
Abstract
Background
There is increasing evidence suggesting a correlation between neurodegenerative diseases (NDDs) and constipation; however, their genetic relationship and causal mechanisms remain inadequately elucidated.
Objective
We aim to investigate the causal link and shared genetic basis between NDDs and constipation.
Methods
We obtained summary statistics from large-scale genome-wide association studies, encompassing five NDDs, including Alzheimer's disease (AD), Parkinson's disease (PD), multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), Lewy body dementia (LBD), as well as constipation. The primary analysis employed five Mendelian randomization methods to evaluate causal effects, while linkage disequilibrium score regression (LDSC) and high-definition likelihood (HDL) were utilized to investigate genetic correlations. Additionally, significant pleiotropic SNPs were identified using pleiotropic analysis under the composite null hypothesis (PLACO) and functional mapping and annotation (FUMA). Finally, enrichment analysis was conducted to explore the biological pathways associated with the identified pleiotropic genes.
Results
MR analysis revealed a significant causal relationship between AD and an enhanced risk of constipation was demonstrated (OR = 1.043, 95% CI: 1.015–1.073, p = 0.003), while no causality was found between PD, MS, ALS, LBD, and the risk of constipation (p > 0.05). LDSC and HDL analysis revealed a significant positive genetic correlation between AD and constipation. Using PLACO combined with FUMA, we identified 30 overlapping pleiotropic loci, with pathway enrichment analysis revealing important biological pathways related to Aβ metabolism and processing, tau protein process, and the complement and coagulation cascades.
Conclusions
Our study indicates that AD is a contributing factor to constipation and uncovers the complex genetic mechanisms linking AD and constipation, which holds significant implications for diagnosis and treatment of both conditions.
Introduction
In various neurodegenerative diseases (NDDs), including Alzheimer's disease (AD), Parkinson's disease (PD), multiple sclerosis (MS), amyotrophic lateral sclerosis (ALS), and Lewy body dementia (LBD), gastrointestinal dysfunction is evident throughout all stages of disease progression and has become an integral component of their clinical manifestations, with constipation being one of the most typical symptoms.1,2 Recent studies have revealed that the central nervous system and gut biology mutually regulate each other's functions through gut-brain connecting neurons, with NDDs causing persistent gut dysfunction, while gut neurons and gut physiology are involved in the pathogenesis of NDDs. 3 This indicates a potential genetic link and shared biological mechanism between NDDs and constipation. However, to our knowledge, few studies have investigated the shared genetic etiology between NDDS and constipation. Thus, analyzing their common genetic risk loci from a genetic perspective may be beneficial for disease management.
NDDs encompass a wide spectrum of neurological conditions, marked by a progressive deterioration in both the structure and function of the central or peripheral nervous system. 4 This decline develops into multiple dysfunctions such as dementia and ataxias, eventually progressing towards disability and death. The global impact of dementia alone is profound, while it has cost $1 trillion and is predicted to affect 130 million people by 2050. 5 Among NDDs, AD is the most widespread type, which affects approximately 20% of women and 10% of men and accounts for 70% of dementia cases across the globe. Meanwhile, as the second most common NDD, PD has been estimated to impact over 6 million people worldwide. 6 The global prevalence of NDDs will grow with increasing life expectancy, posing rising challenges for public health and the social economy.7,8 Additionally, patients with these NDDs are often troubled by constipation, which significantly impacts their quality of life. 9 Therefore, elucidating the causal relationship and shared genetic etiology between NDDs and constipation may help improve disease management and enhance patients’ quality of life.
Constipation is a prevalent gastrointestinal disorder that has a significant impact on patients’ quality of life and imposes considerable demands on healthcare systems globally. 10 Typical symptoms of constipation include hardened stools, excessive straining, rare defecation, bloating, and abdominal discomfort. Apart from reducing the quality of life, constipation may also enhance the risk of cardiovascular and kidney diseases in patients, which is thought to be mediated by alterations in the gut microbiota. 11 The latest research reveals that constipation has a global prevalence of 14% and the rate escalates with age, 12 which places a heavy financial burden on healthcare systems. In the United Kingdom, the annual cost related to constipation has reached £162 million, while in the United States, it amounts to $ 6.9 billion per year.13,14 Thus, it is imperative to prioritize the prevention and early management of constipation. Some factors are recognized as causes of constipation, including abnormal intestinal structure, neurological disorders, metabolic disturbances, and medications. 15 Recently, several studies have focused on the relationships between NDDs and constipation. Two reviews reported that constipation could be triggered by PD and MS. 16 Another research proposed that constipation was a common gastrointestinal feature of PD. 17 What's more, a combined case-control and cohort study found that constipation significantly increased the risk of PD compared with AD, 18 while a retrospective study indicated that constipation could accelerate cognitive impairment in patients with AD. 19 Although existing clinical research have shown a correlation between NDDs and constipation, the causal relationship and genetic overlap between the two require further exploration.
We recognize that existing studies on the genetic associations between NDDs and constipation have certain limitations. Studies have shown that certain NDDs are associated with gut-brain axis. For instance, PD patients often exhibit constipation years before the onset of motor symptoms, while gut dysfunction in AD may accelerate cognitive decline.20,21 However, to the best of our knowledge, no studies have systematically investigated the genetic associations between MS, ALS, or LBD and constipation. The unclear causal relationship and genetic overlap between warrant further exploration. Secondly, observational studies may have uncontrolled confounding factors, such as dietary patterns and medication use, which could obscure the true association between NDDs and constipation. Additionally, while randomized trials (RCTs) are considered the gold standard for establishing causal relationships, their implementation is often costly and time-consuming. Therefore, to gain a more comprehensive understanding of relationship between NDDs and constipation, there is an urgent need fore large-scale, standardized studies combined with advanced statistical tools to uncover their shared genetic etiology and potential causal mechanisms. Notably, Mendelian randomization (MR) is a novel approach for investigating causalities between diseases and other factors, which employs randomly allocated single nucleotide polymorphisms (SNPs) during meiosis as instrumental variables (IVs) to avoid the disturbance from confounders and reverse causation. 22 Consequently, MR serves as an ideal design for exploring causal associations between NDDs and constipation.
In this study, we aim to investigate the causal associations and overlap between various NDDs (AD, PD, MS, ALS, and LBD) and constipation. We employed a two-sample MR approach based on large-scale genome-wide association study (GWAS) data to evaluate the bidirectional causal relationship between NDDs and constipation. In addition, we used various genetic analysis tools to identify genetic associations between different diseases, shared pleiotropic loci, and related pathways (

An overview of the study design.
Methods
GWAS data for NDDs
In this study, five typical NDDs, including AD, PD, MS, ALS, and LBD, were selected as study objects. The criteria for our preliminary screening of GWAS data was the European background and as large a sample size as possible, thereby laying a strong foundation for reliable MR analysis. Specifically, the GWAS datasets for five NDDs were as follows: (1) The AD GWAS summary dataset was from the published study in 2022, which includes 39,106 AD cases and 46,828 controls. 23 (2) The PD GWAS summary dataset was from Nalls et al. and involved 33,647 cases and 499,506 controls. 24 (3) The MS GWAS summary dataset was derived from MS published by the International Multiple Sclerosis Consortium, involving 47,429 cases and 68,374 controls of European descent. 25 (4) The ALS GWAS summary dataset was obtained from Project MinE, including 27,205 cases and 110,881 controls. 26 (5) The LBD GWAS summary dataset was obtained from a published genome-wide association study, including 2591 cases and 4027 controls 27 (Table 1).
Detailed information on the studies and datasets used for Mendelian randomization analyses.

To validate our results by conducting replication analysis and meta-analysis, we used additional datasets for AD, PD, MS, ALS, and LBD. Specifically, for AD, the data were from the GWAS Catalog (42,034 AD patients and 272,244 controls); for PD, the data were from the US National Institute of Neurological Disorders AND Stroke (NINDS; 1713 PD patients and 3.978 controls); for MS, the data were from the International Multiples Sclerosis Genetics Consortium (IMSGC; 14,498 MS patients and 24,019 controls); for ALS, data were from the International Amyotrophic Lateral Sclerosis Genomics Consortium (IALSC; 20,806 MS patients and 59,804 controls); and for LBD, data were from a published genome-wide association study (1180 LBD patients and 657 controls).
GWAS data for constipation
The constipation GWAS summary data were obtained from the FINNGEN. 28 In total, there were 41,124 constipation cases and 371,057 control cases. Additionally, this study also used the constipation dataset from the IEU OpenGWAS project (15,902 constipation patients and 24,019 controls) for further replication analysis and meta-analysis. Constipation was diagnosed with ICD-10 code as K590. A complete list of all the genetic datasets used in this study is displayed in Table 1.
Instrumental variable selection
First, SNPs that had a strong link with NDDs from GWAS (p < 5 × 10−8) were chosen as IVs. For MS as an exposure factor, a more permissive threshold (p < 5 × 10−7) was employed to select IVs to identify more causal relationships. Besides, during reverse causality validation, the threshold at p < 5 × 10−6 was adopted to determine the presence or absence of reverse causation more accurately. After deleting SNPs in linkage disequilibrium (r2 < 0.001 or distance >10,000 kb), the lead SNPs attained genome-wide significance. 29 Secondly, SNPs that were related to confounders and outcomes were excluded. In order to alleviate bias arising from the use of weak instruments, F statistics were computed for each SNP to evaluate the statistical strength, as previously described. 30 The SNPs with F statistics F < 10 were considered weak instruments and removed from MR analysis. The F statistics were calculated by taking into account the variance in exposure explained (R2) by SNPs for each exposure, using the formula [(N-K-1)/K × R2/(1-R2)], where K represents the number of SNPs and N denotes the sample size. 31 Third, MR-PRESSO models were utilized to detect outliers, and then the detected outliers were eliminated, followed by re-analyzing the remaining SNPs. 32
MR analysis and sensitivity analysis
A bidirectional two-sample MR analysis was conducted on the collected GWAS data, following the harmonization of the effect allele across the GWASs of exposure. The main analysis method we selected was IVW MR with multiplicative random effects, 33 which involved the combination of the Wald ratio estimates for each SNP on the outcome. IVW could derive an aggregated causal estimate that effectively improved the significant statistical power. 34 With the random-effect IVW method, it was allowed to assume that all instruments are ineffective when the overall horizontal pleiotropy remains balanced. Four other additional methods, namely MR-Egger, WM, simple mode and weighted mode were also used and allowed for horizontal pleiotropy with a slightly diminished statistical capability compared to the IVW. The results were visualized using forest plots.
Furthermore, a range of supplementary sensitivity analysis methods were utilized. To represent potential horizontal pleiotropy, heterogeneity markers (Cochran, Q-derived p < 0.05) were employed, which were obtained from the IVW approach. 35 The intercept served as an indicator of directional pleiotropy (the existence of directional pleiotropy was considered when p < 0.05), which was derived from the MR-Egger regression analysis. 36 MR-Egger regression was conducted to test the pleiotropy, while leave-one-out (LOO) analysis was employed to assess if the MR estimate was driven or biased by any single SNP. 37
Then, in order to guarantee the robustness of our data's reliability, a replication of the IVW analysis was performed with an independent dataset of NDDs and constipation data from the IEU OpenGWAS project, followed by a meta-analysis using the Revised Manager random-effects IVW model.
Genetic correlation analysis
Linkage disequilibrium score regression (LDSC) 38 and high-definition likelihood (HDL) 39 methods were applied to evaluate genetic correlations between traits. The LD scores for LDSC were derived from European ancestry samples in the 1000 Genomes Project, which served as the reference panel. 40 For HDL, the reference dataset included 1,029,876 quality-controlled HapMap 3 SNPs. To ensure data quality, SNPs were filtered to exclude those with non-bipartite or stand-ambiguous alleles, lacking rs tags, duplicates, SNPs absent from 1000 Genomes Project or with mismatched alleles, SNPs within the MHC region (chromosome 6:28.5–33.5Mb) due to its complex LD structure, and those with a minor allele frequency (MAF) ≤ 0.01.
Cross-trait GWAS analysis
To investigate the potential pleiotropic genetic loci influencing both AD and constipation, this study performed a pleiotropy analysis under the composite null hypothesis (PALCO). The PALCO method identifies pleiotropic SNPs, revealing potential genetic correlations between these two traits. 41 First, we imported the raw GWAS data for each pair of traits, then calculated the product of the Z-statistics for genetic variants of each SNP in the data to test the null hypothesis. The PLACO method further constructs a null distribution for the test statistic, defining it as a mixture distribution. This allows each locus variant to be associated with either both traits or only one of them, thereby addressing potential non-independence issues
At each locus, we utilized the ‘PLACO’ function in the R package to compute PLACO statistics, including both t-palco and p-palco values. Using this method, we quantitatively analyzed the shared genetic variants between the two traits. To ensure significance, we applied a threshold filter, retaining only SNPs with p-value less than 5 × 10−8. These identified pleiotropic SNPs will provide new insights into the potential genetic mechanisms between AD and constipation, contributing to a deeper understanding of their shared genetic basis.
Functional mapping and annotation
To gain a deeper understanding of the genetic mechanisms, we conducted a systematic analysis using FUMA (functional mapping and annotation) to achieve functional mapping and annotation of genetic associations. FUMA consists of two primary functional modules: SNP2GENE and GENE2FUNC. Using PLACO analysis, we identified gene loci with p-value below 5 × 10−8 and subsequently performed functional mapping with the SNP2GENE module, setting a maximum mapping distance of 500 kb. To ensure the accuracy of the results, we used the default parameters of SNP2GENE, with an r2 threshold of 0.6 for independent significant SNPs and an r2 threshold of 0.1 for lead SNPs.
Results
Forward causal effect
In our MR analysis with NDDs as exposures and constipation as the outcome, 58, 23, 91, 12, and 6 IVs were obtained for AD, PD, MS, ALS, and LBD, respectively. Both the individual IVs’ F-statistics and the aggregate overall F-statistics exceeded 10, suggesting a minimal bias attributable to weak instrument variation. The MR estimates utilizing the inverse-variance weighted (IVW), weighted median (WM), MR-Egger,simple mode and weighted mode analyses for the causal effect of AD, PD, MS, ALS and LBD on the risk of constipation were presented in Figure 2 in detail. In Figure 3, scatter plots displayed the potential causal directions between five NDDs and constipation obtained from five MR methods. Specifically, when the line moved upward from its intersection with the Y-axis, a positive correlation was suggested. Conversely, the line shifting downward from left to right indicated a negative causal effect. As a result, the IVW analysis predicted a significant association between AD and an elevated risk of constipation (OR = 1.043, 95% CI: 1.015–1.073, p = 0.003). The WM, simple mode, and weighted mode estimates also exhibited the same causal direction, while the MR-Egger method did not yield substantial evidence of a causal association (OR = 1.024, 95% CI: 0.973–1.077, p = 0.372). However, according to the five MR analyses, neither PD, MS, nor ALS was found to be significantly correlated to constipation.

Mr estimates for the neurodegenerative diseases on the risk of constipation in the primary MR analysis.

Scatter plots of MR analyses for the causal association between neurodegenerative diseases and the risk of constipation.
To estimate the robustness and the potential bias of the above results, sensitivity analyses were executed to determine the existence of heterogeneity and pleiotropy, involving the Cochran's Q test, MR-Egger intercept test, and MR-PRESSO global test.42,43 The p values derived from Cochran's Q test and I2 shown in Supplemental Table 1 indicated the absence of heterogeneity, while intercepts from the MR-Egger analysis revealed minimal likelihood of horizontal pleiotropy. As displayed in Supplemental Figure 1, the results of the LOO analysis supported the non-existence of pleiotropy. Then the forest plots presented the effects of each SNP on the outcome and no outlier was found (Supplemental Figure 2). Additionally, in Supplemental Figure 3, the funnel plots showed that SNPs were mostly symmetrically distributed, indicating few possibilities of influences from potential bias.
To ensure the reliability of causal findings, the replication analysis was carried out utilizing another independent GWAS dataset, and the comprehensive meta-analysis was conducted with IVW estimates from both primary and replicated MR analyses. The integrated estimates from the meta-analysis in Figure 4 confirmed a statistically significant causal relationship between AD and a rising risk of constipation. As for the other NDDs, the meta-analysis results still indicated no causal association between PD, MS, ALS and LBD with constipation. Thus, the causal result of AD remained stable, and AD was demonstrated to causally enhance the likelihood of constipation (OR = 1.05, 95% CI: 1.03–1.06, p < 0.00001). Furthermore, there was no evidence of pleiotropy or heterogeneity found between AD and the risk of constipation, suggesting the robustness of the obtained MR estimate.

Meta-analysis of IVW results from primary and replication MR analysis for the causal association between neurodegenerative diseases and the risk of constipation.
Reversed causal effect
The causal effect analysis was conducted in the reverse direction, with constipation as the exposure and NDDs as the outcome. A significance threshold at p < 5 × 10−6 was set to facilitate the observation of reverse causality. In the primary analysis as shown in Supplemental Table 2, the results derived from IVW analysis revealed no evidence of a causal association between constipation and the risk of AD (OR = 0.988, 95% CI: 0.885–1.120, p = 0.946). What's more, no causal connection was found between constipation and the risk of PD (IVW: OR = 0.878, 95% CI: 0.617–1.249, p = 0.469), MS (IVW: OR = 1.094, 95% CI: 0.652–1.836, p = 0.735), ALS (IVW: OR = 1.000, 95% CI: 0.795–1.258, p = 1.000) and LBD (IVW: OR = 0.891, 95% CI: 0.287–2.773, p = 0.843). The detailed MR estimates derived from five MR approaches were displayed in Supplemental Figure 4. In sensitivity analysis (Supplemental Table 3), no heterogeneity was found in all five NDDs. Besides, there was no pleiotropy existing in all five NDDs. Subsequently, to confirm the causal result, we further conducted the replicated MR analysis and meta-analysis, which supported the absence of causality between constipation and the risk of five NDDs (Supplemental Figure 5).
Genetic correlations between AD and constipation
We utilized LDSC and HDL analysis to evaluate the genetic correlation between AD and constipation. The LDSC results showed a significant positive genetic correlation between AD and constipation (rg = 0.121, p = 0.0185), with the HDL analysis revealing similar findings (Table 2). These positive genetic correlations suggest the potential presence of underlying shared genetic mechanisms between AD and constipation. Consequently, we performed additional analysis to identify specific shared genetic loci.
Genetic correlation between AD and constipation.

rg refer to the genetic correlation coefficient.
Shared loci between AD and constipation
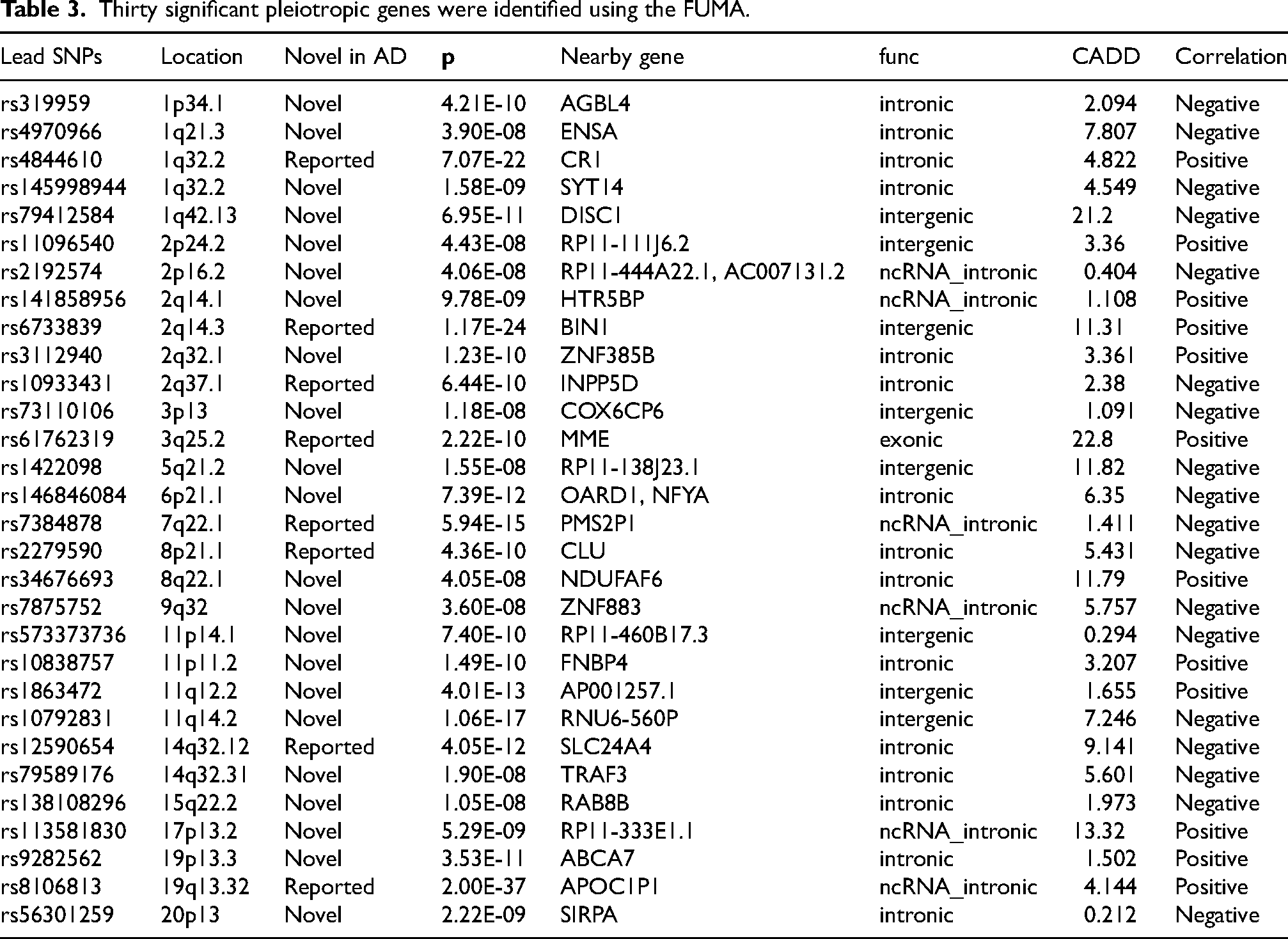
The conditional Q-Q plots showed successive increments in SNP enrichment for AD as a function of significant associations with constipation, suggesting polygenic overlap between AD and constipation (Figure 5). Using PLACO and subsequent FUMA analysis, we identified 943 quality-filtered pleiotropic SNPs, which mapped to 30 independent genomic risk loci across 14 distinct chromosomal regions (Table 3, Figure 6). Among the 30 pleiotropic loci associated with AD and constipation annotated by FUMA, 22 were newly identified for AD (Table 3). Subsequently, we analyzed the effect direction of the primary SNPs at each shared genomic locus. Among these 30 SNPs, 12 (40%) showed consistent associations, suggesting that these genetic variants may simultaneously influence the risk of both AD and constipation. In the other SNPs, we observed inconsistent associations, indicating potential multiple biological mechanisms (Table 3).

Conditional quantile-quantile plot. The dashed line represents the expected distribution under the null hypothesis, while the leftward deflection indicated the extent of pleiotropic enrichment.

Shared loci between AD and constipation. The Manhattan plot illustrated the relationship between each SNP's -log10 transformed p-value (y-axis) and its chromosomal position (x-axis). The red horizontal line represents the statistical threshold for significant shared associations.
Thirty significant pleiotropic genes were identified using the FUMA.
Functional mapping and annotation
The integrated functional annotation of candidate SNPs revealed that among the SNPs associated with both AD and constipation, 15 were located in intronic regions, 6 in non -coding RNA intronic regions, 8 in intergenic regions, and 1 in an exonic region (Table 3). In addition, three loci shared between AD and constipation had CADD scores exceeding 12.37, indicating that these loci may have potential deleterious effects (Table 3).
Additionally, we mapped 30 candidate SNPs that are jointly associated with AD and constipation to protein-coding genes (Table 3). Some genes were mapped to loci associated with both AD and constipation, are related to synaptic function and neuronal development. For instance, DISC1 regulates neuronal development, synapse formation, and axonal transport; SYT14 controls synaptic vesicle release and neurotransmitter transmission; CR1 and CLU are known genetic risk factors for AD.44–46
Finally, these mapped genes were subjected to GO and KEGG pathway enrichment analyses (Figure 7). The GO enrichment analysis indicated that these genes are involved in pathways associated with Aβ metabolism and processing (GO:0050435, GO :1902430, GO:0097242), tau protein-related processed (GO:0048156), and neuronal function and synaptic pathways (GO:0050769, GO:0008021). KEGG analysis highlighted the complement and coagulation cascades and the Fcγ receptor-mediated phagocytosis pathways (hsa04666).

Go and KEGG functional enrichment analysis of mapped genes between AD and constipation.
Discussion
To the best of our knowledge, our study is the first systematic investigation to integrate LDSC, HDL, PLACO, FUMA analysis, and MR methods to explore the causal relationship between NDDs and constipation, as well as their shared genetic basis. The results revealed a positive causal relationship between AD and an increased risk of constipation, while no causal association was observed between constipation risk and PD, MS, ALS, or LBD. In reverse MR analysis, we found no evidence supporting a potential causal relationship between constipation and the five NDDs. Through LDSC and HDL analysis, we identified a positive correlation between AD risk and constipation, indicating a genetic overlap between the two conditions. Finally, PLACO and FUMA analyses identified 30 highly overlapping risk loci, while enrichment analysis uncovered multiple shared pathways. Notably, some of these significantly enriched pathways were associated with Aβ metabolism and processing, as well as tau protein-related processed.
To date, a consensus has not been reached about the relationship between NDDs and constipation, with the causative factors and underlying mechanisms still unclear. In patients with AD, constipation manifests as a typical symptom, characterized by decreased bowel movement frequency and challenges in defecation, which seriously impacts their daily activities and quality of life. 47 Kim et al. investigated the factors associated with constipation and AD, revealing that the neuropathological constipation phenotype observed in AD may be closely related to dysbiosis of the fecal microbiota. 48 Another cross-sectional study found that the prevalence of constipation was significantly higher in patients with AD and mild cognitive impairment compared to those with normal cognition.49,50 Thus, our finding demonstrating the causal impact of AD on the heightened likelihood of constipation is consistent with the previous studies. In the reverse direction, a bi-national cohort study revealed that constipation increases the risk of developing AD. 51 The following reasons may explain this phenomenon: (1) observational studies primarily focus on clinical symptoms rather than intrinsic links, which may introduce bias due to environmental factors and reverse causation; (2) the definition of constipation is often vague, its prevalence high, its etiology diverse, and comorbidities are severe in elder populations. Consequently, the underlying bias in traditional clinical studies may lead to its discrepancy from our MR results suggesting no substantial evidence of a causal correlation between constipation and the risk of NDDs.
Several potential mechanisms have been put forward to elucidate the heightened chance of constipation in individuals with AD. Firstly, the gut-brain axis, which serves as a sophisticated bidirectional network facilitating communication between the gut and the brain, is thought to play a significant role. 52 The brain can impact the gut microbiota, as demonstrated by the significant changes in gastrointestinal microbiota observed under short-term stress. 53 The brain can also affect the function and composition of gastrointestinal bacteria by altering intestinal permeability, which can result in the migration of these bacteria across the gut epithelium and trigger an immune reaction in the gastrointestinal mucosa. 54 A study discovered dysbiosis of the fecal microbiota in AD mice, specifically a decline in Bacteroidetes populations and a rise in Firmicutes and Proteobacteria populations at the phylum level, leading to neuropathological constipation. 48 Secondly, both neurochemical and neurophysiological changes in the brains of AD patients contribute to the clinical symptoms. AD is primarily marked by extensive loss of neurons, deposition of Aβ plaques, and the appearance of neurofibrillary tangles in various brain regions. These changes contribute to a substantial reduction in brain function, especially in the hippocampus and frontal cortex areas. 55 In particular, impairments in the cholinergic system play a significant role in directly affecting gastrointestinal motility, 56 causing gastrointestinal disorders involving constipation. Thirdly, commonly used medications in AD treatment, such as acetylcholinesterase inhibitors and glutamate-receptor antagonists, may aggravate constipation problems. 57 These drugs decrease cholinergic activity in the gut, resulting in reduced intestinal motility.
Among the 30 pleiotropic loci associated with AD and constipation annotated by PLACO and FUMA, 22 were newly identified for AD. The genes mapped to these loci encompass a wide range of biological functions, including metabolic signaling (AGBL4, ENSA, NDUFAF6,),58–60 synaptic function and neuronal development (SYT14, DISC1, SYT14),61–63 and immune regulation (TRAF3, SIRPA).64,65 Notably, several non-coding RNA genes (e.g., RP11-111J6.2, RP11-444A22.1, RP11-138J23.1) were also identified, suggesting their potential roles in gene regulation and disease pathogenesis. These newly identified shared loci underscore the involvement of neural signaling, immune responses, and metabolic processes, warranting further experiments and research for confirmation. Further GO enrichment analysis revealed that these significant pleiotropic genes are involved in critical pathways closely related to the pathogenesis of AD, including Aβ metabolism and processing, tau protein-related process, and pathways essential for neuronal function and synaptic activity. These findings are consistent with previous evidence indicating that the accumulation of Aβ plaques, aggregation of tau protein, and synaptic dysfunction are hallmark pathological features of AD. Additionally, KEGG pathway analysis highlighted the involvement of complement and coagulation cascades and the Fcγ receptor-mediated phagocytosis pathway. These pathways underscore the pivotal role of immune responses and inflammation in AD pathology. Together, these findings emphasize the complex interplay of metabolic, neuronal, and immune pathways in AD and suggest that certain shared loci may exert dual roles through their influence on the gut-brain axis.
This study has certain limitations that need to be considered. First, it only included participants of European ancestry, which limits the generalizability of the findings to other ethnic populations. Second, the lack of individual-level data restricted more detailed analysis of NDDs patients across different ages and sexes. Lastly, the pleiotropic loci identified in this study may have diverse biological functions, and understanding how these functions regulate the relationship between AD and constipation could be quite complex, requiring further experimental validation and functional studies.
Conclusion
In conclusion, our two-sample MR study confirmed the causal relationship between AD and constipation. Through comprehensive genetic correlation and overlap analysis, combined with the use of various biological tools, we identified significant genetic correlations and several potential pleiotropic genetic loci, as well as enriched pathways linking AD and constipation. These novel findings may provide crucial evidence for the precise identification, assessment, and treatment of constipation in AD patients, highlighting the importance of early intervention and meticulous management of this condition.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251362469 - Supplemental material for Causal associations and shared genetic etiology between neurodegenerative diseases and constipation
Supplemental material, sj-docx-1-alr-10.1177_25424823251362469 for Causal associations and shared genetic etiology between neurodegenerative diseases and constipation by Weidong Sun, Anlong Zhu, Hanman Chang, Junyi Xia, Jun Gao, Zhiqiang Zhang, Fengxu Chi, Yuekun Zhu and Xuhui Bao in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
Our data are taken from the publicly available GWAS database. We thank the genetics consortiums for making the GWAS catalog data publicly available.
Ethical considerations
All GWAS databases were publicly available and had been approved by the corresponding ethical review board in the original GWAS.
Author contributions
Weidong Sun: Conceptualization, Writing – original draft.
Anlong Zhu: Writing – review & editing.
Hanman Chang: Supervision.
Junyi Xia: Investigation.
Jun Gao: Formal analysis.
Zhiqiang Zhang: Investigation.
Fengxu Chi: Formal analysis.
Yuekun Zhu: Conceptualization, Supervision, Writing – review & editing.
Xuhui Bao: Supervision, Visualization.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 82272696 to Y.-K.Z, 82272817 and 82361138567 to X.B.), Science and Technology Development Fund of Shanghai PudongNew Area (Grant No. PKJ2022-Y50 to X.B.), Academic Leaders Training Program of Pudong Health Bureau of Shanghai (Grant No. PWRd2023-01, to X.B.), Young Clinical Investigator Training Program of Fudan University Shanghai Medical College (Grant No. DGF828019-3 to X.B.), and Cultivation Program for Single-cell Sequencing Scientific Research of Shanghai Pudong Hospital (Grant No. YJDXB2023-01 to X.B.). The funders had no role in study design, data collection, and analysis, the decision to publish, or the preparation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All GWAS summary statistics analyzed in this study are publicly available for download by qualified researchers. The GWASs for AD, PD, MS, ALS and LBD can be obtained through the IEU data portal (https://gwas.mrcieu.ac.uk/). The GWASs for constipation were provided by the FINNGEN (![]() ).
).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.