
Abstract
Purpose
Gaining understanding of glaucoma-related malpractice litigation may highlight ways to improve patient care and minimize risk of litigation. This study aims to analyze the outcomes and characteristics of glaucoma-related malpractice litigation.
Materials and Methods
The Westlaw legal database (Thomson Reuters, New York, NY, USA) was used to identify cases regarding ‘malpractice’ AND ‘glaucoma’ or related terms. Cases were analyzed for characteristics such as alleged cause of malpractice, outcome, and demographics.
Results
The initial search terms yielded 498 results, 107 of which met further inclusion criteria. 38 (36%) were resolved via jury trial. Of these, verdicts in favor of the plaintiff were issued in 14 cases (34%), with median adjusted damages of $702,986. Of all 107 cases in the study reviewed, 65 (61%) resulted in verdicts in favor of the defendant. Ophthalmologists were named as defendants in 85% of the cases (with glaucoma specialists representing 7% of the ophthalmologists); optometrists in 24%. Sixty percent of the cases involved non-surgical treatment. The most common medical reasons for litigation were failure to diagnose (38%), and inappropriate/negligent treatment (36%). The most commonly litigated surgical procedures were cataract surgery (48%) and iridotomy/iridectomy (19%).
Conclusion
Glaucoma-malpractice litigation has increased, with medical mismanagement alleged in the majority of cases. Defendants are frequently successful in obtaining pre-trial dismissal, but the risk of liability increases in cases going to trial. A minority of cases involved glaucoma specialists. This historical analysis of glaucoma-related malpractice cases might provide perspective and aid physicians seeking to avoid litigation.
Introduction
Ophthalmologists have a high risk of facing malpractice claims during their careers, as between 5% and 10% of ophthalmologists face such a claim annually.1, 2 These realities have negative consequences for patients and physicians alike. Encumbered with an increasing frequency of claims, mounting legal fees, and skyrocketing awards to plaintiffs, physicians have become more likely to modify their behavior in response to these pressures. 3 Insurance premiums are also affected by the threat of litigation, and this results in the practice of defensive medicine, which can lead to further increases in healthcare costs.3–5
While previous studies in glaucoma-related malpractice litigation are informative and provide valuable data, they are limited to using the database of one insurer and often focus primarily on ophthalmologists rather than optometrists.6–8 We aim to add to the existing literature by analyzing outcomes and characteristics of all medical and surgical glaucoma-malpractice litigation cases in the WestLaw database for legal research; this database spans over 75 years and contains information from greater than 40,000 databases of cases and settlements across the country. A prior study using the WestLaw database analyzing ophthalmologist-only litigation from 1960 to 2014 reported that glaucoma-related litigation comprised 6.5% of all ophthalmology cases resulting primarily in favor of the defendant (62%) and found similarities among verdicts and settlements between glaucoma-related malpractice litigation and ophthalmology as a whole. 9 The present study provides further insight into litigation also involving optometrists as well as analyses into specific glaucoma procedures. This paper aims to highlight ways to improve patient care, as well as how providers can minimize their risk of glaucoma-related malpractice litigation.
Materials and methods
Our findings were reported using descriptive statistics. The WestLaw database (Thompson Reuters, New York, NY, USA) was searched during August of 2019 to identify cases regarding ‘malpractice’ AND ‘glaucoma’ or related terms including: ‘angle closure’, ‘aqueous drainage’, ‘bleb’, ‘cyclophotocoagulation’, ‘CyPass’, ‘express shunt’, ‘goniotomy’, ‘intraocular pressure’, ‘iridotomy’, ‘iStent’, ‘Xen’, ‘narrow angle’, ‘trabeculotomy’, ‘suprachoroidal shunt’, ‘trabeculectomy’, ‘trabeculoplasty’, and ‘tube shunt’. The included search terms yielded 498 results, 107 cases of which involved a malpractice case centered on medical and/or surgical management of glaucoma. Reasons for exclusion included: irrelevance (82%; not involving ophthalmology or optometry), involving ophthalmology but not glaucoma (8%), cases in duplicate lawsuits which were eventually combined with later decisions (5%), cases excluded upon the advice of our legal expert who determined they were not convincing for the dataset due to irrelevance to our study question (3%), and cases excluded for lack of information available (2%).
Legal record review included: case name and number, year of suit, state of filing, whether or not the case was closed, and award amount either by jury or settlement, plaintiff and defendant, case outcome, and legal procedural information. Medical analysis of the cases included: summary of clinical course, whether the intervention was medical or surgical/procedural, the type of surgery, type of medical misadventure, alleged complication, and clinical diagnosis. Defendant analysis included: gender, age at initial contact with patient, type of practice, presence of board certification and/or glaucoma fellowship training, and medical training (we chose to include both ophthalmologists and optometrists). Not all information was available for every case. Settlements and awards were adjusted for inflation to 2019 US dollars (https://www.usinflationcalculator.com/) to permit meaningful comparison.
The t test (Microsoft Excel), chi-squared test, and Fisher's exact test (https://www.socscistatistics.com/default.aspx) were used when comparing groups. A P < 0.05 rule for decisions was established as the null hypothesis rejection criteria for all tests.
Results
Of the 107 cases analyzed, 24% featured optometrists, 86% featured ophthalmologists, and 7% featured glaucoma specialists specifically. The cases spanned 1942 to 2019 (Figure 1). The four states with the most glaucoma-related malpractice cases in this study were New York (19%), California (12%), Louisiana (8%), and Indiana (7%). All other states were named in less than 5% of cases.

Number of glaucoma-malpractice cases per decade in the WestLaw database. Glaucoma-related malpractice cases increased over time, with the most notable increment between the 1980s and 1990s, and with most cases occurring in the last decade.
Ninety-eight ophthalmologists were named as defendants (mean ± standard deviation [SD] age: 49.4 ± 12.7 years old; 92% male). A majority (82%) of ophthalmologists named as defendants were board certified. Most (44%) practiced in a private practice setting, 25 (26%) practiced in a hospital setting, 29 (29%) practiced in an unspecified setting, and 1 (1%) practiced in a military setting. Twenty-five optometrists were named as defendants (mean age 44.9 ± 11.5 years old) and a majority were male (84% male). Most optometrists (72%) were in a private practice setting, whereas 28% practiced in an unspecified setting.
Of the 107 cases, 64 cases (60%) involved non-surgical treatment. Of the 81 allegations of medical misadventure extracted, ‘failure to diagnose’ was the most common (48%), with some cases having more than one allegation (Figure 2A). The remaining 42 cases (40%) had surgical treatment, across which 54 procedures were extracted with some cases having more than one reported procedure (Figure 2B); cataract surgery (48%) was the most commonly performed procedure.
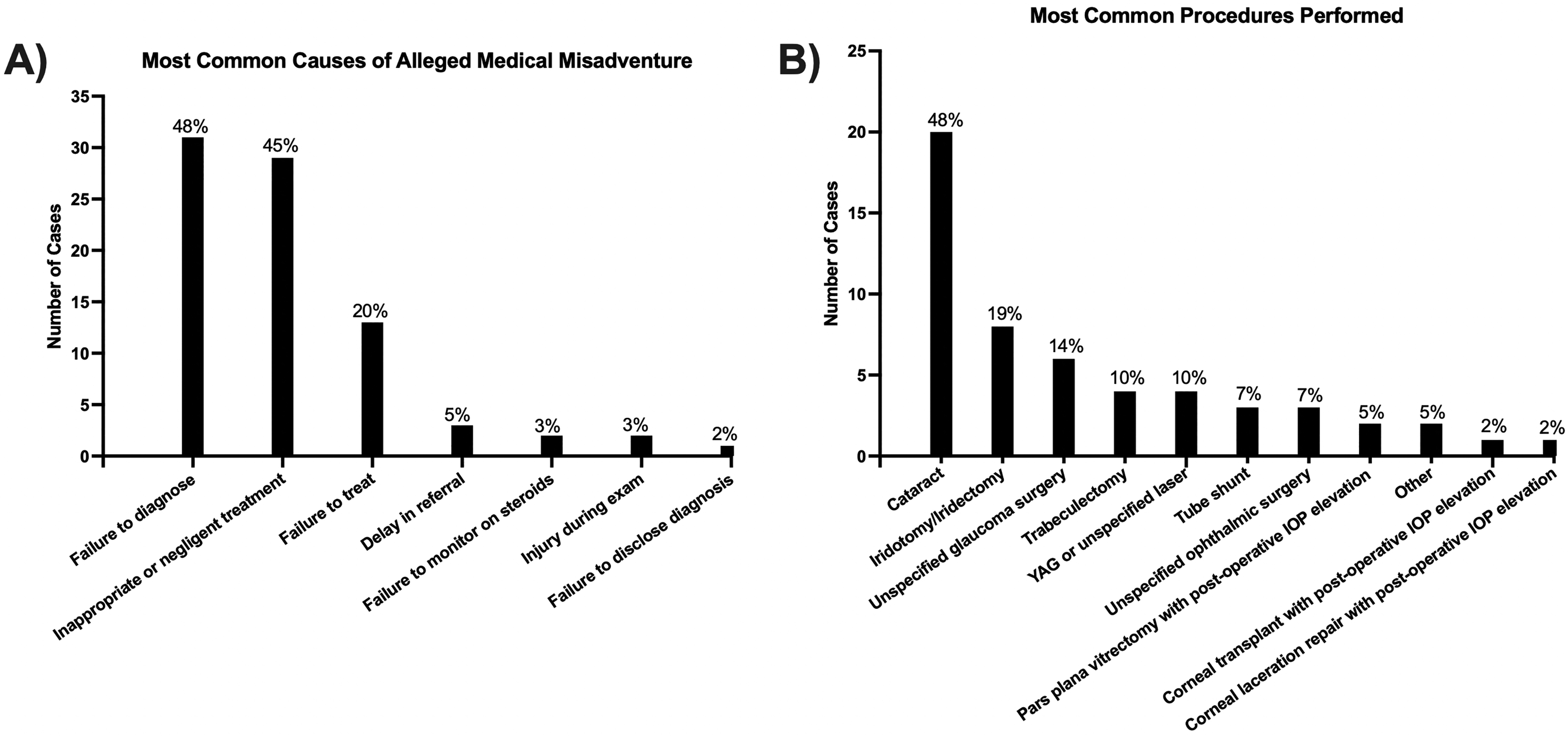
Most common causes of alleged medical misadventure (A) and most common surgical procedures performed in glaucoma-related malpractice litigation (B).
Table 1 outlines glaucoma diagnoses related to medical misadventure and surgical complications with an unspecified type as the most common in both categories (67% and 62%, respectively). However, the surgical treatment group had a higher proportion of angle closure glaucoma (X2 = 9.978, P = 0.002) and secondary glaucoma (X2 = 4.137, P = 0.04) compared to the non-surgical group.
Glaucoma diagnoses of plaintiffs in cases with alleged medical misadventure or a surgical etiology.

Percentages are calculated as number of appearances in cases divided by the number of cases. Only one glaucoma diagnosis was made per case. The category ‘angle closure glaucoma’ includes: acute angle closure and chronic angle closure glaucoma.
Of the 97 allegations involving surgical complications extracted, 42 cases involved surgical treatment with alleged blindness and vision loss in 83% of cases; importantly, some cases noted more than one alleged complication (Table 2).
Most frequently alleged surgical complications in glaucoma-related malpractice litigation.

Abbreviation: IOP (intraocular pressure); Note there may be multiple complications per case. Percentages are calculated as the number of appearances in cases divided by the total number of surgical cases. The “other” category includes complications that did not fall into any of the categories within this table, including: unspecified neurological damage, unspecified injury to the eye, excess lacrimation, and discharge.
Legal analysis
Among the 107 cases that met inclusion criteria, 14 (13%) resulted in favor of the plaintiff and 93 (87%) resulted in favor of the defendant (Figure 3). Forty (37%) cases took place in jury trials, 76 (72%) cases involved appellate ruling, and 68 (64%) cases involved either pre-trial or post-trial rulings. On a party's motion, a court may make a pre-trial determination that there are no material facts in dispute and either the plaintiff or defendant must win as a matter of law. Without pre-trial judgment, the court will proceed to holding a full trial, with the verdict determined either by the judge or jury based on the facts presented and applicable law. Any party may appeal the decision resulting in either a reversal or affirmation of the pre-trial or trial decision. Sixty-six (62%) cases resulted in a defense ruling during a pre-trial motion; 3 (3%) resulted in a defense verdict during an appeal; and 1 (1%) resulted in a defense verdict during a post-trial motion. There was 1 case (1%) that involved a defense verdict during a pre-trial motion that was later reversed in the appeals court. Looking only at trial court decisions, 16 (37%) jury trial cases resulted in a plaintiff verdict during trial court and 25 (40%) resulted in a defense verdict including 3 cases that followed appellate reversals from pre-trial defendant motions.
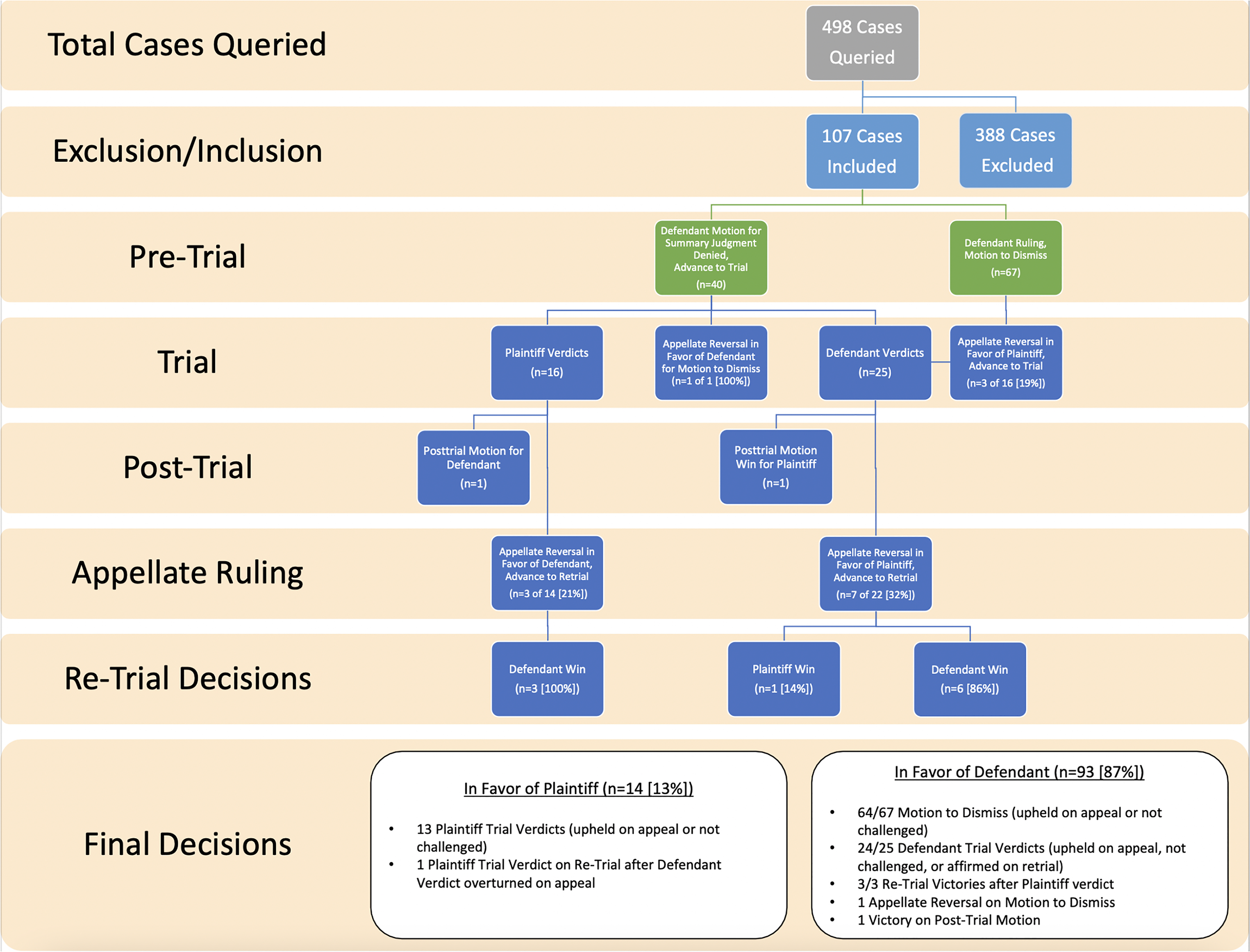
Flow chart demonstrating the progression of legal proceedings and a summary of the outcomes.
Overall awards and settlements
Plaintiffs may receive awards in two different circumstances: (1) a settlement from the defendant to prevent proceeding to trial, or (2) a trial award determined by the jury following a verdict. In total, plaintiffs received awards in 13 cases with a mean value of $613,715 (±$293,393) and median value of $710,286 (range, $117,662–$914,319). Plaintiffs received trial awards in 10 cases with a mean value of $640,701 (±$298,083) and median value of $767,922 (range, $117,662–$914,319). Plaintiffs received settlement awards in 3 cases with a mean value of $523,762 (±$317,579) and median of $635,950 (range, $165,316–$770,021). A defendant received an award in only one case ($8177). The defendant won sanctions against the plaintiff after he was sued for a second time, after the court had already dismissed the prior case with prejudice (signifying that the plaintiff could not sue again).
Medical misadventure
For cases involving medical misadventure, five cases resulted in plaintiff awards with a mean of $595,850 (±$277,994) and median of $635,950 (range, $174,274–$896,946). The most common allegations of medical misadventure within these cases included failure to diagnose (n=4), failure to treat (2), and negligent and inappropriate treatment (2). The diagnosis in all five cases was glaucoma, type unspecified.
Optometrist-only cases
Of the cases featuring optometrists, 20 (77%) involved optometrists only. Among these 20 cases, failure to diagnose (13) was the most common allegation, with negligent treatment (6) as the next most frequently reported. Other reasons for litigation were failure to treat (2), delay in treatment or referral (2) and injury during exam (1). The alleged complications in these cases included progression of glaucoma (15), blindness (4), and progression of glaucoma and blindness (2). Overall, there were 15 defense, 2 plaintiff, and 1 unknown trial verdicts and one case with a defense verdict with partial settlement claims awarded in the 20 optometry-only cases. One plaintiff verdict resulted in a $896,946.68 award with the other plaintiff award value unknown. Two cases were decided pre-trial: 1 defense pre-trial motion win and 1 plaintiff pre-trial motion win. Of the 14 defense trial verdicts, one case involved a partial settlement ($15,827.96). Similarly, 13 of 87 (15%) cases involving at least 1 ophthalmologist resulted in a plaintiff verdict.
Surgical cases
For cases involving a surgical treatment, nine cases resulted in plaintiff awards with a mean of $624,881 (±$320,989) and median of $767,922 (range, $117,662–$914,319). The most common alleged surgical complications within these cases were blindness (n=5), elevated IOP post-operatively (5), and choroidal hemorrhage (2). The most common diagnoses were glaucoma, type unspecified (three) and secondary glaucoma (two). When reviewing specific surgeries, there were three (15%) plaintiff verdicts in cataract surgery cases with a mean award of $884,180.04 (±$609,873.63). Among incisional glaucoma surgeries, one (25%) of four trabeculectomy cases ended with a plaintiff verdict with an unknown settlement amount, all tube shunt surgeries ended with defense verdicts, and one (17%) of six unspecified glaucoma surgeries ended with a plaintiff verdict with an unknown settlement amount. Lastly, four (50%) iridotomy/iridectomy cases ended with a plaintiff verdict and mean award of $682,177.63 (±$589,919.18).
Discussion
This litigation review provides the most in-depth analysis into the legal and clinical features of glaucoma-related malpractice cases through multiple insurers.
Glaucoma-related malpractice litigation has been steadily increasing over time. The greatest increment in glaucoma-related malpractice litigation was between the 1980s and 1990s. It is likely that this increase in glaucoma-related malpractice litigation is a reflection of the increase in national rates of malpractice litigation across all medical specialties with increases from 1.5 claims per 100 covered physicians in 1956 to approximately 15 per 100 in 1990. 10 In cases involving ocular oncology, 11 pediatric ophthalmology, 1 and ophthalmic trauma, 12 75%, 90%, and 95% of litigation cases, respectively, took place after 1980. This parallels trends in glaucoma where litigation cases were more frequent following 1980.
Regardless of the mounting rates of malpractice litigation, based on the high pre-trial dismissal rate and high rate of defendant verdicts relative to the millions of Americans with glaucoma, one may infer that glaucoma patients are receiving a high standard of care. On the other hand, our frequent rulings in favor of defendants (86%) may in part also be due to access to more successful legal counsel, presence of procedural loopholes, breach in standard of care without proof of causation, or statute of limitations due to excess years since the alleged breach in standard of care.
When considering the clinical analysis performed in this study, we believe that we have identified several important points for providers. Firstly, the majority of glaucoma-malpractice litigation was attributed to medical misadventure, as was found by past glaucoma-malpractice studies of single insurers.6, 7 Given that over one-third of alleged medical misadventure was attributed to ‘failure to diagnose’ glaucoma, it is essential that glaucoma patients and glaucoma suspects receive a full workup including a detailed history, a thorough dilated examination, and structural and functional testing. 13 The challenge of detecting glaucoma is follow-up as physicians must stress adherence to follow-up appointments for all patients regardless of degree of glaucoma risk. The second and third most frequent causes of alleged medical misadventure included ‘inappropriate or negligent treatment’, followed by ‘failure to treat’. Similarly, the three most common allegations in cases involving optometrists-only were identical. In contrast, Engelhard et al. studied 69 glaucoma cases between 1962 and 2014 and reported ‘mismanagement’, ‘failure to diagnose’, and ‘drug effect’ were the first, second, and third most common causes of litigation in glaucoma, respectively. 9 This difference may be attributed to the inclusion of cases involving optometrists, the difference in study period, or the larger sample size in our study. Regardless, these findings again emphasize the importance of patient follow-up, adjustment of medical therapy as warranted by patient circumstances and clinical exam, and/or early referral to a glaucoma specialist. There were several cases involving IOP elevation with steroid response; this highlights the importance of judicious use of steroids and monitoring IOP during steroid treatment. These findings are consistent with those of previous glaucoma-malpractice studies, which also listed diagnostic error and failure to treat glaucoma as some of the most common alleged causes of malpractice litigation.6–8
Similar to ophthalmologists, optometrists were also at risk for glaucoma-related litigation with 19% of cases only involving optometric care. Optometrist-only litigation resulted in similar plaintiff verdicts (10%) compared to cases involving at least 1 ophthalmologist (15%). Since the most common causes of alleged medical misadventure in optometrists are identical to those reported overall, the recommendations to avoid litigation for these eye care providers remain the same: a full workup with a detailed history, a thorough dilated examination, structural and functional testing, and stressed adherence to follow-up appointments regardless of degree of glaucoma risk. 13 In addition, early referral to glaucoma specialists for closer monitoring may also benefit the patient as well as prevent future glaucoma-related litigation.
In addition, previous glaucoma-malpractice studies looked only at alleged cause of malpractice litigation in glaucoma-associated surgical cases6, 9; however, we chose to more deeply investigate cases with a surgical etiology by separating cases according to procedure, glaucoma diagnosis, and alleged surgical complication. Upon review of these cases, there appears to be a higher proportion of claims related to non-glaucoma surgeries that result in the development of glaucoma post-operatively rather than complications related to glaucoma surgeries, with cataract surgery representing nearly half of the procedures performed in the cases included in this study. Additionally, elevated post-operative IOP was the second most common alleged surgical complication. This indicates that in addition to preventing injury during glaucoma surgery, it is also critically important that IOP should be carefully monitored and managed following all ophthalmic surgeries. Notably, cataract surgery led to greatest mean settlement among plaintiff-verdict surgical cases, further emphasizing the importance of close monitoring following surgery.
When comparing diagnostic data in cases with a medical versus surgical etiology, cases with alleged medical misadventure had a greater variety of glaucoma diagnoses, and significantly fewer diagnoses of both secondary and angle closure glaucoma than the surgical etiology case group. Within the surgical etiology case group, there were several instances in which a patient who underwent ophthalmic surgery suffered from a complication that resulted in either angle closure glaucoma or secondary glaucoma.
Another finding that we wish to highlight is the high pre-trial dismissal rate of 63%: therefore, a substantial portion of all glaucoma-related malpractice litigation is dismissed before even reaching trial. This indicates that plaintiff's glaucoma-related claims are frequently meritless and not permitted to even reach a jury trial. In terms of litigation strategy, defendants should carefully consider settlement options if they are not able to obtain a pre-trial dismissal.
Both glaucoma specialists and optometrists appear far less frequently in glaucoma-related malpractice litigation than do other ophthalmologists. However, this must be considered in the context that glaucoma specialists are a small fraction of practicing ophthalmologists. For both ophthalmologists and optometrists, the majority of defendants were between 40 and 59 years old (54% and 63%, respectively); this is in line with findings from previous ophthalmology malpractice litigation studies. 5
Our analysis of glaucoma-related malpractice litigation revealed generally consistent payments to plaintiffs in both settlements and awards: excluding outliers, they occurred over a narrow band, with adjusted amounts between $600,000 and $800,000 for settlements and $700,000 and $800,000 for awards, with no payments over a million dollars. It is unsurprising that plaintiffs received larger awards at trial as opposed to in a settlement. There was no significant difference in the mean payment to plaintiffs between cases with alleged medical misadventure versus a surgical etiology; this was also reported by Craven in a previous glaucoma-malpractice litigation study. 6 Only one case with an optometrist as a defendant involved payments to plaintiffs; only one case with a female physician named as a defendant involved payment. Furthermore, the 2015-inflation adjusted mean settlement and mean plaintiff award in Engelhard et al. ($955,988 and $977,476, respectively) was higher compared to our study, 9 which may be due to lower litigation outcomes in optometry cases and/or in the years after their study period.6, 7
Interestingly, our analysis had fewer cases involving overall payments to patients in glaucoma-related malpractice litigation than in other ophthalmology subspecialty-related malpractice litigation, even in those studies that had fewer total cases included.1, 3, 4, 9, 14 This may be due to the difficulty in proving to a court of law that glaucomatous damage is the direct cause of injury to the eye. Malpractice cases in other ophthalmology subspecialties appear to be more straightforward: for example, oculoplastic injuries such as cranial nerve damage or facial deformity are more observable than glaucomatous damage. The more straightforward the diagnosis is, the more likely a verdict in favor of the plaintiff can be made along with a payment to the plaintiff, and this is inherently more challenging in glaucoma-related malpractice litigation.
Overall, it is difficult to predict the occurrence of litigation and it can influence physicians to practice defensive medicine, which may involve unnecessary medications or tests, or unnecessary referrals to hospitals or specialists. 15 Since each malpractice case will be different, suggestions to prevent future occurrences will be case dependent. However, general recommendations to decrease the likelihood of experiencing malpractice litigation may also include social workers to address barriers to care or a committee to review malpractice cases to avoid recurrence.
Through using the WestLaw database, we have been able to acquire information over a wide range of time and from a variety of insurers. However, the weaknesses of our study originate primarily from the inherent limitations of the WestLaw database: though WestLaw has been used in many studies of medical malpractice litigation, it does not provide information regarding out-of-court settlements and dropped cases, only jury verdicts and settlements from federal and state court records.16–19 Previous studies examining glaucoma-related malpractice litigation utilized the databases of individual insurers such as the Ophthalmic Mutual Insurance Company (OMIC) or the Physician Insurers Association of America (PIAA) Data Sharing Project (DSP).5–7 WestLaw may not be representative of all litigation related to glaucoma, which may be why the number of cases and payments included within our study is less (107 claims, with 13% resulting in payment) than that of previous glaucoma-related malpractice litigation studies using insurer databases: the study by Craven involved 194 claims with 30% resulting in payments 6 and the study by Brown et al. involved 207 claims with 23% resulting in payments. 7 In addition, the WestLaw database began as an online resource in 1975, so cases prior to its inception may not reflect all glaucoma cases as some may not have been uploaded at the time of the present study. It has been found that 78% of claims made against physicians of all specialties failed to result in payments to plaintiffs. 2 It is likely that the true total amount of payments to plaintiffs in glaucoma-related malpractice litigation is underrepresented in our study due to cases unavailable in the WestLaw database. Another limitation was the variable level of clinical detail regarding cases, with older cases typically offering less information regarding clinical history or surgical procedures. For these reasons, this study should be viewed as a representation of glaucoma-related malpractice litigation and cannot be used to definitively determine the overall prevalence of glaucoma-related malpractice litigation in the country or the number of suits relative to the number of glaucoma patients, or the prevalence of glaucoma-related malpractice generally. Even with the aforementioned limitations, this review provides an important analysis of litigation trends within an ophthalmology subspecialty that treats one of the leading causes of blindness in the world.
In summary, glaucoma-malpractice litigation is becoming more prevalent, with medical mismanagement alleged in the majority of cases. A minority of cases involved glaucoma specialists; a majority of glaucoma-related cases resulted in favor of the provider. Defendants are frequently successful in obtaining dismissal via pre-trial motions, but the risk of liability increases substantially in cases going to trial.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Review Board at Wills Eye Hospital (Philadelphia, PA, USA) and with the Declaration of Helsinki 1964 and its later amendments or comparable ethical standards. All data in this study are available to the public and no human subjects were involved, therefore the Institutional Review Board of Wills Eye Hospital classified this study as exempt from IRB approval and informed consent.
Financial disclosures
DL has received research support from Allergan, Equinox, Glaukos, Mati, Nicox, Olleyes, and Santan, lecture fees from Glaukos, and consulting fees from Quidel Eye Health. JSM has received research support from AbbVie, Aerie, Equinox, Glaukos, Guardian, Haag Streit, Laboratories Thea, Nicox, Olleyes, Santen and has consulted with AbbVie, Aerie, Avisi, Elios, Glaukos, Haag Streit, MicroOptx, and Olleyes. NNK received research support from AbbVie/Allergan, Guardion Health Services Inc, Equinox, Nicox, Olleyes, Santen, Glaukos, Diopsys, and Aerie, and consulting fees from AbbVie/Allergan (myself, spouse), Regeneron (spouse), Alimera (spouse), and Genentech (spouse). JW, NAM, and MA declare they have no financial disclosures.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix: Summary of Practical Advice to Avoid Litigation

|
Glaucoma patients and glaucoma suspects should receive a full workup including a detailed history, a thorough dilated examination, and ideally structural and functional testing. Emphasis should be placed on the importance of monitoring and adherence to follow-up appointments for all patients regardless of degree of glaucoma risk. Judicious use of steroids and close monitoring of intraocular pressure during prolonged steroid treatment should be considered. It remains important to carefully monitor and manage IOP elevation following all ophthalmic surgeries. Defendants should carefully consider settlement options if they are not able to obtain a pre-trial dismissal since 40% lead to initial verdicts in favor of the plaintiff. Social workers could be involved to manage patient–physician conflict as well as address barriers to care. A committee to review malpractice cases can be helpful to avoid litigation recurrence. |