
Abstract
Background
Episodic memory impairment is the core clinical feature of patients with typical Alzheimer's disease (AD) at an early stage. Since sleep plays a very important role in memory consolidation, the relationship between memory impairment and sleep disorders in AD patients is worthy of investigation.
Objective
To investigate sleep disturbances and their correlations with memory impairment in patients with AD and amnestic mild cognitive impairment (aMCI).
Methods
Forty-three patients with AD, 43 patients with aMCI, and 43 cognitively unimpaired controls (CUCs) were recruited and subjected to memory assessment via the Hopkins Verbal Learning Test–Revised and objective sleep evaluation via polysomnography (PSG).
Results
The total sleep time and the percentages of nonrapid eye movement (NREM) sleep stage 3 (N3) and the rapid eye movement (REM) were lower, while the percentages of NREM sleep stage 2 (N2) were greater in the AD and aMCI groups than in the CUC group (all p < 0.01). Compared with the CUC group, the AD group also presented a longer sleep latency and higher NREM sleep stage 1 (N1) percentage, apnea-hypopnea index (AHI), periodic limb movements during sleep index (PLMSI), and arousal index (AI). Both total learning scores and delayed recall scores were positively correlated with the N3 sleep percentage and negatively correlated with the AHI and PLMSI (all p < 0.01). Recognition scores were positively correlated with the N3 sleep percentage and negatively correlated with the AI (all p < 0.01).
Conclusions
Our results suggest that sleep disturbance is correlated with learning and memory disability in AD and aMCI patients. PSG is useful for screening and monitoring AD.
Introduction
As the global population over 60 years of age will increase to 21.2% by 2050, the number of individuals with Alzheimer's disease (AD) is expected to approach 131.5 million at that time. 1 AD is a progressive neurodegenerative disease that is pathologically characterized by extracellular amyloid-β (Aβ) plaques, intracellular neurofibrillary tau tangles, and neuronal loss in the brain, which can be observed one or two decades before a patient develops dementia. Currently, AD is recognized to exist as a continuum of the disease spectrum, in which mild cognitive impairment (MCI), particularly the amnestic type (aMCI), is a prodromal stage with slight initial symptoms. 2 It has been reported that more than 10% of patients with aMCI develop AD annually. 3
Numerous studies have shown that sleep disorders are closely related to AD and dementia, even in the early stages.4–6 The incidence of sleep disorders has been reported to be much greater in AD and aMCI patients than in cognitively unimpaired controls (CUC).7,8 On the other hand, a meta-analysis revealed that persons with sleep disturbances had a 1.19 times greater risk of developing all-cause dementia and a 1.49 times greater risk of developing AD than did those without sleep disturbances. 9
Polysomnography (PSG) is a standard and objective measurement of sleep structure and quality in clinical practice and research. Previous studies have reported several types of sleep disturbances,4,10–13 such as decreased sleep stage 3 and the rapid eye movement sleep stage4,10 and increased sleep apnea-hypopnea and periodic limb movements during sleep indices,10,11 as measured by PSG, in both AD and aMCI patients. There is a complex and bidirectional relationship between sleep and AD pathology, including but not limited to Aβ plaque accumulation 14 and an impaired melanin-concentrating hormone system, which compromises hippocampus-dependent functions. 15 The clinical associations of sleep disturbances with different AD stages are worthy of investigation.
In our previous study, negative correlations between learning performance and delayed recall on the Hopkins Verbal Learning Test–Revised (HVLT-R) and subjective sleep quality and sleep efficiency measured with the Pittsburgh Sleep Quality Index (PSQI) were observed in patients with aMCI. 16 In the present study, we compared verbal learning and memory abilities and objective sleep structure obtained via PSG between patients with AD, patients with aMCI, and CUCs and further explored the associations between the memory ability and various types of sleep disturbances.
Materials and methods
Participants
Participants aged 50–80 years and with at least 6 years of education were consecutively recruited from the memory clinic of the Tianjin Medical University General Hospital between July 2019 and September 2022. Patients with AD met the criteria for probable AD according to the National Institute on Aging-Alzheimer's Association (NIA-AA), 17 with a Mini-Mental State Examination (MMSE) score ≤24 and a Clinical Dementia Rating (CDR) score ≥1. Patients with aMCI were diagnosed according to Petersen's criteria, 18 with a logical memory score less than 1.5 standard deviations from the mean for healthy individuals of the same age and education level, with an MMSE score >24 and a CDR score = 0.5. Age-, sex- and education level-matched CUCs who had no complaints of memory or cognitive impairments and no obvious abnormalities on neurological, neuropsychological, or neuroimaging examinations, with an MMSE score > 26 and a CDR score = 0, were consecutively recruited from an older community cohort. All participants had a Geriatric Depression Scale score ≤ 10 and a Hachinski scale score ≤ 4. This study was approved by the institutional review board and ethics committee of the Tianjin Medical University General Hospital. All participants and their guardians were informed about the full context of the study and voluntarily signed informed consent forms.
Patients with cognitive impairment caused by other neurological, mental or systemic disorders, such as Parkinson's disease and related disorders, cerebrovascular diseases, frontotemporal lobar degeneration, schizophrenia, major depressive disorder, thyroid disease, or vitamin B12 deficiency, were excluded.
Procedures
All participants underwent memory assessment, subjective sleep evaluation and PSG. Memory assessment and subjective sleep evaluation were separately performed by two different raters in the morning within 3 days before PSG measurement in a quiet testing room. An overnight PSG was then conducted in the sleep laboratory of our hospital. All patients had a table dose of a medication for AD, e.g., cholinesterase inhibitors and memantine, and did not take psychotropic drugs, such as antidepressants, anxiolytics, antipsychotics, or antiepileptics, within 3 months before recruitment. No participants took any type of hypnotic within 1 week before PSG measurement.
Memory assessment with the HVLT-R
The HVLT-R, 19 which consists of a total of 12 words belonging to three semantic categories (jewels, animals, and dwellings), was administered to all participants. The rater read 12 words aloud one by one at a rate of approximately 1 word per second to the participants. Then, the participants were asked to immediately recall as many words as possible. The same word list was learned 3 times. After 20 min, the participants were asked to recall the words that they had learned (delayed recall). Finally, a “yes-no” recognition test was conducted in which 24 words, including 12 target words and 12 nontarget words (6 semantically related and 6 semantically unrelated), were read one by one to the participants. The total score from the 3 learning trials, the delayed recall score and the recognition score were used to evaluate memory in this study.
Subjective sleep evaluations
Subjective sleep evaluations, including the PSQI, Epworth Sleepiness Scale (ESS), and Insomnia Severity Index (ISI), were performed after HVLT-R testing by a trained rater. The PSQI, 20 which consists of seven subscales, was used to evaluate nighttime sleep quality and daytime function, with a higher score indicating worse sleep quality. The ESS 21 and ISI 22 were used to assess the severity of daytime sleepiness and insomnia, respectively, with higher scores indicating more severe symptoms.
Sleep assessment with PSG
An objective sleep evaluation was performed via an overnight video PSG (Nicolet V44, Nicolet) in the sleep laboratory within two days after the neuropsychological assessments. Each participant was asked to return to bed at their usual bedtime and underwent PSG assessment by a trained technician. The results of PSG were recorded, and its parameters were analyzed according to the guidelines of the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events. 23 The sleep parameters analyzed in this study included the total sleep time (TST), sleep efficiency (SE) and sleep onset latency (SL) for evaluating sleep efficiency; the percentages of the time in nonrapid eye movement (NREM) sleep stages 1, 2, and 3 (N1, N2, and N3); and REM for evaluating sleep structure. The AHI was calculated as the number of apnea events plus hypopnea events per hour of sleep for evaluating sleep-breathing events; the PLMSI was calculated as the number of leg movements per hour of sleep for evaluating sleep movement events; and the arousal index (AI) was calculated as the total number of arousals divided by the duration of sleep in hours for evaluating spontaneous and passive arousals during sleep.
Statistical analysis
Statistical analyses were performed via the SPSS 25.0 software (SPSS Inc., Chicago, IL, USA). Since most data on subjective sleep quality, memory tests and sleep structure did not follow a normal distribution according to the Shapiro‒Wilk test, all data are expressed as the median and interquartile range for continuous variables. The demographic and clinical data of the patients with aMCI and those with AD and CUCs were analyzed via the Pearson chi-square test for categorical variables (e.g., sex) or the Kruskal‒Wallis test for continuous variables. The differences in subjective sleep quality and memory test scores and sleep structure data among the three groups were analyzed via the Kruskal‒Wallis test, followed by the Bonferroni t test for post hoc pairwise comparisons, with age, sex, and years of education as covariates. All the tests were two-tailed, and values of p < 0.05 were regarded as significant. Spearman rank correlation was used to analyze the associations between the memory ability (total learning score, delayed recall score and recognition score on the HVLT-R) and PSG outcomes in patients with AD and those with aMCI, with age, sex, and years of education as covariates. The Bonferroni correction was used after Spearman rank correlation, and a corrected statistical significance threshold of 0.003 was set.
Results
Demographics of all participants
The sample size was determined via the PASS software. To compare the means of the three groups, a medium effect size of 0.80 was established. The level of significance was 0.05, and the statistical power was 0.90 across the three groups. Accordingly, a minimal sample size of 12 participants in each group was suggested.
Forty-three patients with mild to moderate AD (25 males), 43 patients with aMCI (28 males) and 43 CUCs (23 males) were recruited. All participants completed the memory tests, subjective sleep questionnaires and PSG measurements in this study.
The demographic and clinical characteristics of all participants were analyzed via the Pearson chi-square test for categorical variables (sex) or the Kruskal‒Wallis test for continuous variables, as shown in Table 1. All the participants were right-handed. No significant differences in age, sex, education, or body mass index were found among the AD, aMCI and CUC groups. Significant differences in MMSE scores were observed between two groups (all p < 0.01), with the highest score being in the CUC group and the lowest score being in the AD group.
Demographics and clinical information of all participants.

Values are presented as medians and interquartile ranges for continuous data and as the probability (percent) for categorical variables. Demographic data were analyzed using the Pearson chi-square test for categorical variables (*) or Kruskal-Wallis test.
AD: Alzheimer's disease; aMCI: amnestic mild cognitive impairment; CUC: cognitively unimpaired control; BMI: body mass index; MMSE: Mini-Mental State Examination.
Comparison between AD and aMCI, p < 0.05.
Comparison between AD and CUC, p < 0.05.
Comparison between aMCI and CUC, p < 0.05.
Comparison of memory scores and objective sleep quality among the three groups
The differences in subjective sleep quality and memory among the three groups were analyzed via the Kruskal‒Wallis test, followed by the Bonferroni t test for post hoc pairwise comparisons, with age, sex, and years of education as covariates (Table 2).
Comparison of HVLT-R scores and sleep questionnaire scores between the AD, aMCI and CUC groups.

Values are presented as medians and interquartile ranges. The differences in subjective sleep quality and memory among the three groups were analyzed via the Kruskal—Wallis test, followed by the Bonferroni t test for post hoc pairwise comparisons, with age, sex, and years of education as covariates.
AD: Alzheimer's disease; aMCI: amnestic mild cognitive impairment; CUC: cognitively unimpaired control; PSQI: Pittsburgh Sleep Quality Index; ESS: Epworth Sleepiness Scale; ISI: Insomnia Severity Index.
Comparison between AD and aMCI, p < 0.05.
Comparison between AD and CUC, p < 0.05.
Comparison between aMCI and CUC, p < 0.05.
There were significant differences in the total learning scores (all p < 0.05) and delayed recall scores (all p < 0.01) on the HVLT-R among the three groups. The AD group also had lower recognition scores than did the other two groups (all p < 0.01); however, there was no difference between the aMCI and CUC groups.
In terms of the PSQI, ESS, and ISI scores, there were significant differences among the three groups. The AD and aMCI groups presented higher self-assessment scale scores than did the CUC group (all p < 0.01). The AD and aMCI groups did not differ in these questionnaire scores.
Comparison of the sleep structure among the three groups
The differences in the sleep structure among the three groups were analyzed via the Kruskal‒Wallis test, followed by a post hoc test (Bonferroni t test), with age, sex, and years of education as covariates. Significant differences in most sleep structure outcomes were observed among the three groups (Table 3). The percentages of N3 and REM individuals were the lowest in the AD group and the highest in the CUC group (p < 0.05 between each pair of groups). Patients with AD presented greater percentages of N1 and greater PLMSI and AI than did aMCI patients and CUCs (all p < 0.05); however, no differences were found between the aMCI and CUC groups, except for the AI. The AD and aMCI groups both had significantly shorter TSTs, longer SLs and higher percentages of N2 individuals than did the CUC group (all p < 0.01), and no differences were found between the AD and aMCI groups. In addition, a lower SE and a higher AHI were found in the AD group than in the CUC group (p < 0.01).
Comparison of sleep structure between the AD, aMCI and CUC groups.
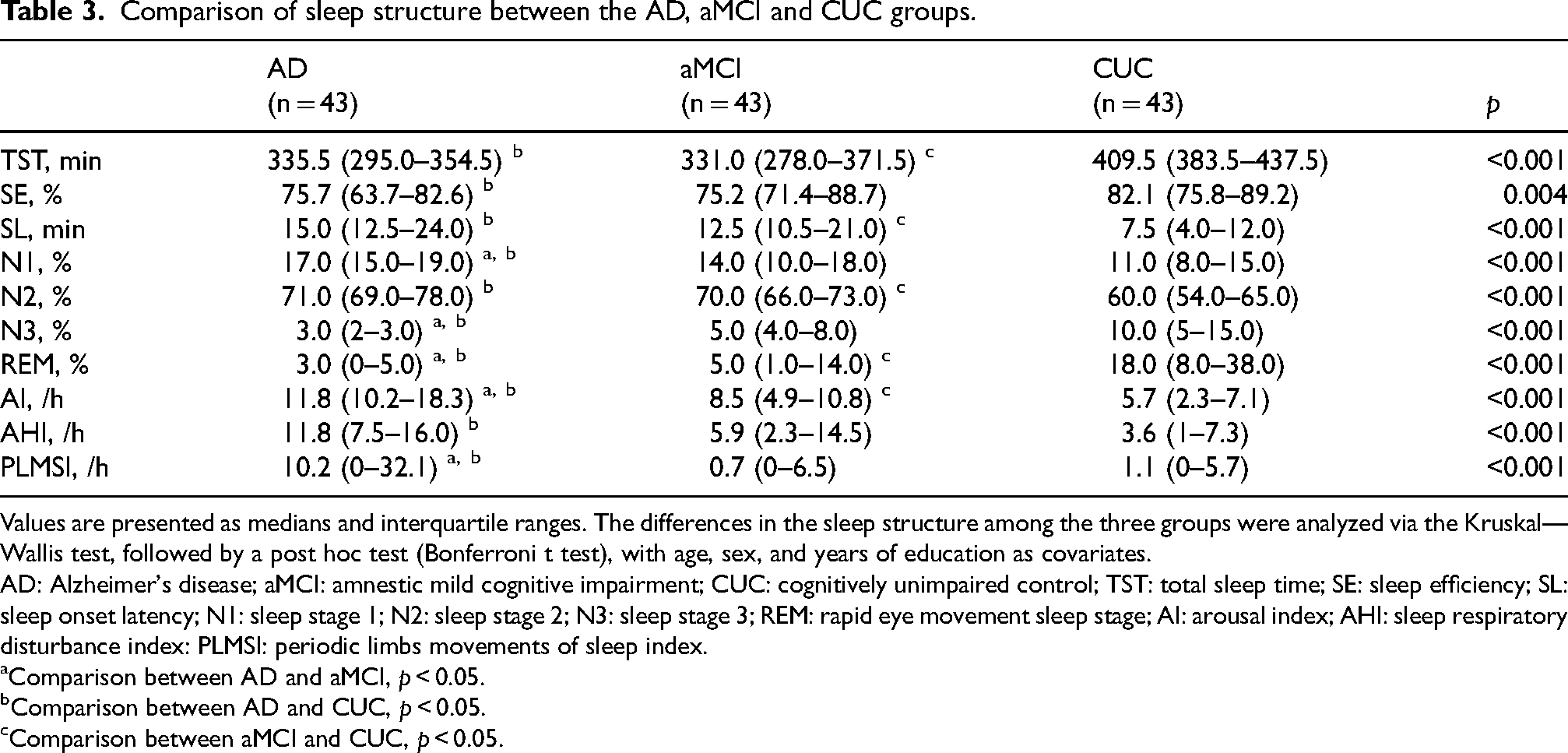
Values are presented as medians and interquartile ranges. The differences in the sleep structure among the three groups were analyzed via the Kruskal—Wallis test, followed by a post hoc test (Bonferroni t test), with age, sex, and years of education as covariates.
AD: Alzheimer's disease; aMCI: amnestic mild cognitive impairment; CUC: cognitively unimpaired control; TST: total sleep time; SE: sleep efficiency; SL: sleep onset latency; N1: sleep stage 1; N2: sleep stage 2; N3: sleep stage 3; REM: rapid eye movement sleep stage; AI: arousal index; AHI: sleep respiratory disturbance index: PLMSI: periodic limbs movements of sleep index.
Comparison between AD and aMCI, p < 0.05.
Comparison between AD and CUC, p < 0.05.
Comparison between aMCI and CUC, p < 0.05.
Associations between the HVLT-R scores and sleep structure in patients with AD and aMCI
Spearman rank correlations were used to clarify the relationships between HVLT-R scores and sleep structure, with age, sex, and years of education as covariates. Specifically, the N3 sleep percentage was associated with the total learning score (r = 0.616, p < 0.0001), delayed recall score (r = 0.622, p < 0.0001), and recognition score (r = 0.683, p < 0.0001); the REM sleep percentage was associated with the delayed recall score (r = 0.282, p = 0.008); the AHI and PLMSI were associated with the total learning score (r = −0.399, p < 0.0001; r = −0.436, p < 0.0001, respectively) and delayed recall score (r = −0.438, p < 0.0001; r = −0.324, p = 0.002, respectively); and the AI was associated with the recognition score (r = −0.535, p < 0.0001), as shown in Figure 1.

Correlations between HVLT-R scores and PSG outcomes in Alzheimer's disease and amnestic mild cognitive impairment patients based on Spearman rank correlation. The total learning score was positively correlated with the percentage of N3 sleep (A) and negatively correlation with apnea-hypopnea index (AHI) (B) and periodic limb movements during sleep index (PLMSI) (C). The delayed recall score was positively correlated with the percentages of N3 sleep (D) and REM sleep (E) and negatively correlated with the AHI (F) and PLMSI (G). The recognition score was positively correlated with the percentages of N3 sleep (H) and negatively correlated with arousal index (AI) (I).
Discussion
In this study, we observed robust verbal learning and memory disabilities in patients with AD and aMCI, although recognition was still preserved in patients with aMCI. Sleep disturbances were demonstrated by either self-assessment scales or objective PSG measurements in both AD and aMCI patients. In general, the AD and aMCI groups presented worse sleep quality and daytime function, more excessive sleepiness, and more insomnia than did the CUC group. Specifically, sleep structure disruption (e.g., a decreased total sleep time and decreased percentages of N3 and REM sleep) was an early marker observed in aMCI patients, and increased apnea-hypopnea events and periodic limb movements during sleep were observed only in AD patients. All these PSG parameters were strongly correlated with memory impairment.
In our study, sleep structure disruption was prominent in patients with AD and even in patients with aMCI. Specifically, the percentages of slow-wave sleep (SWS) and REM sleep decreased, which was also correlated with decreased learning and memory abilities in AD and aMCI patients. These findings are consistent with those of several previous studies in which reductions in N3 and REM sleep stages were observed in AD patients, even at the mild stage, and in aMCI patients and correlated with cognitive impairment measured with the MMSE and Montreal Cognitive Assessment (MoCA).10,11 Accordingly, decreased N3 sleep and REM sleep might be early sleep markers of AD, which continuously worsened during disease progression. Measuring disruption and longitudinal decreases in N3 sleep and REM sleep by PSG could be used for early screening and monitoring disease progression in patients with AD and aMCI.
In the hippocampus, the CA1 and CA3 regions strongly contribute to memory encoding and consolidation.24,25 During SWS in particular, CA3 pyramidal neurons are spontaneously activated in synchronous bursts that trigger massive activation of CA1 pyramidal cells, promoting the strength of connections between clusters and ultimately completing the consolidation of memories. Moreover, hippocampal levels of the memory-associated transcription factors CREB and cAMP are elevated during REM sleep. 26 Therefore, both SWS and REM sleep contribute to the consolidation of declarative memory and are associated with delayed recall performance.27–31
We also found that the AHI was significantly greater in AD patients than in aMCI patients and was negatively correlated with both learning and delayed recall. These findings are supported by the findings of several previous studies that revealed a relationship between mild to severe obstructive sleep apnea (OSA) and poor cognition 32 and negative correlations between the AHI and learning and memory abilities in patients with AD or aMCI.16,33,34 Intermittent hypoxia and subsequent oxidative stress and redox reactions in the brain (particularly in the hippocampus), caused by OSA, can lead to accelerated Aβ deposition 35 and, ultimately, to neuronal apoptosis and cortical thinning. 36
Similarly, a significantly increased PLMSI was found mainly in AD patients and was negatively correlated with both learning and delayed recall in this study. These findings are consistent with those of most previous studies.37–39 Another study reported significantly higher PLMSI scores, even in aMCI patients, and their associations with lower MMSE and MoCA scores. 10 Several hypothetical mechanisms related to the PLMSI in patients with AD, such as iron deficiency, 40 neurotransmission (e.g., acetylcholine and serotonergic) impairment, 41 and comorbidity with synucleinopathy, 42 have been suggested. According to our findings, longitudinally increased AHI and PLMSI, as measured by PSG, may suggest clinical worsening in individuals with AD.
Since obvious sleep disturbances were observed in both AD and aMCI patients and were correlated with their memory deficits, sleep intervention could be a potentially preventive and therapeutic target for AD. There is some evidence suggesting that a reduction in the sleep time is correlated with increased cortical Aβ deposition and that sleep quality rather than the duration is closely associated with the tau burden in the medial temporal lobe in both cognitively normal older adults and AD patients..43–45 In addition, increased uptake of amyloid tracers on PET was observed in middle-aged cognitively normal individuals with severe OSA and was significantly correlated with the AHI. 46 Therefore, improving sleep quality, e.g., increasing N3 and REM sleep percentages and treating OSA to alleviate hypoxia or apnea during sleep, are helpful for ameliorating neuropathological changes and slowing cognitive decline in AD patients.
This study comprehensively evaluated objective sleep quality via PSG in patients with AD and aMCI and focused on its correlations with learning and memory abilities, which are the earliest and most prominent symptoms in patients with typical AD. However, there are several limitations to this study. First, our study included a small number of patients, although the sample size was sufficient to detect significant differences. In addition, given that participants who consented to an overnight PSG might be more likely to have sleep complaints, there was a possibility of selection bias, which could hinder the interpretation of the current findings in the context of real-world conditions. Second, objective measures of sleep disturbance were assessed only by one-night PSG, which may have been influenced by occasional conditions, such as a delayed sleep latency, although we attached the PSG device 4–6 h before participants’ bedtime to allow them to adapt. Third, all the patients included in this study, especially patients with aMCI, whose etiology might be heterogeneous, were diagnosed clinically, without pathological or biomarker confirmation. Biomarkers (e.g., amyloid and tau in the cerebrospinal fluid or measured by PET) are suggested to enhance diagnostic precision in future research. Finally, since this was a cross-sectional study, the causal relationship between sleep disturbance and memory impairment could not be determined. Longitudinal studies are needed to confirm the causal relationship between sleep disturbances and cognitive decline in persons on the AD continuum.
In conclusion, our findings suggest that sleep disturbances persist early in the pathological process of AD and might contribute to the initial symptoms of episodic memory impairment. PSG, as an effective tool for the comprehensive evaluation of sleep disorders, is useful in screening, evaluating and monitoring AD.
Footnotes
Acknowledgments
The authors thank the participants for their supports during the study.
Authors contributions
Linyang Cui (Conceptualization; Data curation; Methodology; Writing – original draft); Yahui Wan (Formal analysis; Writing – original draft); Yunyao Lu (Data curation); Meng Meng (Investigation); Nan Zhang (Conceptualization; Methodology; Project administration; Resources; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Science and Technology Innovation 2030—Major Project (2021ZD0201805) and the Tianjin Key Medical Discipline (Specialty) Construction Project (grant number TJYXZDXK-004A).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available upon request from the corresponding author. The data are not publicly available.