
Abstract
Background
YouTube is increasingly used by patients and caregivers as a source of health information. However, the quality and reliability of content on Alzheimer's disease dementia (ADD) remain uncertain.
Objective
This study aimed to determine whether YouTube videos on ADD provide reliable and high-quality information for caregivers and to assess whether the most popular videos are also the most trustworthy.
Methods
In December 2024, YouTube was systematically searched for ADD-related videos. Two independent physicians reviewed each video, scoring it using modified DISCERN (mDISCERN) for reliability and the Global Quality Scale (GQS) for content quality. Videos were categorized by goal and assessed for quality, accuracy, comprehensiveness, and specific content.
Results
There were 117 videos included in the study. Using the mDISCERN scale, 70 videos (59.8%) were deemed with good reliability, 33 videos (28.2%) have moderate reliability, and 14 videos (12%) have poor reliability. Using the GQS, 61 videos (51.1%) have high quality, 16 videos (28%) were assessed as excellent quality, 34 videos (29%) as moderate quality, and 7 videos (6%) as low quality. Videos from academic institutions, news agency and physicians exhibited higher mDISCERN and GQS scores compared to other groups and a significant correlation was seen between mDISCERN and GQS (p < 0.001).
Conclusions
The videos on ADD produced by healthcare professionals and academic institutions have high quality and good reliability, covering disease properties, treatment choices, and patient experiences. However, video popularity does not significantly correlate with content reliability and quality.
Introduction
Alzheimer disease dementia (ADD) is the most common type of dementia, accounting for about 60–70% of cases. 1 ADD involves the buildup of abnormal proteins known as amyloid-β and phosphorylated tau in the brain, along with the loss of neurons. This process leads to changes in both the structure and function of the brain. 2
Currently, there is no definitive treatment that can reverse cognitive function damage. However, an early and accurate diagnosis has proven effective in enhancing overall quality of life. 3 The approach gives patients and their family caregivers enough time to understand and adjust to the changes that happen as the disease advances. It is essential to improve public understanding and awareness of ADD to enable timely intervention.
Previous studies have shown notable differences in dementia literacy, even among wealthy countries.4–6 The Facing Dementia Survey carried out in six European countries showed that people in the community had a limited understanding of the early signs and treatments for ADD. 4 More than 80% of those surveyed thought that most people wouldn't be able to recognize early signs, and 76% believed that effective treatments were not available. 4 A study in the United Kingdom found that while most participants were actively involved in managing their health, they had a limited grasp of the risk factors linked to dementia. 5 A preliminary study in Australia found that 80% of elderly individuals were able to accurately recognize dementia symptoms. However, their views on the treatments available and the steps they deemed acceptable for seeking help differed greatly. 6
In the face of these knowledge gaps, patients and caregivers increasingly turn to the internet for informatio.7,8 YouTube, the world's second-largest search engine and one of the most visited platforms globally, has emerged as a popular source of health-related content.9,10 It offers broad access to educational material but lacks formal content regulation or peer review. Surveys show that 86% of health information seekers question the credibility of online content, and 44% believe that only part of the information available is reliable. 11 YouTube has the potential to provide valuable education on dementia, but the accuracy and quality of videos related to ADD are still uncertain. 12
Although Tang et al. performed a thematic content analysis on YouTube videos linked to AD, with an eye toward source type, message framing, and communication strategies, the reliability and quality of these videos as teaching tools are still largely unexplored. 13 Especially lacking is a measurement grounded on validated evaluation tools like the modified DISCERN (mDISCERN) and the Global Quality Scale (GQS). Moreover, past research has not particularly addressed how these videos meet the information needs of family caregivers, who frequently turn to internet resources for guidance.
To address this current gap in literature, our study aimed to systematically evaluate YouTube videos related to ADD using the mDISCERN and GQS. We assessed their reliability, quality, and potential as educational tools. Our primary research objective was to determine if YouTube videos on ADD offer reliable and high-quality information for caregivers. As a secondary objective, we wanted to assess if the most highly-viewed and liked videos also reflect high-quality and reliable content. This evaluation will facilitate informed decision-making for both caregivers and clinicians.
Methods
This research was a cross-sectional observational study carried out in September 2024. To avoid any external factor that might affect the data gathering, no YouTube account was used and Google Chrome was placed in “incognito mode”. YouTube was searched using the separate key terms, “Alzheimer's Disease, Alzheimer's Dementia, Dementia”. The “Relevance-Based Ranking” was used to filter the YouTube search for this study. 14 For each search query, the top 90 results were exported to a separate database (Microsoft Excel) for manual review, along with the title of each result, the table also included source, upload date, number of views, likes, dislikes, and comments. Only the first 90 videos that appeared for each keyword are evaluated, as studies have shown that 90% of internet users did not view more than three pages (corresponding to 30 videos per page), and duplicates are removed. 15
Inclusion and exclusion criteria
The YouTube videos in English and Filipino incorporated in this research specifically examined the symptoms, etiology, and therapeutic interventions pertaining to ADD. Voice-over videos that were between twenty seconds and twenty minutes in length were also included. Previous studies have indicated that the majority of YouTube videos have a duration of less than 20 min, and audiences mostly exhibit interest in watching these shorter video formats but not less than 30 s since the content of these videos will be difficult to assess. 16 We eliminated videos with durations below 20 seconds and above 20 minutes, based upon similar researches.17–19 Videos that did not discuss anything related to ADD were excluded from the study. Likewise, videos focused on other types of dementia (e.g., frontotemporal, Lewy body, vascular, and others) were also excluded. Duplicate entries and irrelevant videos were all excluded from consideration (see Figure 1).

Flow chart showing the selection of YouTube videos on Alzheimer's disease dementia.
Variables extracted
Apart from evaluating content reliability and quality, we also collected video engagement data to investigate the relationship between educational value and popularity. This is to support the secondary objective of determining whether highly regarded and popular videos also feature high-quality and reliable content. Quantitative video attributes (such as view count, video duration, like and dislike counts, comment count, time since upload, and number of channel subscribers) were retrieved. Derived engagement indices, such as the like ratio, view ratio, and video power index (VPI), were calculated using standard formulas. The like ratio was calculated as the “number of likes/(number of likes + number of dislikes) × 100,” view ratio as the “number of views since upload/number of days since upload,” and VPI as the “like ratio × view ratio/100 were recorded using the “vidIQ Vision” plugin for YT”. 20 These metrics were later analyzed for correlation with mDISCERN and GQS scores to determine if popularity indicators align with information reliability and quality.
Grouping of videos
Each relevant video was curated and compiled in a final database using Microsoft Excel. A total of 270 videos were identified through the search, and 163 videos related to the study topic were subjected to a preliminary evaluation. Two independent senior neurology residents (LCA and CJN) reviewed the specified videos separately in October 2024.
The video sources were categorized into six classifications: academic institutions/ professional organizations, health information websites, physicians, healthcare professionals excluding physicians (such as nutritionists, nurses, and physical therapists), news outlets, and independent users. The videos were categorized based on the target audience: healthcare professionals and the general population. 21 The video content was also categorized into three classifications: (a) definition, pathophysiology, diagnostic and management, (b) personal experience, and (c) dementia care.
Reliability and quality assessment
The mDISCERN, a validated instrument derived from the original DISCERN instrument, intended to assess the accuracy of consumer health data. It consists of five dichotomous questions that evaluate clarity of aims, use of reliable sources, and disclosure of uncertainty. 22 Previous studies have indicated that mDISCERN has a great inter-rater reliability and is helpful for assessing online health videos.20,21,23 A score of greater than three in this study denotes high reliability.
The GQS, the five-point Likert scale, assess the general quality of online health content, through patient value, structure, flow, and simplicity of use. 23 Previous studies consistently report good to excellent inter-rater reliability when using the GQS, particularly when applied by trained healthcare professionals.17,21
The mDISCERN emphasizes source credibility and openness, while the GQS shows the informational depth, coherence, and user-friendliness of the video. These tools taken together offer complimentary points of view: GQS assesses data presentation quality, and mDISCERN tests dependability. Two independent reviewers, LCA and CJN, who are both senior neurology residents, assessed the videos with the mDISCERN and GQS. Before scoring, both raters participated in a standardized orientation and calibration session. This included reviewing sample videos and discussing the criteria of the tool to ensure that their scoring was consistent.
Statistical methods
Descriptive statistics, including means, medians, ranges, and standard deviations, were used for the continuous variables. Pearson correlation test was used to find differences between categorical variables and Chi-square independent test on nominal data. Inter-rater agreement was calculated using intra-class correlation coefficients. Statistical analyses were conducted using SPSS version 30, with p values of < 0.05 considered as statistically significant.
Results
Among the 270 videos found, 107 videos were initially excluded as duplicates. A total of 163 videos were screened, and 23 videos were further excluded (5 were less than 20 seconds in duration, 18 videos were longer than 20 minutes). A total of 140 videos were watched, of which 23 were further excluded (11 videos did not discuss ADD and 12 videos focused on other types of dementia). Thus, 117 videos were included in the study and summarized in Figure 1.
Video source
A total of 117 videos were included and evaluated. Most of the videos (n = 36, 30.8%) were from academic institutions/ professional organizations, closely followed by news organizations (n = 28, 23.9%) (Figure 2). Physicians and other healthcare professionals both yielded 12% (n = 14) of the videos. About 11.1% (n = 13) have health information website as the source, while independent users contributed the least at 10.3% (n = 12). Among the 117 videos, only a single video is in Filipino, obtained from a news segment in the Philippines.
Video content and target audience
The majority of videos (n = 93, 79.5%) targeted the general public, whereas only 20.5% (n = 24) targeted health care professionals and physicians. More than half of the videos (n = 67, 57.3%) discussed the symptoms, pathophysiology, and treatment of ADD. In contrast, a quarter of the videos (n = 32, 27.4%) looked into the personal experiences of patients and carers, while 15.4% (n = 18) addresses dementia care.
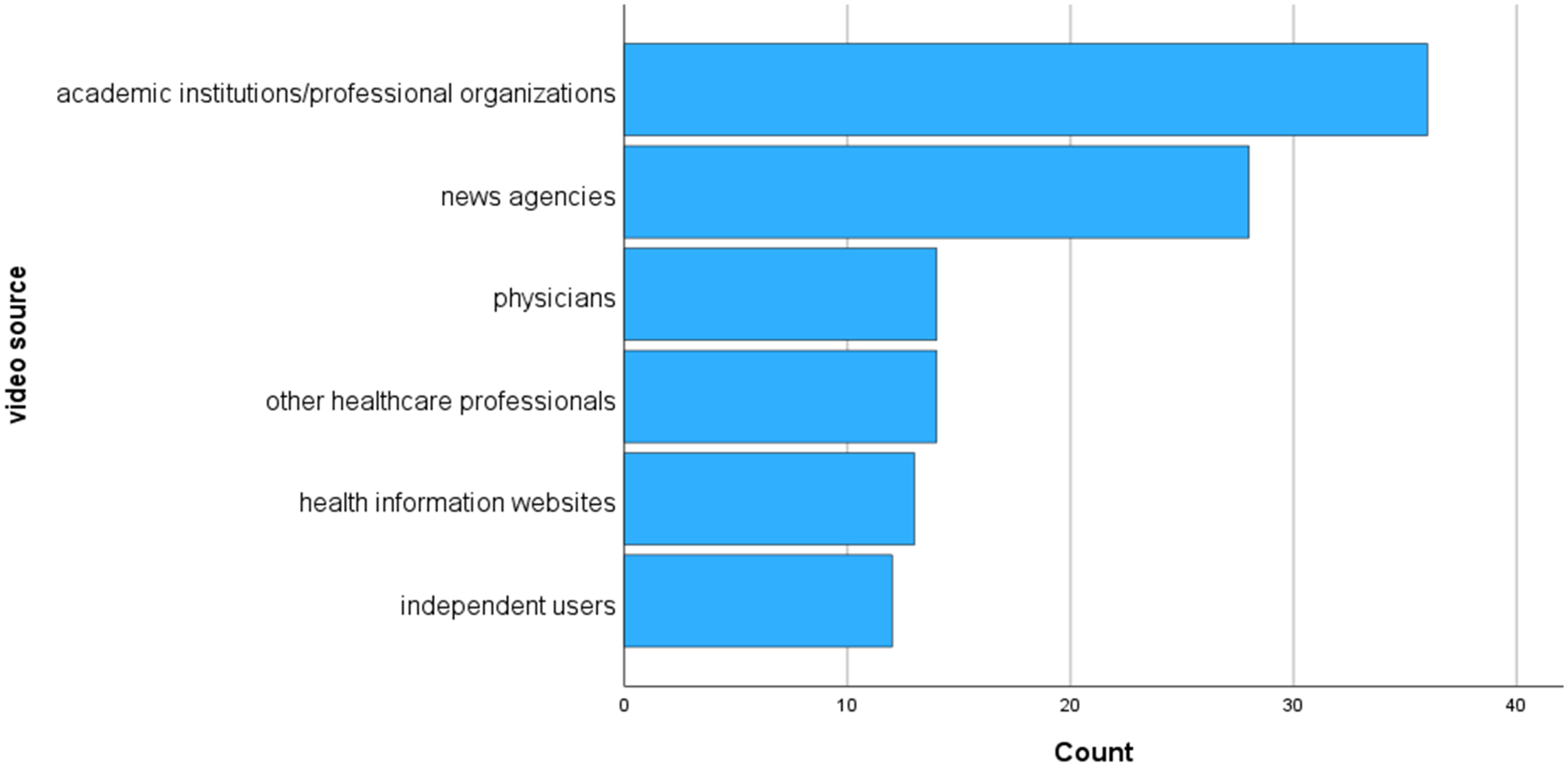
Sources of Alzheimer's disease dementia related videos.
Video statistics
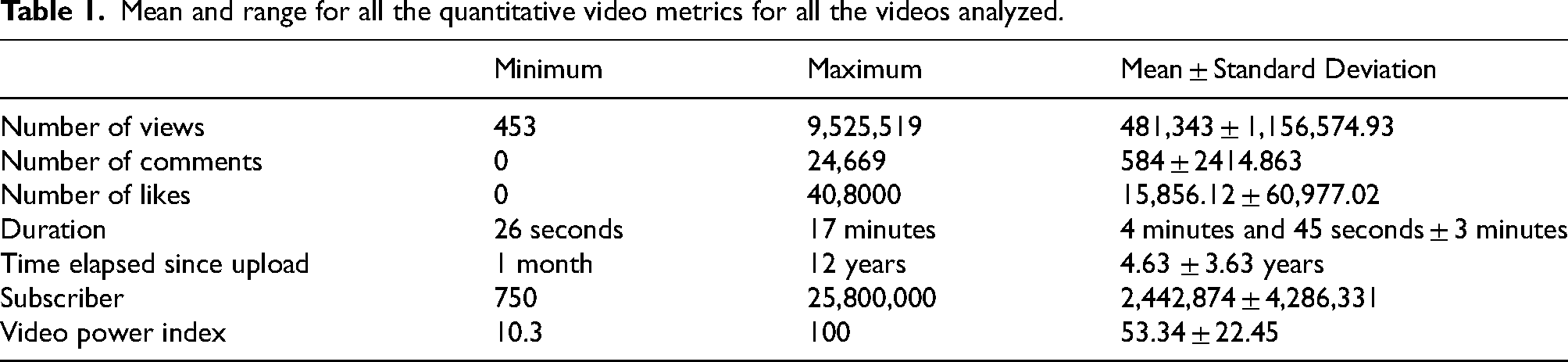
The following are the mean and range for all the quantitative video metrics for all the videos analyzed: the view count (mean, 481,343; range, 453–9,525,519), number of comments (mean, 584; range, 0–2192), number of likes (mean 15,856; range, 0–408,000), duration (mean, 4 min and 45 s; range, 26 s–17 min), and time elapsed since upload (mean, 4.63 years; range, 1–144 months), the mean channel subscribers were 2,442,874 (range, 750–25,800,000), and the VPIs were 53.34 (range, 10.3–100) (see Table 1).
Mean and range for all the quantitative video metrics for all the videos analyzed.
Quality statistics
Most of the content across different sources has good-to-moderate quality and excellent-to-moderate reliability. Around 80.6% (n = 29) of videos from academic institutions were rated as having good reliability and 61.1% (n = 22) rated as excellent to high quality. Videos from physicians, healthcare professionals, and news agencies also performed well, with around half of their videos rated as having good reliability and of excellent to high quality. Health information websites and independent users demonstrated moderate reliability (53.9%, 41.6% respectively) and variable quality, since more than half (53.9%) of health information websites have high quality, while around half of videos (58.3%) from independent users were rated as moderate quality (see Table 2).
Evaluation of YouTube videos using the Global Quality Scale and mDISCERN criteria.

SD: standard deviation; mDISCERN: modified DISCERN.
The mean mDISCERN score from the two raters was 3.83 ± 0.76 (range, 2–5) and 3.91 ± 94 (range, 2–5), respectively. The mean GQS score from the two raters was 3.85 ± 0.70 (range, 2–5) and 3.91 ± 0.86 (range, 2–5), respectively. The combined mean mDISCERN score was 3.85 ± 0.80 (range, 2–5), while the combined mean GQS score was 3.89 ± 0.72 (range, 2–5) suggesting that videos on ADD had good reliability and high quality.
For absolute agreement in mDISCERN scoring, the intra-class correlation coefficient between the two raters was calculated as 0.982 (95% confidence interval (CI), 0.975–0.987) for single measures and 0.991 (95% CI, 0.988–0.993) for mean measures. In the GQS scoring, the intra-class correlation coefficient between the two raters was 0.971 (95% CI, 0.961–0.979) for single measures and 0.986 (95% CI, 0.980–0.990) for mean measures. This result indicates an excellent inter-rater reliability for both scoring systems.
Quality statistics and user engagement metrics
There was a significant strong correlation between mDISCERN and GQS (r = 0.74, p = 0.001). There was no significant association found between mDISCERN and video source (p = 0.26), video target (p = 0.24), and video content (p = 0.85). Furthermore, there was no association found between GSQ and video source (p = 0.33), video content (p = 0.45) and video target (p = 0.25).
There was no significant correlation between mDISCERN and user engagement metrics such as the view count (p = 0.22), time elapsed since upload (p = 0.17), duration (p = 0.72), number of comments (p = 0.44), number of likes (p = 0.15), view ratio (p = 0.614), and subscriber (p = 0.705). There was no significant correlation between GQS and number of views (p = 0.573), time elapsed since upload (p = 0.195), duration, number of comments (p = 0.44), number of likes (p = 0.60), view ratio (p = 0.84), VPI (p = 0.62), and subscriber (p = 0.37). However, there was a significant correlation between GQS and duration time (r = 0.21, p = 0.02) (Table 3).
Correlation of video features and the Global Quality Scale and mDISCERN scores.

* Correlation is significant < 0.05 level; ** Correlation is significant at the 0.01 level (2-tailed).
mDISCERN: modified MDISCERN.
Discussion
This study found that most YouTube videos about ADD, particularly those made by academic institutions, doctors, and healthcare professionals, were of high quality and reliable. Academic institution videos also scored the highest in both metrics. No significant correlation was found between the quality or reliability of content and video popularity metrics like view count, likes, or comments. However, a modest but statistically significant correlation was found between video duration and content quality (r = 0.21, p = 0.02).
This highlights the danger of assuming that a video's popularity is an indicator of its reliability or quality. This also suggests that relying solely on engagement metrics may lead caregivers and the public to unknowingly encounter false or inadequate information. Our research found that videos made by medical professionals and academic institutions consistently received higher scores in both mDISCERN and GQS, highlighting the significance of source credibility. Independent user videos showed modest to good reliability and quality, which reflected growing awareness and effort to provide accurate dementia-related content online.
Our findings support earlier research on gout, infantile colic, and hemifacial spasm, showing that videos created by healthcare professionals and academic institutions are more trustworthy and informative than those from non-experts or commercial entities.21,23,24 This is in contrast with studies on hip arthritis, COVID-19, prostate cancer, and amyotrophic lateral sclerosis which suggested that many videos were misleading or of poor quality.11,19,25,26 The differences show that the quality of YouTube content can vary based on the health topic. Conditions such as ADD could greatly benefit from stronger public advocacy, increased research interest, and greater involvement from academic institutions in developing relevant content.
We found no link between user engagement metrics and content quality or reliability, similar to a paper on medial epicondylitis. 20 This highlights the danger of confusing popularity with accuracy. This disconnection may be affected by the presentation and amplification of videos through platform trends than their educational merit. It has been reported that viewers often favored misleading content and personal narratives over scientifically accurate video. 27 The popularity of a video might depend more on how it's presented and current platform trends rather than its educational content.
Our study has several limitations. We only included English and Filipino videos, as these are languages the authors can understand and those uploaded up to a certain date. Due to the study design, our study only looked at the content of the videos and was unable to directly measure the impact of these videos on the intended audience/ viewers. YouTube also does not have any stratification of videos as to the target audience. These videos are accessible by everyone. The inter-rater reliability was ensured by having two scorers. The name/ identity of the video uploader could also not be blinded. The involvement of physician raters could potentially lead to a certain level of professional bias that favors content that is clinically accurate or technically detailed. This approach facilitated a thorough assessment of medical reliability; however, future research should explore the inclusion of non-expert raters, such as patients or caregivers, to enhance the evaluation of content accessibility and its practical significance for everyday users.
Several practical implications can be identified based on these findings. To start, content creators and health educators should first consider applying validated health communication frameworks and considering tools like mDISCERN and GQS to guarantee accuracy, openness, and comprehensiveness through the development process. We also propose that current platform-based verification systems, like Facebook's verified page badge and YouTube's channel verification, be more rigorously implemented and modified to emphasize reliable health information sources. It is advisable for platforms to prioritize content from medically affiliated or professionally verified creators within their ranking algorithms and search results for health-related inquiries. Implementing this approach may assist caregivers in more effectively recognizing reliable information while minimizing their exposure to misleading or overly simplistic content. Lastly, future studies should investigate how video characteristics influence user comprehension, decision-making, and behavioral outcomes, beyond passive engagement metrics.
Conclusion
The videos on ADD produced by healthcare professionals and academic institutions have high quality and good reliability, covering disease properties, treatment choices, and patient experiences. However, video popularity does not significantly correlate with content reliability and quality. These findings provide empirical support for directing caregivers toward medically vetted content and reinforce the importance of source credibility in digital health education.
Future work should also examine how such content influences viewer understanding, decision-making, and caregiving behaviors in real-world settings.
Footnotes
ORCID iDs
Ethical considerations
This study did not involve human participants, animals, or patient data. It was based entirely on publicly available YouTube content and did not require institutional ethics board approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study (i.e., video list, scoring sheets, and extracted metrics) are available from the corresponding author upon reasonable request.