
Abstract
Children at risk for placement instability are subpopulation in out-of-home care with a critical need for enhanced mental health services, but little is known about the types and adequacy of the mental services they receive. This descriptive study sought to identify the types of mental health services and psychotropic medications provided to children with a risk for moves, foster parents’ perceptions of their adequacy, consistency of therapy services with evidence-based models, and racial and gender differences in service provision. Foster parents completed telephone surveys for a randomly selected sample of 144 children aged 8–14 in specialized or traditional family foster care with a history of placement moves or hospitalizations in a large state in the US. Over two-thirds of children were reported to have mental health diagnoses, with ADHD most frequent (52%). Most children with a diagnosis received psychotherapy (75%) and psychotropic medications (90%). The majority did not receive additional services. A quarter received therapy supporting use of behavioral interventions in foster homes, with 40% of foster parents reporting this was inadequate. Additionally, half reported inadequate initial training. No racial differences in services were reported. However, girls were more likely to receive therapy described as trauma-focused than boys (30.9% and 5.6%, respectively); more boys received treatment for anger (17%) and psychotropic medication (60%). Findings indicate that children at risk for multiple moves receive a high level of services, but questions are raised about the content and adequacy of these services. Evidence-based psychosocial interventions are needed to support positive outcomes and potentially reduce psychotropic medication use.
Keywords
Children who experience multiple moves while in foster care are vulnerable to behavioral disorders, difficulties with executive functioning, attachment issues, and poor physical health (Fisher et al., 2013; Pears et al., 2015; Villodas et al., 2015). Disruptive behavior problems and difficulty forming relationships can then contribute to a cycle of additional moves and other negative placement outcomes. Child welfare systems increase access to assessment, treatment, and respite services (Farmer et al., 2001; Leslie et al., 2005) with the potential to shift these outcomes, but the extent that effective services reach children with the greatest needs and across all racial groups is unclear. Although children with behavior problems are more likely to receive mental health services than other children in care (Burns et al., 2004; Pullmann et al., 2018), placement moves resulting from behavior problems frequently disrupt services provided by both community agencies and schools, potentially leading to gaps in services and undermining effectiveness (Raghavan et al., 2007).
Understanding service patterns for children with a history of moves is critical to create a responsive, effective service system for the most vulnerable children in out-of-home care. This descriptive study addresses this need by examining the types and intensity of different mental health services provided to children with a history of moves, foster parents’ perceptions of the adequacy of mental health services and use of effective service models, and race and gender differences in service provision.
Provision of mental health services in out-of-home care
The majority of children entering substitute care through the child welfare system in the US receive an initial mental health screening, as all states have adopted mandates for universal screening for either behavioral or trauma symptoms at entry into care (Pullman et al., 2018). An estimated 50–70% with a significant mental health need also receive some type of mental health service such as therapy while in out-of-home care (Petrenko et al., 2011; Pullmann et al., 2018; Tarren-Sweeney, 2010). Behavior problems and entry into substitute care predict both referral to services and initiation of services (Fong et al., 2018). While these findings support that placement in out-of-home care facilitates identification of mental health needs and receipt of services, these data potentially mask important variation in the intensity and content of the services provided as well as racial disparities in access. Many children entering foster care receive a single mental health assessment or limited services rather than comprehensive services to address identified needs (Tarren-Sweeney, 2010). Concerns about racial inequities in service provision have also been raised. Latino and African American youth identified with mental health needs appear underserved relative to non-Hispanic white youth (Stein et al., 2016), potentially receiving services less than half as often (Kim & Garcia, 2016).
When screening identifies mental health needs, multiple factors potentially inhibit provision of services and result in unmet needs for many children (Mersky et al., 2020; Petrenko et al., 2011). Demands on a caseworker’s time may limit caseworkers’ ability to address children’s needs beyond basic safety and protection (Hoffman et al., 2016). Caseworkers also frequently lack the training needed to identify the youth’s specific mental health needs and then assist foster families and youth in navigating complex systems of care (Hoffman et al., 2016; Kerns et al., 2014). Accessing services can be an additional barrier. Many treatment providers do not accept Medicaid due to low reimbursement rates and other restrictions related to managed care plans (Raghavan et al., 2007; Schneiderman & Villagrana, 2010), and long wait times for community-based mental health services are common (Kerns et al., 2014).
Providing comprehensive psychosocial mental health services that include foster parent training and support, individual child treatment and adjunctive services such as respite is particularly important to address issues such as behavior problems, risk to others, and difficulties with parenting that predict additional moves (Aarons et al., 2010; Leathers et al., 2019). However, the extent that services reach children who have the greatest need for services and are sustained over time is unknown. Children with frequent moves have more tenuous connections with caregivers, which might result in less caregiver advocacy and involvement in services and more fragmented, less effective services. Alternatively, moves might trigger more comprehensive mental health services than typical among children in foster care and greater system oversight through administrative review processes (see Leathers et al., 2021).
Types of services provided
Identifying the specific types of services provided to high-risk children is important as a range of services could have a role in supporting positive outcomes. For example, schools play a major role in supporting children with mental health needs, with a nationally representative study in the US finding that schools provided counseling to 20% of children with child welfare involvement over an 18-month period, while 30% received services in other settings such as outpatient clinics, inpatient hospital stays, emergency rooms, and day treatment programs (Stein et al., 2016). Additionally, 24% of children received special education services. School-based counseling, classroom-based behavioral supports, tutoring, and group interventions at school could be essential for children in foster care given their significant academic delays (Trout et al., 2008) and the reciprocal effects of school failure and disruptive behavior and negative outcomes in adulthood (Forsman et al., 2016). An unaddressed question is the extent that children at risk for moves receive these services from schools.
Other services potentially provided to children with mental health needs in foster care include respite services, caseworker support to foster parents, and foster parent training to understand the impact of trauma and how to provide behavioral support in their homes. These services can lessen foster parent stress, improve foster parents’ understanding of the needs of the child and effective parenting strategies, and help stabilize placements (Barnett et al., 2019; Frederico at al., 2017; Price et al., 2008; Redding et al., 2000). Although studies of mental health services have tended to focus on psychotherapy services, receipt of these nontraditional services and foster parent perception of their adequacy potentially contributes to negative placement outcomes. For example, in one study, two-thirds of foster parents considering discontinuing as a foster parent said that they had not received enough initial training (Randle et al., 2017). Similarly, in another recent study, foster parents rated children’s behavior problems as their greatest challenge in fostering and identified a need for better parent training and preparation and foster parent support in addition to specialized mental health treatment (Barnett et al., 2018).
Receipt of an enhanced rate to care for a child with significant mental health needs is not a specific mental health service, but also could be a factor supporting placement stability among children at high risk for moves. The higher rates provided in specialized family foster care are typically provided with more intensive caseworker support and other services and also appear to have positive effects on placement outcomes, independently from enhanced services (Chamberlain et al., 1992). Despite the potential benefits of providing specialized foster care with higher care rates, the proportion of youth with a high risk for moves receiving enhanced rates is unknown.
For some children, appropriately prescribed psychotropic medications are also a key component of treatment. For attention deficit hyperactivity disorder, for example, treatment with stimulant medication should be considered for children aged six and older (Pliszka, 2007). While psychosocial interventions such as behavior interventions are helpful reducing medication dosages and improving functioning (Evans et al., 2018), medication is most effective in reducing core symptoms of ADHD such as hyperactivity and inattentiveness (Pelham & Altszuler, 2020). Similarly, early onset schizophrenia and bipolar disorder, when accurately diagnosed in children and adolescents, typically require antipsychotic and mood stabilizers to address core symptoms of these disorders (Bishop & Pavuluri, 2008; McClellan et al., 2007; McClellan & Stock, 2013).
However, significant questions have been raised about a high level of use of psychotropic medication in foster care (Alavi & Calleja, 2012; Cummings, 2012; Daviss et al., 2016). An estimated 18% of children in foster care take one or more medications, a rate 2.7–4.2 times higher than other Medicaid-insured children (US GAO, 2012). Of particular concern are the high rates of use of multiple medications and off-label use of medications such as antipsychotics with potentially serious side effects (Bush et al., 2021). Children with a history of moves in care could be more likely to have mental health disorders requiring medication, but due to their more tenuous connections with caregivers could also be at particularly high risk for questionable prescribing practices. This can include use of polypharmacy prior to trying a single medication, use of two medications of the same class, or use of medications with opposing actions, such as a stimulant and an antipsychotic (Bush et al., 2021). A high risk of these prescribing patterns has been found for children in treatment foster care, who frequently have complex mental health needs and a history of moves, with 22% flagged for questionable polypharmacy (Brenner et al., 2014).
To reduce excessive and inappropriate use of medications, federal legislation in the US has required states to monitor psychotropic medication use among children in foster care since 2011 (see Child and Family Services Improvement and Innovation Act). However, these processes vary widely across states, and many do not involve clinical oversight or prospective consultation prior to prescribing off-label medications and appear to have little effect on medication use (Mackie et al., 2017). Two recent studies also highlight continued issues with prescribing patterns. One found that among children with ADHD receiving state-administered medication review services, 16% received both a stimulant and antipsychotic, with the majority of children prescribed either both at once or the antipsychotic prior to the stimulant, counter to prescribing guidelines (Bush et al., 2021). The second tracked prescribing patterns over time and found that among children prescribed more than one medication and/or an antipsychotic, deprescribing rarely occurred, suggesting that children who begin these medications are unlikely to discontinue them (O’Brien et al., 2020). In the present study, we explored the possibility of excessive or inappropriate use of medications among children with a history of moves by examining the types of medications prescribed for different mental health conditions and use of multiple and off-label medications.
Perceived adequacy and correspondence with evidence-based practices
Other unaddressed questions relate to foster parents’ perceptions of the adequacy of services and the extent that the most effective service models are used in foster care. As noted, foster parent perception of services is important because of the potential for negative service perceptions to contribute to risk for decisions to discontinue with fostering. Gaining an understanding of the extent that services are consistent with evidence-based practice is also critical because evidence-based interventions services are more effective than “services as usual” to treat behavior problems, trauma symptoms, and other mental health issues in both the general population and in foster care (Chamberlain et al., 2008; Cohen et al., 2018; Horwitz et al., 2010; Landsverk et al., 2009; Price et al., 2008). However, multiple factors inhibit the use of evidence-based therapy models, and previous research suggests that most community-based treatment is either not evidenced-based or less intensive than intended by intervention developers (Herschell et al., 2020). Among providers who accept Medicaid and are willing to work with youth in foster care, only a limited number are experienced and trained in evidence-based practices (Hoffman et al., 2016; Kerns et al., 2014).
Difficulties in directly measuring mental health services content has contributed to the lack of information about the degree to which services are evidence-based. However, recent research has pointed to the use of specific quality indicators that provide an accessible method to indicate whether therapy services are consistent with evidence-based models. For example, Barnett et al. (2020) identify caregiver attendance as an easily measured indicator of potential use of an evidence-based treatment for a child whose primary identified issue is externalizing behavior problems or ADHD since caregiver attendance is a required component of evidence-based interventions to treat these disorders (Evans et al., 2018; Steiner et al., 2007). Although caregivers might attend therapy sessions that are inconsistent with evidence-based practices, therapy with children that does not include a caregiver in the sessions the majority of the time is highly unlikely to be an evidence-based treatment. As also noted by Barnett et al. (2020), caregivers’ involvement in services supports more positive treatment outcomes across a range of internalizing childhood mental health issues in addition to externalizing behavior problems. A meta-analysis of cognitive-behavioral intervention studies for internalizing disorders including depression, anxiety, and post-traumatic stress disorder (PTSD) found that caregiver involvement was associated with more positive outcomes at follow-up (Sun et al., 2019), further supporting caregiver attendance as a quality indicator for other types of interventions.
In addition, the structure of evidence-based therapies for externalizing behavior problems and ADHD facilitates measurement of these interventions. The focus on teaching parents to use discrete strategies (e.g., creating a reward chart and learning specific discipline methods) provides the opportunity assess use of these interventions by asking parents if they were taught these strategies in therapy sessions (see Chamberlain et al., 2008; Price et al., 2008). The same parenting strategies are also incorporated into the leading cognitive-behavioral treatment for trauma to address the behavior issues that often accompany trauma symptoms (Cohen et al., 2017). Thus, given the high rates of behavior problems and trauma experiences among children with a history of moves, these active parent training components should be frequently included in treatment of children with disruptive behavior in foster care. By analyzing the extent that these indicators were present in treatment of children with diagnoses of ADHD and disruptive behavior disorders, in particular, we estimated the extent that services were consistent with evidence-based service models for these disorders.
In summary, despite the particular importance of effective services for children with a high risk for moves, no previous studies have examined the types of services provided, use of psychotropic medications, foster parents’ perceptions of service adequacy for specific types of services, indicators of use of effective therapy models for externalizing behavior, or racial and gender differences in service provision among this specific population of children. Addressing these questions is an important step toward building an effective service system. This study focused on these questions by interviewing foster parents caring for a sample of randomly selected children with a high risk for moves in foster care.
Research questions
Because this study was descriptive, no specific hypotheses were defined. Research questions included the following: What types of mental health services are provided to children with a risk for moves, and how do services vary across categories of children with mental health diagnoses and current symptoms? What proportion of children with a history of moves are taking psychotropic medications, and how many are taking multiple or off-label psychotropic medications? What proportion of foster parents report inadequate services across service types, and does this vary for children with mental health diagnoses and current symptoms? What proportion of therapy services provided to children with ADHD and/or behavior problems appear consistent with evidence-based services? Are there racial and gender differences in types of services provided, their adequacy, and the focus of psychotherapy services?
Methods
Study design
This study involved cross-sectional telephone interviews with 144 foster parents who were currently caring for a randomly selected child or young adolescent with a history of moves or prior hospitalization. Mean interview length was 90 minutes. Historical placement data from administrative files were matched with interview data to code children’s placement histories.
Eligibility criteria
Children selected for the study were aged 8 to 14, currently placed in a foster home (traditional, specialized, and kinship), and under state guardianship (rather than temporary custody). Cases were randomly selected from all youth who met study criteria statewide (N = 590). All of the children selected for the study (N = 167) had a history of two or more placement moves after their first 6 months in care, residential placement, or two or more psychiatric hospitalizations. We selected these specific criteria after analyzing historical placement data and finding that these factors significantly increased chances of moving in the next year as compared to children who did not meet any of the criteria. Over 30% of children who met one or more criteria moved to a new foster home or a residential setting in the following year. The response rate was good (86%, N = 144). The most common reason given for decline was not having time for the interview. A university and the state child welfare institutional review boards approved the study protocol, and foster parents received a US$40 gift card for participating.
Measures
Mental health diagnoses and current symptoms
Foster parents provided all mental health diagnoses that the child had received. This information is given to foster parents at the time of placement when a diagnostic interview has previously been completed and after assessments that occur while placed in the home, and foster parents did not typically have any difficulty in recalling diagnoses; just five responded that the child had a diagnosis but they did not remember it. Dichotomous variables coded each diagnosis separately (e.g., 1 for ADHD, 0 for no ADHD). Foster parent report of one or more diagnoses also corresponded to a separate question that asked whether they believed that the child had an emotional or behavioral issue, regardless of whether the child had a diagnosis; 85.4% of those reporting one or more diagnosis also thought that the child had a significant issue. Because of the significant comorbidity in the sample, we also created a variable that coded clusters of diagnoses to differentiate between those with one or more “severe and persistent” or pervasive developmental disorders, those diagnosed with a single disorder, and those diagnosed with ADHD and a disruptive behavior disorder or a trauma-related disorder, including PTSD and reactive attachment disorder (RAD).
Additionally, as both mental health diagnosis and current mental health symptoms are important aspects of children’s current mental health needs, a four-category variable was also created using foster parent report of mental health diagnosis and current emotional and behavior problems. Categories included (1) mental health diagnosis without current clinically significant symptoms, (2) mental health diagnosis with current clinically significant symptoms, (3) no mental health diagnosis or current symptoms, and (4) no mental health diagnosis but with current clinically significant symptoms. Current mental health symptoms were measured using the Ohio Youth Problem, Functioning and Satisfaction Scales (Ogles et al., 1999), a 40-item scale measuring current internalized and externalized child behaviors and current functioning. The developers of the scale report good reliability and validity for the symptom scales (see Ogles et al., 1999 for psychometric properties across multiple studies). In this study, we were able to use results from a statewide study of 3960 children who were beginning therapy services in the same state to identify mean Ohio scale scores in a clinical sample of Medicaid-insured children (Starin et al., 2014). Based on this study’s results, we defined “current symptoms” as behavior problems that were at the mean or higher than in the statewide clinical sample. Those categorized with current symptoms also all had functional impairment, a standard deviation or more than the community mean in Ogles’ and colleagues’ study. Using these criteria, current symptoms were coded dichotomously to create the four-category measure of mental health diagnosis and current symptoms.
Mental health services
The Services for Children and Adolescents–Parent Interview (SCAPI; Jensen et al., 2004) measured therapy or counseling, psychiatric services for medication monitoring, medication, hospitalizations, and school-based services. The SCAPI has been found to have acceptable validity (Jensen et al., 2004) and has been previously used in other studies with foster parents. When scheduling interviews, foster parents were asked to have the bottles of any medications taken by the child available for the interview so they could provide the exact names of medications. Additional project-developed questions following the same format used in the SCAPI measured respite care, caseworker services, foster parent training focused on mental health needs, services to support positive behavior in the child’s classroom, and availability of crisis intervention services. To code receipt of specialized foster care, the child’s placement at the time of the interview was coded from administrative data.
Dichotomous variables were created for each service type. For example, receipt of respite services in past 3 months was coded with a 1 while no use of respite services in the past 3 months was coded with a 0. Similarly, any psychotherapy service in the past 3 months was coded with a 1, and consistent psychotherapy was coded with a one for all children who had had a minimum of nine sessions in the past 3 months. Training at the time of the child’s placement on mental health needs was coded with a 1 for all foster parents who reported more than an hour of training.
Perceived services adequacy
Items assessing perceptions of services were project-developed or adapted from the National Survey of Child and Adolescent Wellbeing, a large nationally representative study that includes interviews with foster parents (U.S. Department of Health and Human Services, 2001). Instead of combining items into a single measure, multiple indicators were used so that variation in service adequacy across different types of services could be examined. Variables included adequacy of initial training provided to address mental health needs, support to address the child’s behavior in the home, help from the caseworker when they spoke about the child’s behavior problems, support and resources provided by the therapist, and support and resources provided by the provider prescribing the child’s psychotropic medication. For example, following the question “Since the start of therapy services, how often has the therapist provided you with any support, education, or resources to help you understand the child’s needs?”, foster parents were asked “Was this adequate, or could you have used more?” Similarly, to measure training adequacy, foster parents rated “I received adequate training to handle my foster child’s mental health needs” on a 5-point scale ranging from very true to not true at all. To provide a clear indicator of inadequate services, responses to each variable were dichotomized, with not adequate or not true responses coded with a 1 and other responses coded with a 0.
Off-label psychotropic use and polypharmacy
To identify the proportion of children who were taking “off-label” medications or one or more psychotropic medications, a cross tabulation for medication type and all diagnoses for each child was examined. All children taking a medication (e.g., an antipsychotic) who did not have a diagnosis for which the medication was approved were coded as positive for off-label use. Children taking two or more psychotropic medications were coded as positive for multiple psychotropic medication use.
Indicators of effective treatment for behavior problems
Foster parents were asked how many of the child’s therapy sessions they had attended in the past 12 weeks. Foster parents tended to participate in therapy for 50% or more of the sessions or not at all, so participation in therapy was coded as a dichotomous variable (1 = attended 50% or more; 0 = less than 50%). This indicator is likely to have low sensitivity, as some foster parents attend therapy sessions that do not follow evidence-based guidelines. However, lack of participation in therapy sessions is likely to suggest use of child-focused interventions that are less effective, particularly for behavior problems, which require extensive caregiver involvement for effective treatment.
Behavioral parent training with foster parents was measured with three items that assessed distinct common components of behavioral parenting therapy, including (1) How often has the therapist talked with you about using a behavior or incentive chart to address the child’s behavior issues? (2) How about talking with you on ways to discipline, like how to use time out or privilege removal? and (3) How often has the therapist provided you with any training on how to work with the child in your home? Responses on four-point scale ranged from never to often. Foster parents had no difficulty responding to the questions, with none replying that they did not know. The items were moderately to strongly correlated, but rather than combine the items into a single measure, each item was dichotomized and then analyzed separately. Responses were coded so those receiving the training often were coded with a 1 and those replying at times or less often were coded with a 0.
Therapy focus
For all children enrolled in therapy, foster parents were asked what the focus on the child’s therapy was in an open-ended question. Responses were coded into a categorical variable that included issues such as behavior problems, aggression, trauma, placement issues, and depression and anxiety. Coding accuracy was confirmed by a second coder.
Demographic and control variables
Foster parents provided their demographic information and years foster parenting in the interviews. For children, demographic and control variables were coded from administrative data, including sex (female = 1, male = 0); race (African American/multiracial African American = 1, white/other race = 0); time in foster care; time in the foster home; age; and number of prior placements. Number of placements included a count of all placements with a new foster parent, residential placements, and group home placements. Hospitalizations, shelter stays, and runaway episodes were not counted, as these experiences are short-term events and are not typically viewed as placements.
Statistical analyses
Following descriptive analyses, cross tabulations with chi-square tests were used to identify the proportion of children receiving different types of mental health services across four groups of children, including those with (1) a mental health diagnoses but no current symptoms, (2) a mental health diagnosis and current symptoms, (3) no mental health diagnosis and no current symptoms, and (4) no mental health diagnosis but with current symptoms. We then analyzed the proportion of foster parents who thought services of different types were inadequate across the four diagnostic categories. Cross tabulations were then used to identify the percentage of children with disruptive behavior diagnoses or ADHD whose therapy appeared consistent with evidence-based practice. Chi-square statistics were used to identify statistically significant differences, followed by Bonferroni-adjusted post-hoc tests to identify the specific categories that were different. Despite the small number of children who did not have a mental health diagnosis but did have current symptoms, this group is retained in the analyses as the descriptive results suggest some trends that could help inform future studies.
We then examined racial and gender differences in service provision, medication use, and therapy focus across race (African American or multiracial African American compared to white and other) and gender using t-tests and chi-square tests. Because few children were Latino, reflecting the broader foster care population in the state, ethnic differences (e.g., Latino/non-Latino) could not be examined. Descriptive and bivariate results are of particular interest in this study given its focus on identifying the types of mental health needs and services provided within different groups. However, because some gender differences in types of mental health needs as well as services were found, we also conducted a post-hoc multivariate logistic regression analysis of medication use to understand whether the gender difference found was explained by gender differences in mental health needs.
Results
Descriptive outcomes
Sample characteristics and mental health diagnoses
Child and foster parent characteristics.
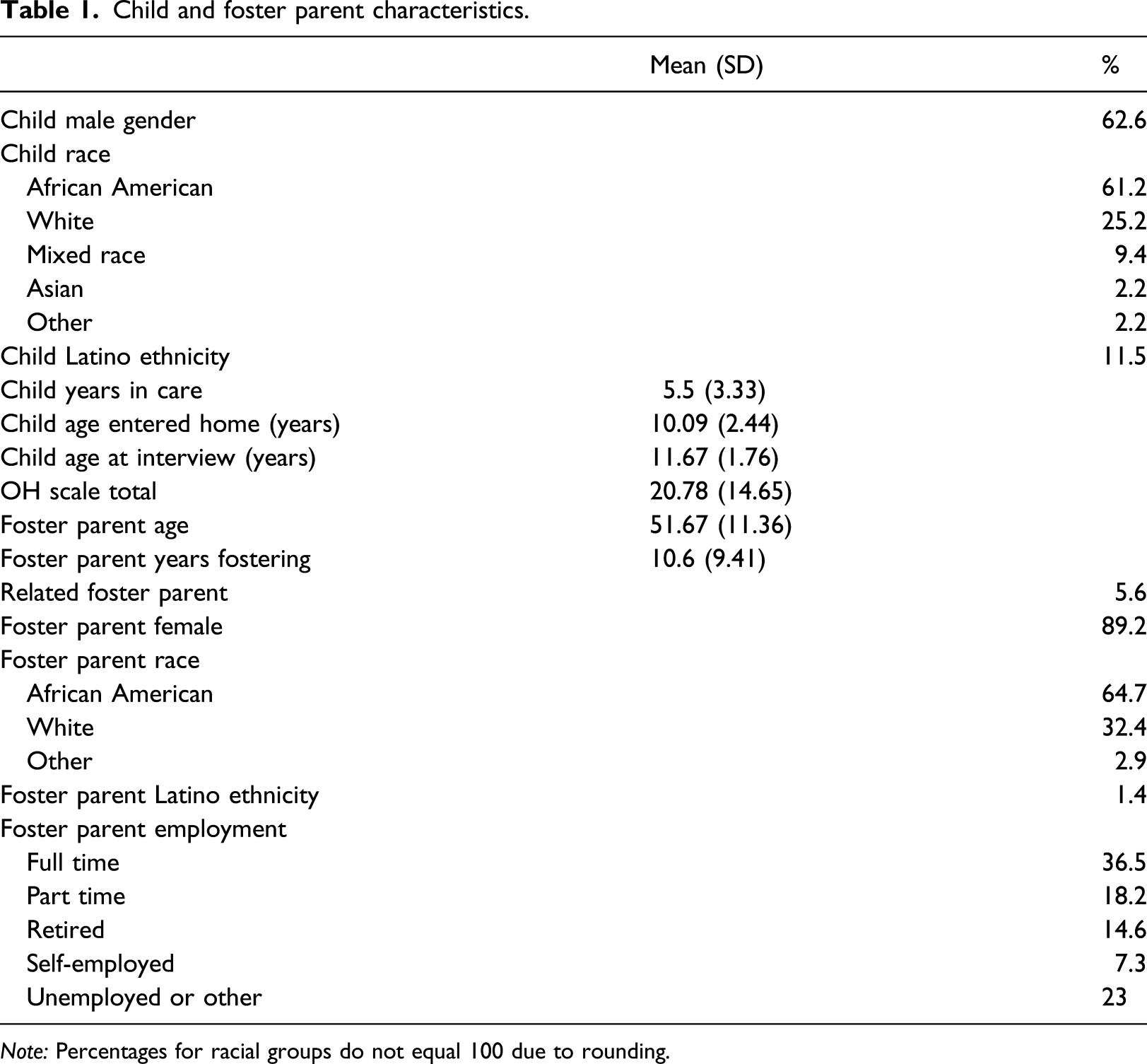
Note: Percentages for racial groups do not equal 100 due to rounding.
Mental health diagnoses reported by foster parents.
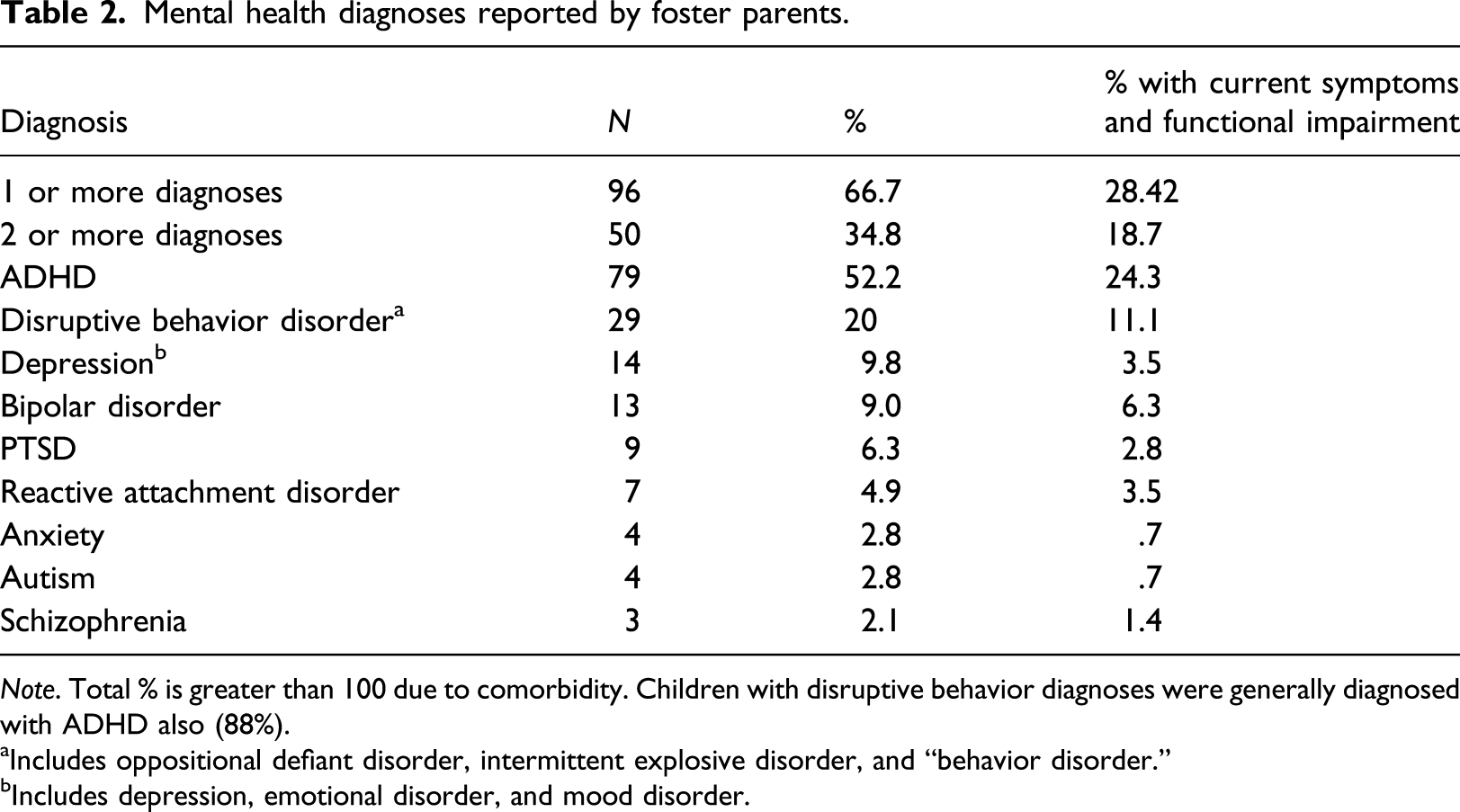
Note. Total % is greater than 100 due to comorbidity. Children with disruptive behavior diagnoses were generally diagnosed with ADHD also (88%).
aIncludes oppositional defiant disorder, intermittent explosive disorder, and “behavior disorder.”
bIncludes depression, emotional disorder, and mood disorder.
Mental health services provided across mental health groups
Services provided across mental health and current symptoms categories.
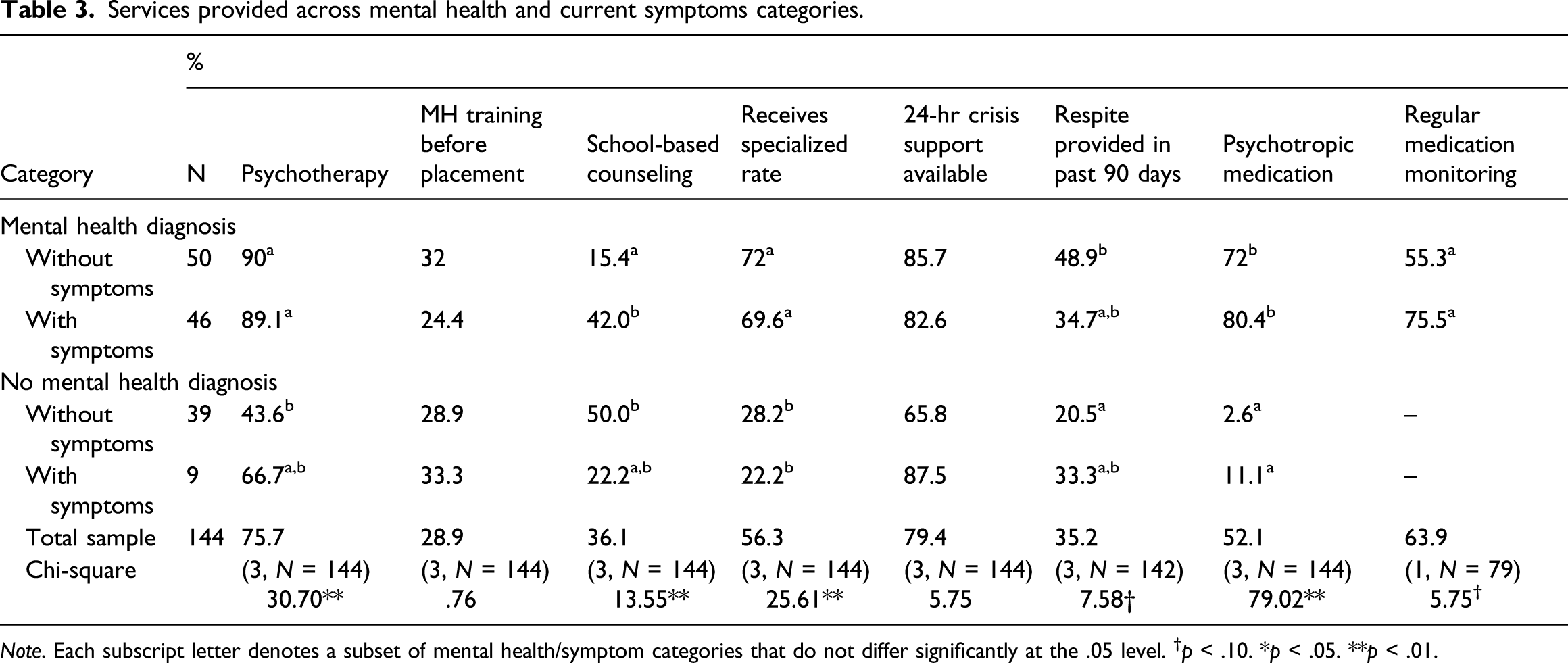
Note. Each subscript letter denotes a subset of mental health/symptom categories that do not differ significantly at the .05 level. †p < .10. *p < .05. **p < .01.
Services less frequently provided included respite care and training on how to meet the child’s mental health needs prior to placement. Most foster parents did not receive these services, and the level received did not vary across the diagnosis and symptom groups. While the group of children who had symptoms but did not have a diagnosis is very small (n = 9, 6.3%), this group is of interest as they appeared to have lower service provision in some areas. In particular, as shown in Table 3, they were less likely to receive a specialized rate and psychotropic medication than children with a diagnosis with or without current symptoms.
Foster parents reported that over a third of children currently had an Individual Education Plan (IEP) at school due to ADHD, behavior issues, or emotional disturbance. Over a third (36%) of children received school-based counseling, with those with mental health diagnoses more likely than those without diagnoses to receive counseling (Table 3). Most children receiving school-based counseling were also receiving counseling outside of school, with just 9 children (6.3%) only receiving counseling at school.
Psychotropic medication types, polypharmacy, and off-label use
Psychotropic medications prescribed within diagnostic categories.

Note. One child with ADHD and a disruptive behavior disorder also took an anti-anxiety medication. This was the only anti-anxiety medication prescribed.
aIncludes children with ADHD and a disruptive behavior disorder (e.g., oppositional defiant disorder). Does not include children with bipolar, schizophrenia, or autism or children with PTSD/RAD diagnoses.
bIncludes children with bipolar, schizophrenia, or autism. All have comorbid diagnoses.
cIncludes children with PTSD or RAD; all have comorbidity, with 12 also reported to have ADHD.
To understand the types of medications prescribed to children with different clusters of diagnoses, the diagnostic categories in Table 4 prioritize the child’s most severe diagnosis and separate children with ADHD into different categories based on comorbidity. Categories include (1) ADHD alone; (2) ADHD with a disruptive behavior diagnosis; (3) severe and persistent disorders (bipolar, schizophrenia, and autism); (4) complex PTSD and RAD; (5) behavior disorders without ADHD; and (6) depression or anxiety without comorbidity. Most children in groups 3 and 4 had comorbidity including ADHD. To understand whether the ADHD-only group was different from the ADHD/disruptive behavior and other groups, total behavior scores from the Ohio scales were compared across groups. As shown in Table 4, those with ADHD alone reported had lower behavior scores than those with ADHD and disruptive behavior, a severe and persistent disorder, or PTSD/RAD.
Consistent with the high percentage of children with ADHD diagnoses, ADHD medications were most frequently prescribed, with the majority who took medication receiving an ADHD medication, and 43.1% of the overall sample taking either a stimulant or non-stimulant ADHD medication (56 and 18 children, respectively). Although the majority of children with different categories of diagnoses took medication, the proportion varied across the categories (Table 4).
Additionally, 20.1% of the sample was currently taking an atypical or “second-generation” antipsychotic such as risperidone. Most antipsychotics were prescribed off-label, with atypical antipsychotics prescribed to 11.4% of children with ADHD without another disorder, 44.4% of children with ADHD and a disruptive behavior disorder, and 28.6% with complex PTSD/RAD. Overall, 20 children who did not have psychosis or bipolar disorder were taking an antipsychotic and 5 took a mood stabilizer, representing 13.8% and 3.4% of the sample. Additionally, 15 children (10.4%) with behavior problems or ADHD without a diagnosis of depression were taking an antidepressant not approved for ADHD treatment. Because seven children took two or more off-label medications, the total number taking an off-label medication was 33 (22.9%).
The diagnostic categories in Table 4 prioritize the child’s most severe diagnosis and provide an indication of the level of comorbidity in the sample, but obscure the extent that individual disorders are treated with corresponding psychotropic medications. Examining medication use within each diagnosis separately indicates a high level of medication use corresponding to individual diagnoses for ADHD, schizophrenia, and bipolar disorder. When examining all children across diagnostic clusters who had ADHD (n = 78), 83% were taking an ADHD medication; for schizophrenia (n = 3), all three were taking an antipsychotic; and for bipolar disorder (n = 13), 53.8% were taking an atypical antipsychotic (also approved to treat bipolar disorder) and one (16.7%) was taking a mood stabilizer. Additionally, a high proportion of children with disruptive behavior disorders (n = 32, most of whom had comorbidity) were taking medication (94%).
Focus of psychotherapy services and indicators of evidence-based services
Psychotherapy characteristics: indicators of evidence-based treatment of behavior problems (N = 109).

*p < .05.
When foster parents were asked in an open-ended question what the child’s therapy was currently focused on, they were most likely to report externalizing behavior including behavior problems, anger, and ADHD (38%, 11.1%, and 6.5%, respectively). Trauma was identified as a focus for 20.2% and placement issues for 17.6%. Fewer were reported to be focusing on attachment issues (7.3%) or anxiety or depression (2.8% for each). No differences in the frequency or characteristics of therapy services, including training behavioral interventions, were found across these areas of focus.
Perceived adequacy of mental health services
Services adequacy across mental health and current symptoms categories.
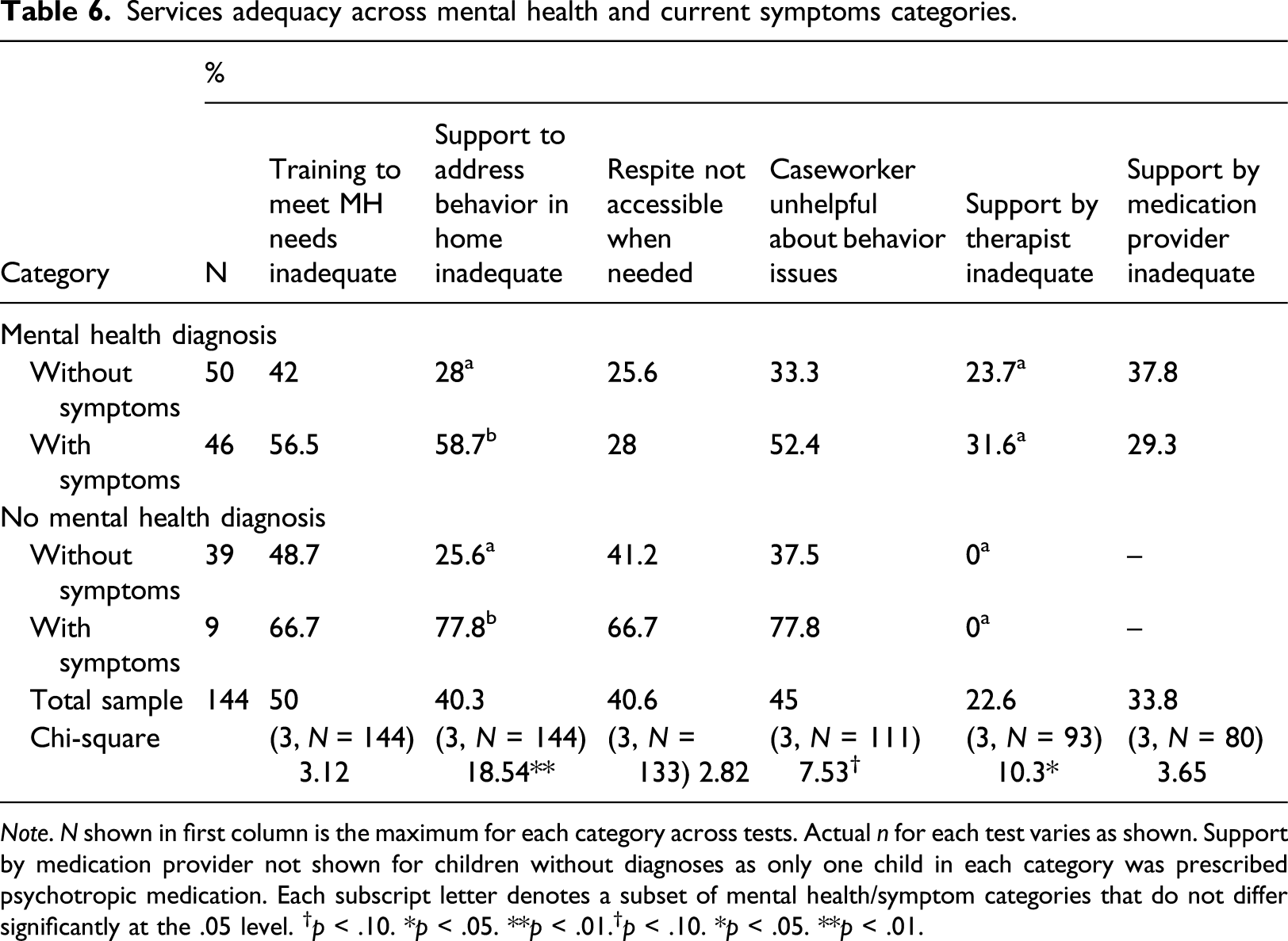
Note. N shown in first column is the maximum for each category across tests. Actual n for each test varies as shown. Support by medication provider not shown for children without diagnoses as only one child in each category was prescribed psychotropic medication. Each subscript letter denotes a subset of mental health/symptom categories that do not differ significantly at the .05 level. †p < .10. *p < .05. **p < .01.†p < .10. *p < .05. **p < .01.
Support to address behavior in the home was also reported to be inadequate for 40% of the sample, with inadequate support significantly more frequently reported when children had current symptoms (for those with diagnoses, 58.7%, and for those without diagnoses, 77.8%). Support and resources provided by the therapist were viewed more favorably, especially for those caring for children without diagnoses. About a quarter of those foster parents of children with mental health diagnoses reported inadequate therapist support, while none of those without diagnoses reported inadequate support. Support provided by the child’s psychotropic medication prescriber was described as inadequate by a third of foster parents with no difference for those with and without diagnoses.
Gender and racial differences in mental health services
Services provided across gender and race.

†p < .10. *p < .05. **p < .01.
Discussion
Types of mental health needs
This study sought to understand the types of mental health services provided to a distinct, identifiable group of children with a risk for instability in foster care due to their histories of prior moves or hospitalizations. Consistent with the findings from previous studies of children with multiple moves (Villodas et al., 2015), many children had complex mental health issues. Two-thirds had one or more mental health diagnoses, and over a third had two or more diagnoses. Rates of ADHD diagnosis were particularly high, with over half (52%) of all children reported to have ADHD, while disruptive behavior diagnoses (e.g., oppositional defiant and conduct disorder) were reported for 20%. Although we did not anticipate the predominance of ADHD diagnoses, previous studies suggest that 15%–20% of youth in foster care have a diagnosis of ADHD (Garland et al., 2001; McMillen et al., 2005; White et al., 2007). Similarly, a national study suggests that ADHD is the most commonly diagnosed disorder in foster care, affecting 22% of children (Turney & Wildeman, 2016), while rates of disruptive behavior disorders are nearly as high at 17.5%.
Mental health diagnoses are unlikely to adequately capture the complexity of the mental health needs of children in care given their histories of trauma and disrupted caregiving both prior to placement and while in care (Tarren-Sweeny, 2010). However, the high prevalence of ADHD diagnoses in this random sample of children with a history of moves suggests that ADHD-types of symptoms could pose a unique risk for placement instability, either directly or through associated relational difficulties. The impulsivity and hyperactivity that frequently characterizes ADHD can impose a considerable burden on caregivers, disrupting families’ routines and requiring considerable adjustments on the part of both parents and schools (Davis et al., 2012; Raggi & Chronis, 2006). Findings from a study in which foster parents reported children’s most challenging behaviors is consistent with this, with the executive functioning deficits that are a core characteristic of ADHD found account for the greatest proportion of variance in the behaviors described as challenging (Octoman et al., 2014). Although studies in the general population indicate a high level of genetic transmissibility of ADHD (Nyman et al., 2007), for children in foster care the impact of trauma experiences as well as poverty could also be strongly intertwined with this symptomatology (Webb, 2013). Research has demonstrated associations between early traumatic experiences and ADHD as well as physiological differences in brain structure that are associated with early adverse experiences and ADHD diagnoses (Humphreys et al., 2019). An important question is the extent that the potential etiological differences of ADHD in foster care and the general population affects the effectiveness of treatments developed in the general population for children in foster care.
Mental health service provision
An encouraging finding from this study is that children with mental health diagnoses received a high level of services, particularly individual therapy services. Overall, 75% of children received psychotherapy in the past 3 months, and 70% of these children had attended sessions regularly. These services were targeted to those with greater need, with 9 out of 10 children with a mental health diagnosis receiving psychotherapy. Schools also provided additional services, particularly for children with diagnoses who had current symptoms, with half of these children receiving school-based counseling. The strong association between diagnosis and therapy might not mean that this high percentage of children with a need were served since diagnostic assessments typically occur prior to initiation of services. However, in this study just 6.3% of children had clinically significant symptoms but did not have a diagnosis, suggesting that diagnosis captured the majority of children with significant mental health issues.
In comparison, 61% of children in the general population whose parents report a mental health diagnosis are estimated to receive services (Lu, 2017). The higher level of services in this study also compare favorably to other older studies of children in foster care, which suggested that about half of children with significant behavior problems receive some type of additional mental health service (Leslie et al., 2005). In this study, most children in services also received them consistently. A history of moves frequently triggers additional service planning (Leathers et al., 2021), and, for 56% of this sample, a move to specialized foster care, which supports a higher level of services. Although this study did not assess changes in mental health needs over time, at the time of the survey less than half of those with diagnoses currently had elevated behavior problems accompanied by functional impairment (28%). This suggests that about half of children in services now had positive functioning, while over one in four in the overall sample continued to have significant needs.
Foster parents’ perceptions of service adequacy
A less encouraging result than the high proportion receiving services is the high percentage of foster parents who reported that the mental health services provided were inadequate. Initial training has been identified as particularly important for foster parents who will care for children with challenging behavior, and need for more training is associated with decisions to discontinue fostering (Randle et al., 2017). Our results suggest that more training is critically needed. Training on how to address children’s mental health needs frequently did not occur, with 60% reporting they had received no training at all, and 28.8% reporting that they had received more than an hour of training. Support and training in how to address behavior problems after placement was viewed as particularly inadequate, with 40% of the entire sample and over half of those caring for children with current symptoms reporting that they did not have enough support to address behavior problems that occurred in the foster home.
Consistency of therapy services with evidence-based practices
Foster parents’ report of inadequate support in how to address behavior problems is consistent with the child-focused services typically provided. Although a high percentage of children received therapy, regular foster parent participation occurred for only a third of families. This finding is concerning as it indicates that therapy providers were not generally using evidence-based treatments or focusing on the parenting difficulties that can proceed placement disruptions (Leathers et al., 2019). Parenting-focused interventions are the primary evidence-based psychosocial treatment for both externalizing behavior and ADHD (Evans et al., 2018; Price et al., 2008) and caregiver participation is required to provide these interventions. Additionally, even for the issues less frequently reported by foster parents as a focus of services, such as trauma symptoms, depression, and anxiety, caregiver involvement is associated with more positive treatment outcomes (Sun et al., 2019). Furthermore, participation in sessions did not always involve direct support of the foster parent to learn and use evidence-based parenting strategies to address behavior problems in the foster home. Just a quarter of foster parents whose child was in therapy reported consistent therapist training, support, and resources, with similar proportions reporting consistent training in specific behavioral strategies such as use of a behavior chart or discipline strategies. Notably, a focus on foster parent training and support was no higher for children with current symptoms than for those without current symptoms.
Psychotropic medication use
Use of psychotropic medications was high, with 52% of the sample currently taking one or more of these medications, as compared to an estimate of 18% in foster care overall (US GAO, 2012). Significantly more boys (nearly 60%) were taking medication than girls (40%), consistent with findings from other studies (Bush et al., 2021; Leslie et al., 2011). These rates indicate that medication may be prescribed at particularly high levels to children with a history of moves, especially boys, who are more likely to have disruptive behavior and ADHD. On one hand, psychotropic use is an indicator of evidence-based treatment of some disorders, including ADHD, which typically requires use of an ADHD medication to address the core symptoms of the disorder in elementary school-aged and older children. The moves experienced by children in this sample appeared to have triggered full assessments and strong access to psychiatric care; 83% of children with ADHD diagnoses were currently taking an ADHD medication. However, 29.2% of the sample was taking two or more medications and 13.8% who did not have schizophrenia or bipolar disorder were taking an off-label antipsychotic medication. The use of multiple medications and off-label use of antipsychotics raises questions given the tendency for prescribers to continue medications over time rather than use them for short periods (O’Brien et al., 2020) and the low level of behavioral interventions provided. Could off-label prescriptions and multiple medications be reduced by providing additional psychosocial interventions with established effectiveness for disruptive behavior?
Findings from the general population suggest that this could be the case. Results from Multimodal Treatment Study of ADHD, a large, controlled intervention study found that combining a range of behavioral interventions with stimulants provided broader benefits than stimulants alone and for some children reduced medication dosages (Pelham & Altszuler, 2020). Notably, this study managed symptoms without adjunctive use of additional medications such as off-label use of antipsychotic medications. Benefits in areas such parent–child relationship difficulties and oppositional behavior are particularly relevant, as these behavioral issues are likely to lead to adjunctive use of an antipsychotic medication (Daviss et al., 2016). Although it could be argued that children’s trauma histories complicate their treatment needs and could require use of more medications than in the general population, concerns have been raised about the child welfare system resorting to more easily administered solutions like medication over more time-consuming, long-term supports to address mental health needs (Alavi & Calleja, 2012). Administering medication is also reimbursed at higher Medicaid rates than therapeutic interventions, potentially incentivizing use of off-label medications over expensive initiatives to increase assess to evidence-based therapeutic interventions. Counteracting these incentives is possible; most of the 10 states that have implemented prior authorization programs for Medicaid-insured children and have data available appear have reduced pediatric use of antipsychotic medications (Mackie et al., 2021). Although this indicates potential for these types of programs to reduce unneeded use, given the potential harms associated with the use of multiple and off-label medications, the child welfare system also has an obligation to invest in evidence-based psychosocial interventions to address the behavioral needs leading to use of these medications.
Race and gender differences in service provision
This study did not replicate racial disparities in service provision reported in previous studies (Kim & Garcia, 2016). Moves might trigger assessment and service planning processes resulting in a higher level of services across all groups, diminishing racial inequities. Some of the racial disparities reported in earlier studies might also have diminished or vary across different systems. In contrast, significant gender differences in foster parents’ reports of the child’s focus in therapy were found. Trauma was the focus of therapy services for three in 10 girls but only 1 in 20 boys. Boys may have more externalizing expression of traumatic stress, which could mask the role of trauma in their symptoms. Understanding gender differences in the effects of trauma experiences, subsequent symptoms, and treatment is important to ensure that the role of trauma experiences in symptom presentation are not overlooked in boys. Boys were significantly more likely than girls to be focusing on anger issues in therapy and, as noted, also more likely to be taking a psychotropic medication, including off-label medications. Evidence-based interventions for both trauma and behavior problems could be particularly important to reduce these gender differences.
Limitations and future research
In-depth assessment of specific mental health issues and inclusion of a trauma scale and more comprehensive checklists to measure ADHD and attachment-related symptoms would significantly strengthen this study’s methods. Despite the high correspondence between ADHD medications and ADHD diagnosis, the high number of ADHD diagnoses could be the result of prior misdiagnosis or use of this label for a more complex range of symptoms, including attachment difficulties and trauma-related symptoms. Trauma symptoms such as difficulty staying present and dissociation could potentially lead to misdiagnosis of ADHD among children with histories of trauma (Szymanski et al., 2011). If this is the case, treatment of trauma could lessen these symptoms more effectively than an ADHD treatment. Alternatively, ADHD might be increased by trauma due to the effects of these experiences on children’s neurological and endocrine systems, resulting in a disorder that is potentially responsive to an ADHD-specific treatment. Additional research is needed to understand the nature of these types of needs and effective treatments.
The cross-sectional design of this study limited our ability to address questions related to changes occurring over time or the relative importance of service perceptions and adequacy at different points in the placement trajectory. Service provision at the point of initial placement or immediately after a child is diagnosed with a mental health need could be particularly important, for example. Foster parents who are unable to tolerate particular behaviors or felt particularly unsupported earlier in the placement might end a placement after a short period and so would be less likely to be selected in a cross-sectional study. A cohort study that followed placement moves prospectively would provide a clearer understanding of service needs and the consequences of inadequate services.
We focused on a narrow range of interventions by examining the extent that foster parents reported that therapists provided parent training in behavioral parenting interventions. This choice was based on the level of empirical support for behavioral intervention for children with behavioral issues in foster care, but our assumption that these types of interventions would improve outcomes for the majority of children in this population could be incorrect. Interventions with a different theoretical basis are important to further develop and study for children in care given their complex family and placement histories. It is also unclear whether therapists who provided training in these areas were using an evidence-based protocol so our estimates of use of these interventions could be inflated.
Our relatively small sample size also presents a limitation that was apparent in the small number of children in some important categories, such as those with significant emotional and behavioral issues who had not been diagnosed with a mental health disorder. We did not anticipate that so few children would have significant needs that were unidentified. These children appeared to be underserved relative to children who had diagnoses, including those who did not currently have significant symptoms, but we did not have enough children in this category to explore this. Similarly, very few children had primarily internalizing mental health disorders, possibly due to the predominance of externalizing symptoms in children with multiple moves. Additional research with larger samples is needed to better understand the needs of these subgroups.
Finally, despite the long length of the interview, information was incomplete in several areas. In addition to more comprehensive measures of children’s mental health issues, use of longer, validated measures in some areas would increase confidence in the findings. More information about school-based services, coordination of care, and supports foster parents seek out such as online support groups is needed. These services could play a key role in supporting both children and foster families.
Conclusions
Results from this study suggest that children in care who have a history of moves receive a high level of psychotherapy services. Nearly all with a mental health diagnosis were currently receiving therapy services. However, although over half received a higher rate to provide specialized care, they were much less likely to receive other services focused on supporting foster parents, such as respite services, training prior to placement, and caseworker support with how behavior problems can be addressed in the foster home. Additionally, just a quarter of foster parents reported receiving therapy services that supported behavioral interventions in their homes, despite the predominance of ADHD and externalizing behavior problems, indicating a low level of use of evidence-based interventions. Given the high risk for additional moves among children with a history of moves and the high levels of psychotropic medication use in the sample, future work is needed to understand the benefits of more comprehensive foster parent support and use of evidence-based interventions.
Footnotes
Author’s note
Sonya J. Leathers, Beth L. Vande Voort, and Catherine Melka-Kaffer are at the University of Illinois at Chicago.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Illinois Department of Children and Family Services (DCFSs). The views expressed in this paper solely reflect the views of the authors and do not necessarily reflect the views of DCFS.