
Abstract
Background
The advent of disease modifying therapies for dementia has highlighted the need for simple, accessible and low-cost diagnostic tests. Blood and digital biomarkers increase accuracy in highly selected research populations. However, their real-world applicability for diverse clinical populations remains unknown.
Objective
We will investigate the utility of plasma neurofilament light chain (NfL) and voice acoustic analysis in a multi-ethnic and multi-lingual population. We hypothesise that NfL and voice acoustic biomarkers will discriminate between individuals with a neurodegenerative diagnosis and those with non-neurodegenerative causes; abnormal biomarker findings will have high prognostic validity for clinical progression; and shorten the time to diagnosis and reduce costs.
Methods
All adults presenting with a cognitive concern to outpatient and inpatient settings at a community-based healthcare network in Melbourne, Australia are eligible to participate. Plasma NfL and speech sample recordings are performed at baseline and functional status (modified Rankin Scale) is recorded. Clinical diagnostic consensus meetings are convened wherein baseline diagnostic class (neurodegenerative vs non-neurodegenerative), syndrome (diagnosis), and certainty (low, moderate, high) are confirmed with the clinician prior to and following disclosure of NfL to examine effect on clinical decision-making. Participants complete cognitive, functional and mood screens and speech sampling via 12-month follow-up phone call.
Discussion
Blood and digital biomarkers are transforming the landscape of dementia diagnosis. Our study design allowing inclusion of people from diverse linguistic, cultural and racial backgrounds offers an opportunity to evaluate the utility of NfL and speech markers in real-world clinical settings.
Trial registration
https//www.clinicaltrials.gov (NCT06339190), Apr 2024.
Keywords
Introduction
Background/Rationale
The number of individuals affected by dementia world-wide is projected to reach 135 million people by 2050 and the cost of dementia care is expected to reach $USD1 trillion by 2030. 1 The time to diagnosis of dementia and type is on average 2–3 years. 2 Delays have been attributed to the complex diagnostic process, poor access to dementia and cognitive disorders clinicians, and accurate, accessible biomarkers. 2 Dementia symptoms can be nonspecific and may resemble symptoms of aging, primary psychiatric disorders (PPD) or even relationship discord, especially in young onset and atypical dementias.3,4 Family members often notice subtle changes but wait for symptoms to progress before pursuing medical follow-up. 2 During pre-diagnostic stages, people with dementia may experience disruptions to personal relationships and independence. People with young onset dementia who are in the workforce experience loss of employment, demotion and career shifts causing adverse financial consequences and reputation harm, before the underlying disease is recognised. 2 Geographic, economic, social and racial disparities result in enormous variation in access to cognitive and dementia services.5,6
There is no single gold standard test for detecting neurodegeneration and instead a combination of cognitive assessments, patient and informant history, brain imaging and cerebrospinal fluid (CSF) analysis are used. 1 Cognitive testing presents another challenge to diagnosis as most tests have been normed on educated Caucasians and do not account for an individual's cultural background, First Nations status, and educational attainment. 7 In a 10-year audit of patients from a specialist cognitive service, it was found that clinicians changed their diagnosis for roughly a quarter of patients after ongoing review. 8 This uncertainty was greater in primary care centers with over half of diagnoses at referral changed by a specialist. This highlights a degree of uncertainty when diagnosing cognitive disorders, contributing to delays in accessing services and potential disease modifying treatments.
Biomarkers can help overcome limitations associated with current diagnostic processes. Amyloid-β (Aβ) and tau biomarkers measured with positron emission tomography (PET) are reliable biomarkers of Alzheimer's disease (AD) as they reflect core AD pathology. 9 Further, CSF phosphorylated-tau (p-tau) and Aβ42 have been shown to correlate with disease onset and progression, especially in sporadic and familial AD. 10 CSF biomarkers have shown excellent diagnostic accuracy, but the lumbar puncture procedure for sample collection is perceived to be invasive and access to hospital day beds can be problematic. 11 Molecular PET scans are rarely utilized outside research settings due to their high cost and low accessibility.
More recently, brain-derived plasma proteins offer promise as biomarkers for diagnosing specific neurodegenerative diseases. 12 Plasma or serum biomarkers can be examined with a simple blood draw and have shown good correlation to CSF and Aβ PET biomarkers.11,13,14 In particular, ratios of Aβ42 to Aβ40 (Aβ42/Aβ40), p-tau181 or 217, glial fibrillary acidic protein (GFAP) and neurofilament light chain (NfL) in plasma and/or serum have shown excellent accuracy against gold standard tests.9,12 Plasma Aβ42/Aβ40 and p- 12 while elevated plasma GFAP in AD has been reported to reflect AD pathology associated neuroinflammation.9,15 Although these biomarkers show effectiveness for identifying AD, they are less useful for dementia types unrelated to Aβ pathways such as frontotemporal and vascular dementias, therefore excluding a significant proportion of dementia syndromes.
In contrast, NfL, an axonal cytoskeletal protein, is elevated in the CSF and consequently in the blood in individuals with neurodegenerative diseases and brain injury.11,13,16,17 Plasma NfL has shown a strong correlation with CSF NfL,11,13,18 and can be measured via a variety of ultrahigh sensitivity immunoassays, including single molecule array (Simoa) techniques. 19 While NfL and GFAP are non-specific biomarkers, NfL indicates more generalized neurodegeneration in contrast to specific astrocytic activity reflected with GFAP. 16 When comparing the ability of GFAP and NfL to distinguish behavioral variant frontotemporal dementia (bvFTD) from PPD, both biomarkers were successful, although NfL proved superior. 20 Plasma NfL correlates with neuroimaging changes of degeneration 13 and higher levels have been reported to predict faster cognitive and functional decline in individuals with mild cognitive impairment and AD. 9 Furthermore, NfL levels increase at a faster rate in people with AD compared to controls, exhibiting its prognostic and longitudinal monitoring potential. 9 We have demonstrated that NfL distinguishes those with FTD syndromes, FTD phenocopies, and PDD in clinical populations. 4
Research for the application of NfL in real-world clinical settings is lacking and there are currently no guidelines for its use in clinical practice. Dementia syndromes with a genetic cause such as FTD can be difficult to diagnose. NfL levels do not always distinguish individuals with genetic or slowly progressive syndromes. 21 NfL estimation is influenced by factors unrelated to neurodegenerative disease such as age,13,22 hypertension, 13 kidney disease, 22 chemotherapy, 23 body mass index, 22 and diabetes mellitus. 24 Thus, integrating a combination of clinical tests, establishing guidelines for their use in the diagnostic processes, and improving timely access to genetic testing for neurodegeneration seems necessary.
Communication can be compromised in degenerative conditions and voice acoustic markers; as digital biomarkers, are altered in some neurodegenerative conditions such as bvFTD 25 and Parkinson's disease. 26 Changes in speech can result from reduced respiratory, cognitive and motor performances. 27 These manifest in reduced breath support, poor coordination, slowing of rate, limited vocal control and reduced voice quality. Cognitive changes can also result in altered language function. For example, social communication deficits can lead to inappropriate responses or interactions, reduced processing speech can result in increased response latency, memory issues leading to word finding difficulties and attention deficits results in poor topic maintenance. 28 It is possible to capture these changes objectively via signal (speech) and natural language processing protocols. The addition of speech analytics as an objective and potentially meaningful clinical outcome assessment in suspected neurodegenerative conditions is useful in improving the diagnostic accuracy and capacity to monitor change in dementia and specific syndromes.25,26,29–31
Most prior research using biomarkers for enhanced dementia diagnosis has been done in highly-selected, Caucasian participants. 7 There has been little representation of people of Asian, Hispanic or African descent,7,32 and First Nations peoples.33,34 This highlights global research inequities in gender and ethnicity which impact healthcare delivery and dementia care.
The primary aim of the Neurofilament And Voice Acoustics In Dementia Diagnosis (NAVAIDD) study is to investigate the utility of plasma NfL in detecting neurodegenerative disease. In addition, we seek to explore the utility of voice acoustics as diagnostic biomarkers, estimate the added value of early genetic testing in people at high risk of a genetic cause for their genetic syndrome; develop diagnostic guidelines and health-care systems policies for the use of these tests in clinical practice and assess the impact of plasma NfL on clinical decision making. Additionally, we aim to evaluate the economic impact of implementing blood-based NfL and digital biomarkers to improve the early diagnosis of cognitive complaints and potential neurodegenerative disorders. By developing a health economic model, we will assess the cost-effectiveness of this approach, with the goal of demonstrating how earlier, more accurate diagnosis can lead to substantial cost savings. These savings may result from reduced reliance on unnecessary consultations, diagnostic procedures, and hospitalizations. We present a study design with minimal participant burden involving one in-person visit coinciding with presentation to clinic or whilst an inpatient at a single Australian healthcare network.
Objectives
Overall, our objective is to provide evidence that supports the integration of blood and digital biomarkers into clinical care to enhance diagnostic accuracy and support scalable health systems implementation. The primary objective of the study is to examine the diagnostic utility of NfL for distinguishing neurodegenerative diseases in a diverse clinical population. The secondary objectives are to evaluate the diagnostic performance of voice acoustic biomarkers in this cohort and to examine correlations of blood and speech biomarkers with diagnostic class, syndrome, certainty and progression. Exploratory objectives include assessing the impact of NfL on clinicians’ diagnostic certainty using a nested clinical decision-making paradigm; diagnostic genetic testing for potential monogenic variants in people at high-risk of a genetic cause; and a health economic model to determine the cost-effectiveness of these biomarkers.
We hypothesize that (1) abnormal biomarker findings are more prevalent in people with neurodegeneration versus those without brain degeneration, (2) abnormal biomarker findings will have high prognostic validity for clinical progression, (3) the use of biomarkers in initial diagnostic testing will shorten time to diagnosis and reduce costs and (4) early provision of blood biomarkers will improve diagnostic decision making.
Methods
Study design
The NAVAIDD study is a cohort study to assess the utility of NfL in diagnosing neurodegeneration in a clinical setting, designed to minimize barriers for participation. Within NAVAIDD we will conduct six studies responding to each aim (e.g., Study 1 corresponding to Aim 1, Study 2 corresponding to Aim 2 etc.).
Study 1, Estimation of plasma NfL Study 2, Analysis of speech recordings Study 3, Optional saliva sample collection for testing monogenic mutations Study 4, Roundtable discussion to inform guideline and policy recommendations Study 5, Evaluation of the impact of NfL on clinical decision-making Study 6, Optional health economic analysis using Medicare data
As per Figure 1, participants have minimal study visits, including an initial on-site visit at baseline where written consent is obtained, blood is collected, and a speech assessment is completed. This onsite visit is followed by a 12-month follow-up phone call where cognitive, functional and mood assessments and a second speech recording is administered. All study activities, excluding collection of a venous blood sample at baseline, can be completed remotely. During Clinical Diagnostic Consensus Meetings (CDCMs) clinicians discuss the impact of NfL on their diagnostic certainty.

Study design workflow of (1) participant (2) clinician and (3) research team for the study duration. Clinicians obtain verbal consent from participants and complete a referral checklist denoting diagnostic class (neurodegenerative vs non-neurodegenerative), clinical certainty (low, moderate, high), years of symptoms and provisional diagnosis. Clinicians attend clinical diagnostic consensus meetings throughout the study to re-assess checklist items for their patients after receiving NfL (pg/mL) results. Baseline procedures occur on the same day of attendance at clinic or as an inpatient and follow-up is completed remotely via telephone interview or coinciding with an outpatient appointment at 12 months. Written informed consent is obtained before completing Visit 1 procedures. Consent for health economic analysis and genetic testing are optional. Participants self-administer activities immediately after their follow up and if these are incomplete, a study coordinator will contact them to complete this.
Several guidelines; listed in Table 1, will be followed and include the STrengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines, 35 Standards for reporting of diagnostic accuracy studies (STARD), 36 Consolidated Health Economic Evaluation Reporting Standard (CHEERS) checklist, 37 and the Appraisal of guidelines research and evaluation (AGREE) reporting checklist. 38 The study is registered with the National Library of Medicine on ClinicalTrials.gov (NCT06339190). Refer to Supplemental Material 1 for detailed information of study registration data.
Guidelines utilized in the NAVAIDD study.

Setting
Hospital wards and clinics of the Eastern Health network, Melbourne, Victoria, Australia, comprising 10 hospitals. This public healthcare network captures the largest geographical area in Victorian metropolitan health services, covering metropolitan, outer suburban and rural regions. Eastern Health's catchment area also includes a significant culturally diverse network with a higher-than-average representation of Aboriginal and Torres Strait Islander peoples and approximately 25% of patients are born in a non-English speaking country. 39
Clinic and ward settings
Recruitment mainly occurs at two hospitals within the Eastern Health network: Box Hill Hospital and Wantirna Health. Three clinic sources are used, the Eastern Cognitive Disorders Clinic, Cognitive Dementia and Memory Service and Movement Disorders Program, but participants can be referred from any clinic or ward in the health care service. Patients presenting as inpatients within the hospital network are identified on ward lists for inclusion, if being investigated for a potential dementia or neurodegenerative syndrome.
Participants
Inclusion and exclusion criteria
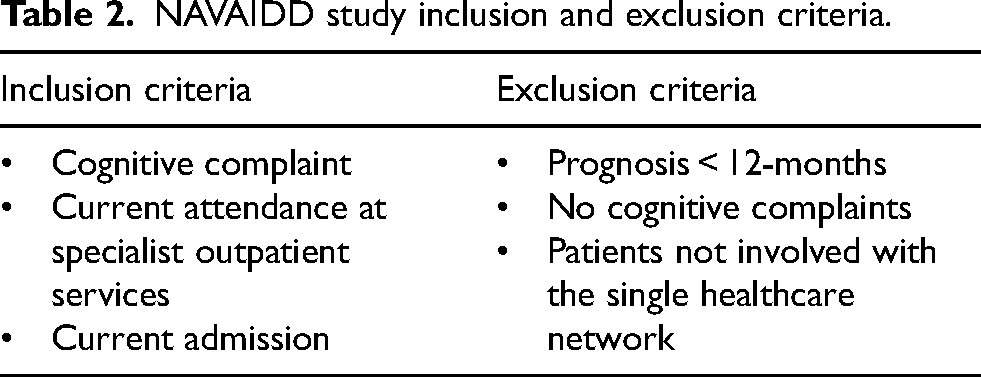
All adult patients presenting to the listed Eastern Health services with a cognitive complaint or potential neurodegenerative disorder are considered as potential study participants if they are likely to live for at least 12 months as determined by clinicians. There are no other inclusion or exclusion criteria as the findings are intended to be generalizable and to reflect the utility of NfL in real-world clinical settings (Table 2).
NAVAIDD study inclusion and exclusion criteria.
Informed consent process
The consent process is outlined in Figure 2 and participants are screened for inclusion from both outpatient and inpatient settings. Participants from the three main clinic sources are screened as eligible if they have a cognitive complaint as stipulated in a referral letter. Participants receiving letters and consent forms may contact study staff to express their interest in participation and the research team will schedule an on-site visit coinciding with their clinic appointment. Participants from inpatient settings are flagged as appropriate from ward lists by research staff and approached for participation by their respective clinicians.

Timeline of participant study visits and informed consent processes in outpatient and inpatient settings. Inpatient settings include patients from neurology and geriatric evaluation medicine (GEM) services and emergency departments. EH: Eastern Health.
Consent for main study procedures as outlined in Studies 1, 2, and 4 include:
Two encounters, including (1) baseline activities involving a single blood test and a speech recording, and (2) a phone call after 12-months to administer questionnaires and a second speech recording. Access to Eastern Health medical records to obtain relevant medical history regarding their diagnosis, as well as blood test and brain imaging results.
Optional consent can be provided for the following:
Sharing of blood test results and/or samples with other studies being conducted in Australia and internationally. Genetic testing of 14 common genes associated with dementia syndromes, for those at high risk of a monogenic cause for their disease (e.g., FTD/MND with strong family history) for Study 3. Involvement in an optional analysis of Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data for Study 6.
Declining participation in optional consent items does not impact participants’ involvement in the main study activities if they decline. All participants can withdraw their samples and/or data from the study at any point in the study.
Primary outcome
Baseline plasma NfL level (pg/mL)
Secondary outcomes
Voice acoustic and language metrics at baseline and 12 months
Exploratory outcomes
The modified Rankin Scale (mRS) assessed by a member of the research team at baseline and 12 months.
Montreal Cognitive Assessment (MoCA) assessed by a blinded rater at 12 months.
Hospital Anxiety and Depression Scale (HADS) assessed by a blinded rater at 12 months.
WHO Disability Assessment 2.0 12 item telephone interview assessed by a blinded rater at 12 months.
WHO Disability Assessment 2.0 36-item self-assessed at 12 months.
Clinical Global Impression of Change (CGI-C) assessed by a blinded rater at 12 months.
DNA testing of 14 genes (C9orf72, CHCHD10, CHMP2B, DCTN1, FUS, GRN, HNRNPA2BT, MAPT, SQSTM1, TARDBP, TBK1, TREM2, UBQLN2, VCP) from saliva samples at any time point during the study.
Study procedures
Study visits
There are 2 study visits (as detailed in Table 3). Participants have no in-person study visits above those clinically indicated. Written consent is obtained at baseline, blood and speech samples are collected, along with mRS. This aligns with presentation to clinic (out-patient) for physician review, or on the ward if an in-patient.
Participant schedule of activities during baseline and follow-up at 12 months. mRS: modified Rankin Scale 41 ; MoCA: Montreal Cognitive Assessment 42 ; HADS, Hospital Anxiety and Depression Scale 43 ; WHODAS: World Health Organization Disability Assessment Schedule 44 ; CGI-C: Clinical Global Impression of Change. 45

*Optional. Participants only conduct baseline activities once written consent is obtained, either prior to or on the day of t1. Consent for saliva samples may occur at any point during the study and participants are sent a collection tube to fill before sending this back to the research site.
Several optional consents are offered to participants including plasma and DNA biobanking of blood samples, testing of saliva for genes associated with genetic dementia syndromes, and access to Medicare data for health economic evaluation. At 12 months, a follow-up is conducted by phone or in-person and includes blinded assessment of clinical outcome measures, estimation of a second mRS score and a repeat speech sample.
Baseline (Visit 1)
After written informed consent is obtained, participants have blood collected by venepuncture, and a speech sample taken using Redenlab® software. Participant's mRS is also assessed. The mRS has been amended as a flowchart of questions for the research team to denote a number on the scale (Supplemental Material 2). Participants are asked to report their first language, place of birth and ethnicity. Ethnicity is recorded according to ‘narrow groups’ listed in the Australian Standard Classification of Cultural and Ethnic Groups by the Australian Bureau of Statistics 1249.0 (2019) (Supplemental Material 3). 40 Total time commitment of the baseline visit is approximately 30 min.
Clinicians complete a referral checklist form stating a provisional diagnosis for participants along with their impression and certainty of the presence of a neurodegenerative process (refer to Supplemental Material 4). This is used as baseline data for the purpose of our nested clinical decision-making paradigm.
12-month telephone interview (Visit 2)
Study staff contact participants via phone details shared at time of consent. A time is arranged to allow assistance from family members or interpreters if required.
An unblinded member of the research team arranges a follow up phone call or face-to-face visit for the completion of clinical outcome measures. Participants can be assessed on-site if this is their preference and it aligns with a clinic review appointment (if annual). Requisite materials are mailed to participants prior to the appointment (Supplemental Material 5). Follow up is conducted by trained raters, blinded to participants’ diagnosis and medical history.
The following scales are administered at Study Visit 2 (see study measures below): mRS 41 ; MoCA (Blind Version 8.1) 42 ; HADS 43 ; 12-item interviewer administered World Health Organization Disability Assessment Schedule 2.0 (WHODAS) 44 ; and CGI-C. 45 The 36-item, self-administered, WHODAS is sent to participants for completion after their phone call and materials are provided for participants to send this back to the research team. A second speech recording is completed by participants after their phone call by scanning a QR code with their personal devices to access Redenlab® software via a secure online portal. Speech tasks are identical to those completed at baseline. Total time commitment of the follow up and additional procedures is approximately 40 min.
Study measures
Blood biomarker acquisition (Study 1)
Participants provide 9 mL of blood via venepuncture, unfasted at the time of consent. Samples are collected in a 9 ml K3 EDTA vacuette tube (Greiner Bio-One, Kremsmünster, Austria), and cooled to 4°C in a fridge or on ice before processing. As soon as practicable, the blood is centrifuged at 4°C at 3000 rpm (approximately 1420 g) for 10 min. The plasma layer is removed and divided into nine 500 µL aliquots and stored at −80°C. One aliquot per participant is transferred on dry ice to the Florey Institute of Neuroscience and Mental Health, Austin campus, where it is stored at −80°C until thawed and processed for measurement of NfL using the Quanterix NfL Advantage PLUS Assay on the Simoa HDX Analyser (Quanterix, MA, USA).
Voice acoustic acquisition (Study 2)
Speech samples are completed by trained research staff at baseline in a private room using the AKG 520C condenser microphone connected to Redenlab® software on a laptop and a Roland Rubix 24 audio interface. If a participant cannot complete the speech tasks on site at baseline due to time constraints, a QR code is provided for participants to complete this remotely from their mobile phone, iPad or laptop.
Once complete, samples are uploaded to a desktop on a Redenlab® portal and stored de-identified with a patient identification (PID) number. This desktop is accessed by research staff to monitor retention of remote assessments. We anticipate some individuals with significant disability will not be able to complete some or all the speech tasks.
Speech will be analyzed acoustically using Redenlab's® Analyze pipeline for measures of timing (e.g., pause length in reading and monologue tasks), vocal control (e.g., fundamental frequency and loudness variation from vowel and monologue), and vocal quality (e.g., dysphonia measured derived from sustained vowel) and composite measures of intelligibility and naturalness. Language analysis will involve natural language processing techniques for parts of speech and morphosyntactic markers as well as composite measures using Redenlab® Analyze.
The time commitment for the speech test is 10 min and contains 5 tasks:
Speech agility, syllable repetition– repetition of “pataka” (repeated once) Short vowel, voice quality – “ah” (repeated once) Reading paragraph Monologue (1–2 min) Picture description
Disability severity
The mRS will be assessed by a clinician or a member of the research team at baseline and 12 months. The scale is a validated measure of neurological impairment and was chosen to capture potential functional change in participants over 12 months.41,46 Participants are asked about their current independence in completing daily activities. This will be evaluated as change at follow up from baseline, with scores ranging from 0–6 and higher scores indicating greater disease progression.
Cognitive screen
MoCA telephone assessment is staff-administered at 12 months via telephone interview. Scores include an overall MoCA score (0–22) and Memory Index Score (MIS, 0–15) with greater scores indicating greater cognition. The MoCA telephone assessment has shown good sensitivity and specificity for identifying individuals with dementia in visually impaired people. 42
Mood screening
HADS is staff-administered at 12 months via telephone interview. This scale is a validated measure of anxiety disorders and depression. 43 Scores include a total depression score (0–21) and total anxiety score (0–21); grouped according to normal (0–7), borderline abnormal (8–10) and abnormal (11–21). Participants identified as having clinically significant levels of psychological distress, defined as falling in the moderate to severe range (scores > 11), will have their primary physician notified to mitigate the overall risk of harm.
Functional screen
WHO Disability Assessment 2.0 12-item telephone interview scale is staff-administered at 12 months via telephone interview. The WHO Disability Assessment 2.0 36-item self-report scale is self-administered by the participant. Both scales will be scored as an overall percentage disability, with higher scores indicating poorer function. The scale was chosen due to its validation as a functional scale irrespective of disease syndrome and has shown a high test-retest reliability. 44 It is accessible in 27 languages and an analysis of robust factors by Üstün, Chatterji 44 showed no change in varying cultural backgrounds, suiting the demographic of this study cohort.
Global rating of improvement/change
CGI-C score is staff-administered at 12 months via telephone interview. This will be scored on a 7-point scale, with scores closer to 0 indicative of greater improvement and scores close to 7 representing much worse since baseline. The scale has shown high interrater reliability and has been standardized for assessing change in illness over time. 47
Optional data sharing and DNA biobanking
All participants are offered participation in DNA and plasma banking as an optional part of the study. Consent will be provided by participants as a tick box on the main information consent form and participants consent to have their plasma samples and an additional whole blood sample, shared with approved studies and/or stored for contribution to international collaborations. Participants will have an additional 6 mL of blood from the same venepuncture used to estimate NfL. Whole blood samples are collected in a 6 mL K3 EDTA vacuette tube (Greiner Bio-One, Kremsmünster, Austria). After collection, samples are temporarily stored at −20°C before being transferred to −80°C. Biobanked aliquots of plasma and whole blood samples are stored at the School of Translational Medicine, Alfred Centre, Melbourne.
Optional genetic testing for people at high-risk of monogenic mutations (Study 3)
Participants with a suspected FTD syndrome or with a family history of genetic AD are offered monogenic sequencing of 14 genes, (selected as the most common monogenic mutations in dementia syndromes), by industry partner Invitae as an optional part of the study. Saliva samples are collected and tested using ‘Invitae Frontotemporal dementia with C9orf72 Panel’. 48
Participants can participate at any point during the study and after providing written informed consent on a separate consent form, saliva testing kits are sent to participants; or alternatively, buccal kits, if saliva samples are not feasible or well-tolerated. Participants provide 2 mL of saliva into an OrageneTM OG-500 DNA saliva tube and then send their samples to the Eastern Clinical Research Unit (Box Hill, VIC, Australia) after which the research team ship these samples, at ambient temperature, to Invitae (San Francisco, CA, USA) for processing and reporting. These procedures have been adapted to improve donor care and compliance with painless, non-invasive sample collection. Participants can choose whether, and to whom, their result is disclosed. If the participant agrees to results disclosure, results are released via a letter signed by the Principal Investigator with contact details, should they wish to discuss their result. If the participant does not consent to disclosure, but wishes to have their findings used for research, the Project Officer uploads the result to the REDCap database and their referring clinician is notified of the result with strict instructions not to disclose or upload the result to any medical records. Patients are told they should consider themselves as not having had genetic testing.
Data collection from participants’ medical records
The research team collates additional data from participants medical records. Cognitive screens are completed for most patients presenting to clinic with cognitive complaints. Scores for these cognitive screens are noted by research staff along with the date completed by their clinicians to assess functional progression. Participants’ most recent estimated glomerular filtration rate is noted.
Data collection retention
Several plans have been implemented to promote participant retention and completion at follow-up.
A data tracking log has been created in Microsoft Excel® for tracking participant enrolment and to easily identify those with missing data (e.g., in the instance of a failed venepuncture). If a blood sample was not collected at baseline, a member of the research team contacts a participant before their next review clinic appointment to schedule another on-site visit coinciding with attendance at clinic. This allows completion of a second attempt to collect the blood sample. To increase participant retention at follow-up, a member of the research team contacts participants one month before their follow-up. Contact includes an initial phone call and text message and a second phone call one week later. This timeframe is intended to allow ample time to accommodate for participant and rater availability, as well as shipment of the study pack to participants’ addresses and to organize interpreting services, if required.
For participants completing remote speech samples and the WHODAS 36-item self-administered questionnaire, a member of the research team tracks completion. For incomplete assessments, a text message is sent to participants as a reminder to complete the assessment, along with a phone call to address any difficulties. For non-English speaking participants, an English-speaking carer is contacted to facilitate the administration of instructions, or an interpreter is scheduled during this phone call.
The study allows for 50% attrition at follow-up. Where a follow-up is not completed, a trained study coordinator accesses medical records to estimate the mRS score using available clinical notes from the anticipated follow-up period. If no clinical notes are available, the score is left blank.
Data management
A REDCap database tracks participant consent, follow up and withdrawals and contains participant details, and all results and data collected. A PID is used to label all documents and blood and speech samples.
Saliva samples are required by Invitae to be labelled with at least two identifiers and a PID and date of birth is used. Precautions have been implemented to prevent the accidental disclosure of results to participants who consented to not receive results for a genetic test where they supplied their saliva. Only the Project Officer has access to the ordering and receiving of results, shared only with the clinician/s involved on a secure Invitae portal. Results are added to the REDCap database by the Project Officer, and they remain hidden until data extraction (refer to Supplemental Material 6).
Development of guidelines and policies (Study 4)
Clinical implementation of plasma NfL will require clear guidelines and cut-offs normed for local populations. NfL is influenced by factors such as age, renal impairment and BMI. A policy and guidelines working group will be created to provide recommendations for utilization of NfL as a diagnostic tool in both primary and secondary care settings. The group will include representation of individuals from diverse clinical, industry and consumer backgrounds, including people with living experience, carers, dementia clinicians and peak body representatives from Dementia Australia. This group will meet monthly after the final participant completes Study Visit 2. Policies will be developed in a series of stages as per prior implementation trials. 49
Clinical diagnostic consensus meetings (Study 5)
Clinical diagnostic consensus meetings are convened with clinicians; junior and experienced, to assess the impact of NfL levels on diagnostic outcomes. We have recently found a degree of uncertainty when diagnosing people with cognitive complaints in our specialist cognitive service. 8 The impact of blood biomarkers on clinician certainty has not been investigated. For this reason, clinicians complete a referral checklist at baseline to identify clinical impression before NfL and are asked the questions “does this participant have a degenerative condition?” and “what is your certainty of this?” assessed as ‘low’, ‘medium’, ‘high’ and ‘certain’ (‘certain’ applied if confirmed by imaging or genetic testing). A provisional diagnosis and duration of symptoms (years) is also requested. A case-crossover design, similar to that as previously described by Ha, Churilov 50 will be applied and information collected at baseline for each participant will form their own control.
CDCMs follow 4 stages (as outlined in Figure 3). Stage 1 involves clinicians identifying if there have been any changes to their baseline impressions as identified clinically (e.g., new imaging results confirming diagnosis, etc.). The NfL result (pg/mL) is presented at stage 2. At stage 3, clinicians are asked whether the NfL changes their certainty of the presence or absence of degeneration and qualitative comments are collected to ascertain if NfL was helpful to clinicians’ diagnostic confidence. A review of participants’ medical history, including eGFR levels (if available), is conducted to identify potential confounding factors influencing NfL levels, in accordance with established literature. Finally, stage 4 involves documenting any clinician action prompted by the NfL result, such as reviewing of imaging if the result lowered diagnostic certainty. If the NfL level is deemed unhelpful or as expected, no further actions are required by clinicians.

Flow and description of data collected during clinical diagnostic consensus meetings (CDCMs). Baseline data that are discussed during CDCMs are collected at Stage 0 via completion of a checklist upon referral to the study. CDCMs are split into 4 stages: Stage 1 Pre-NfL disclosure, Stage 2 NfL disclosure, Stage 3 Post-NfL disclosure and Stage 4 action required. eGFR = estimated Glomerular Filtration rate.
CDCMs are convened by a project officer when individual clinicians have NfL results for at least 10 of their referred patients (the frequency subject to change conditional to recruitment and NfL processing). Discussions are limited to 5 min per participant and meetings are scheduled in 30–60-min blocks. They are arranged per clinical service to ensure only participants relevant to the specific clinic service are discussed, addressing inter-service privacy concerns. A minimum of two clinicians are expected at the meetings and in the instance that a consensus meeting cannot be arranged due to clinicians’ unavailability, the Principal Investigator attends as a second member. A case ID is assigned to participants in the order they are discussed during CDCMs, per clinician. The purpose of this is to track changes to understanding of NfL as clinicians observe emerging trends over time.
Supplement to Figure 3 (displayed as a key points box in margins)

Health economic evaluation (Study 6)
An optional analysis on the cost-effectiveness of NfL is available to participants. Participants are required to sign a separate consent form; at the time of providing main consent, which will be forwarded to ‘Services Australia’ in batches for releasing their Medicare data during the study period. A health economic model will be developed to compare the short-term and long-term costs and the potential benefit of blood and digital biomarkers in diagnostic pathways. We will collect comprehensive clinical and cost data to inform our model. Data relevant to our study cohort will be compared and includes epidemiological data for patient management pathways, costing data such as primary care (GPs, specialist visits, examinations, pharmaceuticals), emergency department (ED) visits, hospitalizations, and allied healthcare, patient-reported outcomes (i.e., WHODAS 2.0) and anxiety/depression indices. We will use a range of sources to inform the health economics model, including primary care information from the data linkage of the Medicare Benefits Schedule and the Pharmaceutical Benefits Scheme, and hospitalization/ED data from hospital departments.
Quality control measures
Source data verification, twice yearly
Source data verification is completed by the Principal Investigator twice yearly. Verification includes random selection of participants’ documents by a member of the research team, and cross-examining with the respective data entered onto the REDCap database.
NfL assay quality assurance
NfL results are sampled twice and are reported as mean (pg/mL) and precision of measurements are measured with a coefficient of variation (CV). In accordance with guidelines produced by the International Council for Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH), NfL results with a CV > 20% are re-sampled using replicates to confirm the results. Inter-assay precision has been determined with the addition of a sample control in three assays.
Staff training and compliance with GCP
The research team are required to undergo training using the WebDCUTM to complete the mRS. Redenlab® have created training slides and a dedicated project manager to train all staff with use of speech recording equipment. Speech data pass through Redenlab's Automatic Audio Pre-processing Pipeline (RAAPP) to ensure quality. All staff are required to complete ongoing GCP training and protocol-specific training before beginning study activities. Once training is complete, a delegation log is signed by the Principal Investigator, permitting a staff member to conduct study activities.
Bias and blinding
Unblinded research staff organize the follow-up phone calls for participants at 12-months. During this time, participants are advised not to disclose their diagnosis or symptoms with staff during the phone call. If a participant reveals information pertaining to their diagnosis during the phone call, the assessor will cease the visit and inform the participant that their appointment will be rescheduled with an alternate assessor. To reduce the risk of mortality bias and missing data, participants with a prognosis less than 12-months are not included.
Sample size and power calculation
This study has been powered to achieve our primary aim which is to establish the utility of NfL as a test for the presence of dementia/neurodegeneration.
As this aim is of an estimation nature, the required sample size was derived using a precision-based (rather than power-based) approach. We aim to recruit sufficient participants to estimate both test sensitivity and specificity with adequate precision (defined as half-width of the 95% confidence interval around the estimated value). We expect it to have at least 0.7 sensitivity and at least 0.8 specificity for the test to have a sufficient clinical utility and to be useful for clinical practice. We have estimated our sample size as 820 participants and expect 15–20% attrition (i.e., not available for follow-up at the 12 month point due to death, illness, or relocation out of the study area). Therefore, we will aim to recruit 1000 participants to allow for unusable samples and for attrition.
Diagnostic utility estimation
We expect around 70% of the patients presenting to cognitive and dementia clinics to have a clinical diagnosis of dementia or other neurodegenerative disease at 12 months, with the remaining 30% not having a diagnosis of dementia. This is based on published studies and on audits of 10-year clinic data on diagnostic conversions. 1 Surprisingly, there are scant data on diagnostic conversions in clinical settings. We note this is a different question to many studies of “mild cognitive impairment” or MCI, a research term used for people with cognitive impairment who are believed to be at risk for AD. It is noted that the conversion of MCI to AD has been well-documented, but still varies enormously depending on whether people are tested in a clinic setting or as part of a community study.
To estimate test specificity of 0.8 or higher with the precision of 0.05, 246 patients without the outcome of neurodegeneration at 12 months would be required. Therefore, the total sample size of 246/3*10 = 820 (consisting of approximately 574 participants (70%) who are expected to exhibit the presence of neurodegeneration at 12 months and 246 participants (30%) who are expected not to exhibit this outcome) would provide sufficient precision (0.05 or higher) to estimate the assumed test specificity of 0.8 or higher. This sample size would also provide 0.038 or higher precision to estimate the assumed test sensitivity of 0.7 or higher based on the expected number of outcome positive subjects of 574.
Incidence estimation
The planned total sample size of 820 would provide the estimate of one year incidence of diagnostic conversion with precision (half width of 95% confidence interval) of 3.5% for the assumed population incidence of 70% and precision of 4% for the most conservative estimate of the incidence at 50%.
Statistical analyses
The primary aim of the Neurofilament And Voice Acoustics In Dementia Diagnosis (NAVAIDD) study is to investigate the utility of plasma NfL in detecting neurodegenerative disease. To achieve aim 1 and 2, we will estimate the sensitivity, specificity, area under the curve (AUC), values within the receiver operating curve (ROC) framework. We will identify the optimal threshold for the biomarker value to maximize AUC and generate diagnostic odds ratios for the chosen cut-off point. As a part of sensitivity analysis, we will generate positive and negative predictive values for the test by varying the value for potential prevalence in the population.
Analysis of aims 3–6 will be largely exploratory. Descriptive statistics will be largely used for aims 3 and 4. We will follow similar protocols used by Kwakkel, Lannin 49 to develop a consensus of recommendations on a core set of guidelines in relation to aim 4. Analysis of aim 5, will be undertaken within a random effect repeated measures regression framework with individual patient cases as random effects, whether the diagnosis was made with or without NfL information as independent variable, and diagnostic certainty as the dependent variable. An economic evaluation will be performed to achieve Aim 6 to compare both costs and health outcomes in the scenarios where the diagnosis is established with or without NfL information. Data from genetic testing will be incorporated into the health economic analysis to determine the impact of early genetic testing.
Model of inclusive design
Inclusion of non-English speaking participants
The limitations of the documents in obtaining informed consent from non-English speaking minorities are acknowledged and, therefore, video invitations in Eastern Health's top 5 common languages have been produced: English, Cantonese, Mandarin, Greek and Italian. The ‘Invitation to participate’ letter includes a quick response QR code link to these videos, which are available on the Eastern Health website. The industry partner Redenlab® has the technology to create a speech battery in 30 languages. Therefore, speech tasks are available for completion in the above-mentioned languages with the option to add extras as required. The interpreting service at Eastern Health will be utilized, if required, for consenting and all study procedures.
Inclusion of mobility restricted participants
While participants are only required on-site for a single visit at baseline, remote consenting procedures have been introduced to limit participant burden of attendance on-site and if preferred consent may be obtained via video call. These methods have been adapted from the PISCES-ZODIAC protocol, introduced during the COVID-19 pandemic, and implements the zoom (www.zoom.us) platform for video call. 51 Visit 1 will coincide with participants’ clinic appointment and follow-up at 12 months will be via telephone, meaning participants do not require any additional travel for the purpose of the study.
Recruitment strategies
Strategies have been implemented to ensure achievement of the target sample size. Firstly, study visits have been created for minimal participant burden. Where participants have limited time after their clinic appointments, a QR code to speech tasks can be provided which enables participants to complete this later on their own device.
All participants screened as appropriate, receive letters to participate with a link to a video invitation which they may view in advance to consider the study. Videos are translated in multiple languages and interpreters are available to allow the opportunity for non-English speaking individuals to consider participation. A phone dedicated specifically to the study is listed on invitation letters for participants to call to express interest and/or inquire about the study. In this way, participants may choose to provide written consent and complete their baseline visit either before or after their clinic appointment.
Finally, to facilitate referral of suitable participants across the healthcare network, the staff of the wider neurology department and in geriatric medicine have been provided with information of the study, along with inclusion and exclusion criteria to communicate the study with patients presenting on the wards. The research team consists of 7 research nurses, providing ample cover if staff are required to take leave.
Confidentiality
Participant details including name, UR number, date of birth and contact details, are stored on a secure password protected REDCap database and access to this is restricted to essential members of the research team with varying levels of access. This enables researchers to re-identify documents or blood samples in cases where participants wish to withdraw or have their data/samples destroyed. Speech samples are completed on Redenlab® servers and uploaded to a secure desktop, restricted to only those authorized. This software is password-protected, and passwords are required to be changed every 3-months in line with clinical trial guidelines. Only authorized users have access to Redenlab® speech software.
Results for saliva samples are obtained from an Invitae portal. Researchers and clinicians are required to have their own password protected accounts to limit the number of personnel with access to results. Storage of data on the Invitae database are de-identified according to Health Insurance Portability and Accountability Act (HIPPA) requirements. Results are stored securely on Invitae databases for 7 years in accordance with National Association of Testing Authorities’ (NATA) requirements.
Publications and/or presentations generated from this research project will provide information in a way such that participants cannot be identified.
Discussion
Blood and digital biomarkers are increasingly being studied as an objective method for detecting neurodegeneration. However, most studies exclude people from diverse cultural, educational, linguistic and geographic settings, limiting the real-world generalizability of any findings. This research is unique in its broad inclusion criteria and its limited burden on participants. The study design with only one in-person Visit coinciding with participant clinic appointments that occur as part of usual clinical care, and a follow up phone call after 12-months, is expected to be convenient for most study participants, improving the accessibility for patients within our healthcare network. The planned sharing of data with other research studies in Australia and internationally will ensure the results from this diverse study cohort will translate globally. Inclusion of a nested clinical decision-making paradigm will allow the utility of NfL for clinicians in real-world clinical settings to be established. Convening of a policy and guidelines working group will provide recommendations for the clinical implementation of plasma NfL. Finally, a health economic analysis will explore the cost-saving potential of biomarkers and early genetic testing.
Study status
Recruitment for the NAVAIDD study was initiated in August 2021 and currently 515 participants have been enrolled at time of submission. Ethics approval of the current protocol version was received on 27 March 2025: Protocol v8. Follow-up visits were delayed over the pandemic and commenced in January 2023. The current rate of completion/attrition is at 51%, as expected. CDCMs began in January 2023 and remain ongoing. Two-hundred and sixty-three participants have completed the speech task. Recruitment is expected to be completed in 2026.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-1-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-2-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-2-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-3-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-3-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-4-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-4-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-5-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-5-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-6-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-docx-6-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-doc-7-alr-10.1177_25424823251395325 - Supplemental material for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings
Supplemental material, sj-doc-7-alr-10.1177_25424823251395325 for Neurofilament light chain and voice acoustics in dementia diagnosis (NAVAIDD): Protocol for a cohort study assessing the real-world diagnostic utility of blood and digital biomarkers in clinical settings by Svetlana Ivanic, Adam P Vogel, Pratishtha Chatterjee, Julie Baird, David Darby, Emilio Werden, Lan Gao, Peteris Darzins, Sheila K Patel, Isabelle Burke, Tracy Morris, Leonid Churilov, James Bice, Michelle M Mielke and Amy Brodtmann in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors would like to acknowledge all clinician referrers supporting the study including Dr Chris Kyndt, Dr Maja Christensen, Dr En Ye Ong, Dr Susanna Hii, Dr Will Lee, Dr Lin Zhang, Dr Christine Ng, Dr Ryan Cheng, Dr Claire Taylor and Dr Nicola Hogan. We would like to thank the dementia trials team at the Eastern Clinical Research Unit for their assistance with recruitment activities including Sarah Shue, Shruthi Patlori, Maria Lacson and Claire McCarthy. Special thanks to Malcohm Chung, Cynthia Zupan and Georgia Papagiannopoulos for creating translation videos and to all the administration staff at Box Hill Hospital and Wantirna Health hospital for their guidance with clinic lists and overall support. We thank the team at the Florey Institute, Adam Southon and Sheila Patel, for their efforts in processing the samples for measurement of NfL. Lastly, the authors would like to acknowledge Dementia Australia representatives, Leanne Emerson and Kylie Miskovski.
Ethical considerations
The study has received ethics approval by Eastern Health lead Human Research Ethics Committee and Research Governance (Local reference E21–006-72840).
Consent to participate
All participants provided written informed consent prior to enrolment in the study.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the National Health and Medical Research Council Medical Research Future Fund [MRFF2022896], Victorian Medical Research Acceleration Fund (VMRAF), Eastern Health Foundation Research and Innovation, Monash University (sponsoring academic organisation and academic partner) and industry partners Redenlab® Pty Ltd, Dementia Australia and Invitae. Professor Vogel received funding from the Australian Research Council Future Fellowship (#220100253).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof Brodtmann reported receiving grants from the National Heart Foundation, NHMRC and MRFF (that supported the submitted work), paid to her via her institution; serving on scientific advisory boards for Eli Lilly, Roche, Novo Nordisk, and Eisai; and acting as an honorary medical adviser for DARF, all outside the submitted work. Professor Vogel is Chief Science Officer of Redenlab® Inc. a pharma services company. Professor Mielke has served on scientific advisory boards and/or has consulted for Acadia, Beckman Coulter, Biogen, Cognito Therapeutics, Eisai, LabCorp, Lilly, Merck, Novo Nordisk, Roche, and Siemens Healthineers, all outside the submitted work. All other authors report no conflicts of interest.
Data availability statement
The datasets and research material generated during and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author on reasonable request.
Auditing procedures
The Eastern Health Research Auditing Program is conducted by the Office of Research and Ethics and aims to audit multiple randomly selected projects running throughout EH. The NAVAIDD study was successfully audited by the Office of Research and Ethics at Eastern Health in September 2023 and received feedback of study conduct and documentation being of a “high quality.” The Office of Research and Ethics implemented a National Clinical Trial Governance Framework in February 2024 involving Short Notice Accreditation Assessments (SNAP). SNAP is constructed on National Safety and Quality Health Service Standards and aims to ensure clinical trials are conducted in a safe environment and in a high-quality manner. The study has not been selected for a SNAP.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.