
Abstract
Background
Off-label outpatient parenteral ketamine programs are expanding, yet rare perisession events requiring urgent escalation of care are difficult to quantify for local risk management. This documentation-based audit estimates denominator-based upper bounds for prespecified onsite escalation-of-care actions; it does not assess efficacy or long-term outcomes.
Methods
Retrospective chart audit of routine outpatient IV/IM ketamine sessions at two anesthesiology clinics in Japan (Nagoya: January 2010–June 2025; Tokyo: December 2024–June 2025). Adults (≥18 years) with ≥1 parenteral session were included. Two clinicians audited each session record for Tier 1 escalation-of-care events from initiation until discharge; session counts were reconciled with operational records. Exact one-sided 95% upper confidence bounds were calculated under zero events.
Results
Among 299 unique adults identified, 296 received ≥1 parenteral session (1985 sessions: IV 1779; IM 206). No Tier 1 events were chart-documented (0/1985), yielding a one-sided 95% upper confidence bound of 0.15% per session (IV 0.17%; IM 1.44%); the patient-level upper bound was 1.01% (0/296). A fall requiring ambulance transport was documented after formal discharge (outside the prespecified onsite perisession observation window).
Conclusions
Over a 15-year program horizon, no Tier 1 escalation-of-care events were chart-documented during the onsite perisession window. Findings provide documentation-based upper bounds for rare, high-acuity onsite events relevant to monitoring and rescue planning, but may underestimate reactions not prompting urgent intervention and harms after discharge.
Introduction
Ketamine is a dissociative anesthetic used in anesthesiology and pain medicine and is increasingly delivered off-label in outpatient settings for heterogeneous clinical presentations.1,2 From a patient-safety and clinical risk management perspective, the most safety-critical perisession harms are those that trigger unplanned escalation-of-care actions (e.g., airway support or emergency transfer), because these events directly determine monitoring intensity, staffing, and rescue readiness. However, controlled studies and many observational series are not designed or powered to quantify rare escalation-of-care events, and real-world documentation practices vary.3–5
A pragmatic governance approach is to audit prespecified escalation-of-care actions within a defined onsite perisession window and to report denominator-based upper bounds rather than over-interpreting “zero events” as proof of zero risk. This approach encourages explicit denominator reconciliation (to avoid undercounting administrations) and supports incident learning for program governance.
We conducted a documentation-based audit of routine outpatient parenteral ketamine administration at two anesthesiology clinics in Japan spanning January 2010 through June 2025. Our primary objective was to estimate upper bounds for prespecified Tier 1 onsite perisession escalation-of-care events (from initiation of administration until discharge). Secondary objectives were to describe utilization patterns and selected programmatic responses relevant to risk management. This audit does not assess treatment efficacy or long-term outcomes.
Methods
Design and setting
We performed a retrospective, documentation-based safety and risk management audit of routine outpatient ketamine administrations at two Japanese outpatient anesthesiology clinics (Nagoya and Tokyo). The audit period was January 2010–June 2025 for Nagoya and December 2024–June 2025 for Tokyo. Ketamine administration was routine clinical care and was not initiated or modified for research purposes. Reporting follows STROBE guidance for observational studies. 6
Participants and session counting
Adults (≥18 years) were eligible if they had at least one documented IV or IM ketamine session during the audit period. A “session” was defined as a single clinic visit with parenteral ketamine administration recorded on a session-level ketamine administration record. Visits without parenteral ketamine (consultation/education only) and oral-only ketamine visits were excluded. Prior to de-identification, patient records were deduplicated across sites by matching patient identifiers (e.g., name and date of birth) with manual review when needed.
To strengthen denominator completeness for risk estimation, the chart-verified IV/IM session count was reconciled against independent operational sources (the controlled-substance ketamine ledger and the Japanese electronic billing system [ORCA]). These sources were used only to confirm session counts and were not used for outcome ascertainment. For the Tier 1 component “unplanned emergency transfer/hospitalization,” we additionally reviewed internal incident and transfer documentation maintained by the clinics for the onsite perisession window.
Routine care context
Ketamine was administered per routine clinical judgment, most commonly as an IV infusion (typically ∼20–60 min) and less commonly as an IM injection. Sessions were conducted under an awake protocol; formal sedation scales were not used. A physician was onsite and standard oxygen and airway/resuscitation equipment was available. In current routine practice, patients are monitored with continuous pulse oximetry during administration; blood pressure is measured at least twice (pretreatment and prior to clearance for ambulation/discharge); safe ambulation is confirmed; and minimum onsite observation targets are at least 30 min after completion of an IV infusion and at least 90 min after an IM injection, with clinician discretion to extend observation as needed. IV infusions were typically delivered without routine adjunctive medications; for IM sessions, oral metoclopramide was routinely used for nausea prophylaxis.
Dose context is provided in the Supplementary Material: among early-session-window administrations with retrievable dose records, recorded IV doses were median 15 mg (IQR 10–28; range 5–70), recorded IM doses were median 60 mg (IQR 47–80; range 22–150), and the overall weight-normalized dose was median 0.31 mg/kg (IQR 0.18–0.50; range 0.05–1.55).
Continuous ECG monitoring was not routinely used; therefore, this audit could not estimate transient or asymptomatic arrhythmias. The Tier 1 arrhythmia endpoint was limited to clinically significant arrhythmia requiring urgent intervention and documented in routine records.
ASA physical status was not routinely assigned in this outpatient awake-protocol setting, and structured comorbidity abstraction was not prespecified or sufficiently consistent across the 15-year documentation archive to support reliable reporting.
Safety endpoint and ascertainment
The primary endpoint was any chart-documented Tier 1 escalation-of-care event occurring during or immediately after a ketamine session within the defined onsite perisession window (from initiation of administration until discharge). A Tier 1 event was defined as any of the following actions, documented in routine clinical records: airway intervention or assisted ventilation (including bag-valve-mask ventilation or endotracheal intubation), cardiopulmonary resuscitation, seizure requiring urgent intervention, anaphylaxis or severe allergic reaction requiring urgent intervention, severe cardiovascular instability requiring urgent rescue treatment (including unplanned rescue antihypertensive treatment for acute severe hypertension, treatment for severe hypotension, or urgent intervention for clinically significant arrhythmia), or unplanned emergency transfer/hospitalization from the outpatient setting.
Ascertainment was documentation-based. Two clinician reviewers (KT and MJ) manually reviewed each session-level ketamine administration record (procedure note and any attached monitoring/vital-sign documentation) and adjudicated potential Tier 1 events by consensus. Absence of documentation does not prove absence of harm. Less severe reactions and outcomes after discharge were not systematically captured through a standardized adverse-event surveillance system and were not abstracted as incidence estimates.3,7
Statistical analysis
Analyses were descriptive. We summarized utilization using counts and medians with interquartile ranges (IQR, interquartile range). For the primary endpoint under zero observed events, we calculated an exact one-sided 95% upper confidence bound (Clopper–Pearson) for the per-session Tier 1 event rate. For context, we also calculated an exact one-sided 95% upper confidence bound at the patient level (≥1 Tier 1 event per patient).
Results
Cohort and utilization
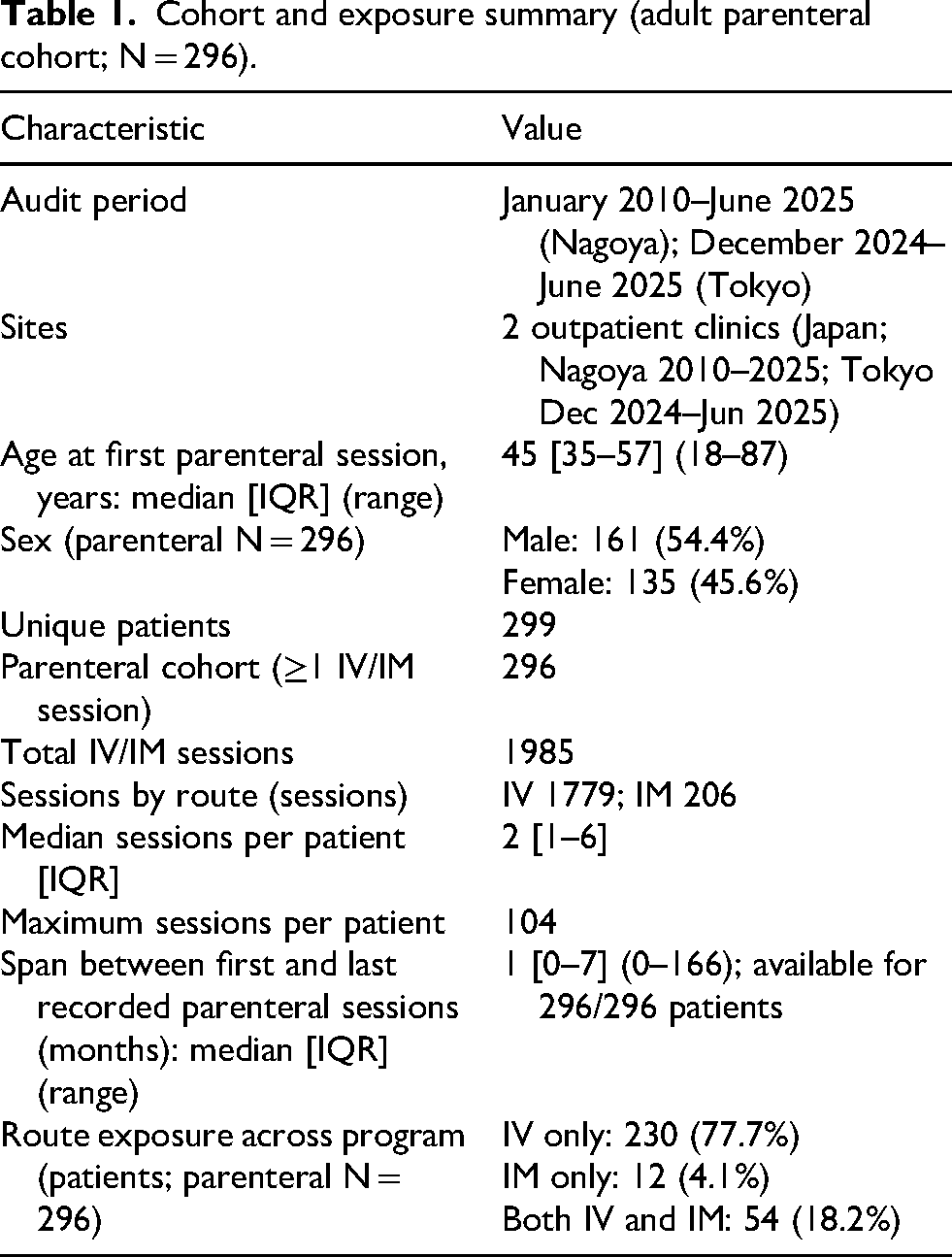
The audit identified 299 unique adult patients, of whom 296 received at least one IV/IM ketamine session and formed the parenteral cohort; three were excluded (oral-only n = 1; consultation/education only n = 2) (Figure 1). A total of 1985 IV/IM sessions were documented (IV 1779; IM 206). The median age at first parenteral session was 45 years (IQR 35–57; range 18–87); 161/296 (54.4%) were male. Exposure was skewed: the median number of sessions per patient was 2 (IQR 1–6), while the maximum was 104 sessions in one patient. The median calendar-month span between first and last recorded parenteral sessions was 1 month (IQR 0–7; range 0–166 months) (Table 1).
Cohort assembly for the chart-based audit (adult primary analysis cohort; excluded from parenteral cohort n = 3: oral-only n = 1; consultation/education only n = 2). Abbreviations: IV: intravenous; IM: intramuscular.
Cohort and exposure summary (adult parenteral cohort; N = 296).
Primary endpoint: Tier 1 onsite perisession escalation-of-care events
No Tier 1 escalation-of-care events were chart-documented during the onsite perisession observation window across 1985 sessions (0/1985), yielding an exact one-sided 95% upper confidence bound of 0.15% per session (Table 2). Route-specific one-sided 95% upper confidence bounds were 0.17% for IV sessions (0/1779) and 1.44% for IM sessions (0/206). At the patient level, no parenteral-cohort patient had a chart-documented Tier 1 event (0/296; one-sided 95% upper confidence bound 1.01% per patient).
Primary endpoint: Tier 1 onsite perisession escalation-of-care events (documentation-based upper bounds).
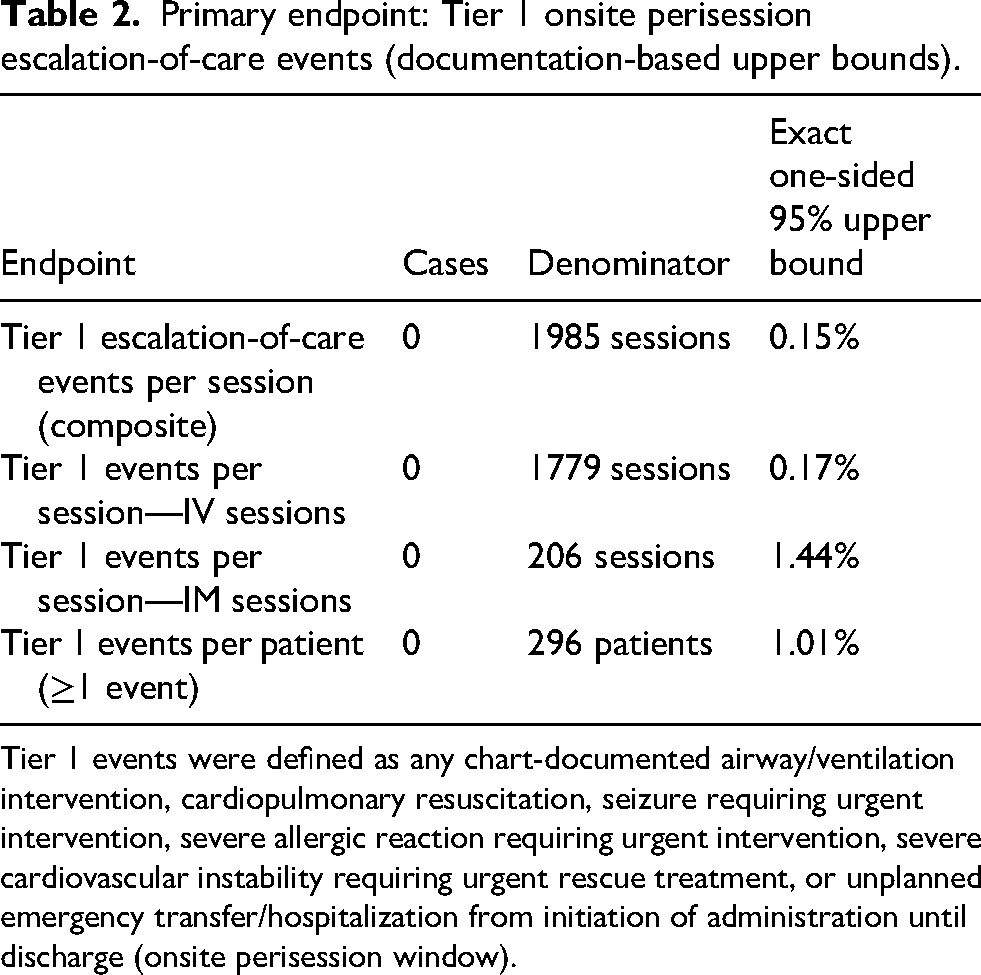
Tier 1 events were defined as any chart-documented airway/ventilation intervention, cardiopulmonary resuscitation, seizure requiring urgent intervention, severe allergic reaction requiring urgent intervention, severe cardiovascular instability requiring urgent rescue treatment, or unplanned emergency transfer/hospitalization from initiation of administration until discharge (onsite perisession window).
Incident learning and programmatic responses (descriptive)
Although this audit did not estimate incidence for less severe or post-discharge outcomes, chart-documented safety signals outside the Tier 1 endpoint informed targeted protocol strengthening as part of routine governance. Examples included reinforcement of discharge readiness checks, minimum observation thresholds, and escort/transport policy after a fall requiring ambulance transport after formal discharge (outside the prespecified onsite perisession observation window), and recommending periodic urologic symptom checks in longer-term courses after urinary frequency was noted in routine documentation (Supplementary Material).
Discussion
In this 15-year outpatient parenteral ketamine program across two Japanese clinics, no Tier 1 escalation-of-care events were chart-documented during the defined onsite perisession window across 1985 adult IV/IM sessions. Under an exact binomial (Clopper–Pearson) model, this corresponds to a one-sided 95% upper confidence bound of 0.15% per session. These estimates should be interpreted as documentation-based upper bounds for high-acuity, high-salience onsite events relevant to outpatient risk management—not as evidence that risk is absent and not as evidence regarding treatment efficacy or long-term outcomes. For patient safety teams and clinical risk managers, these estimates provide denominator-based upper bounds for high-salience onsite events that most directly inform staffing, monitoring, and rescue preparedness.
A key strength of this audit is its explicit focus on escalation-of-care actions that are clinically meaningful and expected to be documented when they occur (airway intervention, resuscitation, urgent treatment for severe instability, or emergency transfer). In addition, we strengthened the session denominator by reconciling chart-verified session counts against independent operational sources and cross-checking internal incident/transfer documentation for unplanned transfers during the onsite window. Together, these steps reduce the risk that “zero events” is driven by denominator undercounting or missed transfers within the defined observation period.
Important limitations remain. First, outcome ascertainment was documentation-based; absence of documentation does not prove absence of harm. Second, we did not systematically abstract less severe but clinically relevant reactions (e.g., nausea/vomiting, oxygen supplementation without airway intervention, agitation requiring rescue medication, or prolonged observation), and therefore cannot estimate their frequency.3,7 Third, postdischarge outcomes were not systematically followed; harms occurring after discharge are likely under-ascertained unless later communicated and documented. Finally, generalizability may be limited to outpatient settings with comparable patient selection, monitoring, and discharge workflows; the Tokyo clinic contributed data only from late 2024 onward. In addition, continuous ECG monitoring was not routinely used, so transient or asymptomatic arrhythmias could not be estimated. ASA physical status and structured comorbidity profiles were not consistently available, limiting assessment of baseline case-mix severity and generalizability to higher-risk populations.
Despite these limitations, the risk management approach used here is transferable. For outpatient ketamine programs and similar ambulatory procedural services, defining a prespecified escalation-of-care composite endpoint, auditing it within a defined onsite window, reconciling denominators, and linking findings to incident learning and protocol strengthening can support pragmatic governance while aligning with general principles for moderate procedural sedation and monitoring.4,5
Conclusions
Across 1985 outpatient IV/IM ketamine sessions delivered to adults over a 15-year program horizon, no Tier 1 escalation-of-care events were chart-documented during the onsite perisession window. These findings provide documentation-based upper bounds for rare, high-consequence onsite events relevant to patient safety and risk management, but they may underestimate less severe reactions and outcomes after discharge.
Supplemental Material
sj-docx-1-cri-10.1177_25160435261466115 - Supplemental material for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan
Supplemental material, sj-docx-1-cri-10.1177_25160435261466115 for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan by Kei Torii and Maho Jinno in Journal of Patient Safety and Risk Management
Supplemental Material
sj-tif-2-cri-10.1177_25160435261466115 - Supplemental material for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan
Supplemental material, sj-tif-2-cri-10.1177_25160435261466115 for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan by Kei Torii and Maho Jinno in Journal of Patient Safety and Risk Management
Supplemental Material
sj-pdf-3-cri-10.1177_25160435261466115 - Supplemental material for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan
Supplemental material, sj-pdf-3-cri-10.1177_25160435261466115 for Chart-documented onsite escalation-of-care during outpatient parenteral ketamine: A 15-year safety and risk management audit of 1985 IV/IM sessions in Japan by Kei Torii and Maho Jinno in Journal of Patient Safety and Risk Management
Footnotes
Acknowledgments
The authors used ChatGPT (OpenAI) to assist with language editing and drafting of portions of this manuscript. All outputs were reviewed and verified by the authors, who take full responsibility for the content. No generative AI tools were used to create or modify study data, analyses, or figures.
Ethical considerations
This study was approved by the Shinkakai Medical Corporation Research Ethics Review Committee (Ministry of Health, Labour and Welfare registration No. 25000131; Approval No. HKK-IRB-2025-002; approval date: 1 September 2025). The committee waived the requirement for individual informed consent and approved an opt-out procedure. Analyses were conducted on de-identified records.
Consent to participate
Informed consent was waived by the ethics committee with an opt-out procedure.
Consent for publication
Not applicable; all data were anonymized and de-identified.
Author contributions
KT conceived the audit, curated data, performed analyses, and drafted the manuscript. MJ contributed to data interpretation and manuscript revision. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KT and MJ are clinicians at the Nagoya and Tokyo Anesthesiology Clinics, which provide ketamine therapy as part of routine clinical services and may derive revenue from such services. These roles represent potential competing interests for both authors.
Data availability
Deidentified data may be made available from the corresponding author on reasonable request, subject to institutional approvals and privacy regulations.
Guarantor
KT is the guarantor of the work. KT accepts full responsibility for the work and the conduct of the audit, had access to the data, and controlled the decision to publish.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.