
Abstract
Background
Dementia is one of the main public health challenges worldwide. To evaluate awareness programs, it is necessary to use validated scales, such as the Dementia Knowledge Assessment Scale (DKAS), the Dementia Attitude Scale (DAS), and the Confidence in Dementia Care Scale (CODE), none of which exist in Russian.
Objective
The present study aims to translate and evaluate the psychometric properties of the DKAS-R, DAS-R, and CODE-R within the Russian-speaking population.
Methods
A cross-sectional online study was conducted using convenience sampling (N = 533). Validation included assessing reliability (internal consistency and four-week test-retest reliability of a subgroup of 130 participants), analyzing structural validity through confirmatory factor analysis, and assessing construct validity through the known-groups method. Additionally, an item analysis was conducted. The STROBE checklist was used to report this study.
Results
Acceptable to excellent internal reliability was found for DKAS-R (α/ω = 0.81), DKAS-R20 (α/ω = 0.81), DAS-R (α = 0.81, ω = 0.84), DAS-R14 (α/ω = 0.84), and CODE-R (α = 0.89, ω = 0.88). The proposed factor structures were confirmed after minor modifications (item reductions and correlated residuals). The known-groups analysis revealed that all scales could distinguish between individuals with or without experience with people with dementia and with or without participation in a dementia course. Retest-reliability was moderate for DAS-R/DAS-R14, good for the DKAS-R/DKAS-R20 and CODE-R.
Conclusions
This study provides the first psychometric validation of the DKAS-R, DAS-R, and CODE-R for the Russian-speaking populations. After minor adaptations, all three scales demonstrated robust structure and reliability, supporting their use in research.
Introduction
Dementia represents one of the most urgent public health challenges worldwide, driven by increased life expectancy and the lack of effective treatments. Projections indicate that by 2050, the number of people living with dementia could reach between 139 and 152 million, placing substantial pressure on healthcare systems globally. 1 Trends in dementia prevalence are also notable in countries where Russian is either an official language or a widely spoken language.2,3 In Russia, an estimated 1.95 million individuals were living with dementia in 2019. Projections indicate that this figure will rise to 4 million by 2050. Dementia assessment in Russia is hindered by limited diagnostic accuracy and availability, particularly during the early stages. 4 Meanwhile, studies underline the critical importance of improving early diagnosis, showing that delaying the onset of Alzheimer's disease by five years could halve its prevalence by mid-century, while a one-year delay could reduce cases by 9.2 million. Such improvements would also significantly lower the number of severe cases and associated caregiving costs. 5 Official reporting diverges sharply from epidemiological projections: federal statistics for 2014 record only 8831 patients coded with Alzheimer's disease, whereas population models estimate well over one million cases. 6 This gulf reflects systemic barriers—late referrals, limited dementia awareness among primary-care physicians, widespread “Dementophobia” in the public, the low sensitivity of routine screening tests, infrequent prescribing of acetylcholinesterase inhibitors, and inadequate specialist training.7,8 Under-reporting is further compounded by ICD-10 practice: Alzheimer's disease is entered under G30 (“Diseases of the nervous system”), while the associated dementia syndrome should be double-coded as F00, a step often omitted in routine workflows. 7 Collectively, these factors seriously impede reliable estimation of the dementia burden and hinder rational healthcare planning in Russia.6–8 Although official documents, such as the “Strategy for the Interests of Older Citizens”, emphasize the significance of dementia as a public health issue and present prevalence data consistent with global trends, there are still no concrete national programs for the prevention and management of dementia.9,10
Issues related to the low level of dementia awareness, both among professionals and the general public, are a significant concern within Russia's professional community. 11 In Russia, the stigma surrounding dementia remains a significant barrier to early diagnosis and support, with many individuals reluctant to disclose a diagnosis, whether their own or that of a relative. This pervasive stigma highlights the need for targeted initiatives to raise awareness and reduce prejudice. However, efforts to implement such projects remain fragmented, limiting their potential to drive systemic change.9,12–15 Similar challenges in dementia prevention, diagnosis, and public awareness are observed in other countries with a high proportion of Russian-speaking populations, such as Belarus, Kazakhstan, and Moldova.16–19
The growing prevalence of dementia is increasingly drawing attention to the issue of awareness among both specialists and the general public. Recent surveys indicate that 34% of respondents in Russia are familiar with dementia, while 24% have never heard of it. 20 Additionally, 48% mistakenly believed dementia to be a natural part of aging rather than a medical condition. 21 This lack of understanding underscores the broader need for education and awareness. The World Health Organization (WHO) first highlighted this priority in its 2006 report on neurological disorders. 22 More recently, the WHO Global Action Plan on the Public-Health Response to Dementia 2017–2025 calls for targeted measures to strengthen knowledge among caregivers and healthcare providers in the face of the worldwide rise in dementia prevalence. 23
In Russia, caregiving for individuals with dementia predominantly falls on family members, reflecting a “familist regime” of care. This dynamic places significant emotional, physical, and financial burdens on caregivers, who often lack formal training and adequate resources. 24
Non-governmental organizations (NGOs) have emerged as key players in addressing these challenges, often surpassing state services in providing community-based care and support. 25 However, despite these efforts, comprehensive official statistics on caregiving are scant, and existing programs frequently operate without systematic evaluation of their effectiveness.
To the best of our knowledge, no validated instruments currently exist in Russian to assess knowledge, attitudes, and caregiving confidence regarding dementia, either within professional communities or for evaluating public awareness. While several questionnaires have been developed internationally, only a few demonstrate adequate reliability and validity, and many remain outdated or limited in scope.26–30 In recent years, the Dementia Knowledge Assessment Scale (DKAS), the Dementia Attitude Scale (DAS), and the Confidence in Dementia Care Scale (CODE) have been increasingly used across countries to evaluate dementia-related knowledge, attitudes, and caregiving confidence among health professionals, caregivers, and the general population.31–36 Building on this evidence, the present study aims to validate these three instruments in Russian, thereby enabling their broader application in research and in the evaluation of psycho-educational initiatives for informal caregivers and public awareness programs.
Methods
Design
A cross-sectional survey was conducted to evaluate the psychometric properties of the three translated instruments: the DKAS-R, DAS-R, and CODE-R. The present study adheres to the EQUATOR guidelines for reporting research, following the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) checklist (https://osf.io/vt6hn/overview).
Participants
A convenience sample of the general population was recruited through newsletters, posters, and flyers, as well as by sharing invitations to participate via social media platforms such as Facebook, WhatsApp, Instagram, and VKontakte. Recruitment took place between June and October 2024. The inclusion criteria were limited to individuals aged 18 years or older whose native language was Russian.
For questionnaire-based studies, a sample size of 150–300 participants is recommended, which suggests 5–20 participants per item.37,38 Given that the DKAS-R was the most extended questionnaire, with 25 items, the resulting sample size was expected to fall within the range of 125 to 500 participants. The final sample size exceeded this target, with N = 533 participants completing the survey. A smaller subsample (n = 131) completed the instruments again after a four-week interval to assess test-retest reliability, which is considered sufficient for a retest analysis to produce stable and generalizable estimates. 39
Data collection and procedure
The research team collected data using Google Forms, where a structured questionnaire was prepared. At the beginning of the survey, participants were informed about the study's objectives, the data collection procedure, and the measures implemented to ensure the protection of personal data. Participants were then asked to provide their informed consent before proceeding.
The questionnaire included sociodemographic data (age, gender, marital status, education level, type of employment, and country of residence), as well as questions about prior experience with people with dementia (PwD), including knowing someone with dementia, providing care for PwD, professional experience working with PwD, and participation in educational programs about dementia. In addition, the questionnaire included the three scales to be validated: the DKAS-R, DAS-R, and CODE-R. Participants who consented to take the test a second time four weeks later to assess test-retest reliability were requested to provide their email addresses and create a code to facilitate the matching of data from both surveys. These addresses were utilized to send invitations and reminders for follow-up participation. Completing the questionnaire required approximately 10–20 min. Google Forms ensured that only fully completed questionnaires were accepted, eliminating any missing data.
Instruments
Dementia Knowledge Assessment Scale (DKAS)
The DKAS is a 25-item tool designed to evaluate general knowledge about dementia, which was introduced by Annear et al. (2015) as a more comprehensive and reliable instrument than previous tools. 40 It includes statements addressing various aspects of dementia, grouped into four subscales: “Causes and Characteristics”, “Communication and Behaviors”, “Care Considerations”, and “Risks and Health Promotions”.40–42 Respondents rate each statement either as “false”, “probably false”, “probably true”, “true”, or could state “I don’t know” in cases of uncertainty. Correct answers receive two points, probably correct answers receive one point, and both completely and partially incorrect answers or “I don’t know” responses are scored as 0. Several items (e.g., 1–6, 8–10, 13, 14, 21, 23, and 25) are reverse-scored as they represent false statements. The DKAS provides an overall score reflecting the respondent's level of dementia-related knowledge, with higher scores indicating greater knowledge. The scale has demonstrated strong psychometric properties, including high test-retest reliability, robust internal consistency (Cronbach's α = 0.85; McDonald's ω = 0.87 in Annear et al. (2017)), and solid construct, concurrent, and factor validity.40,41 Its multidimensional structure makes the DKAS a valuable instrument for the comprehensive assessment of dementia knowledge. To date, the scale has been validated in German, 43 Greek, 44 Spanish, 45 Chinese, 46 and Indonesian. 47
Dementia Attitude Scale (DAS)
The DAS is a 20-item instrument aimed at measuring attitudes toward dementia, 48 which was developed on the basis of the tripartite model of attitudes (cognitive, behavioral, and affective components) and constructed through a combination of qualitative and quantitative methods, including structured interviews. 49 The study was originally validated among college students and direct care workers and had a high internal consistency with Cronbach's α ranging from 0.83 to 0.85. The scale assesses the affective, behavioral, and cognitive components of dementia attitudes. Each item is rated on a seven-point Likert scale, where responses range from 1 (“Strongly disagree”) to 7 (“Strongly agree”). The total score ranges from 20 to 140, with higher scores indicating more positive attitudes toward dementia. Six items (2, 6, 8, 9, 16, and 17) are reverse-scored. The DAS has a two-factor structure reflecting “Social Comfort” (items 1, 2, 4, 5, 6, 8, 9, 13, 16, and 17) and “Dementia Knowledge” (items 3, 7, 10, 11, 12, 14, 15, 18, 19, and 20). The scale provides a nuanced understanding of both the cognitive and affective dimensions of dementia-related attitudes and has been shown to be a valuable tool for evaluating interventions aimed at improving them. The DAS has been validated in several languages, including German, 50 Greek, 51 Croatian, 52 Turkish, 53 and Chinese. 54
Confidence in Dementia Care Scale (CODE)
The CODE scale is a nine-item self-report instrument designed to measure confidence in caring for people with dementia, developed by Elvish et al. (2014).55,56 CODE operates as a unidimensional scale and has demonstrated excellent internal consistency reliability, with a Cronbach's alpha coefficient of 0.91 in the original study. Items are scored on a five-point Likert scale, where responses range from “not confident” to “very confident”. The total achievable score is between 9 and 45, with higher scores reflecting greater confidence. Based on the scoring, three levels of confidence can be identified: 0–18 not confident, 19–35 somewhat confident, and 36–45 very confident. The CODE scale provides a practical and reliable measure of confidence, making it a useful tool in both research and professional training contexts. It has been validated in several countries and languages, including German, 50 Greek, 51 and Chinese, 57 consistently demonstrating robust psychometric properties across settings.55–58
Development of the Russian version
The Russian versions of the scales were developed using the translation-back translation method. 59 Two independent experts with native proficiency in Russian and professional translation qualifications in English, as well as specialized expertise in geriatrics, dementia, and caregiving, translated the original English versions into Russian. The research team reviewed the translations, resolved discrepancies, and ensured cultural relevance to create a synthesized version.
This preliminary Russian version was then back-translated into English by a bilingual expert in public health. The original English and the back-translated versions were reviewed and compared by the research team to ensure semantic equivalence, clarity, and cultural appropriateness. To resolve any translation discrepancies, the translations were verified with the author of the original DKAS scale. Also, certain items, initially tailored for professional caregivers (e.g., “Rewarding to work with people with dementia”), were adjusted for general audiences by replacing “work” with “interact.” Additionally, the term “ADRD” (Alzheimer's Disease and Related Dementias) in the DAS-R was substituted with the simpler term “Dementia” to enhance understanding among participants.
To finalize the Russian adaptation, the questionnaires were pilot-tested with a group of 12 individuals to evaluate the clarity and cultural relevance of the adapted items. Feedback from this process was incorporated to ensure the final version accurately reflected the intended meaning and was suitable for the target audience (Supplemental Material).
Statistical analysis
All statistical analyses have been carried out with IBM SPSS V29.0 60 and the program package IBM AMOS 29.0.61–63 For all three scales, we evaluated the following psychometric properties: structural validity with confirmatory factor analysis (CFA), internal consistency with Cronbach's alpha and McDonald's omega, construct validity through the known-groups method and an item analysis.
Structural validity
All three questionnaires were examined for structural validity. In order to perform the analysis on a consistent factor structure using confirmatory factor analysis (CFA), the IBM AMOS 29.0 software package was utilized to model the CFAs.61–63 Although CODE has a monodimensional factor structure according to the authors, a CFA with maximum likelihood estimation was also performed for this scale. 55 The model was evaluated using the corresponding fit indices based on the evaluation criteria postulated by Hu and Bentler (1999). 64 According to these criteria, a model is deemed acceptable if the comparative fit index (CFI) and the Tucker-Lewis index (TLI) are ≥ 0.90. Furthermore, the root mean square error of approximation (RMSEA) is required to be < 0.08, and the standardized residual mean square (SRMR) is to be < 0.11. A good model evaluation is guaranteed if TLI and CFI are ≥ 0.95, SRMR is < 0.08, and RMSEA is < 0.05.64–67 For the presentation of the CFA results, the authors of this research paper followed the recommendations postulated by Schreiber et al. (2006) and Jackson et al. (2009).68,69
Reliability
To check internal consistency, we used Cronbach's alpha for the entire sample and separately for the groups of study participants who had already completed dementia training and those who had not yet completed it. Cronbach's alpha indicates the degree of common variance of the items on a scale, with 0.70–0.90 being the recommended range of values, whereby alpha values above 0.95 indicate redundant items within the scale.70–72 In addition, McDonald's omega was calculated as a second measure to verify reliability. One advantage of McDonald's omega is that it takes into account the different item loadings on the underlying factor; items related to the construct under investigation are weighted more heavily, leading to more precise reliability. Furthermore, McDonald's omega is more robust against assumption violations such as the assumption of tau equivalence.73–75
To assess test-retest reliability, the total sample (N = 533) was compared with the subgroup that participated again after a four-week interval (n = 131) using the intraclass correlation coefficient (ICC). An ICC above 0.7 was considered an indicator of good correlation, and an ICC above 0.9 was considered excellent correlation.76,77
Construct validity
The construct validity of the questionnaires was evaluated and analyzed using the known-groups method on study participants with and without experience in dealing with PwD, as well as on participants who had or had not yet taken part in a course on dementia. Individuals were considered experienced with dementia if they met at least one of the specific criteria related to experience with dementia in the questionnaire. These criteria included caring for a person with dementia, knowing a person with dementia, or working with a person with dementia.43,50,78 Based on previous research, the hypotheses were as follows: H1: Study participants with experience with PwD achieve higher total scores on all three scales than study participants without experience with dementia; H2: Study participants who have completed a course, training, or seminar on the subject of dementia achieve higher total scores on all three scales than study participants who have not yet completed a course, training, or seminar on the subject of dementia. The corresponding null hypotheses were as follows: H01: There is no significant difference in the total scores achieved on the three scales between study participants with and without dementia experience; H02: There is no significant difference in the total scores achieved on the three scales between study participants who have completed one or no courses, training programs, or seminars on dementia. To statistically test the corresponding hypotheses, we utilized the Mann–Whitney U test. 79 To evaluate the distribution of the tested groups with regard to the interpretation of the test, a two-sample Kolmogorov–Smirnov test was used to check the homogeneity of variance. If the groups show an equal distribution, the Wilcoxon–Mann–Whitney (WMW) test provides information about the medians of the respective groups. If the groups are unevenly distributed, the WMW test makes statements about the mean values of the ranks while simultaneously considering the overall distribution form. The effect size calculation of the WMW test was performed using the Pearson correlation coefficient.80–82
Item analysis for the DKAS-R, including difficulty and ignorance indices
An item analysis was performed for the DKAS-R based on the total sample as well as for the group of participants and non-participants in dementia courses. In the analysis, we estimated ignorance and difficulty indices for each item. We conducted this analysis both for the total sample and separately for the groups of participants and non-participants in dementia courses. The difficulty index was calculated by adding the percentage of correct answers (“probably true” and “true” in the case of correct statements and “false” and “probably false” in the case of false statements). The percentage of the ignorance index was assessed based on the answer “I don’t know”. The difficulty index was divided into six categories to evaluate the items on the scale, with the items classified according to their percentage. The categories were as follows: very easy < 90%, easy 75.1%–90%, somewhat easy 50.1%–75%, somewhat difficult 25.1%–50%, difficult 10.1%–25%, and very difficult < 10%.50,83
In addition, we analyzed the total item correlation of all items on the three scales in order to identify items with low explanatory power for the scale. The inter-item correlation represents the strength of correlation between the items on the scale. A correlation between 0.2 and 0.4 can be used as a benchmark for the mean inter-item and the item-total correlation. Within this range, items should contribute significant information to the scale without redundancy and artificial increases in reliability.84–86
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of the Faculty of Behavioral and Cultural Studies at Heidelberg University, Germany (AZ Teich 2021 1/1 and AZ Teich 2022 2/1). All procedures followed the ethical standards established in the Declaration of Helsinki, as well as the relevant national and institutional guidelines for research involving human participants.
Participation in the study was entirely voluntary. Participants were fully informed about the study's objectives, procedures, and data protection measures. Before proceeding with the survey, the research team obtained informed consent electronically via the online questionnaire.
Results
Participants’ characteristics
The analysis of psychometric properties was based on data collected from 533 individuals. Additionally, a subgroup of 131 participants completed the questionnaire a second time after a four-week interval to assess retest reliability. The key demographic and experiential characteristics of the full sample included individuals ranging in age from 19 to 93 years, with an average age of 48.6 years (SD = 10.03). The majority of the sample were female (89.9%). Educational attainment was high, with 87.3% holding a higher education degree. Most participants (64.7%) reported knowing at least one person with dementia, though relatively few had professional experience in dementia care (5.6%), and only 6.9% had ever participated in formal dementia-related training (Table 1).
Participants’ characteristics of the total sample and the subgroup.

Subgroup after four weeks for the retest
DKAS-R
Internal consistency
The DKAS-R demonstrated robust internal consistency, with a Cronbach's alpha and McDonald's omega of 0.81 for the total sample (Table 2). Reliability increased slightly for participants with dementia training (α = 0.85) compared to those without training (α = 0.79), indicating good consistency.
Psychometric properties of the DKAS-R, DAS-R, and CODE-R.

NoDT = Has not participated in dementia training. bDT = Has participated in dementia training.
Structural validity
The CFA was conducted to confirm the four-factor structure proposed by Annear et al. (2017), using maximum likelihood estimation. 41 The initial model did not fit well, indicating χ2(269) = 746.088, p < 0.001, CFI = 0.771, TLI = 0.745, RMSEA = 0.058 (90% CI [0.053, 0.063]), and SRMR = 0.0598. To improve the model fit, correlated error terms were gradually added based on high modification indices found between items 15 and 16 (MI = 86.878), items 8 and 9 (MI = 42.3002), and items 2 and 7 (MI = 21.477), as well as due to overlapping item content. Based on a detailed examination of the squared multiple correlations, standardized factor loadings, and standardized residual covariances, items 4, 10, 13, 21, and 23 were excluded from our model. The regression weights of the excluded items were all very low (< 0.4). This also applied to the items with very low squared multiple correlation (<0.2). Furthermore, items 4, 13, and 23 had the lowest mean inter-item correlations on the scale, all of which were below 0.2, which supported their removal. 87 The revised CFA showed a good model fit, with χ2(161) = 335.214, p < 0.001, CFI = 0.906, TLI = 0.889, RMSEA = 0.045 (90% CI [0.038, 0.052]), and SRMR = 0.0469 (Figure 1).
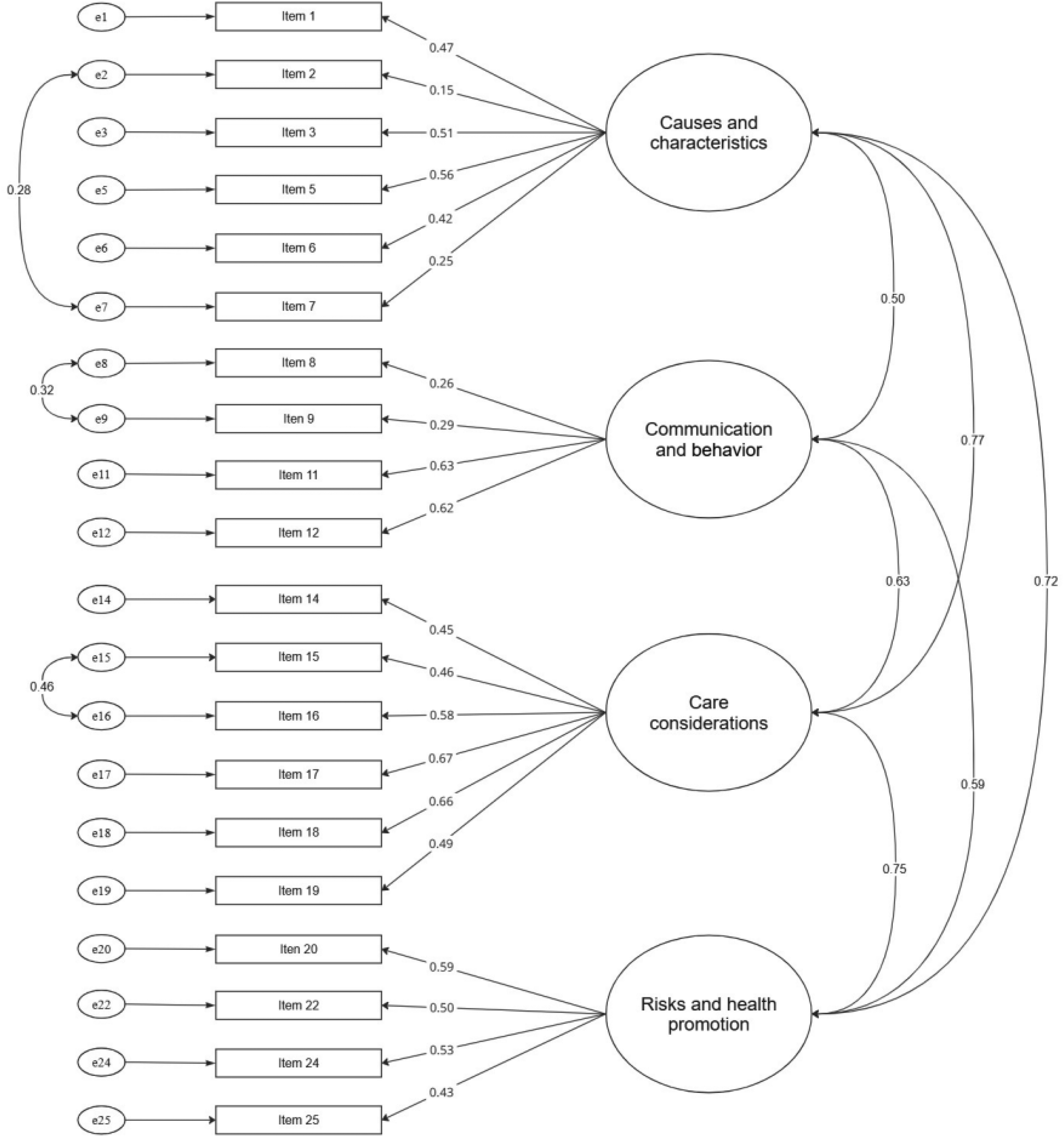
Confirmatory factor analysis of the DKAS-R20. Standardized factor loadings are presented for each item. All path coefficients are statistically significant (p < 0.05).
Construct validity
The results for the known-groups method are shown in Table 3. The Wilcoxon–Mann–Whitney tests demonstrated that the DKAS-R as well as the DKAS-R20 are capable of differentiating between (1) groups with or without previous experience with PwD, with participants having previous dementia experience scoring higher than those without experience, and (2) groups that had participated or not in a dementia training with participants having participated in a training scoring higher compared to those without training.
Results of the Wilcoxon–Mann–Whitney tests for all questionnaires.

U: U-test statistic; bz: z-statistic; cp: significance; dr: effect size; eK–S test: two-sample Kolmogorov–Smirnov test for variance homogeneity. Significant K–S tests are bold-highlighted, numbers highlighted in bold are the descriptive statistics to be interpreted according to the K–S test.
Item analysis
Item-total correlations were somewhat low, with a mean of 0.34 and a range of 0.085 to 0.488. This indicates no redundancy of items, as there was no correlation above 0.8. Items 4, 13, and 23 were problematic and had already been excluded from the CFA due to mean inter-item correlations of less than 0.2. After excluding the items, the item-total correlations were slightly better, ranging from 0.137 to 0.517, and with a mean total item value of 0.38, which ultimately showed better item-total correlations without redundancy of items within the DKAS-R20 scale.88,89
The correlations between the items of the DKAS-R showed a mean inter-item correlation of 0.14, ranging from −0.055 to 0.601. The mean inter-item correlation for the DKAS-R20 was 0.18, ranging from −0.046 to 0.601. Difficulty and ignorance indices were estimated for each item (Table 4), both for the total sample and according to the participation in a dementia program. For the total sample, two items were very easy, five items easy, six items somewhat easy, ten items somewhat difficult, two items very difficult, and ten items received a correct response from at least 65% of participants. Item 23, which was removed in the CFA, is among the two most difficult items. Overall, the subpopulation of participants who participated in a program about dementia showed more correct answers with great differences in items 2, 8, 12, and 20. The percentage of “I don’t know” answers was, in general, lower than for those who never participated in a course about dementia, except for item 6.
Item analysis of the DKAS-R.

*Reverse-coded items; aNoDT: Has not participated in dementia training; bDT: Has participated in dementia training.
DAS-R
Internal consistency
The DAS-R demonstrated robust internal consistency, with a Cronbach's alpha of 0.81 and McDonald's omega of 0.84 for the total sample (Table 2). Reliability increased slightly for participants with dementia training (α = 0.83) compared to those without training (α = 0.80), indicating good consistency. The shorter version (DAS-R14) demonstrated marginally elevated values in all categories.
Construct validity
Participants with prior experience with dementia scored significantly higher on the DAS-R than those without experience. However, the difference to the short version, the DAS-R14, was not significant, presumably due to the uneven distribution of group sizes. Participants with dementia training scored higher than those without training on the 20-item scales as well as on the short version (Table 3). These results validate the DAS-R's ability to measure differences in attitudes related to both dementia experience and training.
Structural validity
The CFA was conducted to confirm the two-factor structure proposed by O’Connor and McFadden (2010) using maximum likelihood estimation. 48 The initial model did not fit well, with χ2(169) = 728.830, p < 0.001, CFI = 0.798, TLI = 0.773, RMSEA = 0.079 (90% CI [0.073, 0.085]), and SRMR = 0.0797. To improve the model fit, correlated error terms were added step by step due to high modification indices observed between the following items: items 18 and 19 (MI = 29.874), items 14 and 15 (MI = 26.925), items 3 and 14 (MI = 16.112), and, lastly, items 2 and 6 (MI = 21.016). This approach was also motivated by overlapping content among the items. Based on a detailed examination of the squared multiple correlations, standardized factor loadings, and residual covariances, items 7, 8, 10, 16, 17, and 20 were excluded from our model. The regression weights of the excluded items were all very low (< 0.4). The same applied to the very low squared multiple correlation of < 0.2. Furthermore, items 8, 10, 16, and 20 demonstrated the lowest mean inter-item correlations on the scale, all of which were < 0.2, which supported their removal. 87 The revised CFA showed a good model fit, with χ2(72) = 240.462, p < 0.001, CFI = 0.926, TLI = 0.907, RMSEA = 0.066 (90% CI [0.057, 0.76]), and SRMR = 0.0550 (Figure 2).
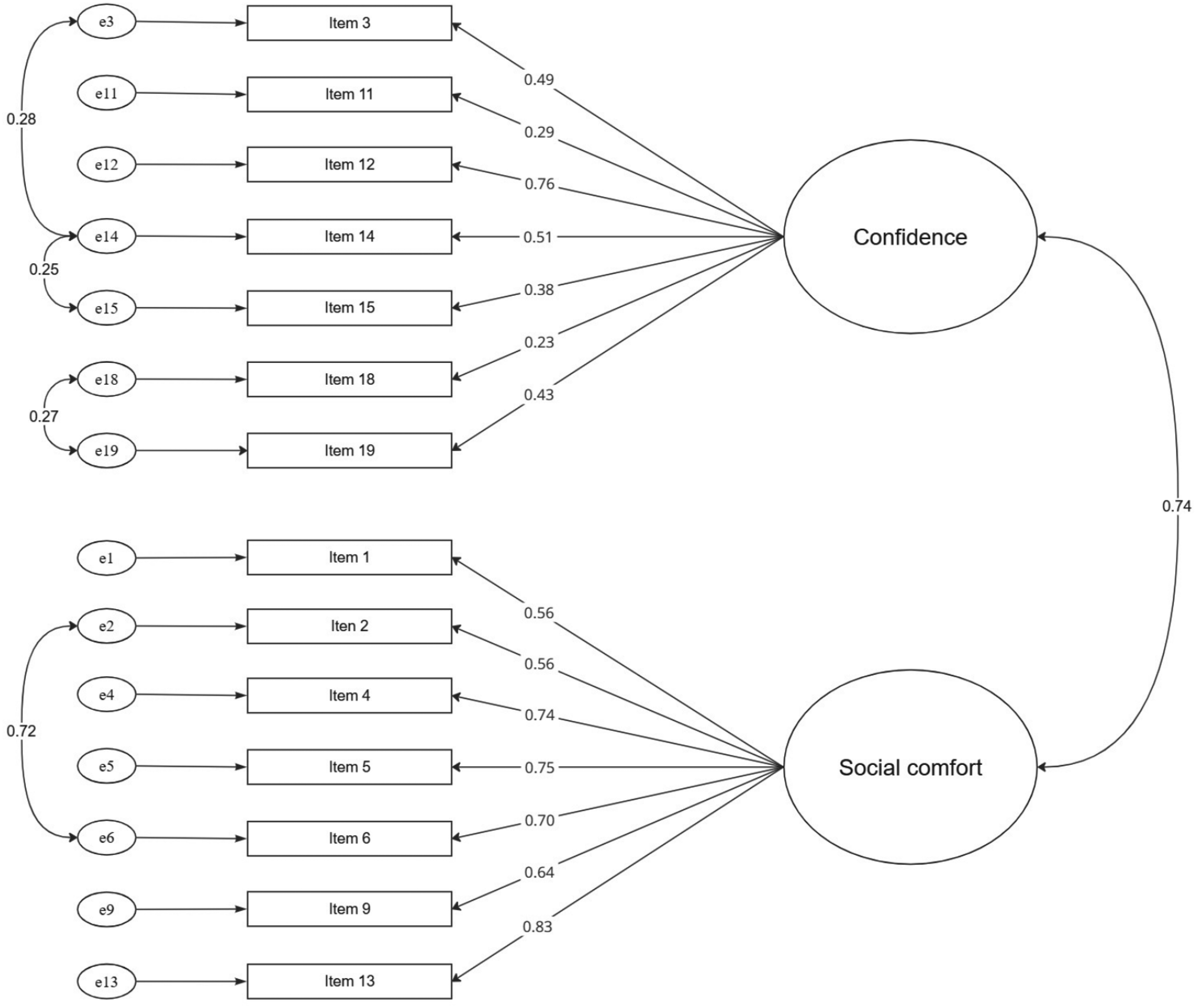
Confirmatory factor analysis of the DAS-R14. Standardized factor loadings are presented for each item. All path coefficients are statistically significant (p < 0.05).
Item analysis
The overall item-total correlations were good, ranging from −0.066 to 0.687, with a mean overall item value of 0.38, indicating a strong correlation without redundancy of items, as there was no correlation above 0.8. The problematic items on the scale were items 8, 10, 16, and 20, which had already been excluded in the CFA due to mean inter-item correlations of <0.2. After excluding the items, the item-total correlations were good, ranging from 0.206 to 0.706, and with a mean total item value of 0.48, which showed better item-total correlations without redundancy of items within the DAS-R 14 scale.88,89
The correlations between the items showed a mean inter-item correlation of 0.173, ranging from −0.210 to 0.609. DAS-R 14 had a mean inter-item correlation of 0.275, ranging from 0.026 to 0.609.
CODE-R
Internal consistency
The CODE-R achieved the highest reliability among the three scales, with a Cronbach's alpha of 0.89 and McDonald's omega of 0.88 for the total sample (Table 2). Subgroup analysis showed similarly high reliability across groups, with α = 0.88 for participants without training and α = 0.86 for those with training, suggesting excellent internal consistency.
Structural validity
The CFA was conducted to confirm the one-factor structure proposed by Elvish et al. (2014) utilizing maximum likelihood estimation. 55 The initial model did not fit well, with χ2(27) = 654.042, p < 0.001, CFI = 0.760, TLI = 0.680, RMSEA = 0.209 (90% CI [0.195, 0.223]), and SRMR = 0.0884. We added correlated error terms one by one due to high modification indices between items 8 and 9 (MI = 277.398), items 5 and 6 (MI = 76.934), items 1 and 7 (MI = 34.043), and items 5 and 6 (MI = 28.954). The addition was necessary due to the overlapping item content. The revised CFA showed a good model fit, with χ2(23) = 137.320, p < 0.001, CFI = 0.956, TLI = 0.932, RMSEA = 0.097 (90% CI [0.081, 0.113]), and SRMR = 0.0541 (Figure 3).

Confirmatory factor analysis of the CODE-R. Standardized factor loadings are presented for each item. All path coefficients are statistically significant (p < 0.05).
Construct validity
The results for the known-groups method are shown in Table 3. The Wilcoxon–Mann–Whitney tests demonstrated that CODE-R is capable of differentiating between (1) groups with or without previous experience with PwD, with participants with dementia experience scoring higher than those without experience, and (2) groups that had participated or not in a dementia training, with participants who participated in a training scoring higher compared to those without training.
Item analysis
The item-total correlations were good, with a range of 0.429 to 0.713 and a mean total-item value of 0.638, indicating a strong correlation without redundancy of the items, as there was no correlation above 0.8.88,89 Correlations between items showed a mean inter-item correlation of 0.466, ranging from 0.281 to 0.807. A strong correlation was only observed between items 8 and 9 (r = 0.807), which was reflected in the CFA, adding correlated error terms between these items.
Test-retest reliability of all scales
The four-week test-retest reliability was evaluated in a subsample of n = 131 using an ICC. As indicated in Table 5, all values ranged from 0.575 to 0.921, indicating the stability of the measure. Values between 0.75 and 0.9 indicate good reliability of the ICC estimate, while values above 0.9 indicate excellent reliability. The ICC estimate was based on a 95% confidence interval. 76
Test-retest reliability with subgroups (n = 131).

Discussion
Validated scales regarding knowledge about dementia, attitude toward dementia, and confidence in dementia care are necessary tools to evaluate educational programs. As there is a lack of validated scales in Russian, this cross-sectional study aimed to analyze the psychometric properties of the Russian versions of the DKAS, DAS, and CODE in the general population.
All three scales demonstrated robust psychometric properties, characterized by high internal consistency, supported factor structures following minor modifications (item reductions and correlated residuals), and sensitivity to group differences, making them reliable tools for Russian-speaking populations. These validations address critical gaps in Russia, where low dementia awareness (34%) and high stigma (51%) still persist.15,20
DKAS-R
The Russian version of the DKAS demonstrated robust psychometric performance with good internal consistency (α = 0.81), aligning with validations in Australia, Spain, Japan, Greece, and Germany (0.80 −0.87).40,43–45,90 Subgroup analysis showed reliable performance for participants with dementia training (α = 0.85) and those without (α = 0.79), supporting its use for healthcare professionals, nursing students, and the general public.31,35,43,46,91 A refined 20-item version (DKAS-R20) was created by excluding items 4, 10, 13, 21, and 23 due to low factor loadings. This version maintained equivalent reliability and achieved good model fit. This refinement process, driven by confirmatory factor analysis (CFA), is consistent with the German and Greek validations, which also excluded exactly five items due to low factor loadings to improve model fit.43,44 Notably, there is an overlap in the specific items removed; for instance, item 4 (from the Causes and Characteristics domain) was excluded in our study as well as in the German and Greek adaptations,43,44 while item 13 (from the Communication and Behavior domain) was removed in our version and the Greek one, 44 pointing to certain items having inherent cross-cultural psychometric weaknesses. This approach differs from the Spanish and Chinese validations, in which researchers conducted a CFA but ultimately retained all 25 items despite noting weaknesses in some.45,46 The Japanese validation represents yet another approach, where the original 27-item version was reduced to 18 items. Seven items were deleted during preliminary analyses, and two further items (2 and 22) were excluded after principal components analysis (PCA). These latter two overlap with those absent in the international 25-item version, while the additional seven deletions are unique to the Japanese adaptation. 90 These adjustments likely reflect translation challenges and the limited familiarity with dementia in Russia (34% awareness), 20 consistent with validations in Japanese and Spanish.45,90 The translation process simplified technical terms to enhance accessibility for non-specialists. The DKAS-R20 confirmed the four-factor structure (causes, health, communication, care) proposed by Annear et al. (2015), 40 which effectively distinguishes groups by training or experience via Wilcoxon–Mann–Whitney tests, as seen in Greek and Spanish studies.44,45 For example, Seltmann and Teichmann (2024) reported improvements in DKAS scores among German nursing students following training, a finding likely applicable to Russian educational settings. 34 DKAS-R20's sensitivity to group differences aligns with its ability to detect knowledge improvements in German and Greek studies.34,44 The “I don’t know” option further reduces response bias by capturing uncertainty. Our item analysis provided further justification for the scale's refinement, revealing that two of the excluded items—addressing the effectiveness of medications (Item 13: Communication and Behavior) and the sudden onset of cognitive problems (Item 23: Risks and Health Promotion)—were among the most difficult for participants. Comparing these difficult items across validations reveals a complex pattern of shared and culture-specific misconceptions. The misperception regarding the effectiveness of medication for behavioral symptoms (item 13) appears to be a widespread challenge, identified as particularly difficult in the Greek 44 and Japanese validations 90 and also showing a very low score in the Chinese data (as their item 19). 46 The belief that a sudden onset of cognitive problems is typical for dementia (item 23) also proved to be a major misconception in the Chinese (as their item 13), 46 and Japanese studies. 90 However, in a notable cross-cultural difference, this same concept was one of the easiest for the Greek sample, 44 demonstrating that not all knowledge gaps are universal. Regarding the ignorance level, our finding that participants with prior dementia training had significantly lower “I don’t know” rates is strongly mirrored in the German validation. 43
This makes the DKAS-R20 valuable for evaluating educational programs in Russia, where misconceptions (48%) are prevalent, 21 as seen in applications for nursing students, 91 healthcare staff, 46 and caregivers. 35
DAS-R
The Russian version of the DAS showed robust internal consistency (α = 0.81, improved to 0.84 in a refined version), a result consistent with the original validation 48 and adaptations in Turkey and Croatia (α ≈ 0.82–0.85).52,53 While the German version demonstrated higher internal consistency (α = 0.90), 50 the Greek version showed slightly lower reliability (α = 0.74), 51 placing our results well within the expected range for this scale. Subgroup analysis confirmed the reliability of the questionnaire for participants with and without training, supporting its use for nursing students, healthcare staff, and caregivers.32,91–93
A 14-item version (DAS-R14) was created by excluding items 7, 8, 10, 16, 17, and 20 due to low factor loadings, thereby improving the model fit while retaining the original two-factor structure. This approach of item removal differs from most other validations, such as the German and Greek,50,51 which retained all 20 items. However, it aligns conceptually with the Turkish and Chinese53,54 studies, in which researchers also identified psychometrically weak items (including items 8, 16, and 20, which were also removed in our version) and subsequently proposed alternative three-factor structures to better fit their data. The Croatian study 52 also found that the original two-factor model was unstable when applied to the general population. This suggests that while the core concepts of the DAS are robust, cultural and linguistic factors may require structural refinements for optimal performance.
Residual covariances between items (e.g., 3 and 14, 14 and 15) were added due to content similarity (e.g., social interaction), reflecting cultural influences like stigma-related avoidance (51% concealment rate). 15 To suit general audiences, items were adapted by replacing “work” with “interact” and “ADRD” with “Dementia”, as was already done in the German and Greek validation studies.44,50 The DAS-R14's two-factor structure (social comfort, dementia knowledge), as established by O’Connor and McFadden (2010), 48 effectively captures attitudinal barriers in Russia, where stigma (51% concealment) 15 hinders care-seeking and diagnosis. 24 The scale demonstrated strong known-groups validity, effectively discriminating between participants with and without prior dementia-related experience (e.g., personal contact or training), a finding consistent with the German and Greek validation studies.50,51 Furthermore, its sensitivity to change makes it a valuable tool for evaluating educational programs, as demonstrated in intervention studies. For instance, Seltmann and Teichmann (2024) observed enhanced social comfort among German nursing students post-training, a finding relevant to Russia's familist caregiving model, where NGOs often lead efforts to reduce stigma.25,34 The DAS-R14's utility extends to diverse groups, including healthcare staff 92 and informal caregivers, 93 making it a key tool for evaluating programs aimed at reducing stigma and improving attitudes in high-stigma contexts.15,50 Future research should investigate the longitudinal impact of the DAS-R14 in Russian-speaking regions, such as Kazakhstan, incorporating cross-cultural perspectives. 18
CODE-R
Our study demonstrated very satisfactory psychometric properties regarding internal consistency, with Cronbach's alpha of 0.89, which falls in the range of 0.84 to 0.91 reported in Germany, 50 Greece, 51 the UK, 56 Ireland, 58 and Malta. 94 The subgroup analysis showed similarly high reliability for participants with and without training, demonstrating its usefulness for a broad range of participants and for evaluating educational programs. This has already been confirmed by its use in nursing staff,57,94 healthcare staff, 92 psychology students, 51 informal carers, 93 and members of the general public. 50
In accordance with the findings of previous studies in this field,50,51,58 the single-factor solution originally proposed by Elvish et al. (2018) was confirmed. 56 This solution indicates that confidence in dementia care can be measured as a single construct. Nevertheless, Chen et al. (2023) proposed a three-factor solution, which divides the scale into the dimensions “Confidence in early-stage dementia”, “Confidence in middle or late-stage dementia”, and “Confidence in dementia as a whole”. 57 This can be explained by socio-demographic differences between cultures, which are influenced by educational frameworks, clinical experiences, and societal attitudes toward dementia care. 95 Because of significant modification indices, we added residual covariances between certain item pairs, which led to a significant improvement in model fit. In addition, the correlated error terms could also be explained by the similarity of the items. For example, in the study by Conway et al. (2025) 58 and in the validation study by Angelidou et al. (2025), 96 who adapted the scale into German Sign Language, high modification indices were found between items 8 (“I feel able to help a person with dementia feel safe during their stay in hospital.”) and 9 (“I feel able to work with people who have a diagnosis of dementia.”), while residual covariances differed between other items. 96 This once again highlights the importance of validation studies, as the individual items can be understood differently in different cultures and linguistic contexts. 95
CODE-R can discriminate between confidence levels, as demonstrated by Wilcoxon–Mann–Whitney tests. This makes it a valuable tool for evaluating educational programs. This has already been confirmed by Elvish et al. (2018) and Rosi et al. (2023), who identified a significant change in the pre- and post-measurements of a dementia training program for hospital staff,56,97 as well as by Seltmann and Teichmann (2024) and Kimzey et al. (2019) for nursing students.34,98 Besides, CODE-R remains stable over time,34,50,56 making it a useful tool in the field of dementia research — both for hospital staff, students, and caregivers. This is particularly relevant in Russia, where CODE-R can assess training programs to boost caregiver confidence amid prevalent stigma and resource constraints.
Limitations
This study has several limitations. First, the cross-sectional online convenience sample likely introduced self-selection and education biases, limiting generalizability beyond the Russian-speaking population; similar overrepresentation of highly educated and dementia-interested participants has been reported in German validations.43,50 Moreover, the sample included a higher proportion of healthcare professionals than is found in the general population. Their prior training and experience may have positively biased their dementia-related knowledge. This potential overestimation should be considered when interpreting the results and may further limit generalizability to the broader Russian-speaking population.
Second, all three instruments were self-reported and were completed during a single online session, which may increase the assessment burden and susceptibility to social-desirability bias. These issues have also been noted in Greek and Turkish adaptations.51,53 Our online form required complete responses, precluding analysis of missing-data patterns.
Third, known-groups comparisons relied on a self-reported “Dementia course/Training” variable (presence/absence), a design choice also used in the German validation. 50
Finally, several cultural and psychometric adaptations—such as wording changes to align DAS-R with the general population and item reductions in the DKAS-R—improve local validity but may limit strict comparability with original versions and other languages. This challenge and the need for broader convergent validity testing have been emphasized in multiple validations.44,50,51
Conclusion
This study provides the first psychometric validation of the DKAS-R, DAS-R, and CODE-R for Russian-speaking populations. After minor, theory-driven adaptations, all three instruments demonstrated robust structure and reliability, supporting their use to assess dementia knowledge, attitudes, and caregiving confidence. The availability of this validated toolkit creates a solid foundation for evidence-based practice—enabling researchers, educators, and public health stakeholders to systematically evaluate existing awareness campaigns and design targeted interventions to improve dementia literacy in regions where Russian is a primary or widely spoken language.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251409406 - Supplemental material for Validation of Russian versions of the DKAS, DAS, and CODE scales: Measuring dementia knowledge, attitudes, and care confidence
Supplemental material, sj-docx-1-alr-10.1177_25424823251409406 for Validation of Russian versions of the DKAS, DAS, and CODE scales: Measuring dementia knowledge, attitudes, and care confidence by Sergey Zakharov, Aaron Schröter and Birgit Teichmann in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
We want to thank Inna Gidor, Pavel Linitsky, and Taisiya Baysalova for their contribution to the translation procedure of the scales. Special thanks to Claire Eccleston, Melissa O’Connor, and John Keady for their permission to translate and validate the questionnaires into Russian, as well as for their valuable consultations. We also thank Olga Vasilieva for her assistance in data collection.
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of the Faculty of Behavioral and Cultural Studies at Heidelberg University, Germany (AZ Teich 2021 1/1 and AZ Teich 2022 2/1). All procedures followed the ethical standards established in the Declaration of Helsinki, as well as the relevant national and institutional guidelines for research involving human participants.
Consent to participate
Participation in the study was entirely voluntary. Participants were fully informed about the study's objectives, procedures, and data protection measures. Before proceeding with the survey, the research team obtained informed consent electronically via the online questionnaire.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the 4EU + Fellowship for Doctoral Candidates and Researchers Impacted by the War in the Middle East.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. B.T. is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.