
Abstract
Background
Cognitive impairments have been reported among disadvantaged populations.
Objective
We aimed to ascertain how demographic factors are associated with cognitive performance in individuals enrolled in a local substance abuse recovery program.
Methods
In total, 106 participants were included in the study. Besides demographic information, vital signs and cognitive function, measured by Mini-Mental State Examination (MMSE) or Montreal Cognitive Assessment (MoCA), were collected from each participant. Welch's t-test and regression analysis were used to analyze how different demographic factors are associated with cognitive assessment scores.
Results
The mean age of African American (AA) participants (n = 43) were 48.35 ± 1.65 years, which are older than that for the White participants of 38.95 ± 1.36 (n = 63) years. Compared to the AA participants, the White participants had a larger variance in attained education levels. The average MMSE scores were 27.09 ± 0.40 for AA participants, which is lower than that for the White participants of 28.52 ± 0.33 (p < 0.05). The average MoCA scores were 23.71 ± 0.54 for AAs, which is lower that for the White participants of 26.65 ± 0.44 (p < 0.001). The AA and White participant groups had cognitive impairment rate of 18.6% and 6.35%, respectively. The regression analysis indicates age and education are two significant predictors for the cognitive performance difference between the two racial groups.
Conclusions
Significant disparities in cognitive performance exist between two racial groups of enrolled in a local substance abuse recovery program. The older age and lower levels of attained education in AA participants can explain the poorer cognitive function than the White participants.
Introduction
According to the 2023 Annual Homelessness Assessment Report (AHAR), 1 there are 653,100 individuals (∼0.2%) in the United States experiencing homelessness. Based on the Point-In-Time (PIT) count, which have been conducted in each January since 2007, the Department of Housing and Urban Development (HUD) released the 2023 count for being the highest. 1 In the State of Alabama alone, about 7 in every 10,000 (0.07%) people experience homelessness. Of those who experiencing homelessness in Alabama, more than 50% are unsheltered. 1 Participants of this study were recruited from a Fellowship House located in Birmingham, Alabama. The Fellowship House is a recovery program that provides housing for individuals who have a history of substance abuse. 2 As a residential program, the Fellowship House provides multi-modes of services such as food, laundry, medical services, and more.
Cognitive function is a critical aspect of human health, encompassing episodic memory, processing speed, global cognition, verbal fluency, crystallized intelligence, and fluid intelligence. 3 Cognitive impairment is widely recognized and varied, which can lead to occupational, social, and/or functional disabilities.4,5 Previous studies reported a high prevalence of cognitive difficulties, substance use, and chronic conditions among people experiencing homelessness.5–7
It has been reported that cognitive performance can vary significantly across individuals due to various factors including age, education, and ethnicity. For instance, previous research has identified a significant prevalence of cognitive impairment among adults who have experienced homelessness. In addition, there is evidence indicating that such impairments can manifest at a younger age compared to the general public.8–11 Furthermore, education has been linked to a slower age-associated decline in some cognitive skills in some studies11–14; nonetheless, other studies report this association as either negligible 3 or nonlinear and sex-biased. 12 Conversely, recent data suggest that the male sex is associated with a higher risk for developing age-associated cognitive impairments than the female sex. 15 Furthermore, there is some evidence of racial and ethnic disparities in cognitive impairment, with the prevalence reported as being higher among African Americans compared to the White participants.16,17
Despite some work having been done,18,19 there is limited research on the cognitive performance of disadvantaged individuals and how it may vary based on demographic factors such as ethnicity, education, and age. There is therefore a dire need to fully identify the factors associated with cognitive impairment among the disadvantaged population. Thus, this study aimed to investigate cognitive impairment among individuals who enrolled in a substance abuse recovery program located in Birmingham, Alabama, with a specific focus on potential differences based on age, education, and ethnicity. By examining the relationships between cognitive performance and various demographic factors, we aim to identify key predictors of cognitive impairment which will be crucial for developing targeted interventions to improve cognitive health and overall well-being of disadvantaged populations.
Methods
This study was approved by the University of Alabama at Birmingham Institutional Review Board (IRB#: 300007866). This research study is sampling from a local residential substance abuse recovery program. Specifically, our participants are from the Fellowship House that is for people who have a substance abuse history and look for a sober and healthier lifestyle. The Fellowship House has the following admission criteria: (1) have no income or insurance; (2) must provide a current assessment or history and physical with an axis I substance dependence diagnosis; (3) must not currently be in physical withdrawal from any substance. Thus, the participants of our study are at the same level of socioeconomic status and qualified for being in the recovery program.
An “open-door clinic” style was adopted as our recruitment strategy, where anybody who can communicate in English and being an adult were invited to participate in our study. They can walk in anytime when our team was on site to collect data. The exclusion criteria are: (1) Individuals who have hypertension with systolic blood pressure higher than 180 mmHg; (2) Individual who could not read or understand English; (3) Individuals who have severe mental illness(es) or known medical conditions related to cognitive impairments (for example, those with a history of alcohol related cognitive impairment including Wernicke's encephalopathy and traumatic brain injury). At the very beginning of our study procedure, one of the team members would explain the details of the consent form and help them to understand the study purpose and what is expected.
Each participant's vital signs were measured (blood pressure, heart rate, respiration rate, body temperature) after their consent was obtained. This study measured the participants’ cognition using two assessment tools: Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE). They are the two most used tools to evaluate cognitive function. 20 Although the two assessment tools share some features, the MoCA was found to be more sensitive than MMSE for detecting mild cognitive impairment. 20 Both assessments are scored on a scale of 0–30. The cutting-off scores for mild cognitive impairment are 27 and 23 for MMSE and MoCA, respectively. 20 If the participant's education level were less than a high school degree, then one point would be rewarded for the MoCA score. In addition, a 10-panel drug screen (amphetamines, THC, cocaine, opiates, phencyclidine, barbiturates, benzodiazepines, methaqualone, methadone, and propoxyphene) was performed with collected blood samples.
Multiple comparisons of the characteristics or outcomes between the African American participants and the White participants were conducted by using descriptive statistics and Welch's t-test. The results are displayed in Table 1 and Supplemental Figures 1 and 2. Means with standard deviation (S.D.) were also used to describe the data. The boxplots demonstrate graphically the distribution of the data in the study, where the median for each dataset is indicated by the black center line, and the first and third quartiles are the edges of the box, which is known as the interquartile range (IQR). The Welch's t-test at α = 5% significance level was used to compare the mean difference of each investigated characteristic or outcome. Logistic regression was used to model a binary outcome variable as a linear function of the predictor variables. In this case, the category of cognitive impairment is coded as 1 and the normal category is coded as 0 in the model.
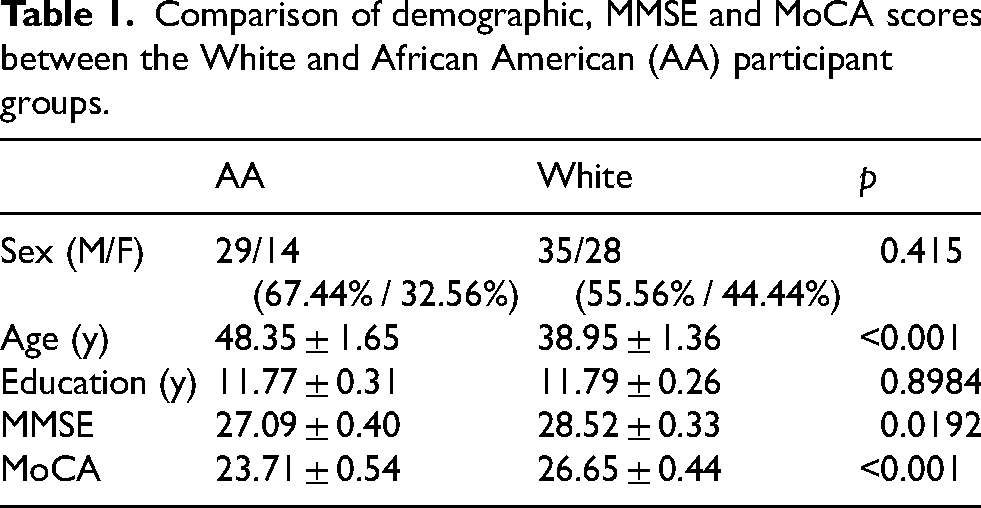
Comparison of demographic, MMSE and MoCA scores between the White and African American (AA) participant groups.
Results
Overall, 106 subjects were recruited from September 1, 2023 to April 3, 2024. Regarding to Sex, there are 64 males (35 AA participants and 29 White participants) and 42 females (14 AA participants and 28 White participants). For all participants, the drug/substance use positive rate is around 7% based on our 10-panel drug screening test.
Regarding race, 63 participants identified as White, 43 participants identified as African Americans. For attained education level, 73 participants achieved a high school diploma or above.
The median age of the 106 participants is 42 years (IQR: 33.0–53.0), ranging from 21 to 67 years. A median education level of 12 years (IQR: 11–13), ranging from 6 to 16 years. The MMSE scores for the entire study participants range from 14 to 30 with a median score of 29 (IQR: 27–30). The median MoCA score was 26 (IQR: 23.0–29.0), ranging from 15 to 30.
Correlation analysis revealed a moderate positive correlation between MMSE and MoCA scores (r = 0.524), a weak negative correlation between age and both MMSE scores (r = −0.296) and MoCA scores (r = −0.345) but a positive correlation between educational level and MMSE scores (r = 0.237) and MoCA scores (r = 0.242).
Detailed comparisons of demographic characteristics along with MMSE and MoCA scores between the White and AA participants are presented in Table 1 and Supplemental Figures 1–4.
From Table 1, the participants consisted of 43 AA individuals (67.44% male, 32.56% female) with an average age of 48.35 years (SD = 1.65), and 63 White individuals (55.56% male, 44.44% female) with an average age of 38.95 years (SD = 1.36). For both groups, there were more men than women. The AA participants were, on average, 10 years older than the White participants. The Chi-square test with p-value 0.415 indicated that there was no statistically significant association between sex and ethnicity (Table 1). Supplemental Figure 1 shows the boxplot (a graph of the five-number summary: minimum, first quartile, median, third quartile and maximum) comparing the ages of the two groups. The ages were in general older for the AA participants than the White participants (Supplemental Figure 1). The medians and both quartiles were all larger for the AA participants than the White participants.
Education levels were similar across both groups, with an average of approximately 11.77 years for the AA participants and 11.79 years for the White participants. However, the education levels of the White participants were more variable as shown by a large IQR ranging from 10.5 to 14 years. On the other hand, the AA participants had a narrower education range (11 to 12 years) (Supplemental Figure 2). For the AA participants, 75% had an education level at or below 12, and almost all had an education level below 13. For the White participants, 50% had an education level 12 or above, with 25% having an education level above 14.
The comparisons of the cognitive assessments MMSE and MoCA (Table 1 and Supplemental Figures 3 and 4) indicated the significant differences between the two groups. The average MMSE scores were 27.09 (SD = 0.40) for AA individuals and 28.52 (SD = 0.33) for White individuals. The average MoCA scores were 23.71 (SD = 0.54) for AA individuals and 26.65 (SD = 0.44) for White individuals. In addition, the Welch's t-tests with a p-value 0.0192 for MMSE and a p-value less than 0.001 demonstrated the significant differences in cognitive performances between AA and White participants. Lastly, the White participants had higher MMSE and MoCA scores for than those for the AA participants evidenced by higher medians and both quartiles (Supplemental Figures 3 and 4).
To generate the magnitude of demographic effects to the cognitive assessments, we conducted a multiple regression analysis to predict the MMSE and MoCA scores from two predictors: age and education. The results were shown in Tables 2 and 3. It was noted that both predictors were statistically significant with p-values less than 0.001in both multiple regression models. The coefficients indicate that older people tend to have lower MMSE and MoCA scores accounting for the other controlled variable: education. Reversely, more educated people have higher MMSE and MoCA scores.
Multiple linear regression modelling MMSE on age and education.

*p < 0.05; **p < 0.01; ***p < 0.001.
Multiple linear regression modelling MoCA on age and education.
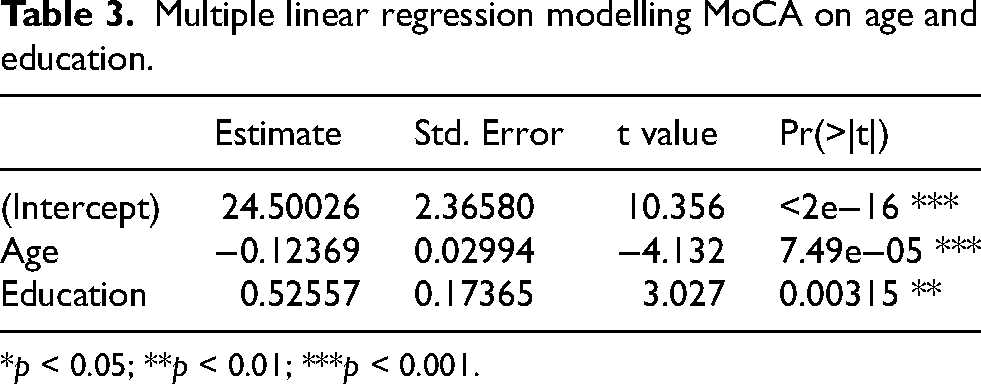
*p < 0.05; **p < 0.01; ***p < 0.001.
Acknowledging the mean age differences between the AA and White groups in the sample, we examined the interactive effects of age and ethnicity on MMSE and MoCA scores. The results are presented in Tables 4 and 5. Regression models indicate that age is a significant predictor of both MMSE and MoCA scores, with p-values of 0.00508 and 0.0156, respectively. However, the sample data does not provide sufficient evidence to suggest an interaction between age and ethnicity as covariates influencing cognitive performance.
Multiple linear regression modelling MMSE on age and ethnicity.
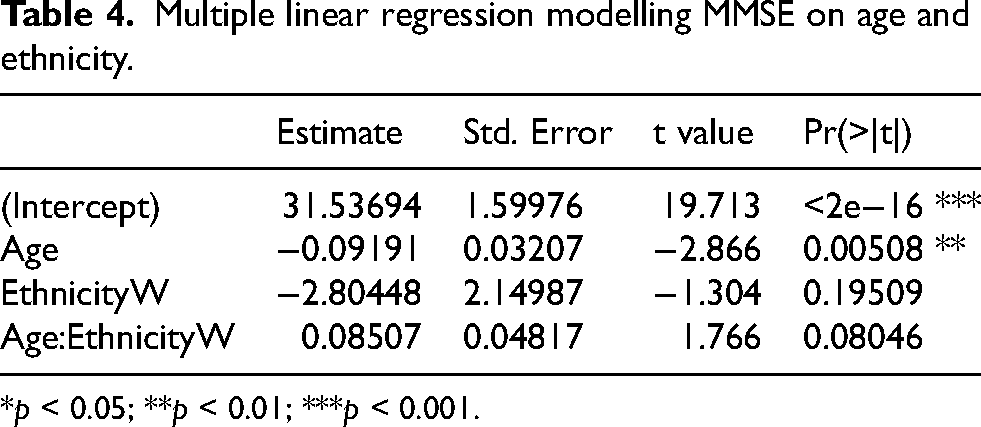
*p < 0.05; **p < 0.01; ***p < 0.001.
Multiple linear regression modelling MoCA on age and ethnicity.
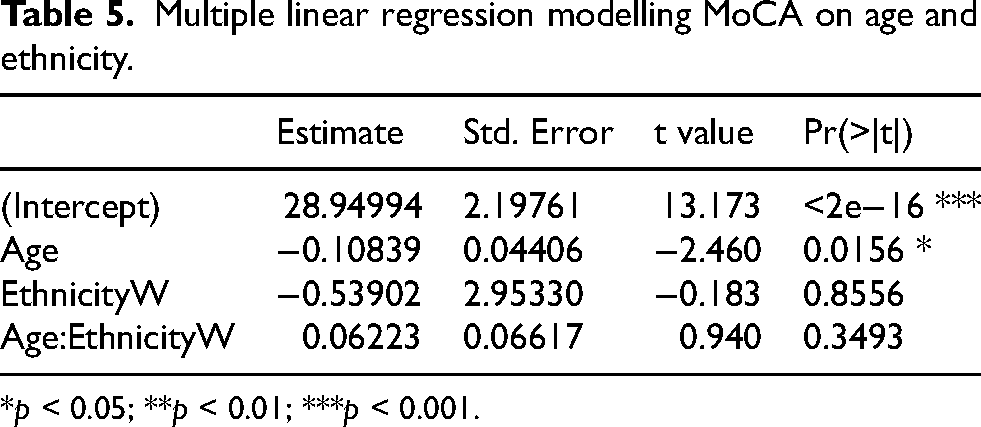
*p < 0.05; **p < 0.01; ***p < 0.001.
Furthermore, we extended the study to identify cognitive impairment by utilizing a logistic regression model. 21 In the study, we defined the classification of cognitive impairment based on the criteria of MoCA scores of 23 or lower and MMSE scores of 27 or lower, respectively. Based these criteria, the prevalence of cognitive impairment was 18.6% and 6.35% in the AA participant and the White Participant groups respectively. The model included variables of Sex, Ethnicity, Age, Education, Systolic blood pressure, Diastolic blood pressure, Heart Rate, and Temperature. The statistical reports are shown in Tables 6 and 7.
Logistic regression modelling cognitive impairment based on MMSE score.
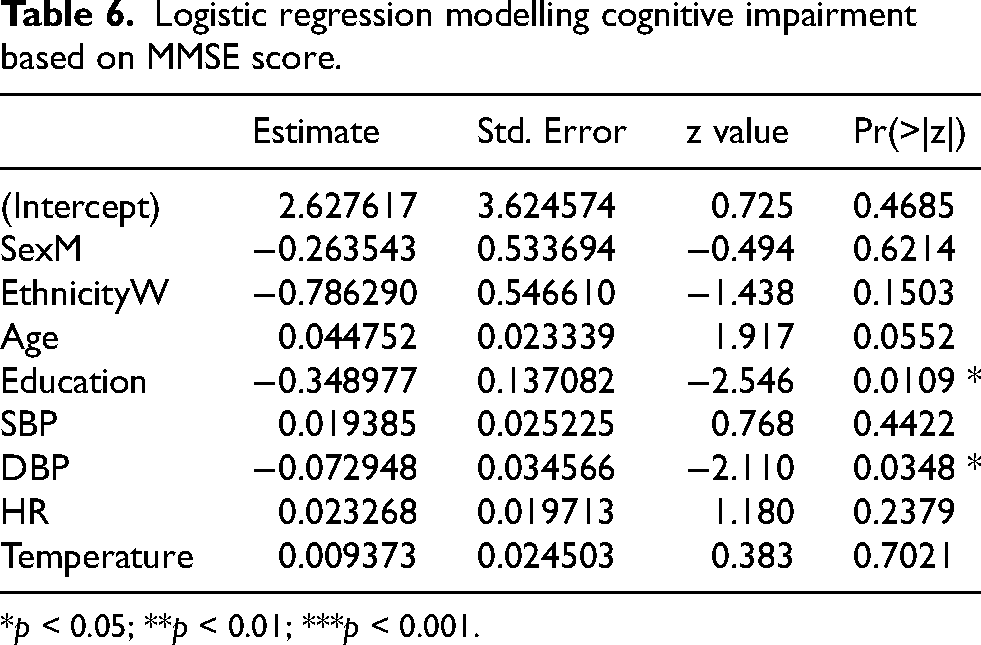
*p < 0.05; **p < 0.01; ***p < 0.001.
DBP: diastolic blood pressure; HR: heart rate; SBP: systolic blood pressure.
Logistic regression modelling cognitive impairment based on MoCA score.
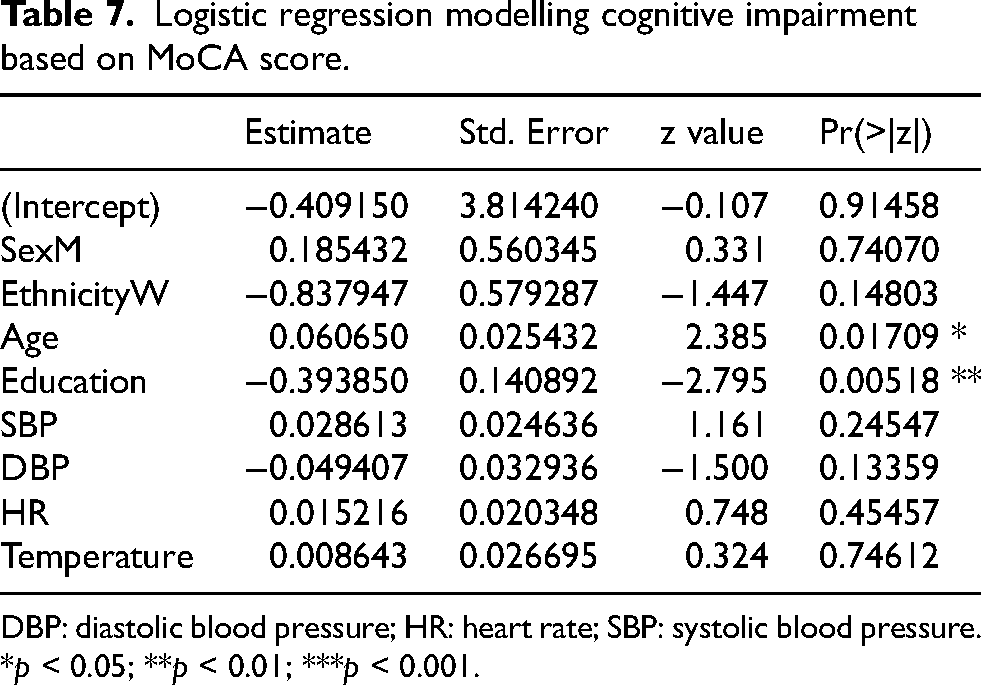
DBP: diastolic blood pressure; HR: heart rate; SBP: systolic blood pressure.
*p < 0.05; **p < 0.01; ***p < 0.001.
The logistic regression analysis showed that Age and Education were two significant predictors among all included predictors to predict individuals falling in the category of cognitive impairment. In the model of MoCA, age had a positive coefficient of 0.06065 (p = 0.01709), indicating that older age is associated with higher odds of having a MoCA score 23 or below. Education had a negative coefficient of −0.39385 (p = 0.00518), suggesting that higher education levels are associated with lower odds of having a MoCA< or =23. Other variables such as sex, ethnicity, systolic/diastolic blood pressure, heart rate, and temperature were not statistically significant.
Similarly, the analysis showed that age and education were significant predictors to identify cognitive impairment in the model of MMSE. Age had a positive coefficient of 0.04475 (p = 0.0552), indicating that older age has a trend to be associated with higher odds of having an MMSE score 27 or below. Education had a negative coefficient of −0.3490 (p = 0.0109), suggesting that higher education levels are associated with lower odds of having an MMSE score 27 or below. In addition, diastolic blood pressure was found to be associated with MMSE with a coefficient of −0.07295 (p = 0.0348).
Discussion
Our study aimed to investigate cognitive impairment in individuals from a substance use recovery program in Birmingham, Alabama, with a focus on potential differences based on ethnicity, age, education, and other factors. Based on our recruitment strategy and sampling process, the analyzed sample can well represent the population. Our findings underscore the significance of demographic factors, particularly age and education, in cognitive performance. This study provides critical insights into the cognitive health disparities among disadvantaged individuals, thereby highlighting the need for targeted interventions.
Our results revealed that age is a significant predictor of cognitive performance. Older age was associated with higher odds of lower cognitive scores. This finding is consistent with previous studies. According to a study by Hurstak, et al., 22 among a cohort of homeless adults, the proportion of cognitive impairment in the older participants was higher than in the younger participants. Brown et al. 8 found that cognitive impairment was more prevalent among the older homeless adult population than the general population. In another cross-sectional study of older adults who first experienced homelessness after age 50, neurocognitive assessment revealed significant deficits commonly among older homeless adults. 23 This association could be due to several reasons including malnutrition, social isolation, and violence towards older homeless adults. Older homeless adults had been shown to be at higher risk of malnutrition due to food insecurity, low income, and limited access to resources. 24 Older homeless adults also often experience significant social isolation and lack of community connections. 25 Additionally, older homeless adults are vulnerable to violence and abuse, which can cause chronic stress and trauma,26,27 negatively impacting cognitive function. All these factors might be involved with the poor cognitive performance in the disadvantaged individuals.
With our study cohort, the correlation coefficient between MMSE and MoCA is 0.524, which indicates a moderate positive correlation. The correlation coefficient is lower than what has been reported before.28,29 Our results also indicate significant differences in cognitive performance between AA and White participants. AAs scored lower on both the MMSE and the MoCA compared to their White counterparts. Specifically, the average MMSE and MoCA scores for AA participants were 5% and 11% lower than those for White participants, respectively. These findings align with previous reports that identified racial or ethnic disparities in cognitive impairment.16,17,22 Indeed, Lin et al. 30 found that AA participants’ scores on cognitive tests were 2.3 points lower than White participants’ scores, and AA participants were also more than twice likely as White participants for having cognitive impairment. It is thus not surprising that, according to the Alzheimer's Association, AA older adults are about two times more likely to develop mental/brain-related diseases like Alzheimer's disease or other forms of dementia as White older adults. 31 The racial disparities in cognitive function may be attributed to several factors, including socioeconomic status, access to education, and healthcare inequalities. Evidence suggests that AAs are more likely to experience socioeconomic disadvantages,32,33 which can adversely affect cognitive development and functioning. Furthermore, systemic barriers in healthcare access and inequality in health care quality may contribute to these disparities.34,35 Additionally, aging is associated with decreased cognitive performance. In our study, we found that the AAs in our study were significantly older than their White counterpart group. Our findings highlight the need for further research to understand how aging interacts with racial disparities in cognitive function.
Our study also identified education as a significant factor in cognitive performance. Higher education levels were associated with better cognitive scores. This is expected since higher educational attainment is associated with greater cognitive reserve.14,36 On the other hand, participants who score lower on cognitive assessment are likely to have lower educational attainment. 22 Langella et al. 37 also found that educational attainment is protective and moderates the pathogenic effect of the ɛ4 allele of the apolipoprotein E (APOE) gene, an allele which has been associated with an increased risk for developing Alzheimer's disease and an earlier age of clinical onset than for individuals without an ɛ4 allele. It is, however, noteworthy that the timing of education is also critical. Evidence suggests that high early-life educational attainment is significantly associated with higher cognitive function compared to those with later-life high educational attainment. 13 Ensuring access to educational opportunities can be a crucial strategy in mitigating cognitive impairment, maintaining cognitive reserve, and promoting overall well-being. These findings underscore the need for educational interventions and programs that support lifelong learning, which can be protective for cognition. Moreover, the effects of educational attainment might be different between AAs and White individuals. To prevent cognitive disparities, there is a need to go beyond racial inequality in access to education and minimize diminished returns of educational attainment for minorities. 38
Overall, our findings have important implications for intervention and policy. The significant disparities in cognitive performance based on ethnicity and attained education highlight the need for targeted interventions that address the specific needs of these subgroups. Interventions should focus on providing comprehensive cognitive assessments and tailored support services that consider the unique challenges faced by disadvantaged groups. The protective role of education against cognitive decline suggests that educational programs and policies that enhance access to education and promote lifelong learning can be effective strategies in mitigating cognitive impairment. This includes initiatives that provide educational opportunities for individuals experiencing homelessness, such as adult education programs and vocational training. Finally, addressing the social determinants of health, including socioeconomic status and healthcare access, is crucial in reducing cognitive health disparities. Policies that aim to reduce societal inequities and takes measures to prevent homelessness can have a significant impact on their cognitive health and overall quality of life.
While this study provides valuable insights into factors associated with cognitive impairment among disadvantaged adults, it is worth indicating that the sample size is relatively small, and the study is cross-sectional, limiting the ability for generalization and causality inferences, respectively. Future research should consider longitudinal studies with larger sample sizes to validate these findings and investigate age and/or education as predicting factors for cognitive performance on the domain level: memory, language or executive functions. Additionally, while this study employed MMSE and MoCA as cognitive assessment tools, future research could incorporate other cognitive measures as well as explore the impact of additional factors such as mental health status, substance use, and trauma history on cognitive performance. Since our study sample came from a substance abuse recovery program, detailed information about the substance use history and how is associated with the current cognitive performance are also worthy to be investigated in the future.
Conclusion
This study highlights significant disparities in cognitive performance among disadvantaged individuals in Birmingham, Alabama, particularly between two races: White and AA. Our findings indicate that AA participants have lower cognitive performance compared to their White counterparts, revealing both age and educational attainment are important factors for explaining the cognitive disparities observed between these two racial groups. These disparities underscore the importance of developing policies and programs that promote access to education and healthcare specifically for the disadvantaged individuals. By addressing these specific needs, cognitive health and overall well-being of the disadvantaged individuals and, ultimately their quality of life, can be improved.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251328239 - Supplemental material for Demographic predictors of cognitive performance in participants of a local substance abuse recovery program
Supplemental material, sj-docx-1-alr-10.1177_25424823251328239 for Demographic predictors of cognitive performance in participants of a local substance abuse recovery program by Ge Wang, Huijun Yi, Daniel Y Li, Elizabeth J Arnold, Damien C Bynum, Isaiah Chamoun, Jordie Johnson, Runze Ma, Shelby A Sliman and Wei Li in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgments
This study was funded by the University of Alabama at Birmingham, School of Health Professions, Honors Program Mentor Award. This work was also supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $1,492,465 with 0% financed with non-governmental sources (Award number: 1D57HP40200-01-00). The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.
Ethical considerations
This study was approved by the University of Alabama at Birmingham Institutional Review Board (IRB#: 300007866).
Consent to participate
Written consent form was signed by every participant.
Consent for publication
All participants agreed for publishing their deidentified data.
Author contributions
Ge Wang (Conceptualization; Formal analysis; Investigation; Methodology; Software; Validation; Writing – original draft; Writing – review & editing); Huijun Yi (Formal analysis; Investigation; Methodology; Software; Visualization; Writing – original draft; Writing – review & editing); Daniel Y Li (Formal analysis; Investigation; Methodology; Software; Validation; Visualization; Writing – original draft; Writing – review & editing); Elizabeth J Arnold (Data curation; Investigation; Methodology; Project administration; Resources; Writing – review & editing); Damien C Bynum (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Visualization; Writing – original draft; Writing – review & editing); Isaiah Chamoun (Data curation; Formal analysis; Investigation; Methodology; Resources; Visualization; Writing – original draft; Writing – review & editing); Jordie Johnson (Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Writing – original draft; Writing – review & editing); Runze Ma (Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Writing – original draft; Writing – review & editing); Shelby A Sliman (Data curation; Formal analysis; Investigation; Methodology; Resources; Software; Writing – original draft; Writing – review & editing); Wei Li (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing – original draft; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $1,492,465 with 0% financed with non-governmental sources (Award number: 1D57HP40200-01-00).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data and data analyses are available upon reasonable request by the following the guideline of University of Alabama at Birmingham.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.