
Abstract
Background
People suffering from Alzheimer's disease and related disorders (ADRD) were severely impacted by the COVID-19 pandemic, both physically and mentally.
Objective
This one-year study aimed to implement a protocol for controlling the spread of SARS-CoV-2 in a Belgian nursing home hosting exclusively patients suffering from ADRD, while minimizing pandemic-associated constraints.
Methods
After confirming the absence of positive cases in the nursing home and the development of a proper immunity against SARS-CoV-2, the staff members enrolled in the study were allowed to remove their mask. Then, a weekly non-invasive saliva RT-qPCR testing for SARS-CoV-2 detection was implemented to detect cases among the staff and residents. A monthly serological monitoring was set up to follow the levels of neutralizing and IgG antibodies against SARS-CoV-2.
Results
Three waves of COVID-19 infection were observed and quickly contained thanks to an effective quarantine policy. We confirmed the stronger humoral response developed by people infected before primo-vaccination compared to naïve-vaccinated ones and the weaker immune response of elderly individuals compared to younger participants, a difference abolished by booster. In parallel, we showed that ADRD people were able to develop a similar humoral response to SARS-CoV-2 vaccination or infection to that of people of similar age not suffering from these diseases.
Conclusions
We show that a strict protocol aimed at early case detection and anti-SARS-CoV-2 immunity follow-up has enabled ADRD residents from a Belgian nursing home to maintain social interactions thanks to the ability of study participants to remove masks, while minimizing the risk of infection.
Introduction
Nursing homes have been disproportionately affected by the COVID-19 pandemic. This was the case in Belgium, with more than 50.8% of deaths occurring in these facilities by the end of August 2021, but also in many other European countries.1,2 Indeed, the virus, although infecting the entire population, affects more severely elderly people who have more underlying medical conditions such as hypertension, diabetes, cardiovascular disease, chronic respiratory or kidney diseases, or cancer.3–6 Moreover, the risk of transmission in nursing homes is high due to residents living in close proximity to one another. They also have frequent direct contact with staff members who establish, with visitors, a complex transmission route for the SARS-CoV-2 between the nursing home and the outside community.7–9 The COVID-19 mortality rate was about 13 times higher inside nursing homes than in the 65-older population outside these institutions in Belgium between March 2020 and February 2021. 10
In Belgium, to limit the spread of the disease, a complete closure during the quarantine periods followed by a severe restriction on the number of visitors to nursing homes was associated with strict hygiene protocols, face mask wearing, physical distancing and proper room ventilation. “La Maison Vésale” is a rest and nursing home exclusively hosting residents who are suffering from Alzheimer's disease and related disorders (ADRD) in various stages of dementia. These residents were particularly vulnerable. Indeed, in addition to being a population of elderly people, most ADRD residents have difficulties complying with barrier practices because they do not understand the purpose of these measures and/or do not remember them. 11 Moreover, some studies have shown, during the lockdown time span, a worsening of cognitive symptoms and functional disability in these patients, with the exacerbation or onset of behavioral disturbances further reducing their ability to comply with COVID-19-related restrictions.12,13 An excess of approximately 8000 deaths unrelated to COVID-19 among individuals suffering from Alzheimer's disease or dementia was observed in England in 2020, compared to expected levels. 14 Firstly, to comply with the rules put in place by the government, “La Maison Vésale” ‘s board of directors decided that the staff, visitors and external service providers, should wear the mask and apply physical distancing among themselves and as much as possible with residents. Residents were exempted from wearing mask. However, with time, in order to limit the feelings of loneliness, anxiety and behavioral modifications generated among residents by the loss of contact and mask wearing, some staff members have expressed the wish to remove their mask when in contact with residents. This was accepted and supported by the management board as well as the public interest organization Iriscare whereas at that time, wearing a mask was still mandatory, especially in nursing homes. 15 In this context, “La Maison Vésale” was in a precarious situation where the absence of masks among elderly ADRD residents (a population unable to comply with barrier practices) and some staff members creates conditions conducive to an increase in COVID-19 cases.
Here, a one-year study has been conducted with the aim of controlling the spread of SARS-CoV-2 in “La Maison Vésale” while simultaneously attempting to maintain residents and staff members’ social interactions during the COVID-19 pandemic. First, once assured of the absence of positive cases in the nursing home and of the development of a proper immunity against SARS-CoV-2 through vaccination or natural infection, permanent staff members involved in the study were permitted to remove their masks during their workday and interactions with residents to foster better social relations. Then, to control the spread of the virus, a weekly non-invasive saliva RT-qPCR testing for SARS-CoV-2 detection was implemented to detect positive cases among the staff and residents. Simultaneously, a monthly serological monitoring was set up to determine the participants’ levels of total and neutralizing antibodies against SARS-CoV-2 and thereby monitor non- or poorly immunized ones more closely. Therefore, the global objective was to assess the aforementioned protocol's practicality in real-world settings, specifically to determine whether regular diagnostic and serological screening in a population prone to increased infection rates could effectively mitigate the spread of infections. If the experiment proved to be successful, this study could serve as a basis for scalable implementation in the event of a future pandemic, thereby avoiding imposing excessive safety precautions in nursing homes. Finally, as no information was available on the subject in scientific literature, the secondary objective was to investigate if elderly people suffering from Alzheimer's disease or dementia had as many antibodies as seniors not suffering from this disease.
Methods
Study design
The study started on March 8, 2021 and ended on March 23, 2022. It exclusively included staff members and residents from “La Maison Vésale” in Brussels (Belgium). All the participants, a trusted person or a legal representative, signed informed consent before enrolling in the study. Most of the residents participating in the study had a legal representative appointed through legal proceedings requested by the family, independently of the study. Furthermore, during the testing sessions, the caregiver never insisted when the resident refused the sample collection. The protocol was approved by the local hospital's ethical committee from CHU Saint Pierre (B0762021210230).
This study aimed to establish a protocol for achieving an optimum balance between providing the most humane care possible and protecting these patients from the virus. Before setting up the whole protocol, blood sampling was performed to measure the seropositivity against SARS-CoV-2 of all participants. Moreover, all of them were also tested two times one week apart by salivary diagnostic test to detect possible infection. A seropositivity of 80% and the total absence of positive results to the salivary diagnostic tests were required to launch the study protocol. The guidelines of the protocol were as follows:
- The permanent staff were allowed to remove mask during their working days and during the contacts with the residents. Moreover, physical-distancing measures may be relaxed. - The participants were weekly submitted to a salivary diagnostic test followed by RT-qPCR assay in order to detect any individual positive to SARS-CoV-2. - Mask removing was forbidden when COVID-19 positive cases were detected among staff or residents. After the receipt of a negative PCR test for all participants, the mask may be removed again. - Quarantine policy: when COVID-19 positive cases were detected among residents, they were confined in their room when case number was ≤ 3. Above this number of cases, the COVID-19 unit was reopened to house them. When a positive case was detected among the staff, the person either went to work in the COVID unit when it was open or took care of COVID-19-positive residents; if this was not possible, they stayed at home. - In order to monitor the presence and the level of anti-SARS-CoV-2 IgG antibodies and anti-SARS-CoV-2 neutralizing antibodies, a blood sampling was performed monthly among participants.
The timeline of the study is depicted in Figure 1.

Timeline of the one-year study protocol. The participants were weekly submitted to a salivary diagnostic test (S) followed by RT-qPCR assay in order to detect SARS-CoV-2 infection and to a monthly blood sampling (B) in order to monitor the presence and the level of anti-SARS-CoV-2 IgG antibodies and anti-SARS-CoV-2 neutralizing antibodies. B: blood sample; S: salivary diagnostic test; W: week.
Study populations
The main cohort of this study was “La Maison Vésale” population. However, in order to analyze different aspects of the results, two other cohorts were involved (see below): the oldest people from the “Jolimont” cohort and the “University of Liège” cohort of the so-called SARSSURV study. 16
The “La Maison Vésale” cohort
This cohort was composed of all permanent staff members and residents from “La Maison Vésale” (Brussels, Belgium) who agreed to take part to this study. New nursing home residents or staff members could be incorporated into the study during its progress. Participants could withdraw their consent at any time and, at times, sample collection for residents was hindered by hospitalization, lack of cooperation, or death, while for staff members, it was due to their absence from work on the day of sampling. A total of 103 participants were included into the study and each of them was associated to a personal unique identification code. Among participants, 69 were residents and 34, permanent staff members. During the protocol, 100% of residents didn’t wear a mask while 70% of permanent staff (participants and non-participants) wore it. At the beginning of the study, 76.7% of the participants had received the two first doses of the Pfizer/BioNTech vaccine (i.e., Primo-vaccination; vaccine period: January /February 2021). 68.9% of the participants received a third booster dose in October 2021.
The Jolimont Hospital cohort
This cohort was composed of all permanent staff members from the Jolimont Hospital (La Louvière, Mons and Warquignies, Belgium) who agreed to take part to the study. The participants could withdraw their consent at any time. The study was conducted from August 15, 2021 to December 20, 2021. The protocol was approved by the hospital's ethical committee (2021/198). The participants were weekly submitted to a salivary diagnostic test followed by RT-qPCR assay in order to detect any person positive to SARS-CoV-2 and a blood sampling was also performed monthly in order to monitor the presence and the level of anti-SARS-CoV-2 IgG antibodies and anti-SARS-CoV-2 neutralizing antibodies.
A total of 124 participants were included into the protocol study and each of them was associated to a personal unique identification code. Among the 124 participants, only 26 were older than 55 and were therefore considered in this study. All the participants wore masks at work during the study protocol. At the beginning of the study, all of them had received the two first doses of the Pfizer/BioNTech or Moderna vaccine (i.e., Primo-vaccination; vaccine period: January/March 2021). Some participants received a third booster dose in November 2021.
The University of Liège cohort (SARSSURV study; 16 )
This cohort included all permanent staff members and students from the University of Liège (Belgium) who agreed to take part to the so-called SARSSURV study. 16 The participants could withdraw their consent at any time. The study was conducted from April 1, 2021 to December 31, 2022. The protocol was approved by the local hospital's ethical committee from CHU of Liège (2021/96). The participants were weekly submitted to a salivary diagnostic test followed by RT-qPCR assay in order to detect any individual positive to SARS-CoV-2. A blood sampling was also performed 15 days, 3 months and 6 months after either a vaccination or a COVID-19 infection in order to monitor the presence and the level of anti-SARS-CoV-2 IgG antibodies and anti-SARS-CoV-2 neutralizing antibodies.
A total of 1706 participants were included into the SARSSURV study and each of them was associated to a personal unique identification code. 164 participants were older than 55 and were therefore considered in the present study.
Salivary diagnostic tests and RT-qPCR assay
Saliva was sampled each week using the INACTIFUN kit (Diagenode, Seraing, Belgium). Participants either sampled themselves or were sampled with the help of a third person (residents from “La Maison Vésale”).
The collection tube contained a buffer inactivating any virus that might be present in the saliva. The collected saliva samples were dropped off by the permanent staff, the same day, in the dedicated collection stand and all the collected tubes were then immediately transferred to the COVID-19 lab of the University of Liège for analysis.
Before RNA extraction, salivary samples were heated in order to inactivate virus that might have been located on the outside of the tube or in the screw thread of the cap. Thereafter, after RNA extraction, samples were analyzed using a RT-qPCR method as previously described16,17 to detect the presence of the SARS-CoV-2. The test result could be negative, positive or uninterpretable. In some cases, the analysis could not be performed due to non-compliant samples.
Blood samples
Blood samples were collected monthly for the “La Maison Vésale” and the “Jolimont” cohorts and 15 days, 3 months and 6 months after either a vaccination or a natural COVID-19 infection for the “University of Liège” cohort in order to determine the magnitude of antibody responses over time and the ability of these antibodies to neutralize SARS-CoV-2. Blood samples were taken by nursing home and hospital nurses. At each time point, a 10 mL serum tube was collected and stored at 4°C until its transfer to the laboratory.
Quantification of anti-SARS-Cov-2 IgG antibodies
The anti-SARS-CoV-2 IgG antibody level was determined by using the Diasorin LIAISON® SARS-CoV-2 TrimericS IgG kit (Diasorin, Stillwater, United States) according to manufacturer's instructions as previously described. 18 The assay was run on a LIAISON XL analyzer (Diasorin, Stillwater, United States). The total anti-Spike IgG antibody concentration measure was expressed as Binding Antibody Units/mL (BAU/mL) with a range from 4.81 to 2080 BAU/ml. Results below 4.81 BAU/mL were reported as “< 4.81 BAU/mL”. Samples with IgG > 2080 BAU/mL were automatically diluted with the LIAISON® TrimericS IgG Diluent Accessory (dilution factor: 1:20). After dilution, values above 41600 BAU/mL were reported as “> 41600 BAU/mL”. The cut-off for positivity was ≥ 33.8 BAU/mL. The clinical sensitivity is 98.7% and the specificity is 99.5%.
Neutralizing antibody titer assay
The neutralizing antibody titer assay was performed as previously described. 16 Briefly, serum samples were heat-inactivated for 40 min at 56°C and two-fold serial dilutions, starting from 1:10 up to 1:640, were performed in triplicate leading to final test dilutions running from 1:20 to 1:1280. Serum dilutions were mixed vol/vol with 100 TCID50 (50% tissue culture infective dose)/reaction of SARS-CoV-2 virus (strain BetaCov/Belgium/Sart- Tilman/2020/1) and were incubated at 37°C for 1 h in a humidified atmosphere with 5% CO2. Then the mixture was transferred onto a confluent Vero E6 cells (ATCC® CRL-1586) monolayer in triplicate. Cytopathic effect (CPE) was evaluated under light microscopy by two independent people 5 days post-infection. Serum dilutions showing CPE were considered as negative (non-neutralizing), while those showing no CPE were considered as positive (neutralizing). Neutralizing antibody titer was reported as the highest dilution of serum that neutralizes CPE in 50% of the wells (NT50).
Data management
For the “La Maison Vésale” cohort, data were collected using the web platform on research electronic data capture (REDCap; University Vanderbilt, 2021). For the “University of Liège” cohort, similar data were collected on a dedicated web platform developed at University of Liège. For the “Jolimont” cohort, data were collected via forms completed manually by participants and electronically encoded by the study staff.
The data included the type of person (resident or permanent staff), age, sex, comorbidities, dates of vaccination and type of vaccines, presence of confirmed cases of COVID-19, the weekly salivary test results and the serological results of each participant.
Statistical analysis
Descriptive analyses were performed to summarize participant characteristics. Accordingly, independent categorical variables were presented with frequency and percentages whereas quantitative variables were described with mean ± standard deviations (SD), according to their distribution. The dependent variables, namely anti-SARS-CoV-2 neutralizing and IgG antibodies were log-transformed and presented as mean ± SD.
Assessment of anti-SARS-Cov-2 antibodies during the study protocol in “La Maison Vésale”
Linear mixed models were employed to examine the neutralizing antibodies and IgG levels over time measured in months after primo-vaccination and after boost with time being treated as continuous. Individual participant level was modelled as a random effect.
First, the mixed models including both main and interaction effects were performed with age categories (under 65 years old and from 65 years old and above), time (measured as months), and groups (depending on the infection and vaccination status). Subsequently, gender, types of vaccine, and comorbidities were added. For better model performance, the measurements of anti-SARS-CoV-2 neutralizing and IgG antibodies were log10-transformed. Assumptions of normality and homoscedasticity were verified by employing the histograms and normal quantile-quantile plots. When assumptions of normality were severely violated, robust linear mixed model was used to account for the impact of outliers.
Missing values concerning anti-SARS-CoV-2 neutralizing and IgG antibody levels were treated as missing at random. Post-hoc analyses of group differences were performed with Bonferroni correction. Group differences were expressed as geometric mean ratio (GMR) with 95% Confidence Interval (CI), derived by back-transforming the log10-scale estimates to the original scale of the anti-SARS-CoV-2 IgG and neutralizing antibodies. Accordingly, a GMR of 1 means no difference, higher than 1 means superior and lower than 1 inferior. A two-sided p-value <0.05 was considered statistically significant.
Comparison of anti-SARS-CoV-2 antibody levels between the Alzheimer's residents from “La Maison Vésale” cohort and participants older than 55 from the “Jolimont Hospital” and the “University of Liège” cohorts
For this analysis, only residents from the “La Maison Vésale” cohort and participants older than 55 from the “Jolimont” and “University of Liège” cohorts were included.
As for the measurement after boost, as we had one measurement (after one month), a linear regression was performed instead of the mixed model with age categories, groups, and the relevant covariates presented in the previous section.
All analyses were performed in R (R Core Team, 2021).
Results
Infection occurrence over time at “La Maison Vésale”
The timeline of the detected positive cases and periods during which the mask has been worn again is shown in Figure 2. During the study, the nursing home experienced 3 waves of COVID-19: one in spring 2021, one in summer 2021 and one during winter 2022. Most of the PCR positive participants belonged to the group of residents. Indeed, 11.8% of the permanent staff members and 26.1% of the residents were detected positive during the protocol. During these waves, mask wearing was again mandatory. In April 2021, participants were forced to wear the masks anew because a non-participating permanent staff member was tested positive to COVID-19 (Figure 2). During December 2021, the mask was not mandatory despite a detected positive case because the concerned person had not been in contact with the residents or the other staff members.

Timeline of confirmed salivary positive tests among residents and permanent staff members and the periods of time during which the mask was again mandatory. The participants were weekly submitted to a salivary diagnostic test followed by RT-qPCR assay in order to detect any staff member (red line) or resident (green line) positive to SARS-CoV-2. During the study protocol, the permanent staff were allowed to remove mask during their working days and during the contacts with the residents but mask removing was forbidden when COVID-19 positive cases were detected among staff or residents. The result of a negative PCR test for all participants allowed mask removing again ending the mandatory mask-wearing period (blue boxes).
All PCR positive individuals presented mild to moderate symptoms (cough, sore throat, headache, fever, …), and some were even completely asymptomatic. No hospitalizations were necessary following these detections, and no deaths were reported.
Assessment of anti-SARS-Cov-2 neutralizing and IgG antibodies in “La Maison Vésale”
Study population
A total of 103 participants from “La Maison Vésale” were enrolled in the study (Figure 3), including 69 residents and 34 permanent staff members. Thirteen of them were excluded due to missing data. Due to the small number of uninfected/unvaccinated participants (n = 1) and infected/unvaccinated participants (n = 6), they were excluded from the analyses. We then only kept participants who were vaccinated with mRNA vaccine (Pfizer BNT162b2 and Moderna mRNA-1273) and thus excluded 4 participants vaccinated with Johnson & Johnson Ad26.COV2.S or Sanofi/GSK. The analysis was performed on the 79 remaining participants distributed between 55 residents and 24 permanent staff members. Five participants deceased during the study and 5 withdrew from the study.

Follow-up flow diagram representing participant selection and their repartition in groups for antibody analysis.
These 79 participants were distributed into 5 groups based on the vaccination and infection timing status as detailed below; to establish the infected before primo vaccination subgroup, the anti-SARS-CoV-2 IgG antibody level was determined on blood samples collected 10 days before vaccination.
Group 1: Vaccinated/Non-infected (n = 15) Group 2: Vaccinated/Infected before primo-vaccination (n = 41) Group 3: Vaccinated/Infected before and after primo-vaccination (n = 10) Group 4: Vaccinated/Infected after primo-vaccination (n = 5) Group 5: Vaccinated /Infected after boost (n = 8)
Descriptive analyses of the participants
The characteristics of the five participant groups are presented in Table 1. Among the 79 retained participants, 56 were women and 23 were men. The age ranged from 24 to more than 90 years old. All participants but one who received the Moderna mRNA-1273 vaccine were first primo-vaccinated with the Pfizer BNT162b2 vaccine. Among them, 84.8% were boosted with the Pfizer BNT162b2 vaccine while the remaining did not receive the booster. Ten permanent staff members and 41 residents were seropositive before the primo-vaccination.
Regarding the clinical characteristics of the participants, only resident information was provided. Hypertension, diabetes, renal failure and obesity were the most commonly observed diseases. Some participants presented more than one clinical risk factors.
Participant characteristics of the “La Maison Vésale” cohort.

Means ± SD of log-transformed anti-SARS-CoV-2 neutralizing and IgG antibodies after primo-vaccination and booster are presented for the different groups in Tables 2 and 3. Data are presented over time after primo and booster vaccination, respectively. Only groups 1, 2 and 5 were included in Table 2 and all groups except group 5 were considered in the Table 3.
Mean and standard deviation of log-transformed neutralizing and IgG antibodies measured over time in months (M) after primo-vaccination.

Data are presented as Mean ± (Standard Deviation). M: Month after primo vaccination; NA: not applicable
Mean and standard deviation of log-transformed neutralizing and IgG antibodies measured over time in months (M) after booster-vaccination.

Data are presented as Mean ± (Standard Deviation). M: Month after booster vaccination; NA: not applicable.
Determinants of anti-SARS-Cov-2 neutralizing and IgG antibodies measured after primo-vaccination
Different factors were considered including age (as two categories, namely under 65 and from 65 years and above), gender, comorbidities (obesity, diabetes, hypertension, chronic obstructive pulmonary disease [COPD], respiratory failure, renal failure, cancer and transplantation), and the infection/vaccination status of the participants.
Apart from age categories, time (measured in months), and groups which were included in the main model, none of the covariates including gender, types of vaccine, and comorbidities were found to be significant as shown in Table 4. The results are presented, therefore, with age, groups, and time as main determinants or significant predictors of anti-SARS-CoV-2 neutralizing and IgG antibodies over time.
Factors related to neutralizing and IgG antibodies after primo-vaccination.

NA: not applicable.
Groups 1 (n = 15) and 5 (n = 8) were combined and compared with group 2 (n = 41), which represents participants infected before primo-vaccination. Due to the low number of measurements at month 1 after primo-vaccination (n = 3) and months 9, 10, 12, 13 (n = 1 for each), the model was only fit from months 2 to 8.
Concerning main effects, the model attempted to investigate the effects of age, time (measured in months after primo-vaccination) and groups, namely infected before primo-vaccination (n = 41) and non-infected or naïve primo-vaccinated (n = 23).
As revealed in Table 5, age had a significant effect such that participants from 65 years old and above presented lower levels of neutralizing antibodies than those under 65 years old (GMR = 0.277, 95%CI: 0.108–0.704). The same observation was observed for anti-SARS-CoV-2 IgG (GMR = 0.065, 95%CI: 0.017–0.248). Participants infected before primo-vaccination had higher levels of neutralizing antibodies than naïve primo-vaccinated ones (GMR =9.850, 95%CI: 3.571–27.143). Moreover, time had a significant negative effect on IgG (p < 0.001) but not on neutralizing antibodies. Accordingly, as per one month increase, the participants showed a 41.5% decline in the IgG level.
Effects of age, group, time and the respective interaction effects on the levels of neutralizing and IgG antibodies after primo-vaccination.

CI: confidence interval; GMR: Geometric Mean Ratio; Ref.: Group with Ref. (Referenced) is the referenced group, to which the others are compared.
Concerning interaction effects, a significant interaction between groups and time was observed. Indeed, over time, participants who were infected before primo-vaccination (group 2) showed a significantly faster decrease in the neutralizing antibody levels than the naïve primo-vaccinated participants (groups 1 and 5) (the decline accelerated to 12.6% as per time unit; Figure 4). On the opposite, the infected before primo-vaccination group showed a significantly slower decrease in the IgG than the naïve primo-vaccinated group (the decline slowed by 31% as per time unit; Figure 4). Moreover, as for age, over time, the slope of IgG decreased to a significantly lesser extent in participants over 65 years old compared to those under 65 years old (the decline slowed by 14.2% as per time unit; Figure 5). However, although this tendency was also observed for neutralizing antibodies, this was not significant (p = 0.225; Figure 5).

Evolution of neutralizing and IgG antibodies after primo-vaccination over time according to groups. Time is measured in months after primo-vaccination.

Evolution of neutralizing and IgG antibodies after primo-vaccination over time according to age categories. Time is measured in months after primo-vaccination.
The interaction effect between age categories and groups was examined in post-hoc comparisons presented in Table 6. Participants infected before primo-vaccination had higher neutralizing antibody levels than those not infected or naïve primo-vaccinated across the two age categories (Figure 6). There was no significant difference in the IgG levels between participants infected before primo-vaccination and their naïve primo-vaccinated counterparts under 65 years old (p = 0.071; Figure 6). However, among older participants, the naïve primo-vaccinated individuals had significantly lower IgG level than the previously infected ones (GMR = 0.009, 95%CI: 0.002–0.035; Figure 6). Within the naïve primo-vaccinated group, the younger participants presented higher levels of neutralizing antibodies (GMR = 2.541, 95%CI: 0.908–7.111), and significantly higher levels of IgG than older ones (GMR = 7.890, 95%CI: 1.560–39.905) (Figure 6). By contrast, within the infected before primo-vaccination group, participants under 65 years old presented lower levels of neutralizing and IgG antibodies. However, the results were not significant. Significantly lower neutralizing antibody levels were found among younger naïve primo-vaccinated participants compared to the older participants infected before primo-vaccination (GMR = 0.103, 95%CI: 0.044–0.240; Figure 6). This observation also applied to IgG antibodies (GMR = 0.073, 95%CI: 0.019–0.277; Figure 6). On the other hand, the older naïve primo-vaccinated participants presented significantly lower neutralizing antibody levels than younger participants infected before primo-vaccination (GMR = 0.078, 95%CI: 0.025–0.241; Figure 6). The same tendency was observed for IgG antibodies (GMR = 0.023, 95%CI: 0.004–0.138; Figure 6).

Evolution of neutralizing and IgG antibodies after primo-vaccination grouped by age categories and group. Time is measured in months after primo-vaccination.
Post-hoc comparisons of neutralizing and IgG antibodies after primo-vaccination.

CI: confidence interval; GMR: Geometric Mean Ratio; Ref.: Group with Ref. (Referenced) is the referenced group, to which the others are compared.
Determinants of anti-SARS-Cov-2 neutralizing and IgG antibodies measured after booster vaccination
The same factors, including age (as two categories, namely under 65 years old and from 65 years old and above), gender, comorbidities and the infection/vaccination status of the participants were considered.
Just as it was the case after primo-vaccination, none of the covariates showed a significant effect as presented in Table 7. The results are presented, therefore, with age, groups, and time as main determinants or significant predictors of anti-SARS-CoV-2 neutralizing and IgG antibodies over time, with the model being fitted from months 1 to 5 after boost. Results are presented in Table 8.
Factors related to neutralizing and IgG antibodies after booster-vaccination.

NA: not applicable.
Effects of age, group, time and the respective interaction effects on the levels of neutralizing and IgG antibodies after booster vaccination.

CI: confidence interval; GMR: Geometric Mean Ratio; Ref.: Group with Ref. (Referenced) is the referenced group, to which the others are compared.
After booster vaccination, no significant effect of age categories and group was observed either for the neutralizing or IgG antibodies. However, time had a significant negative effect (p < 0.001), meaning that the neutralizing and IgG antibodies significantly decreased by 29% and 38% as per time unit respectively over time. For this reason, no post-hoc pairwise comparisons were performed.
Considering the interaction effect, there was no significant effect of group but a significant interaction effect over time was found. Accordingly, participants infected before primo-vaccination and those infected before and after primo-vaccination had their neutralizing and IgG antibody levels decreasing to a lesser extent than naïve primo-vaccinated and boosted ones with all p-values <0.001 (Figures 7–9).

Evolution of neutralizing and IgG antibodies over time after booster vaccination according to groups. Time is measured in months after booster-vaccination.

Neutralizing and IgG antibodies over time after booster vaccination according age categories. Time is measured in months after booster-vaccination.

Evolution of neutralizing antibodies and IgG over time after booster vaccination according age categories and groups. Time is measured in months after booster-vaccination.
Compared to naïve primo-vaccinated individuals, those infected before vaccination showed a 27% slower decline in neutralizing antibodies and 17% slower IgG antibody decline as per time unit. Those infected before and after vaccination provided even stronger protection, reducing decline rates by 63% for neutralizing antibodies and 62% for IgG antibodies.
Comparison of anti-SARS-Cov-2 neutralizing and IgG antibody levels between participants suffering from Alzheimer's disease or dementia and their disease-free counterparts
As far as we know, no study has ever evaluated the immune response induced by COVID-19 vaccines or natural infection in Alzheimer's or dementia residents compared with unaffected people of similar age. We thus performed analyses to determine if residents from “La Maison Vésale” developed an equivalent immune response than participants over 55 years old from the “Jolimont” and the “University of Liège” cohorts. For this purpose, we followed and compared the levels of anti-SARS-CoV-2 neutralizing and IgG antibodies between these 3 cohorts. As the Jolimont study has only been conducted from Augustus 15, 2021 to December 20, 2021, which corresponded to months 6 to 8 after primo-vaccination and month 1 after boost, we were forced to keep, for the 2 other cohorts, only data collected during the same period and corresponding to the same timepoints after primo-vaccination and boost.
Study populations
The “La Maison Vésale” cohort (Figure 10)
For this analysis, 3 of the 55 vaccinated residents from the initial cohort were excluded because of a lack of data for the timepoints M6 to M8 after primo-vaccination. The immune response occurring after primo-vaccination was thus analyzed on 52 participants. Similarly, data for M1 after boost were missing for 6 out of 55 residents. The immune response occurring after boost was therefore investigated on 49 participants.

“La Maison Vésale” cohort: follow-up flow diagram representing participant selection and their repartition in groups for antibody analysis and comparison with participants over 55 years old from the “Jolimont” and “SARSSURV” cohorts.
The “Jolimont” cohort (Figure 11)
A total of 124 permanent staff members of the Jolimont hospital were enrolled in the study. From these 124 participants, 98 were under 55 years old and were therefore excluded. The 26 remaining participants were all vaccinated with Pfizer/BioNTech or Moderna vaccine. For the analysis of the immune response after primo-vaccination, 4 of the 26 remaining participants were excluded because of a lack of data for timepoints M6 to M8 after primo-vaccination. The analysis was thus performed on 22 participants. For the analysis of the immune response after boost, 16 out of the 26 selected participants were excluded because of a lack of data for the timepoint M1 after boost. The analysis was thus performed on the remaining 10 participants.

“Jolimont” cohort: follow-up flow diagram representing participant selection and their repartition in groups for antibody analysis and comparison with residents from “La Maison Vésale” cohort and participants over 55 years old from the “SARSSURV” cohort.
The “University of Liège” cohort (Figure 12)
A total of 1706 staff members and students of the University of Liège were enrolled in the SARSSURV study. For this manuscript, only the vaccinated participants who were over 55 years old at the time of the Jolimont study (from Augustus 15, 2021 to December 20, 2021) were included. From the 1706 participants, 359 were excluded because of a lack of data or study withdrawing and 42 because they were unvaccinated. From the 1305 remaining participants, 164 were over 55 years old. This group included 1 student and 163 personal staff members. These remaining participants were all vaccinated with Pfizer/BioNTech or Moderna vaccine. For the analysis of the immune response after primo-vaccination, 131 out of the 164 remaining participants were excluded because of a lack of data for timepoints M6 to M8 after primo-vaccination. The analysis was thus performed on 33 participants. For the analysis of the immune response after boost, 56 out of the 164 selected participants were excluded because of a lack of data for the timepoint M1 after boost. The analysis was thus performed on 108 participants.

“SARSSURV” cohort: follow-up flow diagram representing participant selection and their repartition in groups for antibody analysis and comparison with residents from “La Maison Vésale” cohort and participants over 55 years old from the “Jolimont” cohort.
The participants were distributed into 4 groups: Group 1: Vaccinated/Non-infected (V); Group 2: Vaccinated/Infected before primo-vaccination (IV); Group 3: Vaccinated/Infected after primo-vaccination (VI); Group 4: Vaccinated/Infected before and after primo-vaccination (IVI).
Descriptive analysis of the participants
Tables 9 and 10 present participants’ characteristics from the 3 cohorts.
Participant characteristics of the 3 cohorts for the analysis of immune response after primo-vaccination.

SD: standard deviation.
Participant characteristics of the 3 cohorts for the analysis of immune response after boost.

SD: standard deviation
For the analysis of the immune response after primo-vaccination, a total of 107 participants were retained, among whom 63 were female and 44 were males. Most of the participants (84.1%) were primo-vaccinated with the Pfizer BNT162b2 vaccine and the remaining with Moderna mRNA-1273 vaccine. Fifty-seven participants (53.3%) were seropositive before the primo-vaccination. Regarding age, the mean age of the “La Maison Vésale” cohort (82 ± 8.56) was higher than the 2 others (58.4 ± 2.82 and 59.4 ± 2.55).
For the analysis of the immune response after boost, a total of 167 participants were included (56.9% females and 43.1% males). Fifty-two participants (31.1%) were seropositive before the primo-vaccination. Regarding age, the mean age of the “La Maison Vésale” cohort (82 ± 8.5) was higher than the 2 others (58.3 ± 2.41 and 60 ± 2.6).
Mean ± SD of log-transformed anti-SARS-CoV-2 neutralizing and IgG antibodies of the different cohorts and groups after primo-vaccination and boost are presented in Tables 11 and 12, respectively. Data are presented over time (in months) after primo and booster vaccination, respectively.
Mean and standard deviation of log-transformed neutralizing and IgG antibodies measured over time in months after primo-vaccination for the 3 cohorts.

Data are presented as Mean ± (Standard Deviation). Ab: antibodies; M: Month after primo-vaccination; NA: Not Applicable; SD: Standard Deviation; V: Vaccinated/Non-infected; IV: Vaccinated/Infected before primo-vaccination; VI: Vaccinated/Infected after primo-vaccination; IVI: Vaccinated/Infected before and after primo-vaccination.
Mean and standard deviation of log-transformed neutralizing and IgG antibodies measured over time in months (M) after boost for the 3 cohorts.

Data are presented as Mean ± (Standard Deviation). Ab: antibodies; M: Month after booster-vaccination; NA: Not Applicable; SD: Standard Deviation; Ab: antibodies; V: Vaccinated/Non-infected; IV: Vaccinated/Infected before primo-vaccination; VI: Vaccinated/Infected after primo-vaccination; IVI: Vaccinated/Infected before and after primo-vaccination.
Determinants of anti-SARS-Cov-2 neutralizing and IgG antibodies measured after primo-vaccination
Different factors were considered including age, gender, and the infection/vaccination status of the participants.
Results of the mixed model are presented in Table 13. Concerning main effects, it appeared that time had a significant positive effect on anti-SARS-CoV-2 IgG (p < 0.001) but it was not significant for neutralizing antibodies. Moreover, we found a significant difference in neutralizing antibodies and IgG levels as a function group based on vaccination profile. Indeed, the infected before primo-vaccination group displayed significantly higher neutralizing antibodies and IgG than the infected after primo-vaccination group. Yet, the GMRs and the respective 95%CIs were inflated with, which might be attributed to the small number of group size (n = 7) and thus should be interpreted with caution. However, adjusted for group, age and sex, no significant difference in the neutralizing and IgG antibody levels between the 3 cohorts was observed. Concerning interaction effects, a significant interaction between groups and time was observed for neutralizing antibodies (p = 0.011) and IgG (p < 0.001).
Linear mixed model results for the difference in neutralizing and IgG antibodies after primo-vaccination.
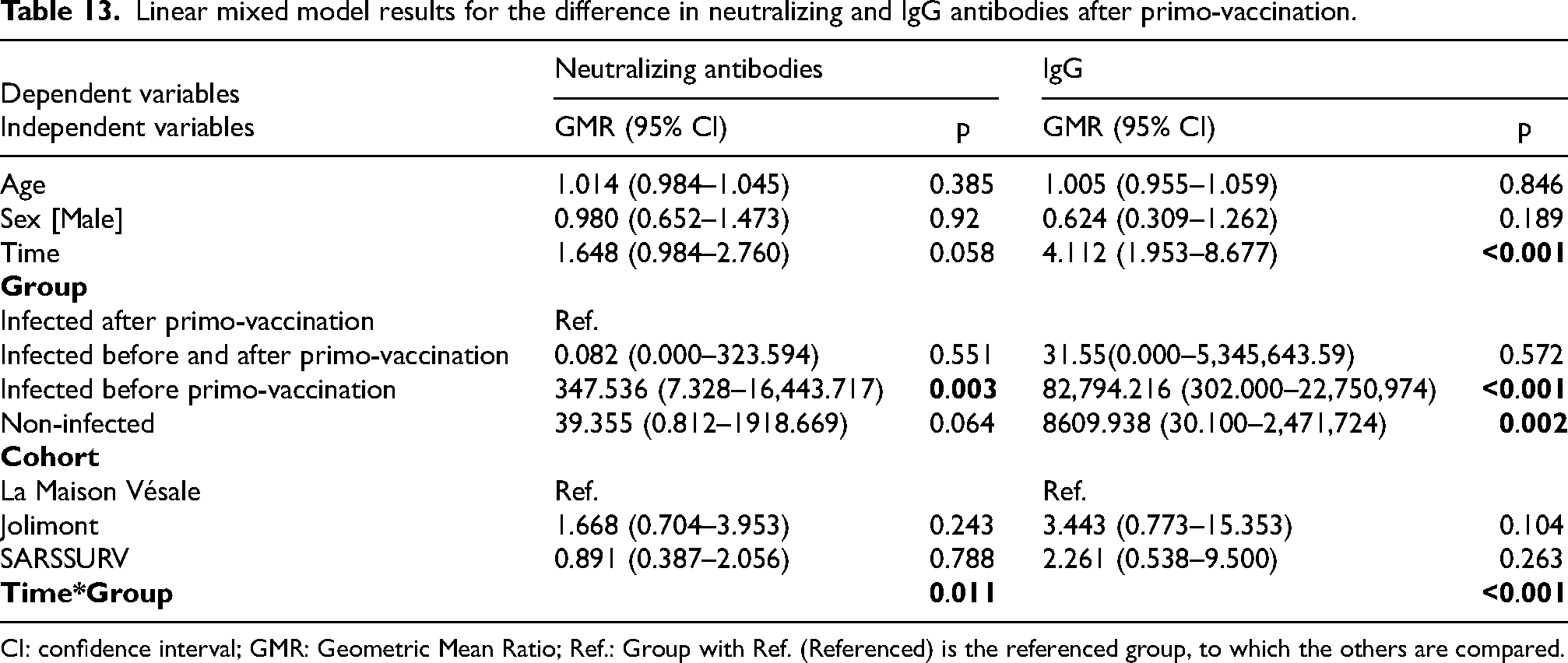
CI: confidence interval; GMR: Geometric Mean Ratio; Ref.: Group with Ref. (Referenced) is the referenced group, to which the others are compared.
Determinants of anti-SARS-Cov-2 neutralizing and IgG antibodies measured after booster vaccination
Different factors were considered including age, gender, and the infection/vaccination status of the participants.
The linear regression models were performed with age, groups and cohorts as described above. The results are presented with age categories, gender, groups and cohorts as main determinants or significant predictors of neutralizing and IgG antibodies measured one month after booster vaccination.
Results of the linear regression model are presented in Table 14. These results indicated that groups remained a significant factor for the difference in the neutralizing antibody levels. Indeed, the non-infected primo-vaccinated group had significantly lower levels of neutralizing antibodies than the infected before primo-vaccination group (GMR = 0.466, 95%CI: 0.313–0.692). Adjusted for group, age and sex, no significant difference in the neutralizing antibody levels was observed between the 3 cohorts. However, surprisingly, the “University of Liège” participants presented significantly lower levels of IgG than “La Maison Vésale” participants (GMR = 0.460, 95%CI: 0.221–0.957).
Linear regression model results for the difference in neutralizing and IgG antibodies after boost.

CI: confidence interval; GMR: Geometric Mean Ratio; Ref.: Group with Ref. (Referenced) is the referenced group, to which the others are compared.
Discussion
In this study, we proposed a protocol aiming at maintaining social interactions for Alzheimer's disease residents from a Belgian nursing home. For this purpose, we strictly followed the SARS-CoV-2 carriage and the level of anti-SARS-CoV-2 IgG and neutralizing antibodies among all studied participants while staff members participating to the study were allowed to remove their mask to ameliorate contact with residents. During this protocol, the nursing home encountered 3 waves of COVID-19 infections which were rapidly contained by the strict quarantine policy. We confirmed that people infected before primo-vaccination developed a stronger immune response than inexperienced ones and that seniors had a lower level of immunity than younger participants. We also demonstrated for the first time that ADRD patients were able to develop an immune response as strong as that of disease-free elderly people.
Nursing homes from many European countries have been severely impacted by the COVID-19 pandemic.2–6,19 In this study, we were interested in “La Maison Vésale” (Bruxelles, Belgium), a rest and nursing home that hosts only residents who were suffering from ADRD in various stages of dementia. The inability to recognize people wearing masks and analyze their facial expressions led to distress among residents. 20 The physical and mental deterioration of residents also caused discomfort among caregivers. This context led us to implement the previously described protocol, aimed at maintaining correct social interactions while limiting the risk of infection.
The screening test was performed using a non-invasive salivary-based RT-qPCR assay that has already demonstrated its effectiveness in disrupting the chain of transmission in nursing homes leading to a significant decrease in the number of absent workers and deaths among residents, and this without further disturbing the residents. 17 Non-invasive salivary sampling was appropriated for this population of people with ADRD problems and moreover, these salivary diagnostic tests were highly effective in identifying infected but asymptomatic individuals. Most of the infected people were residents (26.1% compared to 11.8% for staff members) probably because this population lives in environments facilitating the spread of the virus (close quarters, frequent and close contacts with caregivers, group gathering, etc.). We have only taken into account the positive cases revealed by the salivary diagnostic tests and not by traditional nasal swabs or antigenic tests which were not part of the study protocol; however, some staff members, sick at home, were detected positive by these techniques and their positivity were not included in the results probably accounting for a part of the difference between resident and staff SARS-CoV-2 prevalence during the study. We may also have underestimated this prevalence among residents and staff since, sometimes, some of them were hospitalized, did not cooperate or were not working on the day of sampling.
The first wave of COVID-19 infection occurred in spring 2021 where the variant of concern (VOC) circulating in Belgium at this time was the Alpha one, 21 known to mainly affect younger people and to be associated with higher transmissibility and increased risk of hospitalization or intensive care unit (ICU) admission and mortality than the pre-existing variants.22–24 However, this wave in our study only concerns one asymptomatic resident detected by the salivary diagnostic test. This elderly person was vaccinated four months earlier which could explain the efficient protection against the severe form of the disease. The next wave of infection, detected by the salivary test, occurred during summer 2021, when the VOC circulating in Belgium was the Delta one, 21 and only affected four residents with mild to moderate symptoms that did not require hospitalization although the Delta variant was associated with a higher disease severity and risk of hospitalization, ICU admission and mortality.25,26 The four positive residents were all vaccinated with Pfizer BNT162b2 which has been shown to provide a protection against the Delta VOC that is almost as effective as that observed for Alpha variant, which could partly explain the low number of positive cases and the mildness of the symptoms. 27 Finally, “La Maison Vésale” encountered a third wave during winter 2022 that affected 17 persons (four staff members and 13 residents) who were either asymptomatic or developed mild to moderate symptoms. The first positive case occurred when the Delta and Omicron variants cohabitated in Belgium, the other cases when Omicron was the VOC. 21 Omicron has been shown to be more transmissible than other variants but to induce lower severe symptoms.28–30 This could account for the increased number of positive mild cases encountered during this 3rd wave compared to the previous ones.
Our study is the first to investigate and follow, on a regular basis in a period of one year, the levels of anti-SARS-CoV-2 neutralizing and IgG antibodies on such cohort.
Results revealed that the type of vaccine, gender and comorbidities had no significant effect on the evolution of neutralizing antibodies and IgG levels after primo-vaccination or after the booster. Concerning the type of vaccine, no conclusion could be drawn with our cohort because only one participant received the Moderna mRNA-1273 vaccine while all the others were vaccinated with Pfizer BNT162b2. The absence of correlation between comorbidities and IgG levels or neutralizing antibodies in our study is in line with other studies also evaluating these parameters in elderly people.31–34 On the contrary, Virgilio and colleagues showed that diabetes affected antibody responses to SARS-CoV-2 vaccination in elderly residents from long term care facilities 35 ; this difference could perhaps be explained by the fact that the no diabetes participants from this cohort had a higher prevalence of previous COVID-19 infection which has been shown to boost the antibody response to SARS-CoV-2 vaccination in several studies.18,32,36–38 Pannus and collaborators also suggested a role for health status and thus comorbidities on the antibody response to vaccination but did not demonstrate their hypothesis. 37 However, a limitation of our study is the small cohort size and the presence of relatively few comorbidities. We detected no significant effect of gender regarding the evolution of antibody responses which has been related by others,18,39 although these studies focused on younger cohort than ours. Terpos and collaborators reported an effect of gender on the level of IgG and neutralizing antibodies mostly in octogenarians. 40
Our study, in line with others,37,40–44 showed significant lower IgG and neutralizing antibody responses in participants over 65 years old compared with the younger ones, a difference that could be attributed to immunosenescence and inflammaging in elderly individuals. 45 Parry's team has not observed a correlation between age and the antibody response 38 ; however, this could be explained by the fact that they focused on a cohort of over 80 years old people without comparing them to younger participants. When regarding the infection status of the participants in our study, naïve primo-vaccinated people under 65 years old presented higher IgG antibodies than the elderly individuals. This suggests a stronger immune response to vaccination of the younger as described before. A similar observation was done for neutralizing antibodies but was not significant. On the contrary, infected before primo-vaccination participants over 65 years old showed higher IgG and neutralizing antibodies than the under 65 years old group, although this was not significant. This could be explained by the fact that elderly people, when infected before primo-vaccination, developed more severe forms of the COVID-19 giving rise to a more intense immune response. This was correlated to other studies showing a higher and more persistent immune response in convalescent patients recovering from a severe form of the disease compared to others recovering from a moderate disease.46,47 Pannus and collaborators obtained similar but significant results for IgG and neutralizing antibodies when comparing naïve primo-vaccinated residents and staff but showed no significant difference in IgG and neutralizing antibodies between the infected before primo-vaccinated groups. 37 However, this study has only followed the participants for 4 weeks after primo-vaccination.
As expected, the levels of IgG significantly decreased over time and confirmed a reduced vaccine protection with time which could explain the few positive cases observed in our cohort in summer 2021 48 ; however, the apparition of new variants could also be incriminated as the VOC circulating at this time was the Delta one that has been shown to be more transmissible than the previous Alpha one.21,28 Fortunately, although this decrease in IgG levels, vaccine efficacy or effectiveness against severe disease remained high. Indeed, the humoral response is not the only weapon of adaptative immunity and cell responses have also been suggested to play a key role in protection against COVID-19.49–51
Surprisingly, we observed that participants over 65 years old presented a slower IgG decrease than the younger group. However, this difference could be explained by the fact that older participants began with lower IgG antibody levels at month 2 than the under 65 years old participants and even if the proportion of decrease in antibody between month 2 and 8 was similar for the 2 groups, the slope was higher for the younger individuals. A tendency to a decrease over time was also observed for neutralizing antibodies but was not significant, suggesting that anti-SARS-CoV-2 neutralizing antibodies maintained longer than anti-SARS-CoV-2 IgG. These results were also observed by Levin and collaborators who followed the antibody kinetics of a large cohort of health care workers until 6 months after primo-vaccination. 41 A longer longevity of neutralizing antibodies, compared to IgG, has also been shown by Terpos and colleagues, with female maintaining higher level of antibodies over time. 40
We also demonstrated, as other studies,18,31,32,37,38,52 that people infected before primo-vaccination displayed higher neutralizing antibody levels than naïve primo-vaccinated participants regardless of the age group. A similar tendency was observed for IgG but without signification in this case. This potentiating effect of a pre-infection on the humoral response could be attributed to the “hybrid immunity” phenomena described by Crotty where natural immunity to SARS-CoV-2 is combined to vaccine-induced immunity to give a larger-than-expected immune response. 53
After booster vaccination, we observed no significant effect of age or infection status-depending groups on the IgG and neutralizing antibody levels meaning that naïve vaccinated participants over 65 years old were able to achieve antibody rates equivalent to the infected groups thanks to this boost. However, we showed that IgG and neutralizing antibody levels decreased more rapidly in naïve primo-vaccinated and boosted participants than in people infected before primo-vaccination or infected before and after primo-vaccination. These results confirmed the importance of this booster, especially for COVID-19 inexperienced older people.34,36,54 The booster was also an important weapon in maintaining sufficient immunity against the new Omicron variant appearing in Belgium at this time 21 ; Indeed, although vaccines showed less efficacy against this VOC compared to the previous Delta one, booster attenuated this effect. 55
Several studies have shown that people with dementia are associated with an increased risk of having severe forms of COVID-19 with high mortality rates.56–58 Different reasons could explain this situation: first, dementia is often associated with older people and elderly individuals are more affected by the disease; different medical care was provided to COVID-19 patients with dementia who were rarely admitted to the ICU as physicians preferred selecting younger patients with fewer comorbidities for ICU admission. 58 Furthermore, the APOE ε4 genotype is correlated with dementia and the homozygous genotype is associated with a nearly 15-fold greater risk of developing Alzheimer's disease compared to the current ε3/ε3 genotype. 59 Yet, APOE ε4/ε4 allele has been shown to increase risks of severe COVID-19 infection. 60 Another hypothesis that could be put forward is that ADRD residents have a poorer immune response to vaccine or COVID-19 infection than people of a similar age not suffering from this disease but no study has ever been dedicated to this subject. We thus compared the immune response of “La Maison Vésale” residents with 2 other groups including the over 55 years old participants from both the “University of Liège” cohort and the “Jolimont” cohort staff members. We acknowledge that the selection of these cohorts for comparison with residents of the “La Maison Vésale” cohort was a convenience sample, given that we had this data available from a parallel study. However, the average age of individuals in the other two cohorts was lower than that of those in the “La Maison Vésale” cohort. The results indicating no difference in the immune response between the 3 cohorts, hence, could be considered robust, as it was expected the younger cohorts to have better immunity. We showed that the IgG and neutralizing antibody levels were not significantly different between the 3 cohorts after primo-vaccination and this was also the case for neutralizing antibodies after booster. The IgG levels were even significantly higher for the “La Maison Vésale” participants compared to those of the “University of Liège” cohort. These results showed that ADRD residents displayed an immune response at least as high as that of individuals of a similar age. Therefore, a poor immune response to SARS-CoV-2 infections or vaccines in ADRD residents could not be incriminated in the higher risk of contracting severe forms of the disease in this population.
Limitations
One might wonder about the applicability of our protocol to other nursing homes in Belgium or elsewhere in the world. From the point of view of the risk of greater spread of the virus in other facilities, we can remain confident given that “La Maison Vésale” represents one of the worst possible cases. Indeed, this nursing home is one of the few in the world, exclusively hosting a population of people who can move freely between floors, having a great deal of close contact with each other and with the nursing staff, while being completely unable to comply with barrier gestures. However, our protocol has enabled these people, who need strong human contact, to maintain social relationships without taking excessive risks to their health. However, this protocol requires sufficient staff to help residents perform weekly salivary tests, as they are not always able to do so on their own. Residents must trust the supervisory staff to prevent them from becoming defensive and refusing to provide samples, which could potentially compromise the detection of a possible positive case. In Belgium, nursing homes operate with public and private funds (rent paid by residents or donations) and facilities can use funds exceeding the financed standards to hire the type of staff they want and therefore potentially staff who can help with taking samples. However, financing systems and regulations related to nursing homes vary considerably from one country to another, making feasibility analysis difficult. Nevertheless, patients with ADRD in other nursing homes are generally confined to a section of the facility and represent only a portion of the residents present. Testing should therefore not represent a huge additional workload for staff. The PCR tests carried out following the salivary sampling also have a cost, but this could be covered by the healthcare systems of the various countries where they exist. In any case, these costs would be significantly lower than those incurred in treating these individuals if there were an uncontrolled outbreak of positive cases.
Conclusion
In conclusion, our study confirms that individuals infected before primo-vaccination develop a stronger humoral response than naïve primo-vaccinated people and that elderly individuals show a weaker immune response than younger participants; this difference was abolished by booster justifying the importance to prioritize vaccination with a booster dose for the naïve older persons. Moreover, we demonstrated that ADRD people were able to develop a similar humoral response to SARS-CoV-2 vaccination or infection to that of disease-free elderly individuals. Finally, we have shown that a strict protocol aimed at early detection of potential positive cases and following of anti-SARS-CoV-2 neutralizing and IgG antibodies has enabled ADRD residents from this nursing home to maintain appropriate social interactions, thanks to the ability of study participants to remove masks, without taking any ill-considered decisions.
Footnotes
Acknowledgements
The authors thank all the participants of the study for the time they dedicated to this longitudinal study. We also thank all the staff members of the COVID Diagnostic platform of the University of Liège, the nursing staff from “La Maison Vésale” for their help in the salivary diagnostic tests with residents and blood sampling, the nursing staff from the Jolimont Hospital for their help in blood sampling, Dr S. Gofflot and the Biobank of the University Hospital of Liège (BHUL), the laboratory of Pathology of the Faculty of Veterinary Medicine of the University of Liège, the laboratory of Clinical Microbiology of the University Hospital of Liège. We also thank Cédric François and Nathalie Guillaume for their help in the daily organization.
Ethical considerations
The protocol was approved by the local hospital's ethical committee from CHU Saint Pierre (B0762021210230) on February 8, 2021 and by the local hospital's ethical committee from CHU of Liège on March 26, 2021 (2021/96) and on May 28, 2021 (2021/198).
Consent to participate
All the participants, a trusted person or a legal representative, signed informed consent before enrolling in the study.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cellular and Molecular Immunology laboratory of the University of Liège.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.