
Abstract
Background
In contrast to existing evidence focusing on high-income countries, this study offers novel insights into the demographic and geographical context that have yet to be explored in the existing literature. Comparatively, in Pakistan, cognitive impairment is one of the neglected disorders that can develop into dementia and Alzheimer's disease. As no treatment is available, lifestyle modifications are a valid intervention for cognitive health.
Objective
This study aimed to assess the relationship between physical functionality, adherence to the Mediterranean-DASH diet Intervention for Neurological Delay (MIND), and cognitive impairment among elderly individuals in Pakistan.
Methods
From January to June 2023, this cross-sectional study recruited 462 participants aged 65 and above. We used proven tools in gerontological research, such as the MIND diet quiz and Quick Physical Activity Rating scale (QPAR), to evaluate diet and physical activity levels. Cognitive function was assessed using the Mini-Mental State Examination.
Results
Our analysis revealed that 26.40% of the participants had mild cognitive impairment, whereas 48.50% demonstrated low adherence to the MIND diet. The mean QPAR score was 20.51 ± 18.77. A significant association was found between lower physical activity levels and increased cognitive impairment (adjusted odds ratio 9.94, confidence interval (CI): 6.07–16.27). Additionally, higher adherence to the MIND diet correlated with reduced cognitive impairment (odds ratio 0.29, CI: 0.18–0.46).
Conclusions
These findings highlight the critical role of diet and physical activity in cognitive health among the elderly population. The study emphasizes the need for targeted public health interventions and further longitudinal research to explore the long-term effects of these factors on cognitive health.
Introduction
The global demographic landscape is transforming significantly, marked by a rapidly increasing elderly population. 1 Projections indicate that by 2050, the number of older adults will be more than double, reaching over 1.5 billion, accounting for 22% of the global population. 2 This trend is not isolated to developed nations; developing countries like Pakistan also witness similar shifts. In Pakistan, the percentage of the older population is expected to rise from 7% (14 million) in 2019 to 14% by 2050. 3 Such demographic changes pose substantial challenges, especially in the realm of age-related health issues, with cognitive impairment being a primary concern.
Cognitive impairment, which affects memory, language, attention, and visuospatial abilities,4,5 is a significant public health concern in developing countries like Pakistan,6–8 yet its focus in South Asia is limited.1,9 Previous research in Pakistan has primarily been focused on identifying the prevalence of cognitive impairment and the specific factors contributing to it.5,10,11 Notably, a study at Aga Khan University Hospital found severe cognitive decline among 200 patients with Type 2 Diabetes Mellitus. 12 However, the available data regarding mild cognitive impairment (MCI) is incomplete and fragmented. 13 MCI includes a subjective complaint of memory loss alongside the ability to perform daily activities such as meal preparation without impairment. 14 Additionally, it involves preserving cognitive skills, providing objective evidence of memory loss, and ruling out dementia. 15 Research in Islamabad and Rawalpindi indicates significant regional variability, with varying prevalence of MCI across urban (16.98%) and rural areas (27.64%). 5 Nevertheless, these studies are often limited in scope and do not provide a comprehensive view of MCI prevalence across different demographics and geographical regions.
Understanding the interplay of modifiable factors is critical for developing effective interventions against cognitive impairment.16–18 Research shows that lifestyle choices, such as poor diet and low physical activity, can increase the risk of cognitive decline by 40%. 19 While physical activity is known to mitigate functional decline in aging, 20 the precise relationship between physical activity and cognitive impairment, particularly in the context of neurodegenerative disorders such as Alzheimer's disease (AD), remains inadequately defined. 21
Compelling emerging evidence reveals significant positive impact of physical activity, not only in slowing progressive cognitive decline but also in enhancing cognitive functions in individuals with intellectual disabilities. 22 This dual effect—where physical activity might exert separate benefits for both neurodegenerative and intellectual capabilities—provides a broader framework for understanding its role in cognitive health. 23 Understanding these distinct pathways is crucial for tailoring interventions that could maximize cognitive outcomes across diverse populations. 24 Although many studies have linked physical activity to reduced rates of cognitive decline or dementia, the evidence is not entirely consistent, most probably due to variations in study methodologies, sample populations, or the types and intensities of physical activity measured. 25 Similarly, while adherence to diets like the Mediterranean and MIND (Mediterranean-DASH Diet Intervention for Neurodegenerative Delay) diets has been linked to cognitive health, findings are often inconsistent. 26
Since individuals who engage in regular physical activity are also more likely to follow healthier diets, it is essential to disentangle the effects of these factors to develop targeted public health interventions. 27
Moreover, the typical Pakistani diet, rich in staples like wheat, rice, and various meats and infused with a diverse array of spices such as turmeric and cumin, plays a significant role in the nutritional habits of the elderly population. 28 In contrast, Western studies show that plant-based foods, particularly vitamin A-rich ones, can prevent age-related cognitive decline. 29 Emerging research also highlights the beneficial role of moderate coffee and wine consumption as well as their combined relation with mood and cognition in the older population with chronic subcortical vascular disease and cognitive disorder at risk for both degenerative (i.e., AD), vascular (i.e., VaD), or mixed dementia.30,31 These effects have been shown to persist even after adjusting for confounding factors like smoking. 32 Tobacco is known to reduce the caffeine half-life, which may potentially contribute to a less strong protection of coffee in smokers. 33 Both wine and coffee are also often part of complex dietary patterns (i.e., the Mediterranean diet). 30 Furthermore, comparing the MIND diet with the Mediterranean diet, which also includes these psychoactive compounds, may offer additional insights into optimizing dietary interventions for cognitive health. 34
Evidence on cognitive impairment, MIND diet adherence, and physical activity levels is scarce in developing countries, particularly South Asia, with primary findings from high-income countries.35,36 This study aims to bridge this gap by exploring these relationships and determining the prevalence of MCI in the elderly population of Pakistan. This study hypothesizes that higher adherence to the MIND diet and increased physical activity levels will be associated with a lower prevalence of cognitive impairment among older adults. We expect that the combined effects of improved dietary habits and increased physical activity will contribute to better cognitive health outcomes by enhancing neuroplasticity, reducing neuroinflammation, and improving overall physical function. This cross-sectional study aims to provide valuable insights into these relationships and inform public health strategies in similar developing countries. By identifying the protective effects of physical activity and adherence to the MIND diet, the results can guide the development of targeted intervention programs. Additionally, dietary guidelines could be tailored to incorporate elements of the MIND diet, adapted to local food availability and cultural preferences, to enhance cognitive health across the aging population.
Methods
Study design
In this cross-sectional study, we acquired a representative sample of the respondents using a multistage stratified cluster-sampling technique.
In stage 1, one province in Pakistan was randomly selected, representing the socioeconomic conditions and lifestyles of two key geographical areas in Pakistan (north and east). 37 During the second stage, one city (considered urban with >11,263,000 citizens) and two cities (considered rural with >3,371,600 citizens) were randomly chosen from that one province. The selection was designed to categorize one of the urban cities as economically developed, with a gross domestic product (GDP) at or above the provincial median. In contrast, the other two rural cities were categorized as underdeveloped, with GDPs below the provincial median. 38 During stage 3, we randomly selected two districts from the urban city and six tehsils from the rural cities. Then, in stage 4, a random selection process was employed to choose two communities from each district and two villages from each tehsil. Typically, these communities or villages contained approximately 300–450 households each. In summary, this study employed a four-level sampling structure. The primary sampling unit was the province, followed by the secondary level of cities (urban and rural), the tertiary level of districts (urban) or tehsils (rural), and finally, the quaternary level of communities (urban) or villages (rural).
Study setting
The study was conducted in Punjab, as shown in Figure 1. This province is the most populous in Pakistan and is known for its distinctiveness and relevance. Due to its diverse demographic and socioeconomic composition, this setting is conducive to exploring aging and cognitive health. 39
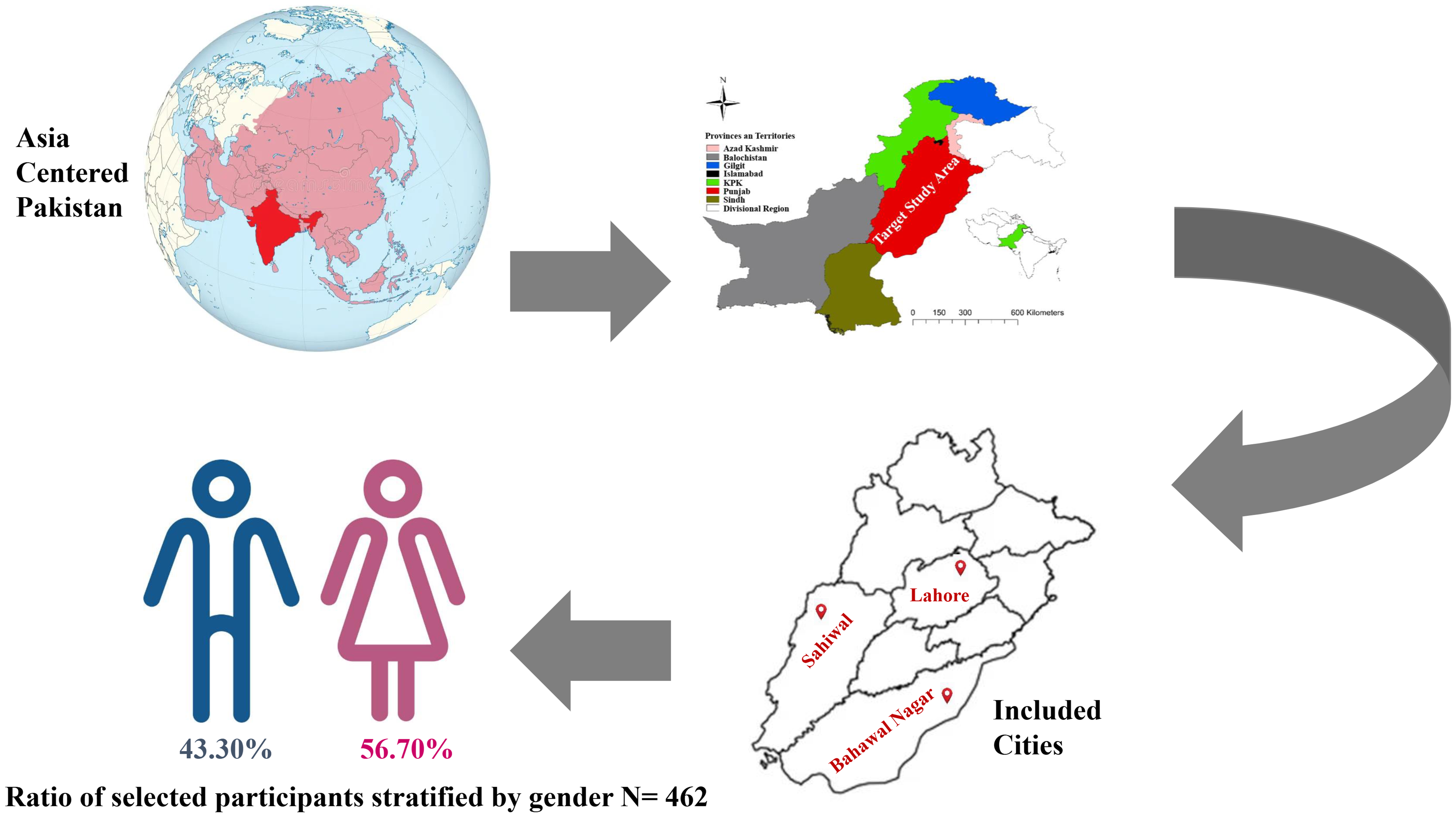
Geographics for data collection.
Study participants
Data is collected between January and June 2023 from diverse participants aged 65 or older, excluding those with life-threatening conditions or major sensory impairments, to ensure reliable cognitive assessments.
Sample size and sampling techniques
Our sample size, calculated for a 95% confidence level and based on an expected cognitive impairment prevalence of 37%, 40 involved 462 participants, aligning with standard epidemiological practices. A pilot survey and subsequent questionnaire refinements ensured the precision and relevance of our data collection instruments.
Data collection and variable measurement
To accurately assess the impact of lifestyle factors on cognitive health, our study measured dietary habits, physical activity levels, and cognitive function among the elderly population using targeted and validated tools.
Dietary assessment. Dietary data were collected using a locally adapted version of the validated Harvard Food Frequency Questionnaire (HFFQ). The FFQ included 72 food items categorized into the following seven groups: Meat, Milk and derivatives, Grains (Cereals), Fruits, Vegetables, Oils and spreads, and Discretionary food items. Participants were asked to report the frequency of consumption for each food item, with frequency options structured as Daily (once a day, 2–3 times per day, 4–5 times per day), Weekly (once a week, 2–4 times per week, 5–6 times per week), and Monthly (never or less than once a month, 1–3 times per month). This approach facilitated the collection of detailed dietary patterns. 41
Construction of the MIND diet score. The MIND diet score was calculated using data obtained from the FFQ. This score assesses adherence based on 15 dietary components divided into ten brain-healthy food groups and five brain-unhealthy groups. 42 The brain-healthy groups include green leafy vegetables, other vegetables, nuts, berries, olive oil, whole grains, fish (not fried), poultry (not fried), beans, and wine. The brain-unhealthy groups consist of red meat and meat products, butter and margarine, cheese, pastries and sweets, and fast-fried food. 43
Adherence to the MIND diet was evaluated using a score sheet that quantifies consumption frequency for each of the 15 food categories.44–48 Participants’ intake of each dietary component was scored as 0, 0.5, or 1, according to predetermined thresholds. Overall adherence was then categorized as low (scores ranging from 2.5 to 6.5), moderate (6.5 to 8.5), or high (8.5 to 15), in line with the thresholds originally proposed by Morris et al. 49
Physical activity assessment. The Quick Physical Activity Rating (QPAR) evaluates the physical activity levels of older adults. Unlike traditional physical activity measurements, which predominantly focus on objective metrics, the QPAR operates through an informant-rated system. 50 This approach allows for evaluating subjective physical performance, capturing a broad physical activity spectrum, including endurance and strength. 51 Individuals with impaired physical functionality can be efficiently identified by QPAR scores below 24, which indicate a high risk of physical impairment. 50
The QPAR is particularly effective due to its brief format comprising a 10-item questionnaire comprehensively covering various daily activities. 52 This range includes passive to strenuous physical activities, such as walking, household chores, and recreation. Each item is evaluated based on the frequency and intensity of the activities over a preceding four-week period, allowing for a nuanced capture of physical activity ‘dosage’ in a population that might not reliably engage in or accurately recall regular physical routines. 53
The validity and reliability of QPAR have been tested, and strong psychometric properties have been found across diverse patient ages, sexes, and cognitive statuses. 54 The scale correlates well with standardized physical performance measures such as dexterity, grip strength, and mobility assessments. Moreover, differentiating between varying levels of physical functionality and predicting potential falls or frailty makes it an indispensable tool in clinical and research settings focused on aging populations. 50
Cognitive function evaluation. Cognitive function was evaluated using the Mini-Mental State Examination (MMSE), a widely recognized cognitive assessment tool validated across various populations. 55
Statistical analysis
Statistical analysis, conducted using SPSS (version 26.0; IBM Corp, Armonk, NY, USA), incorporated both bivariate and multivariate logistic regression analyses, offering a comprehensive examination of the factors associated with cognitive impairment. The level of statistical significance (alpha) was set as 0.05. This approach aligns with contemporary analytical standards in epidemiological research.
Ethical consideration
This study was conducted according to the principles outlined in the Declaration of Helsinki. Ethics approval was granted by the Ethics Approval Council of the Xiangya School of Public Health, Central South University (reference number XYGW-2023-59). Before their enrollment in the research project, all respondents willingly provided informed consent and were allowed to decline or withdraw from the study at any point.
Results
Demographics of respondents
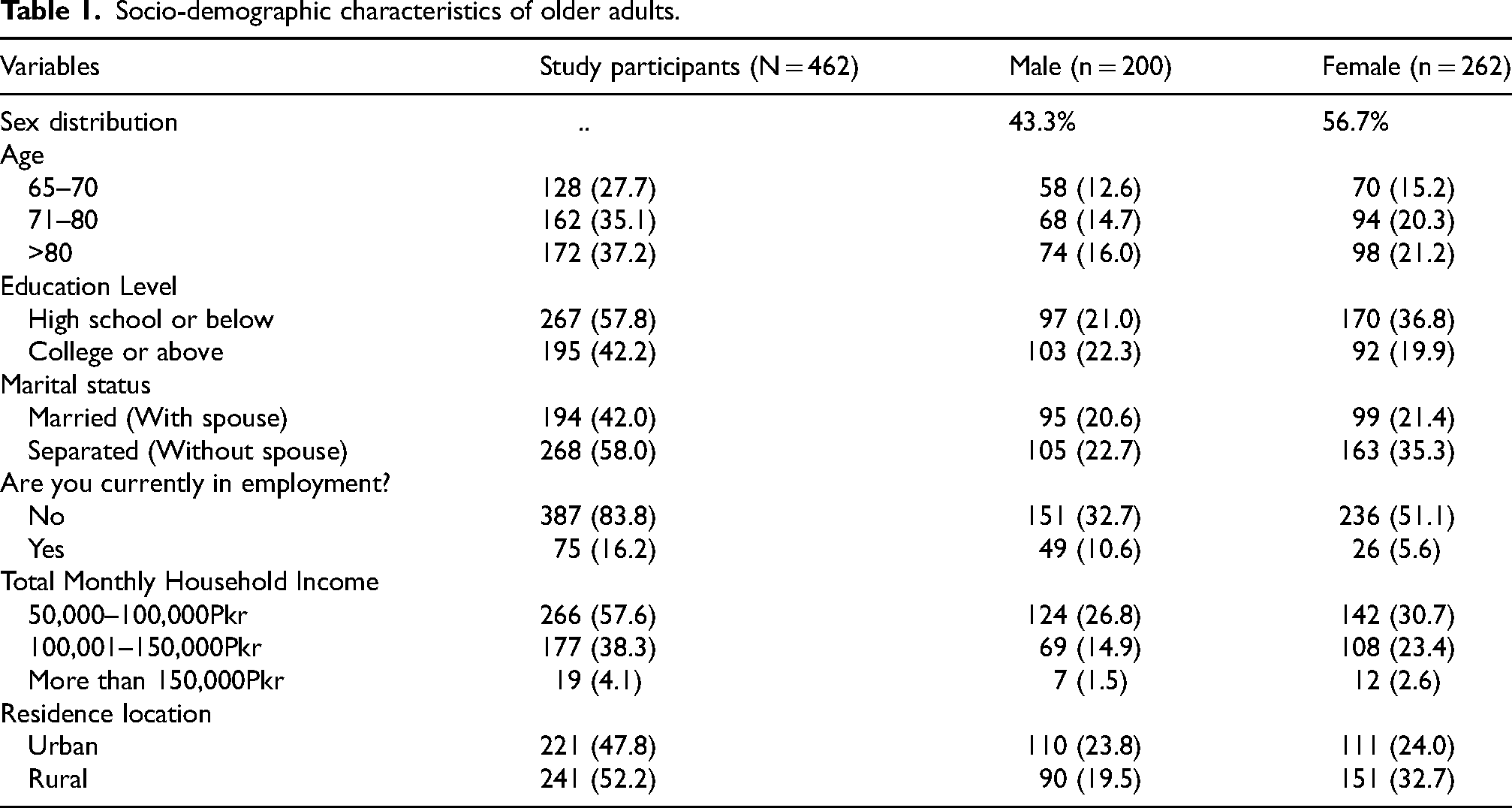
The characteristics of older adults are shown in Table 1. In total, 462 older adults gave thorough responses. Most (58.00%, n = 268) of older adults were separated (without a spouse), and 35.3%, n = 163 of them, were females. About (37.2%, n = 172) were aged > 80, averaging 74.60 ± 8.95 years. Concerning education level, 57.8% of respondents had a high school education or below, while 42.2% had a college education or above. Most respondents were not employed, and the majority had a moderate household income. Approximately 47.8% of the respondents reported to live in urban areas, while 52.2% lived in rural areas.
Socio-demographic characteristics of older adults.
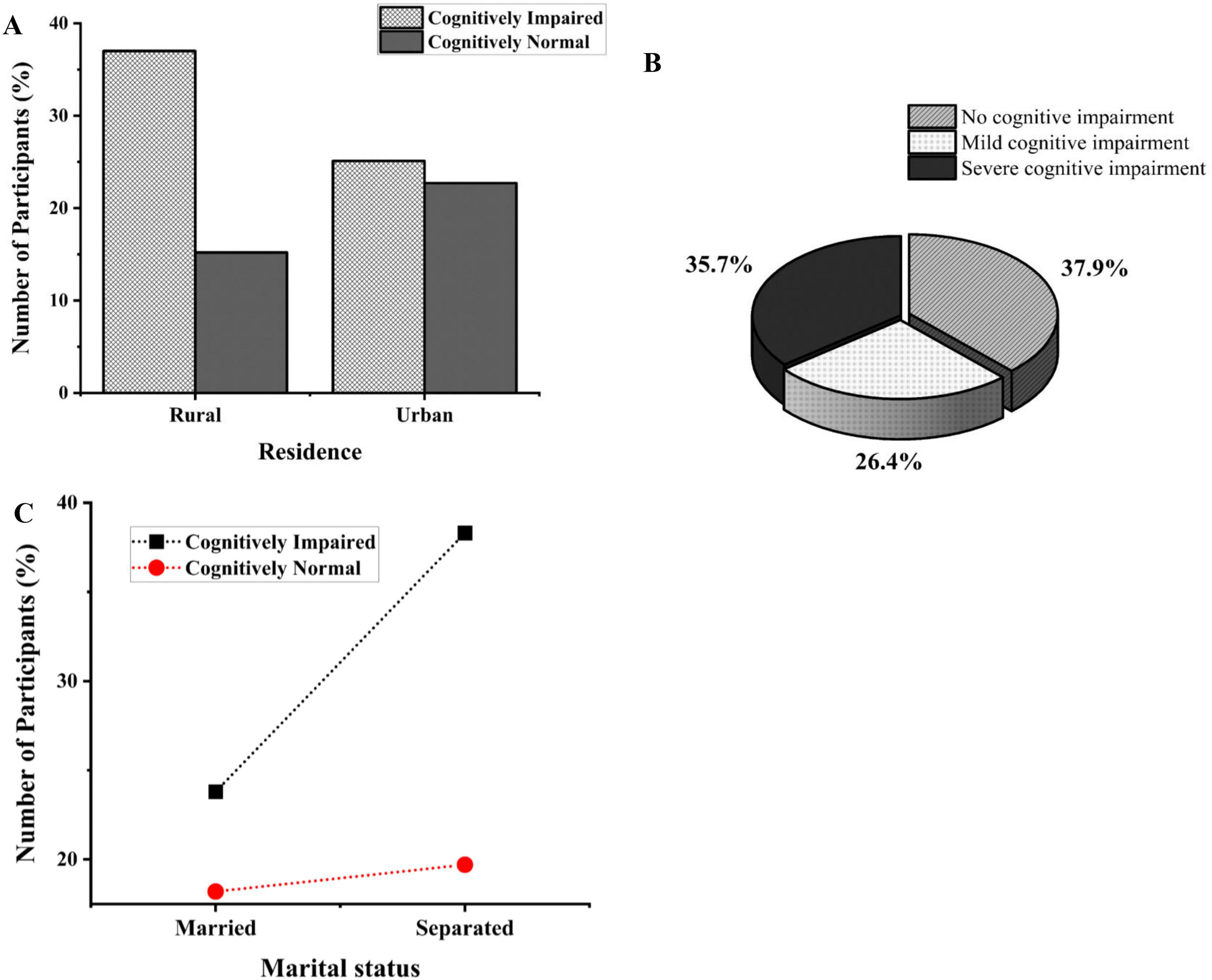
The current status of cognitive impairment in Punjab Province is shown in Figure 2. The study findings suggest that 165 (35.7%) older adults had severe cognitive impairment, 26.40% had MCI, and 175 (37.90%) older adults were cognitively normal. Cognitive impairment was higher in the rural area (37.0% against 25.10%, p < 0.001), and about (38.30%) of older adults with cognitive impairment were separated.
State of cognitive impairment of older adults. (A) Study participants with cognitive status stratified by residence. (B) Prevalence of cognitive impairment in study participants. (C) Study participants with cognitive status were stratified by marital status.
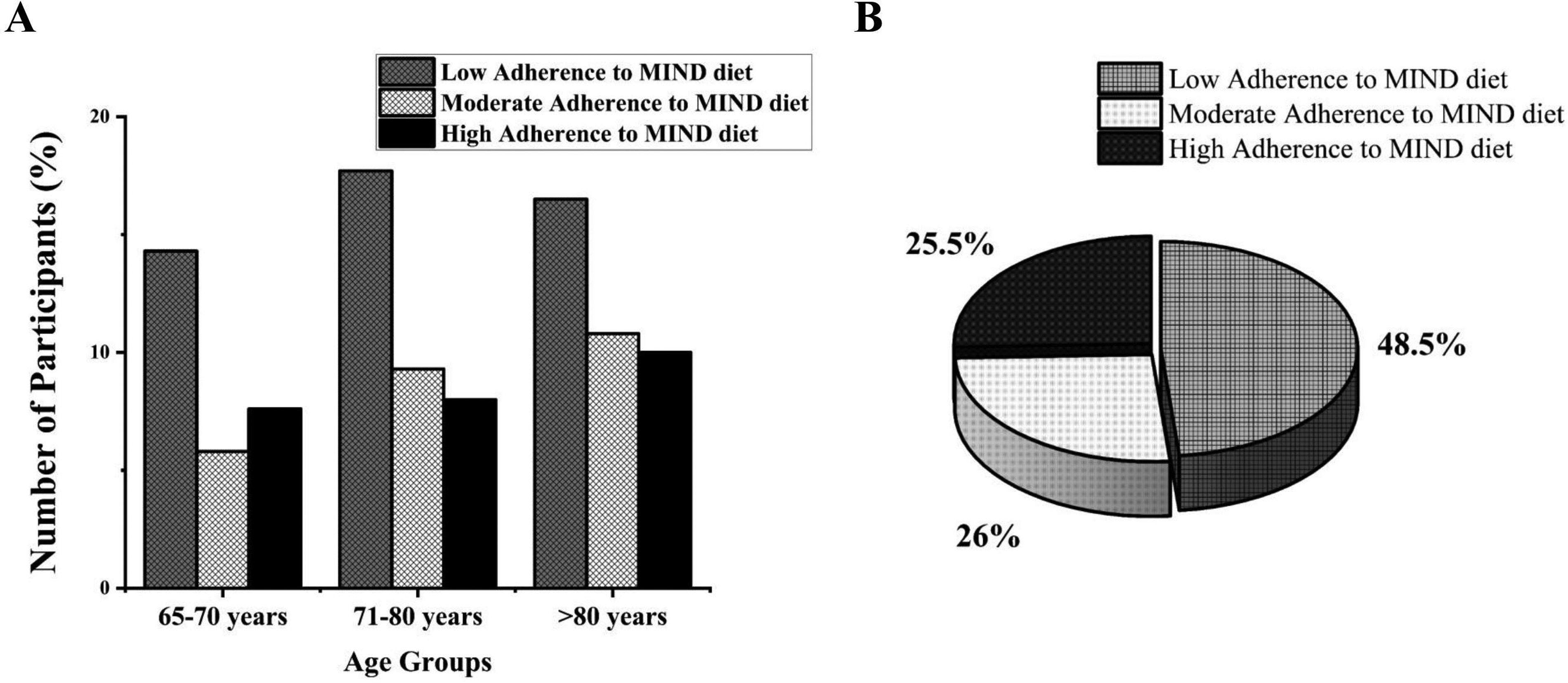
The current status of Adherence to the MIND diet in our study population has been demonstrated in Figure 3. In this study, 48.50%, 26.0%, and 25.50% have low, moderate and high Adherence to the MIND diet, respectively. This means that about 50% of older individuals may be at risk of cognitive impairment, as Adherence to the MIND diet has a negative correlation with cognitive impairment.
Adherence to MIND diet of older adults. (A) Age groups stratified study participants with MIND diet adherence. (B) Prevalence of MIND diet adherence in the study population.
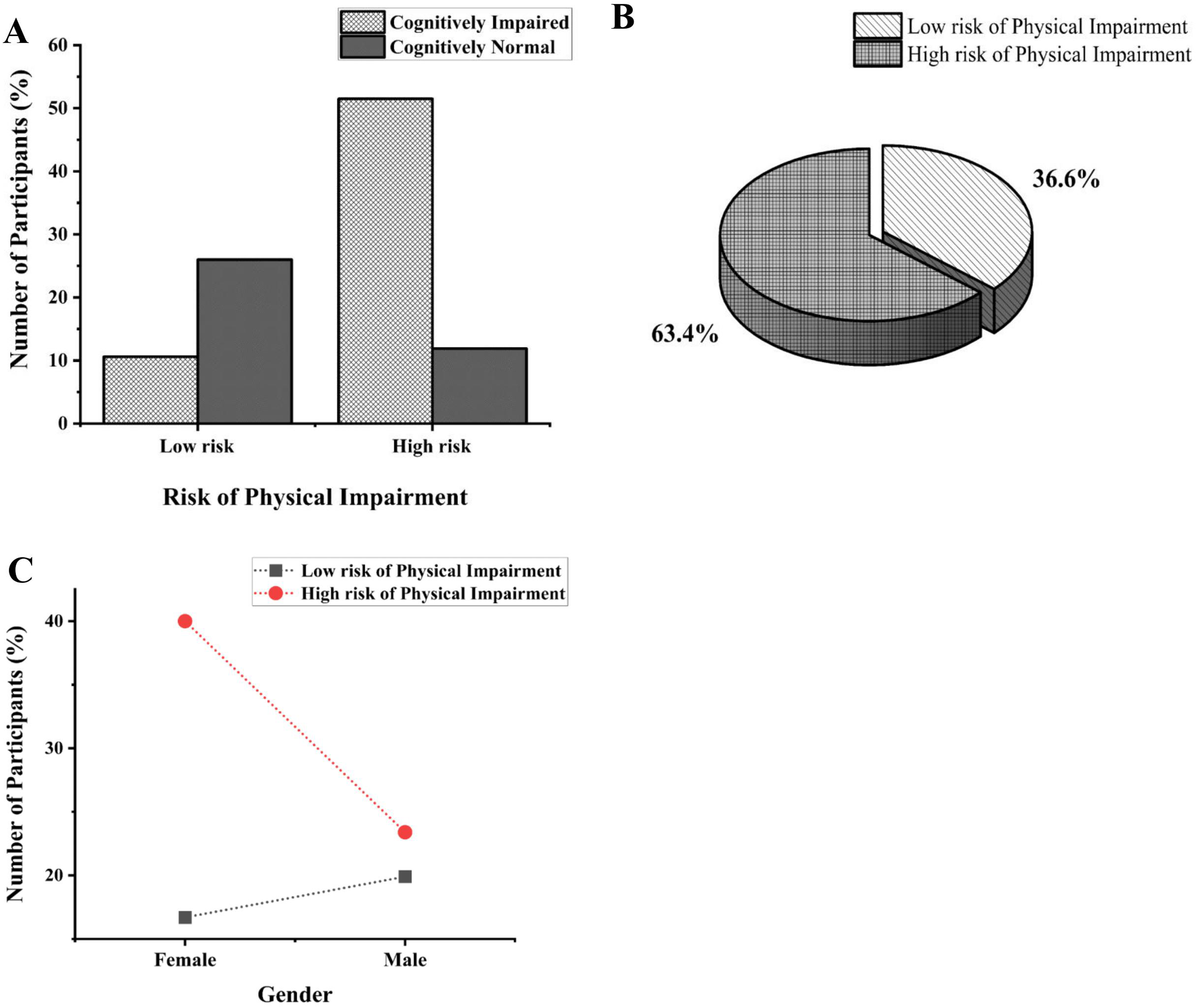
The risk of physical impairment in older adults is shown in Table 2 and Figure 4. The majority of participants were found to be at high risk of physical impairment, with a larger portion being females. The mean QPAR is 20.51 ± 18.77. Individuals with low physical impairment and those at high risk were distinguished based on the QPAR report (44.35 ± 20.55 versus 11.46 ± 5.38, p < 0.001).
State of risk of physical impairment of older adults. (A) Cognitive status of study participants related to the risk of physical impairment. (B) QPAR evaluated study participants and the risk of physical impairment. (C) Study participants with risk of physical impairment stratified by gender.
Distribution of older adults by quick physical activity rating scale.
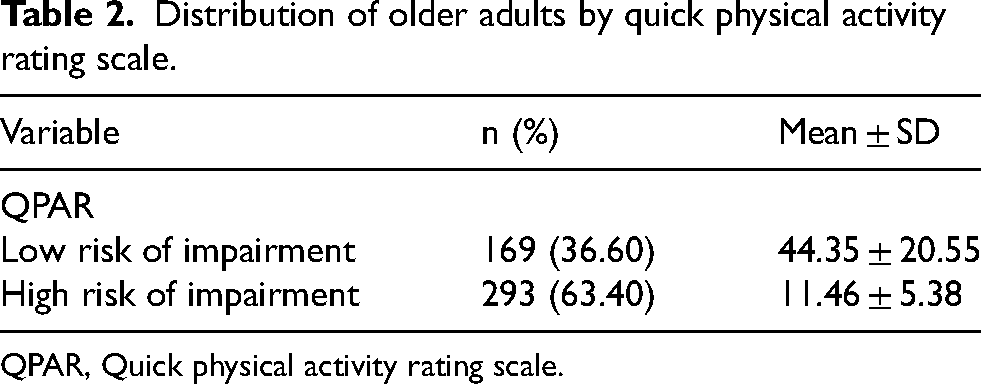
QPAR, Quick physical activity rating scale.
Of the 293 older adults who were at high risk of physical impairment, 119 (25.80%) were aged >80 years, and 103 (22.30%) were aged 71–80 years; 158 (34.2%) had low adherence to the MIND diet, and 65 (14.1%) had high adherence to the MIND diet.
Correlation of cognitive impairment with demographic features
Older adults with and without cognitive impairment are shown in Table 3.
Associations of cognitive impairment with socio-demographic characteristics of the older adults.
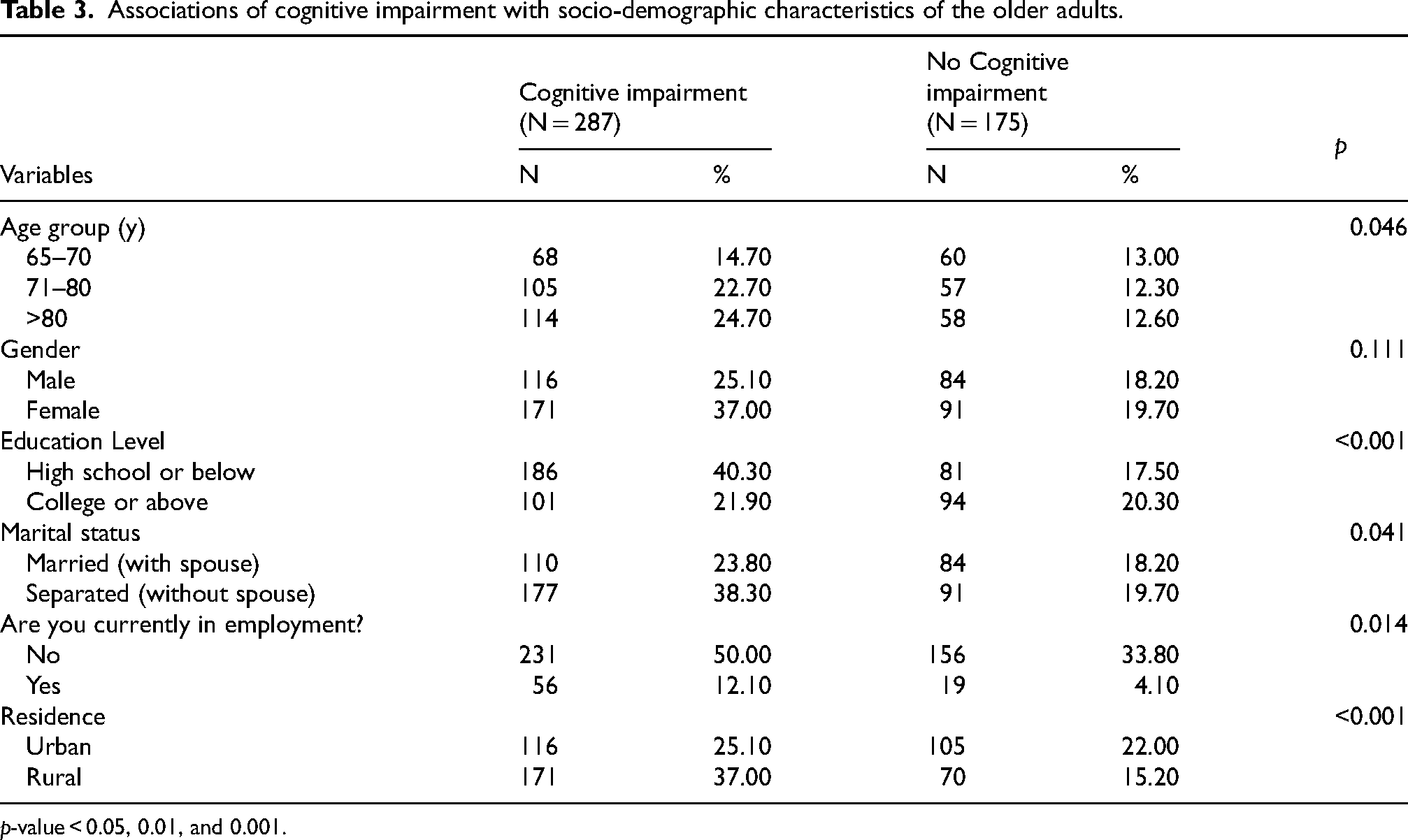
p-value < 0.05, 0.01, and 0.001.
The study found that the prevalence of cognitive impairment in older adults aged >80 years was 24.7%, 22.7% in those aged 71–80 years and 14.7% in those aged 65–70 years (p < 0.001). We found that the prevalence of cognitive impairment was 37.0% in women, compared to 25.1% in men (p = 0.11). Regarding education, cognitive impairment was found in 40.30% of adults with a high school level or below as compared to 21.90% of those with a college education or above (p <0.001). In terms of marital status, cognitive impairment is reported in 38.3% of separated (without a spouse) and in 23.80% of married adults (p = 0.04).
The prevalence of cognitive impairment was 12.10% in employed and 50.0% in non-employed. Approximately 37.0% reported cognitive impairment were living in rural areas as compared to 25.1% those living in urban areas. The chi-square test found significant differences in cognitive impairment with age, education level, marital status, employment and residence.
Analysis of older adults with and without cognitive impairment by the logistic regression
Table 4 displays the logistic regression findings classified by cognitive impairment status. The results of this investigation suggested multiple associations between cognitive impairment and other characteristics. Older adults aged >80 were 1.27 times more likely to be cognitively impaired (adjusted odds ratio (AOR) 1.27, CI: 0.68–2.34) than those aged < 80. Furthermore, we found a significant association between cognitive impairment and individuals who were separated or without a spouse (odds ratio (OR): 1.33, 95% CI: 0.82–2.17).
Characteristics of older adults with and without cognitive impairment about particular socio-demographic features.
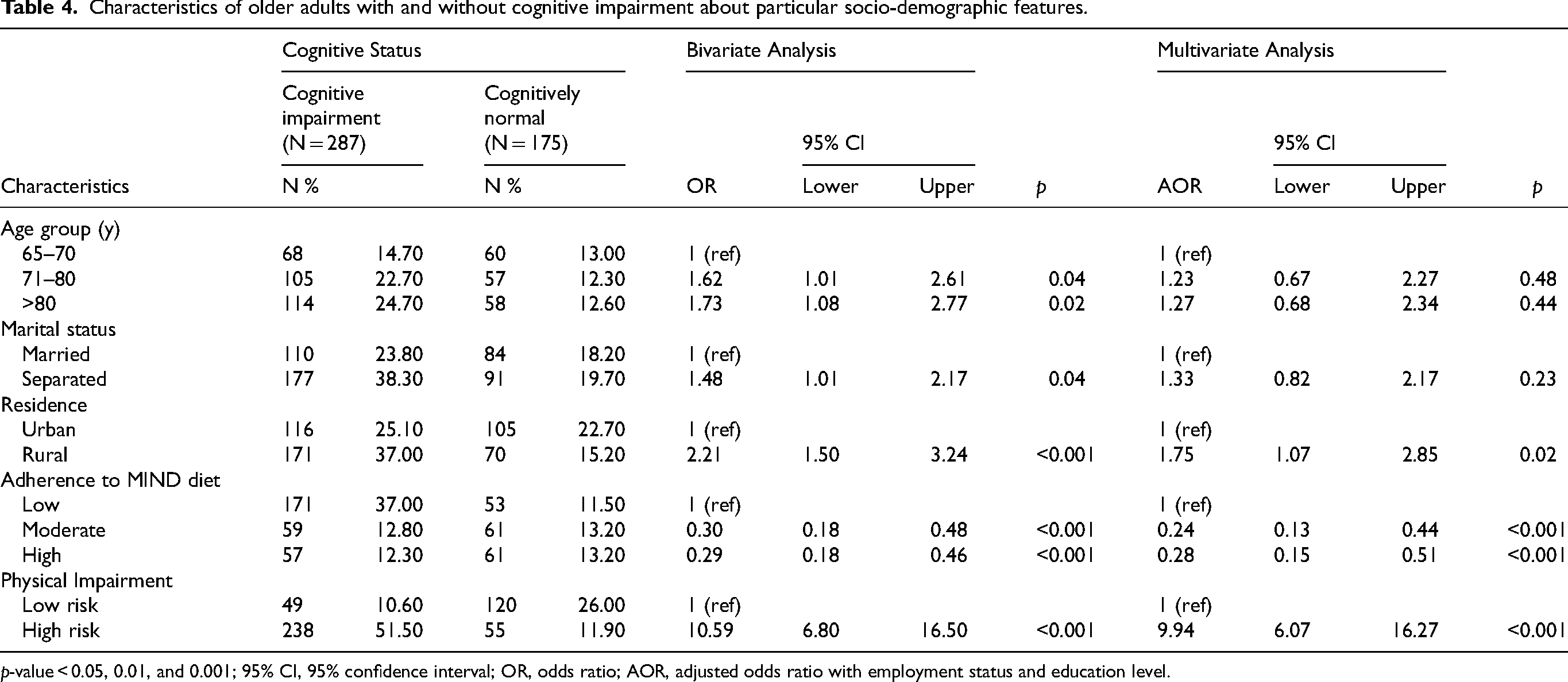
p-value < 0.05, 0.01, and 0.001; 95% CI, 95% confidence interval; OR, odds ratio; AOR, adjusted odds ratio with employment status and education level.
Participants residing in rural areas were found to be 2.21 times more likely to have cognitive impairment (OR: 2.21, CI: 1.50–3.24) compared to those living in urban areas. Additionally, adherence to the MIND diet was a protective factor. Moderate adherence had an inverse relationship with cognitive impairment (AOR: 0.24), while high adherence showed an even stronger inverse association (AOR: 0.28). Furthermore, older adults with a high risk of physical impairment were more likely to have cognitive impairment than those with a lower risk of physical impairment (AOR 9.94, CI: 6.07–16.27).
Discussion
Our cross-sectional study assessed cognitive function among older adults using robust gerontological tools and comprehensive sampling methodologies. The study found that 35.7% of participants had severe cognitive impairment. Almost half of the participants (48.5%) adhered poorly to the MIND diet. An inverse correlation was observed between physical activity levels and cognitive impairment (AOR 9.94, CI: 6.07–16.27). In contrast, a higher adherence to the MIND diet is associated with a lower risk of developing cognitive impairment (OR: 0.29, CI: 0.18–0.46).
Around 26.4% of the elderly population suffers from MCI, a figure which not only aligns with global trends but also reveals regional variations. 40 This rate surpasses previous research in diverse geographical settings, including the Central African Republic (6.3%–25%), 56 Portugal (16.90%), 57 and China (22.24%), 58 yet remains lower than those reported in Massachusetts (54.80%), Washington, DC (50%), 59 and Western Europe (74%). 60 Such comparisons underscore underlying differences in demographic and methodological approaches. This study also highlights significant regional disparities in the impacts of physical activity on cognitive health, particularly in Pakistan, where 63.41% of the elderly population faces higher risks of physical impairment. Socioeconomic factors, gender, and urbanization significantly influence physical activity levels; rural populations typically engage in more physical labor due to agricultural and manual work, whereas urban settings are characterized by increasingly sedentary lifestyles driven by mechanization and desk-bound jobs. Additionally, cultural constraints, especially those affecting women, restrict public engagement in recreational activities, exacerbating the challenge of maintaining physical activity. 61 Despite these regional and cultural challenges, our findings are consistent with international studies, such as Polish longitudinal research (75.6%) and studies from Mexico, Canada, and different Brazilian cities.60,62–67 This consistency might be attributed to the standardized use of the MMSE across studies. However, our results contrast with the Zutphen study, which found no significant association between physical activity and cognitive impairment, possibly due to variations in assessment methods and definitions of lifestyle cognitive impairment.68,69
Dietary choices significantly influence the cognitive health of the older population. In our study, 48.50% of participants had low adherence to the MIND diet, particularly notable among the Pakistani population, where traditional dietary habits are characterized by high consumption of refined grains, sugars, and red meats, starkly contrasting with the MIND diet's emphasis on whole grains, berries, and green leafy vegetables. 70 This divergence is especially pronounced in rural Pakistan, where limited access and a focus on subsistence farming complicate adherence to these dietary principles. 71 Conversely, countries in the Mediterranean region, whose diets align with the MIND diet principles, demonstrate greater adherence and improved health outcomes. 72 Studies in Sweden, Australia, America, France, and Iran have shown a positive correlation between MIND diet adherence and decreased cognitive impairment.7,73–76 However, several studies have found no association between adherence to the MIND diet and cognitive performance, possibly due to differing approaches used to assess the MIND diet and mental abilities. 43 Other dietary patterns have also shown similar findings. 77 For example, previous studies have revealed a consistent association between higher adherence to the Mediterranean diet and better cognitive function, reduced depressive symptoms, and an overall improved quality of life compared to those with lower adherence. However, these findings were shown to be more consistent when considering individuals living in the Mediterranean islands compared to those living in other regions. 78
Cognitive impairment is significantly linked to sociodemographic factors. Notably, separated individuals had a higher prevalence of cognitive impairment at 38.30%. Comparative studies from Sweden, Finland, Mexico, and the US reflect similar disparities.79–83 Moreover, urban regions report a higher prevalence of cognitive impairment at 37.0%, compared to 25.10% in rural areas. These observations are consistent with findings from Northern Portugal, China, and the US, underscoring the influence of environmental and lifestyle factors on cognitive health.84–86 Furthermore, our study reveals that older adults aged >80 experience a higher rate of cognitive impairment (24.70%), aligning with research from China and the US that identifies advancing age as the primary risk factor for cognitive decline.87–89
Prior research in this field has been limited by a dearth of consistent data from certain regions, notably Pakistan, a key South Asian nation with a substantial elderly demographic. To the best of our knowledge, this is the first study on the prevalence of cognitive impairment in the MIND diet and the risk of physical impairment in South Asia. We found a startlingly high rate of cognitive impairment (62.10%) in this group, indicating a distinct demographic profile that warrants further investigation.
Nonetheless, the study's cross-sectional design lacks causality, necessitating further confirmation through longitudinal studies. Self-detailed dietary preferences and potential assessment bias may affect results accuracy. Additionally, data removal due to missing or refusing participants could create biases. Furthermore, Social desirability bias could overstate or understate participants’ adherence to the MIND diet and physical activity.
Conclusion
The prevalence of severe cognitive impairment among adults aged 65 years and older is 35.7%, and the prevalence of mild cognitive impairment in Pakistan is 26.40%. There are significant differences in cognitive impairment based on factors such as education level, marital status, employment status, and place of residence. This study uniquely contributes by examining these socio-demographic factors in the Pakistani context, offering new insights that were previously underexplored. Engaging in regular physical activity and adhering to the MIND diet were protective factors against cognitive impairment. This study adds value by providing region-specific data and highlighting actionable insights for public health interventions. Future research could build on these findings to explore long-term effects and intervention strategies.
Footnotes
Acknowledgments
The authors acknowledge the varied assistance of the entire Xiangya School of Public Health team at Central South University in conducting this study. And many thanks to the senior citizens who consented to respond to the questions.
Author contribution
Binish Islam (Conceptualization; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Jianwu Wang (Conceptualization; Data curation; Formal analysis; Funding acquisition; Project administration; Resources; Supervision; Validation; Visualization); Tianjiao Li (Conceptualization; Data curation; Methodology; Resources; Software); Mengying Xu (Visualization; Writing – review & editing); Dan Yang (Visualization; Writing – review & editing); Hanxiao Lv (Formal analysis; Software; Visualization); Qian Zhang (Data curation; Formal analysis; Software); Goudja Gassara (Software; Writing – review & editing); Tasiu Ibrahim Ibrahim (Conceptualization; Investigation; Methodology).
Funding
This research was funded by Hunan Natural Science Foundation - General Project, Project Code 2022JJ30785, Changsha Science and Technology Plan Project, Project Code kq2202078.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Both the data and the source of the data cannot be disclosed due to ethical and privacy issues.