate teamwork to practice. It is designed to improve the quality, safety, and the efficiency of health care, based in four didactic-based modules: 1) Leadership, 2) Situation monitoring, 3) Mutual support, 4) Communication. 18 The introductory workshop included teamwork training based on leadership and communication modules, which includes 5 key elements: shared mental model, brief, debrief, check-back, and cross monitoring. More than 80% of the residents of each ward attended an introductory workshop for one and a half hour, while the remaining residents received a computer based training with the introductory workshop contents.
Structured observations were done without feedback in the pre-intervention period. After the intervention, feedback was included at the end of the handoff based on improvement of capabilities.
Finally, the I-PASS campaign included memory aids, such as A3 posters with the mnemonics, printed glasses with the logo and screen-savers in the wards' workstations.
The spanish I-PASS version was developed by the investigators with the collaboration of investigators of the I-PASS Institute. A pilot implementation in another institution with collaboration of a principal investigator of the I-PASS Institute took place before the development of the study.
Outcomes
Assessment of written and oral handoffs
We determined the days of patient handoffs observations through simple random sampling. We carried out at least 3 observations per week in each unit.
The researchers completed a form to evaluate the adherence to key handoff elements (Supplement 1) every day of the week excluding weekends; Sheets were completed previous and after the intervention for assessing changes with the application of I-PASS bundle.
Medical errors and adverse events
Different tools were used for the measurement of medical errors and AEs:
GAPPS (global assessment of pediatric patient safety): the methodology of the “trigger tool” has been used for the detection of AEs through retrospective analysis.19,20 GAPPS proved to be reliable in identifying and measuring triggers in medical records (MR) leading to AEs.
21
Discharged patients’ MR were randomly selected and reviewed. Inclusion criteria: hospitalized patients’ MR between 07/01/2017 to 09/30/2017 (pre-intervention), and between 11/01/2017 to 01/31/2018 (post-intervention). Exclusion criteria: incomplete MR, hospitalization shorter than 24 hours, MR of patients hospitalized for psychiatric reasons or social reasons. Error reporting Mailbox: a mailbox was placed in each ward for reporting AEs detected in anonymously way. Medical prescription errors (MPE) data collection worksheet: all inpatient medical’s prescriptions were reviewed on tuesday, wednesday and thursday during the first and third week of each month along the study. The incidence, type of MPE, and severity according to the classification of the Ruiz-Jarabo group were determined.
22
Survey to evaluate physician’s satisfaction & perception: the residents of each ward answered a survey the last month of each period between 4 to 8 hours after receiving a patient’s handoff.
10
Sample size and statistical analysis
The sample size was calculated as AEs per 100 admissions. We used as a reference the AEs measured in the study carried out in 2016 at HGNPE, that showed an incidence of 30 AEs per 100 admissions. 20
We estimated a 20% decrease in AEs, based on previous studies. 15 We calculated 132 MR to be reviewed per period; 23 to obtain a power of 80%, with an alpha error <0.05. The variables were expressed as a percentage according to their distribution, mean and standard deviation or median and interquartile range.
The results collected from the observation forms were grouped into a dichotomous scale for statistical analysis considering adherence to quality elements described as: almost always, always; and non-adherence: sometimes, almost never, never. We compared the pre versus post intervention dichotomous covariate using the Fisher's exact test. To compare time–motion data pre and post-intervention we used the t-Student test. We compared AEs before and after the intervention by Wilcoxon rank sum test for proportions. We considered p values less than 0.05 to indicate statistical significance.
All analyses were completed with STATA/IC for Mac (2013 StataCorp LP®).
Ethics
In accordance with the provisions from regulations applicable to medical research in institutions oversighted by the Government of the City of Buenos Aires, approval by the Research Ethics Committee from the General Children Pedro Elizalde Hospital was obtained (IF-2017–16583833-HGNPE).
The participants signed an informed consent where they freely decided to participate in the study.
Results
We measured pre-intervention outcomes of interest during a three-month period on 14 pediatric residents, from July to September 2017. The intervention was implemented during October 2017 (one month). After that, data was collected from November 2017 to January 2018 (three months). All selected residents used the I-PASS handoff bundle during the intervention. Based on direct and standardized observations, handoff feedback was provided to residents in the postintervention period.
Handoff quality
We evaluated the adherence to key handoff elements based on the observation tool. A total of 115 observations were reviewed (56 observations in the pre-intervention period and 59 in the post-intervention period). We observed an overall key handoff elements compliance of 25% pre-intervention versus 61% post-intervention (p < 0.0001). The global adherence to the ten handoff items evaluated was 56.6% pre-intervention versus 76% post-intervention (p = 0.023). In the pre-intervention period, the most used key element was the patient's summary (66%), while the key element least utilized was the illness severity (9%). In the post-intervention period, the key element that increased its application the most was the action list (18% pre-intervention versus 80% post-intervention) followed by illness severity (9% pre-intervention versus 57.5% post-intervention) (Table 1).
Compliance with quality elements of handoff.

*Global: Handoff duration, Accuracy of Illness Severity Assessments, Quality of Patient Summaries, Omissions of important information, Irrelevant information, plus 5 key elements.
No difference was observed in the time used for the handoff in both periods (pre-intervention 5.5 ± 0.2 and post-intervention 5.3 ± 0.3 minutes per patient [p = 0.59]).
Medical errors and adverse events
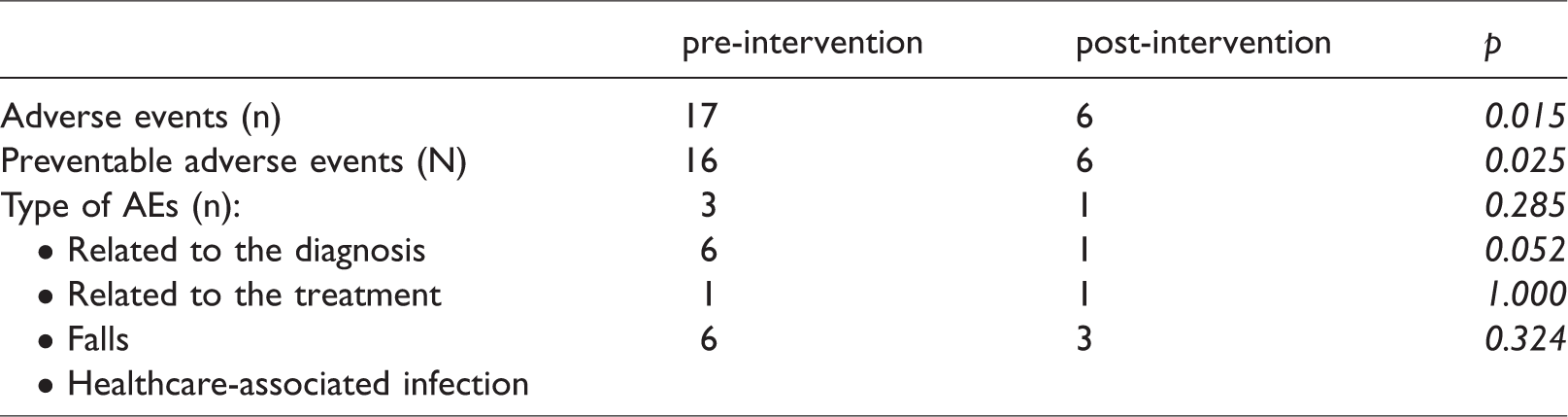
We reviewed a total of 264 medical records (132 in each period) using GAPPS. We observed 17 possible AEs in the pre-intervention period (16 preventable AEs and 1 non-preventable AEs) and 6 in the post-intervention period (6 preventable AEs and 0 non-preventable AEs), indicating 12.9 and 4.5 AEs per 100 admissions respectively (IC95: 0.010; 0.142; [p = 0.025]). This result represents a 65% decrease of AEs post-intervention (Figure 1). Considering only preventable AEs in both periods, we verified an incidence of 12.1 in the pre-intervention period and 4.5 in the post-intervention period per 100 admissions (IC95: 0.0101; 0.142; [p = 0.025]), representing a decrease of 62.8%. Types of detected AEs are shown in Table 2.

Preventable adverse events detected by GAPPS.
Preventable and non-preventable adverse events with the use of GAPPS tool.
We reviewed a total of 5715 prescriptions (pre-intervention period, 3590; post-intervention, 2125 prescriptions). There was no significant change in the rate of MPE (11.5 pre-intervention versus 9.9 post-intervention errors per 100 prescriptions [p = 0.06]). We found more severe MPE in the pre-intervention period, class B (pre-intervention 49, post-intervention 83 errors per 100 prescriptions [p = 0.0001]) and class C (pre-intervention 0.9, post-intervention 1.9 errors per 100 prescriptions [p = 0.003]). We observed a higher number of class A MPE (less severe) in the post-intervention period (50 post-intervention class A errors vs 15 pre-intervention errors per 100 prescriptions [p = 0.0001]).
We collected a total of 12 AEs pre-intervention and 4 AEs post-intervention in the assigned error mailboxes.
End of shift surveys
We took a convenience sample of 39 end of shift surveys (20 pre-intervention, 19 post-intervention). Most of the items related to patient care were improved in the post-intervention period. We did not observe changes in communication of the patient, family care plan and patient family dissatisfaction. Residents reported a higher percentage of handoff AEs, more negative events, and more handoff interruptions in the preintervention period. They also reported a higher common understanding of the patient status at the end of the study (Table 3).
Results of the end of shift survey according to the intervention period.

Discussion
Medical errors and adverse events
We found that implementation of a spanish version of the I-PASS Handoff Bundle in two argentine pediatric inpatient units, was associated with a 65% relative reduction in the rate of preventable AEs. We also found non statistically significant decrease in MPE rate, with a favorable change in the severity according to the proposed classification. This AEs reduction occurred without an increase in the time required to complete handoffs.
In concordance with our results, the initial study I-PASS implementation by Starmer et al., as a single center experience, showed a decrease in AEs from 33.8 per 100 admissions (95% CI, 27.3–40.3) to 18.3 per 100 admissions (95% CI: 14.7–21.9, P < 0.001). 14 Furthermore, in a study done in 9 pediatric residency programs belonging to hospitals in the United States and Canada it was observed a relative reduction of 23% in medical errors and a 30% reduction in preventable adverse events after I-PASS implementation. 15 A decrease in diagnostic, clinical history and physical examination related AEs was reported. However, there was no change in errors related to medication, procedures or nosocomial infections. Both publications reported that there were no changes in physicians’ workload or time spent in handoffs when using I-PASS bundle. Sheth et al. demonstrated that an I-PASS–supported handoff process was associated with improved transfer efficiency and safety culture when executing I-PASS in handoffs between the cardiovascular intensive care unit to an acute care unit. 24 Bigham et al. also showed a significant decrease in errors related to handoff after the use of a standardized tool in 23 pediatric hospitals. 10
After our intervention, we observed a decrease in the AEs reported via the error mailbox system which was very similar to the decrease detected with the use of GAPPS. In contrast, the AEs identified via different methods that we employed were not the same. Nevertheless, the decrease in self-reported AEs cannot be exclusively attributed to the intervention implemented.
Although AEs occurred frequently, our rates include very small and some serious errors and are consistent, or even lower, with the rates found in numerous other studies using the same intensive surveillance methods.20,25,26 At the beginning of the implementation of the I-PASS bundle, the average adherence to items in the procedure was similar to the adherence observed in different centers. After our quality improvement implementation, a significant difference was observed.14,15,27
Handoff quality
In the post-intervention period, we observed an adherence of approximately 60% to the five key handoffs elements which was similar to the adherence detected in the previous studies and significantly better than the pre-intervention period. 15 In addition, as observed by Coffey et al., an improvement in patient safety can be observed regardless of inconsistent adherence to the mnemonic during verbal handoff, explanation which we think applies to our study. 28 According to their study describing resident experiences with implementation of the I-PASS bundle, other important active components were identified in this complex intervention such as auto-importing of patient data into the electronic handoff document, improvements in the handoff environment, and improvements in the teamwork and communication skills. Moreover, they observed that strict adherence to the I-PASS bundle may not necessarily lead to the achievement of the desired outcomes. In our study, the synthesis and feedback component were the most challenging features of handoffs. The mentioned features were also shown to be the most challenging in previous reports.15,29
Lastly, duration of handoff was not significantly increased using I-PASS. Thus, the hand-off time remained almost constant while achieving overall higher rates of inclusion of essential patient information confirming observations from previous studies. 30
End of shift survey
In surveys answered by handoff receiver physicians, we verified improvements in most points related to the perception of AEs. Nevertheless, these results could not be compared due to the small sample size. No variation was identified in percentages related to communication with the patient's family. This was not an expected outcome since this topic was not addressed by our intervention. Surprisingly, we observed high baseline levels of receiver understanding of patients care problems after handoffs. We speculate that this high baseline level resulted from a lack of awareness of the ineffectiveness of the handoff process. Fortunately, common understanding of patients was maintained throughout the study. Other studies have shown similar results regarding the handoff process satisfaction and handoff intervention. 10
Limitations
Among the limitations of our study we can mention its design and representativeness since this is an exploratory study that took place in two hospital wards of a single institution. That precludes us from establishing a definite causal link between the I-PASS Handoff Bundle implementation and any improvement in patient safety. In addition, the external validity of the survey regarding error perception was not evaluated in this study. Furthermore, physician’s behavior and their use of I-PASS format may have been influenced by the observer’s presence. Additionally, the severity of patients’ affections in both periods could not be assessed to ensure their similarity. Finally, patients involved were hospitalized in different seasons of the year which might have caused seasonal bias.
The application of the I-PASS bundle in our cohort of medical providers which combined and applied together several domains (teamwork training, mnemonics, observations and feedback) prevented us from determining which element of the intervention was the most effective. Still, we adopted this approach given that transitions of care are known to endanger the quality of patient care and patient safety and it has been demonstrated to be a successful strategy in a number of previous studies.31–33
Conclusion
We conclude then that the implementation of an spanish version I-PASS bundle in two pediatric wards of an argentine tertiary care center was associated with a significant reduction in the rate of AEs, improvements in handoff quality without modifying duration and it was not associated with a significant reduction in MPE.
To our knowledge, this is the first study that demonstrates positive results with the application of an IPASS bundle in a non-english speaking setting. To improve external validity of our results, a larger study will need to be conducted.
Supplemental Material
sj-pdf-1-cri-10.1177_2516043520961708 - Supplemental material for Improved handoff quality and reduction in adverse events following implementation of a Spanish-language version of the I-PASS bundle for pediatric hospitalized patients in Argentina
Supplemental material, sj-pdf-1-cri-10.1177_2516043520961708 for Improved handoff quality and reduction in adverse events following implementation of a Spanish-language version of the I-PASS bundle for pediatric hospitalized patients in Argentina by Facundo Jorro Barón, Celina Diaz Pumara, María Agustina Janer Tittarelli, Agustina Raimondo, Marcela Urtasun and Lucila Valentini in Journal of Patient Safety and Risk Management
Footnotes
Authors’ contributions
Jorro Barón, Facundo: Conception, study design, data analysis and interpretation, writing of the article, critical review and approved final version of the manuscript. Diaz Pumará, Celina: Data collection, interpretation of data, critical review and approved final version of the manuscript. Janer Tittarelli, María Agustina: Data collection, interpretation of data, critical review and approved final version of the manuscript. Urtasun, Marcela: Data collection, interpretation of data, critical review and approved final version of the manuscript. Raimondo, Agustina: Data collection, interpretation of data, critical review and approved final version of the manuscript. Valentini, Lucila: Data collection, interpretation of data, critical review and approved final version of the manuscript.
Acknowledgements
The author would like to thank specially the residents of pediatrics of the HGNPE who collaborated in this study. The author would like to also thank Ezequiel Garcia Elorrio, Michelle Chismechian and Nicolás Llosa for their assistance in reviewing this article and Amy Starmer for her assistance with the adaptation of the I-PASS bundle.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
In accordance with the provisions from regulations applicable to medical research in institutions oversighted by the Government of the City of Buenos Aires, approval by the Research Ethics Committee from the General Children Pedro Elizalde Hospital was obtained (IF-2017-16583833-HGNPE).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.