
Abstract
Introduction
Patient safety is a global concern for both health professionals and the public. Studies show that evaluating patient safety culture can help improve patient safety outcomes. Nursing care strategically places nurses at the centre of patient safety promotion and their proximity to patients makes them the drivers of patient safety. Managerial decisions regarding patient safety impact greatly on patient safety outcomes in the healthcare organization. This study aimed to assess the managerial patient safety practices that influence adverse event reporting in three hospitals in the Savannah Region of Ghana.
Methods
A quantitative cross-sectional design was used to collect data from 210 participants in three hospitals. Data were analysed using descriptive, Pearson's correlation and linear regression.
Results
It was found that patient safety practices with good positive rating scores were management support (56.6%), managers' expectations (62.8%) and feedback about errors (56.2%). Areas with weak patient safety practices were staffing levels (42.4%), open communication (40.2%) and non-punitive response to errors (36.7%). Again, nurses' attitude towards adverse events reporting was generally low (37.3%). Managerial patient safety practices that had significant associations with adverse events reporting were management support (r = .18, p < .001), open communication (r = .19, p < .001), non-punitive to errors (r = .21, p < .001) and feedback about errors (r = .37, p < .001). Again, the significant predictors of adverse events reporting were feedback about errors (β = .36, p < .001) and non-punitive response to errors (β = .21, p < .01).
Conclusion
Nurses perceived patient safety culture in their units to be good. Although nurses' attitude towards adverse events reporting was low, the significant predictors of adverse events reporting were feedback about errors and non-punitive response to errors. Therefore, healthcare managers should continually strengthen patient safety to ensure optimal care outcomes.
Implications for nursing practice
Feedback on errors and non-punitive response to errors had a great influence on adverse events reporting, managerial failure to provide feedback and a non-punitive work environment could result in under-reporting of adverse events. This can be a major threat to patient safety; hence clinical practice should be aware of this and put in strategies to appropriately address them.
Background
Patient safety has been defined as the prevention of errors and adverse effects associated with health care. 1 Organizations that prioritize patient safety work to minimize preventable harm to patients, ensure high-quality medical care and treatment, and increase the level of patient satisfaction. 2 However, healthcare delivery is not always as safe as it should be.3,4 Therefore, the safety of patients has become a global concern for both health professionals and the public.5,6
Globally, it is estimated that as many as 1 in 10 patients are harmed while receiving care in the hospital. 7 This accounts for 427 million hospitalizations annually worldwide with approximately 43 million adverse events occurring in patients during these hospitalizations. Statistics have shown that on average, one patient gets injured as a result of their healthcare every 35 s in the United Kingdom. 8 In Canada, approximately 185,000 harmful adverse events are recorded every year, and about 38% of these adverse events are preventable. 9 In the United States of America, about 44,000 to 98,000 patients die of preventable medical errors. 10 In the low and middle-income countries (LMICs), it is estimated that 134 million adverse events occur in hospitals due to unsafe care, contributing to 2.6 million deaths annually. 11 In Sub-Saharan Africa, especially in Nigeria and Uganda, evidence suggests that at least 30% of the patients attending hospitals are likely to experience an adverse event. 12 In Ghana, approximately 8.7% of Ghanaians seeking health care are accidentally harmed. 13 Patient safety is compromised in high, middle, and low-income countries, and thus, should be a global priority.
One key determinant of patient safety is safety culture. 14 Patient safety culture has been defined as the set of shared values, attitudes, perceptions, beliefs, and behaviours that support safe practices among individuals in healthcare organizations.14,15 In the context of this paper, the terms patient safety practice and patient safety culture are used appropriately to refer to attitudes and values that influence behaviours respectively. High patient safety culture is associated with low patient mortality rates, 16 high percentages of medical error reporting, and positive patient care assessments leading to high patient satisfaction. 17 The absence of patient safety culture can result in inpatient mortality, disability, patient distrust of the healthcare system, frequent readmissions, prolonged length of stay, increased patient pain, and unnecessary costs.7,18
Vogus, Sutcliffe and Weick consider patient safety culture to be influenced by enabling, enacting, and elaborating practices that influence patient safety outcomes. 19 Each safety practice comprises actions that affect patient safety outcomes. Enabling safety culture focuses on leader or managerial actions that direct attention to patient safety and make it safe for people to speak up. Enacting safety culture implies highlighting threats to safety and effectively mobilizing resources to resolve threats. Elaborating consists of using feedback and information to continuously learn and improve.
Managers and leaders of healthcare organizations play important roles in patient safety culture and can have a significant influence over the organization's patient safety culture, particularly regarding adverse event reporting. It has been suggested that leaders' behaviours such as managers' support, managers' expectations, and actions in promoting patient safety, open communication, non-punitive response to errors, staffing levels, and feedback about errors 18 influence frontline adverse events reporting behaviours. Due to the significant influence leaders can have over an organization's safety culture, particularly regarding adverse event reporting, it is necessary to examine enabling practices in greater detail.
The practice of reporting adverse events is one of the critical components of a patient safety culture. This practice provides the opportunity for employees to report near misses, incidents, and accidents openly and honestly. There is some evidence that an increase in the reporting of adverse events and near misses leads to improved outcomes. A study on medication error reporting indicates that when errors are reported, the reports are used to enhance the communication process, inform education or training, and prompt policy changes. 19
Given that error reporting is associated with improved healthcare outcomes, an important question is whether adverse events are sufficiently reported. In the United States and the United Kingdom, studies have revealed that under-reporting of adverse events may be as high as 96.0% 20 and that only 10% of adverse events were captured with hospital electronic incident reporting systems. 21 In Ethiopia for instance, about 69.0% of the study participants have never reported an adverse event or an error. 22 This evidence is supported by a comparative study in Jordan, where 78.0% of nurses failed to report medication errors. 23 Litany of reasons have been attributed to such low reporting behaviour such as inadequate knowledge, time burden of submitting a report, fears of sanctions by superior and blaming and shaming of staff.24–27 These studies have only been conducted in high income settings and there is a need to understand how these leadership behaviours influence adverse events reporting in low-income settings.
In Ghana, it is estimated that the reporting rate of harmful incidents is 6 in 1,000,000 populations according to the WHO program for international drug monitoring. 28 In two psychiatric hospitals in Ghana, about 56.0% of nurses and nurses assistants surveyed did not report adverse events that occurred in the course of delivering healthcare. 29 This is a clear demonstration that the reporting of adverse events in Ghana and globally is generally low and is far from representative of the actual number of errors and adverse events that occur in healthcare.
In the light of these low adverse event reporting trends among healthcare professionals, there is a need for healthcare organizations to assess managerial patient safety practices that influence adverse event reporting. Thus, this study was aimed at assessing managerial patient safety practices that influence adverse events reporting among nurses of selected hospitals in the Savannah Region of Ghana. This study also aimed to examine the relationship between enabling patient safety practices and adverse events reporting.
Methods
Design and setting
This study was a cross-sectional survey of three selected hospitals in the Savannah Region of Ghana. Savannah Region is in the northeastern part of Ghana with its capital in Damongo. Administratively, the region has 7 districts with a total population of 578,235.30,31 The region occupies a total land area of 37,582 square kilometers (sq. km), constituting 16.09% of the total land area of Ghana. The region has three major hospitals, namely, West Gonja, Bole and Salaga district hospitals.
West Gonja District Hospital (mission hospital, run by a religious institution) has a total bed capacity of 100 with a staff of 320, of whom 133 are nurses. Bole District Hospital (government hospital) has a bed capacity of 132 with a staff of 194, of whom 119 are nurses. East Gonja (government hospital) has a bed capacity of 100 and a staff of 161 of whom 133 are nurses. There are 385 total nurses across all three hospitals. These hospitals do not have a mandatory or voluntary event reporting system.
Sample and data collection
Of the 385 nurses across all three hospitals, the study target for recruitment was 216 to make room for non-response. These nurses included registered general nurses, registered midwives and enrolled nurses. Based on the nursing staff of the hospitals, a ratio of 3:2:3 was used to recruit respondents from the three hospitals. Professional or auxiliary nurses who have worked in the hospitals for at least six months were included in this study. Those with less than six months of experience were excluded due to potential lack of familiarity with the hospital and its patient safety operations. Participants were recruited from the selected hospitals using a quota sampling technique to ensure adequate representativeness of the population. Written informed consent was received from each participant after which the questionnaire was administered. Retrieved questionnaires were cross-checked for completeness and errors and then coded before data entry using Statistical Package for Social Sciences (SPSS) version 20 software.
Study instrument
The English version of the Hospital Survey on Patient Safety Culture (HSOPSC) developed by the Agency of Healthcare Research and Quality (AHRQ) was adapted for data collection. The HSOPSC instrument had Cronbach's alpha coefficient values ranging from 0.63 to 0.84. 32 The instrument had 12 dimensions with 42 items in the questionnaire excluding participants' characteristics.
The six dimensions of the HSOPSC questionnaire (See Appendix 1) that are more applicable to the context of this study were adapted to assess patient safety practices among nurses. These dimensions include management support (3 items), managers' expectations (4 items), communication openness (3 items), non-punitive response to errors (3 items), feedback about errors (3 items) and staffing levels (4 items). The items were 5-Point Likert scale ranging from “5 = strongly agree” to “1 = strongly disagree” or “5 = always” to “1 = never.” Furthermore, the HSOPSC questionnaire includes frequency of adverse event reporting (dependent variable with three items) on a five-point Likert scale, which asks participants to rate how frequently mistakes are reported. The questionnaire was administered to 216 nurses by the researchers. This was done either before the start of work or after each shift so as not to disrupt work in the various wards.
Ethical consideration
The study received ethics approval from both the Ethics Review Committee of Ghana Health Services (ERC- GHS 041/11/19) and the Institutional Review Board of Noguchi Memorial Institute for Medical Research (IRB-NMIMR 032/19-20). Permission was obtained from the authorities of the selected hospitals.
Data analysis
Data were analysed using descriptive and inferential statistics. Descriptive statistics analysed included the participants' characteristics, enabling safety practices and adverse events reporting using frequencies, percentages, means and standard deviations. Additionally, Chi-square test, Pearson's correlation coefficient, and hierarchical multiple linear regressions were used for inferential statistical analysis. The data appeared to follow the normal distribution curve on a histogram and the data were checked for any outliers before the analysis was performed. Hierarchical multiple regression analysis was computed by using adverse events reporting as a dependent variable against the six patient safety practices as independent variables after controlling for participants' variables (gender, work area, and years of work experience). Before computing multiple regressions, items in each of the six dimensions were computed into a single variable to form a composite score. All negatively worded items were reverse coded or recoded. Independent variables (dimensions) were used as linear predictors. In all these analyses, a p-value of <.05 was considered statistically significant.
Validity and reliability
The validity of the study instrument was established through face and content validity. Face validity was ensured by arranging the questionnaire into sections to reflect the research objectives. To maintain content validity, the authors conducted an extensive literature review and structured the sections of the questionnaire to ensure all variables under investigation were covered. For reliability, the instrument was piloted at Tamale West Hospital in the Northern Regional Capital, Tamale, with 20 nurses to identify and revise the questions that were not clear on the instrument. The Cronbach's alpha coefficient values for the adapted instrument ranged from 0.62 to 0.91, hence the authors made minimal changes, including changing a few words such as “agency staff” for “part-time staff” and “crisis mode” for “pressure build ups” to ensure the study instrument was Ghana-specific. Upon collecting the main data, Cronbach's alpha coefficient values were again determined. These Cronbach's alpha coefficient values ranged from 0.64 to 0.83. The authors, therefore, concluded that this instrument had good validity and reliability, thus the instrument was appropriate to assess the patient safety culture of selected hospitals in the Savannah Region of Ghana.
Results
Participants' characteristics
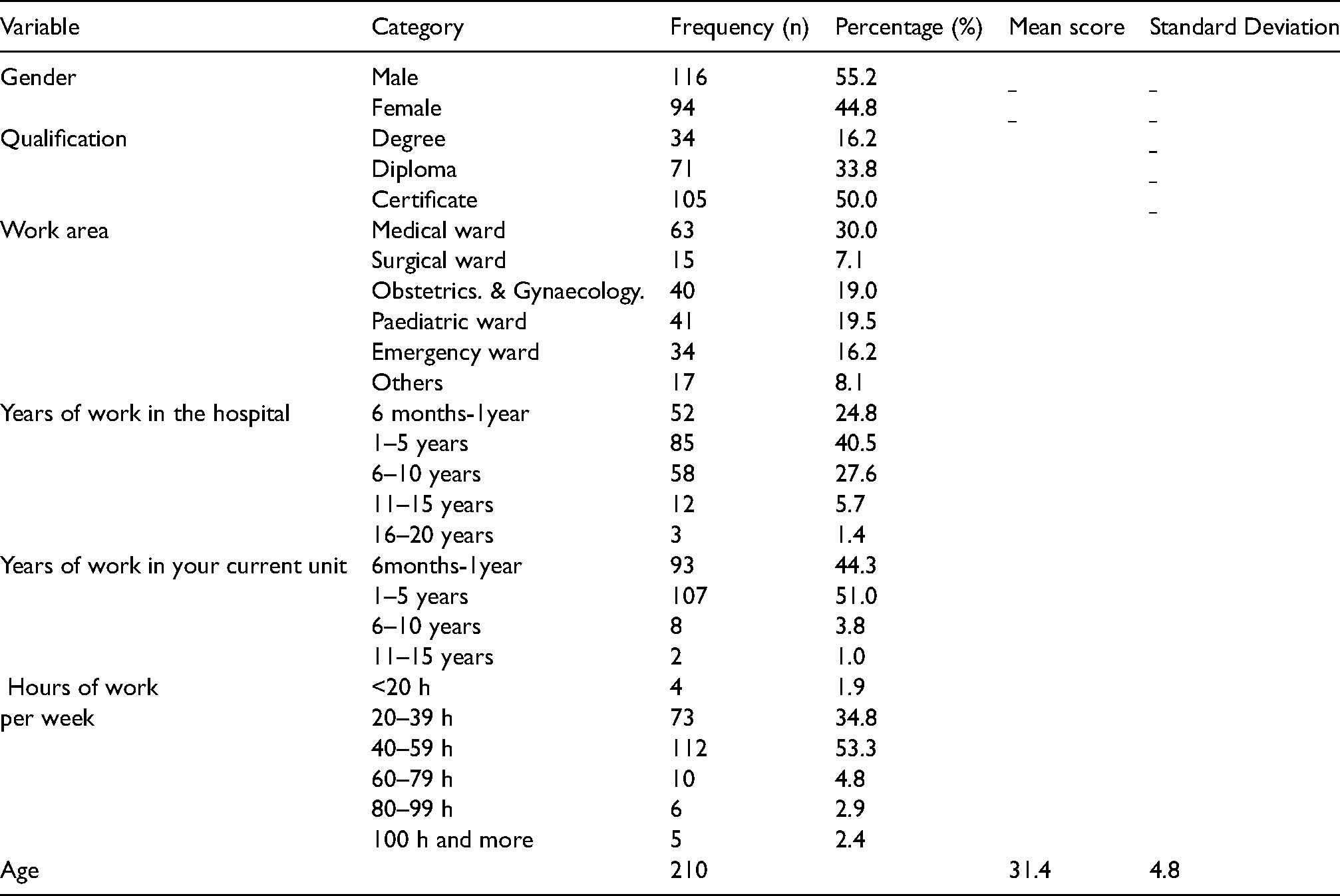
This study had a 97.2% response rate, with 210 out of 216 nurses participating. Out of 210 (100%) nurses who responded to this study, 55.2% were males, 50.0% were certificate holders and 30.0% worked in the medical wards who were either registered general nurses or enrolled nurses. Approximately, 40.5% of the nurses had between 1–5 years of work experience in the hospital, and more than half, (51.0%) of the nurses had worked 1–5 years in their current units. Moreover, most of the nurses, (53.3%), had a weekly workload of between 40–59 h per week. Details of the participants' characteristics are summarized in Table 1.
Participants' characteristics.
Enabling patient safety practices
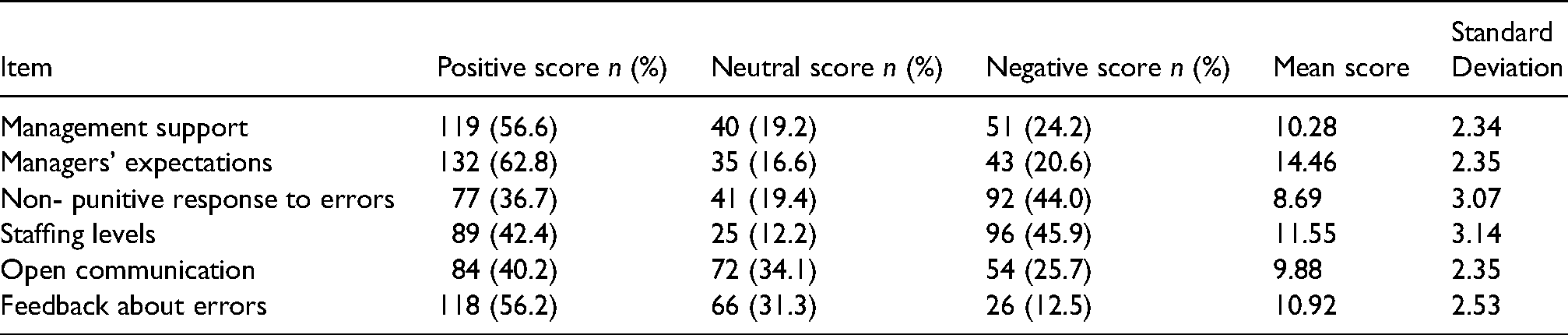
It was found that out of the six enabling patient safety practices, three scored significantly higher than the others. These were managers' expectations and actions in promoting patient safety (62.8%), managers' support for patient safety (56.6%) and feedback about errors (56.2%). Patient safety practices that recorded relatively low positive response scores were non-punitive response to errors (36.7%), open communication (40.2%) and staffing levels (42.4%). Details are presented in Table 2.
Enabling patient safety practices.
Adverse events reporting
Regarding frequency with which adverse events are reported, the results indicated that 37.3% of nurses had reported adverse events, including near misses. This represents a positive score. A higher percentage of nurses (62.7%) had either never reported adverse events or were not sure about whether they had ever reported adverse events. Details are summarized in Table 3.
Adverse events reporting.

Relationships between participants' characteristics and adverse events reporting
A Chi-square test (χ2) was used to examine the relationship between participants' characteristics and the adverse events reported. It was found that there was a significant relationship between gender and adverse event reporting [χ2(1) = 4.14, p = 0.04] with female nurses (53.8%) more likely to report adverse events. Work area and adverse events reporting were significantly related [χ2(3) = 31.20, p < 0.001] with 38.5% of midwives and general nurses working in the obstetrics and gynaecology units most likely to report adverse events when compared with other units. There was a significant relationship between years of work experience in the hospital and adverse events reporting [χ2(2) = 12.72, p < 0.01] with nurses who have had work experience of 6 years or more (47.4%) more likely to report adverse events (Table 4).
Participants' characteristics and adverse events reporting.

Relationship between enabling safety practices and adverse events reporting
Bivariate correlation analysis was conducted to examine the relationships among the studied variables. The results found a significant positive correlation between management support, non-punitive response to errors, open communication and feedback about errors and adverse events reporting (p < .01). However, enabling safety practices such as managers' expectations and staffing levels had no statistically significant relationship with adverse events reporting (p > .05) as acknowledged by nurses (See Table 5).
Bivariate correlation between enabling patient safety practices and adverse events reporting.

* P < .05; ** P < .01.
The influence of enabling safety practices on adverse events reporting
A multiple regression analysis was performed to determine whether enabling patient safety practices and participants' characteristics would be able to predict frequency of adverse events reporting. The results show that out of the four enabling patient safety practices, that had statistically significant relationships with adverse events reporting (Table 4), two enabling patient safety practices, non-punitive response to error (β = .22, p < .01) and feedback about the error (β = .37, p < .001), were found to be significant predictors of adverse events reporting. The participants' characteristics and the other two enabling patient safety practices statistically had no predictive influence on adverse events reporting. Details are summarized in Table 6.
Influence of enabling patient safety practices on adverse events reporting.

Dependent variable: Adverse events reporting criterion level:.05.
Discussion
Enabling patient safety practices
This study assessed managerial patient safety practices that influence adverse events reporting among nurses of selected hospitals in the Savannah Region of Ghana. It explored enabling factors and how these contribute to the reporting of adverse events in respect of patient safety. Enabling safety practices are actions at the managerial level that direct the attention to patient safety and make it safe for people to speak up and act. These practices include manager's support, manager's expectations, open communication, non-punitive response to errors, staffing levels and feedback about errors. Some patient safety scholars have indicated that when enabling safety practices are routinely upheld, they affect the operational level activities. As a result, frontline staff can exhibit certain behaviours such as patient safety event reporting that can influence safety outcomes. 33
Management support for patient safety is a major significant safety practice that has positive impact on the safety of patients in healthcare institutions. In this study, about 56.6% of nurses surveyed agreed that management had shown interest and commitment in all matters related to patient safety. The interest of management in patient safety is an indicator to frontline nurses that patient safety is of paramount importance to ensure positive patient outcomes. As such, there is a strong commitment by management to address any issues that come up in the course of delivering healthcare to patients. Therefore these nurses do not hesitate to report any adverse events to their management as they recognise that there will be prompt response to resolve any difficulties. Such commitment could result in fewer incidences of adverse events. Even in the unlikely event that these adverse events occur, the commitment demonstrated by managers relative to safety-related issues would influence them to report with lessened fears or hesitation. A relatively higher rating score for management support for patient safety has been supported in recent studies by Abuosi, Akologo and Anaba, 34 corroborating the work of Khoshakhlagh et al. 15 Elsewhere, studies have shown that when hospital management supports safety-related issues, there is an increase in adverse events reporting.35,36 Other studies have reported that when management placed emphasis on patient safety and safety-related issues, there is a correlation with better safety outcomes and fewer incidences of adverse effect. 37 Nurses have a duty to report any error, behaviour or conduct affecting patient safety, thus when they perceive there is managerial support relative to patient-safety issues, they are enabled to report adverse events promptly.
Managerial support for patient safety is operationalized by creating an environment that is blame-free on matters relating to patient safety, prioritizing patient safety, and showing interest when adverse events are reported. Such support would encourage healthcare providers, particularly nurses, to report adverse events. Although the scores recorded in the present study, fell short of benchmark criteria defined by AHRQ, the appreciable high scores are indications of management support for patient safety. Therefore, it is recommended for healthcare managers to prioritize safety and invest the needed resources on patient safety.
The nursing staff gave a positive response score for managers' expectations and actions in promoting patient safety, which was the highest of all the enabling safety practices showing that healthcare managers of the selected hospitals consider safety problems and staff suggestions seriously. Clearly, healthcare managers' actions are critical in enabling safety practices and can positively influence patient safety outcomes. Such high rating of managers' actions is not commonplace elsewhere. For example, Rajalatchumi and Ravikumar found that healthcare managers would not under any circumstances encourage staff to disregard safety problems in the discharge of their duties. 38 It is evident how nurses are influenced by their managers' expectations in promoting patient safety. Nurses thus tend to be responsive to these positive expectations and their actions on the wards tend to support patient safety rather than covering up any adverse events that might possibly occur in the delivery of care to patients. For example, the nurses in this study confirmed that they do not compromise on patient care by cutting corners as, such actions could lead to unintended occurrence of adverse events that result in inpatient hospitalization, prolongation of existing hospitalization, death or significant disability or incapacity.
In this study, about 56.2% of the nurses believed that they had been provided with feedback when errors are reported. This means that, though there is room for improvement, the majority of the nurses were informed by their managers about errors that happened in their units and the necessary changes put in place to avert future occurrence of such events. Other researchers have also reported higher rating scores for feedback about errors.34,37 It is apparent therefore that when healthcare workers, including nurses, are given feedback promptly following reported adverse events, they would be motivated to report more of such incidences when encountered and, this would encourage them to inform others that are connected to the errors. The giving of feedback should usually be done in a timely manner by communicating relevant information about the incident and not dwelling on character or personality of the worker involved. This is a positive patient safety practice that healthcare managers can use to enhance effective communication on matters relating to patient safety.
Previous research has demonstrated that non-punitive response to error is associated with likelihood to report adverse events. However, it has been found that non-punitive response to errors is the least developed managerial practice among healthcare workers.39–41 Respondents in this study provided low scores around non-punitive response to error reflecting a system where nursing staff tend to experience some form of punitive measures after adverse events reporting. They were either held personally accountable or records of their errors were saved in their files when they commit errors. A punitive response to error is inadequate to improve patient safety. When an individual is blamed for error, it does not take away system-based drivers of error such as lack of resources, high patient to nurse ratios and poor management practices. 42 The errors are likely to occur again, hence, it is essential to identify the root causes of system failure and address these systemic changes and the safety culture in general. Some patient safety researchers have attributed the low score on non-punitive response to fear and intimidation among healthcare workers43,44 where there is a risk of losing one's job. In such work environments, a culture of silence among healthcare workers regarding their honesty and responsibility for error reporting is created. This could lead to healthcare workers deliberately concealing future adverse events to free them from accountability.
Open communication across the three selected hospitals was generally poor as majority (59.8%) of the nurses acknowledged that they did not feel free to openly discuss safety-related problems. This suggests that there is a weak relationship between nurses and their superiors and among nurses themselves. Such a weak communication system could affect sharing of patient information and negatively impacts patient safety, particularly where the leadership style adopted by management is that which fosters dictatorship. Some studies have reported challenges among healthcare workers in discussing patient safety-related problems with managers38,45 and these have been attributed to weak open communication, poor relationships between healthcare managers and frontline staff and disputes among staff.43,44 The consequence of this weak relationship is a communication gap in the work environment relative to patient safety. Thus, organizing regular patient safety meetings, streamlining communication channels and giving employees a voice can help address this communication gap.46,47 These strategies would offer nurses the opportunity to discuss safety-related issues devoid of fear and intimidation.
Adverse events reporting is critical in improving patient safety in hospitals. In this study, adverse events reporting was low (37.3%). This signifies that adverse events were less frequently reported. This may be attributed to punitive responses to adverse events reports. Such punishment may take the form of dismissal 27 or shaming the individual staff. 35 As a result, many healthcare workers may be apprehensive about the outcomes of reporting adverse events, thus instead of reporting, they would rather conceal their errors to avoid facing sanctions from superiors. Thus, when adverse events are unreported, hospitals cannot learn from similar adverse events to prevent them from happening. Similar findings have been reported showing lower positive response score among healthcare workers on adverse events reporting.48,49
Predictors of adverse events reporting
The authors also examined the relationship between enabling patient safety practices such as manager's support, open communication, feedback about errors and non-punitive response to errors and adverse events reporting. A significant positive relationship was found between adverse events reporting and manager's support, open communication, feedback about errors and non-punitive response to errors. This is consistent with the results of other studies which found that reporting of adverse events depends on the manager's support, open communication, feedback about errors and non-punitive response to errors.37,48 A supportive manager tends to receive information about adverse events because of the enabling environment created in their unit. Nurses working in a facility where the enabling factor of support from their nurse managers is available are more likely to report adverse events from this study. Feedback about errors was found to be a significant predictor of adverse event reporting, as nurses' likelihood of reporting adverse events was correlated with feedback about errors. When the feedback is non-punitive, timely, and judgemental, nurses respond favourably and are ready to report adverse events promptly. This practice can promote confidence among nurses and encourage them to report acts of adverse events committed to their superiors. When healthcare professionals are provided with the needed feedback, it has a predictive effect on adverse events reporting.18,22 Therefore, there is the need to improve adverse event reporting among nurses in hospitals since timely feedback is a facilitator toward this goal. Non-punitive response to errors was found to have a significant influence on adverse event reporting. When management adopts a non-punitive approach to adverse events reported, nurses' hesitation to report adverse events decreases. This goes to show that nurses tend to report when records of adverse events are not placed on staff files to be used against them in the future. Traditionally, the blame, name and shame approach were used to solve problems within the healthcare industry following reports of adverse events, what James Reason calls active failures due to unsafe acts by frontline healthcare providers. 50 Such an approach will do more than good thus safety researchers have therefore advocated for a system approach to problem-solving. This approach focuses on both active and latent failures due to top and middle-level management actions or inactions that give rise to active failures at the frontline. 50 Given this, the work environment should be such that it is blame-free, shame-free and non-punitive in order to increase willingness to report and therefore improve patient outcomes.
Limitations and strength
Though this study provides valuable information regarding adverse events reporting, it is not without limitations. Specific patient safety indicators from event reports such as medication errors, injection abscesses, falls from beds, wound infections, and transfusion errors among others were not directly evaluated. Therefore, it was a challenge to establish a direct relationship between managerial patient safety practices and individual adverse events reported. Additionally, using a structured instrument to collect the data from nurses somewhat restricted the nurses from freely expressing their views relative to patient safety.
Notwithstanding the study limitations, this study adapted a study instrument that has been extensively used on patient safety culture studies with robust reliability. Additionally, due to the large sample size, the findings are more likely to generalize to other areas, although caution should be exercised to reflect the reality of patient safety in other healthcare institutions.
Implications and recommendations
Patient safety culture is an emerging concept in Ghana, most notably in the Savannah Region, yet it is an essential determinant of the health outcomes of patients. In this study, nurses perceived patient safety culture in their units to be linked to managerial support and non-punitive response to errors. It implies that nurses attitude towards adverse events reporting would likely increase if they are not judged and punished by management for errors that occur during delivery of care. The significant predictors of adverse events reporting were feedback about errors and non-punitive response to errors. Therefore, healthcare managers should continually ensure open communication channels and prioritize building a work environment that is non-punitive and blame-free to encourage adverse event reporting among nurses.
In addition, patient safety culture and its implications on care outcomes have not been well established in the region, implying a gap in managers' practices in building a culture of safety. Healthcare managers should therefore create patient safety culture awareness through training programs such as conferences, seminars and workshops to enhance patient safety.
Conclusion
This study sought to assess how managerial patient safety culture practices impact adverse event reporting among nurses in the Savannah Region of Ghana. Managerial patient safety practices rated highly by nursing participants were the manager's support, manager expectations and feedback about errors. Non-punitive response to errors and feedback about errors were found to be significant predictors of adverse events reporting. These findings specify areas in which managers should prioritize in order to improve their event reporting culture and therefore improve patient outcomes.
Footnotes
Acknowledgements
The author (s) would like to thank Rev. Danny Jaynes, management of West Gonja Hospital, Bole hospital, and Salaga for their support and cooperation during the data collection. We also want to thank all the nurses who out of their busy schedules participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Appendix 1
See Table A1.