
Abstract
Hereditary Alzheimer's disease (hAD) and PSEN2 variants are rare, and the benefit of anti-amyloid β-directed monoclonal antibody (mAb) therapy is unknown. We encountered a 51-year-old Japanese woman with PSEN2-associated hAD. A molecular diagnosis revealed a novel uniallelic missense variant (NM_000447:c.356T > G, p.Leu119Arg) in PSEN2. Intravenous mAb therapy was initiated at age 50, and serial amyloid positron emission tomography showed intense Pittsburgh compound B accumulation and a reduction in amyloid-β deposits in the cerebral cortex after 6 months. Our results suggest that treatment with mAbs has the potential to reduce amyloid deposits in the brain, even in patients with symptomatic hAD.
Keywords
Introduction
Alzheimer's disease (AD) is the most common cause of dementia worldwide. The presence of intracellular neurofibrillary tangles and extracellular plaques in the brain is the histological hallmark of AD; these plaques are mainly composed of the amyloid-β peptide (Aβ), a 40–42-amino acid peptide. 1 Hereditary AD (hAD) is rare and caused by pathogenic variants in the amyloid precursor protein (APP) or presenilin (PSEN1 and PSEN2) genes.2–4 APP is the precursor of Aβ, and presenilin-1 (PS1) and presenilin-2 (PS2) are the protease elements of the γ-secretase enzyme complex, which is responsible for the final release of Aβ peptides from APP.5–7 Heterozygous variants of these genes lead to altered Aβ production. Among patients with hAD, PSEN2 variants are relatively rare, and the clinical benefit of anti-Aβ-directed monoclonal antibody therapy (mAb) is still being uncovered.8–10 Here, we report a Japanese patient with a novel missense variant (NM_000447:c.356T > G, p.Leu119Arg) in PSEN2 who was treated with intravenous mAb.
Case presentation
The patient was a 51-year-old Japanese woman (Figure 1A, III-3) born to non-consanguineous parents. The patient's mother (II-4) had a family history of early-onset dementia. She was admitted to a psychiatric hospital in her mid-sixties and died at 75 years of age. At 45 years of age, her husband first noticed her amnesia. The patient was referred to our hospital at 48 years of age.

Clinical features of the patient with a novel PSEN2 p.Leu119Arg variant. (A) Pedigree of the family. (B) Brain magnetic resonance imaging and amyloid positron emission tomography images of the patient with a PSEN2 pathogenic variant at 50 years of age revealed mild cortical atrophy, predominantly in the medial temporal lobe. (C): Amyloid-β-targeted 18F-labeled positron emission tomography imaging revealed amyloid deposition in the entire brain. (D): Direct nucleotide sequencing of PCR-amplified DNA of the PSEN2 gene. The arrow denotes the substituted bases.
Neurological examination results were not conclusive, and a neuropsychological assessment revealed mild cognitive decline, with scores of 27 on the Mini-Mental State Examination (MMSE) and 21 on the Japanese version of the Montreal Cognitive Assessment. An intelligence assessment using the Kohs Block Design Test revealed an intellectual disability, with a full-scale IQ of 74. Results of routine blood tests, including serum Vitamin B1, Vitamin B12, and thyroid function tests, were normal, and serological testing results for syphilis were negative. Plasma biomarker tests associated with AD revealed elevated levels of phosphorylated tau 217 (pTau217, 2.8 pg/mL; normal range < 0.509 pg/mL) but normal levels of neurofilament light chain (NfL, 24.3 pg/mL) and glial fibrillary acidic protein (GFAP, 595.3 pg/mL). The reference ranges for both NfL and GFAP were established with a reference of <27.1 pg/mL and <186.6 pg/mL, respectively, as indicated. 11 Cerebrospinal fluid analysis revealed elevated levels of phosphorylated tau protein (80 pg/mL; normal range 21.5–59.0 pg/mL). Brain MRI revealed mild hippocampal atrophy (Figure 1B). Single-photon emission computed tomography revealed hypoperfusion in the bilateral parietal lobes, posterior cingulate gyrus, and lateral occipital lobes. Amyloid positron emission tomography (PET) revealed intense Pittsburgh compound-B accumulation in the bilateral cerebral cortex (Figure 1C).
At age 50, intravenous treatment with mAb was initiated. When the patient's condition was re-evaluated 6 months later, her cognitive function, assessed based on the clinical dementia rating (CDR), was preserved, with global score of 0.5 and a sum score of 2.5, whereas that of the MMSE had declined from 25 to 22 (Table 1). Serial amyloid PET showed a reduction in amyloid deposits in the cerebral cortex, with the Centiloid scale decreasing from 94.0 to 62.5.
Serial changes after administration of anti-amyloid beta antibody therapy in neuropsychological studies.
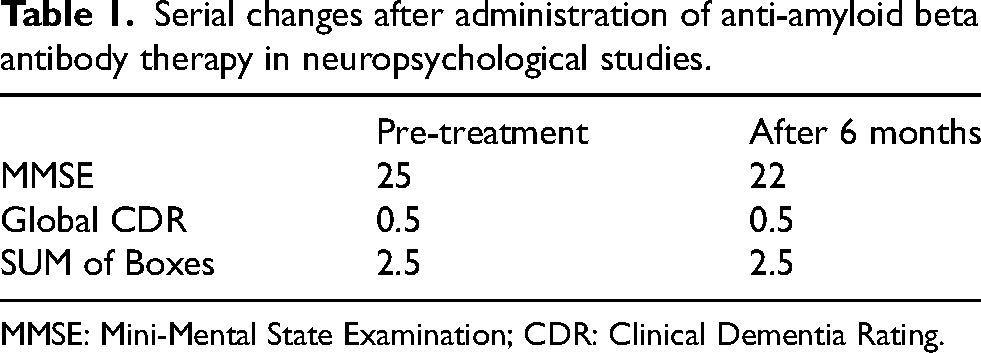
MMSE: Mini-Mental State Examination; CDR: Clinical Dementia Rating.
Because the patient's family history, clinical manifestations, and results of neuroradiological studies were suggestive of hAD, we screened for hAD-associated genes, including APP, PSEN1, and PSEN2, after obtaining informed consent. A molecular diagnosis revealed a novel uniallelic missense variant (NM_000447:c.356T > G, p.Leu119Arg) in PSEN2 (Figure 1D), and the Apolipoprotein E genotype was ε3*4. This variant has not been described in human genome variation databases, including Genome Aggregation Database (gnomAD) (https://gnomad.broadinstitute.org/ or disease-causing mutation databases, such as the Human Gene Mutation Database (HGMD) (http://www.hgmd.org/) and ClinVar (http://www.ncbi.nlm.nih.gov/clinvar/). Genetic counselling has been offered to at risk family members, including the patient's sister. They have not yet requested genetic testing.
Protocol approval
This study was approved by the Ethics Committee of Shinshu University School of Medicine and the Ethics Committee of Niigata University.
Discussion
In this study, we present the first case of a PSEN2 variant in a patient with hAD in Japan. As the clinical, neuroradiological, and laboratory features, including pTau217, were consistent with AD, we searched for variants of APP, PSEN1, and PSEN2 in this patient. A molecular genetic analysis revealed that the patient had a novel heterozygous missense variant, p.Leu119Arg, in PS2. The Leu119 residue of PS2 is located in hydrophilic loop-1 (HL-1), which is situated between the first transmembrane domain (TMD) and TMD2. HL-1 is an intrinsically disordered region that is highly conserved among species. HL-1 of PS1 and PS2 is a key region that appears to participate in substrate docking, γ-processivity, and the binding of γ-secretase modulators (GSMs), including APP and NOTCH1, to enhance processivity. 12 Moreover, HL-1 of PS1, which is highly homologous to that of PS2 (Figure 2), is a hotspot for the pathogenic variants of hAD (https://www.alzforum.org/mutations). These findings suggest that the HL-1 region of PS2 is a potential hotspot for pathogenic variants, similar to those found in PS1. Leu113 may play an important role in the functions of GSMs, specifically stimulating pathogenic Aβ peptide processing. 13 Additionally, p.Leu113Pro in PS1, a homologous residue of Leu119 in PS2, is reportedly pathogenic. 14 In silico prediction programs, including CADD (https://cadd.gs.washington.edu/) and MutationTaster (https://www.mutationtaster.org/), predicted that this variant is highly deleterious, with scores of 26.4 and 1, respectively. Based on the patient's clinical findings and structural and functional properties of p.Leu119Arg, this variant was considered pathogenic.

Schematic images of hydrophilic loop-1 (HL-1) and pathogenic missense variants in PSEN1 and PSEN2. Sequences of PSEN1 (PS1) or PSEN2 (PS2) and missense variants in both PSEN1 and PSEN2 genes, which have been reported as pathogenic or likely pathogenic in the ALZFORUM database (https://www.alzforum.org).
To date, the clinical efficacy of mAb for patients with hAD has not been clearly demonstrated. In this study, our patient received mAb for 6 months, and neuroradiological studies showed reduced Aβ deposition in the brain, with no adverse events, including amyloid-related imaging abnormalities. The results of her cognitive function tests were controversial; however, those of the CDR assessment suggested that her cognitive abilities had not declined. The Dominantly Inherited Alzheimer Network Trials Unit (DIAN-TU) showed the pharmacological effects of gantenerumab on biomarkers. 15 In contrast, a randomized controlled trial (DIAN-TU-001) did not show a significant benefit for pre-specified cognitive outcomes, 16 whereas open-label extension analyses suggested that prolonged, high-dose gantenerumab delays symptom onset and dementia progression. 17
For at risk family members of hAD patients, early intervention with disease-modifying therapies is expected to significantly enhance daily activities for patients with hAD and improve their overall prognosis. In recent years, effective disease-modifying therapies have been introduced for an increasing number of inherited neuromuscular diseases, including hereditary ATTR amyloidosis. For family members at risk of these diseases, clinical management involving predictive genetic testing and genetic counselling could facilitate early intervention with disease-modifying therapies. 18 The successful development of future disease-modifying therapies for hAD could lead to widespread acceptance among individuals at risk, who could benefit from appropriate genetic counseling and proper medical management. Therefore, the long-term pharmacological effects of mAbs in symptomatic patients with hAD and a PSEN2 variant need to be elucidated.
Conclusion
In conclusion, we reported a patient with a novel PSEN2 missense variant. Our results show that treatment with mAbs has the potential to reduce amyloid deposition, even in patients with symptomatic hAD. Studies involving more symptomatic patients and asymptomatic carriers are required to gain further insight to improve hAD management.
Footnotes
Acknowledgements
The authors thank Ms. K. Toba, Ms. S. Takahashi, and Ms. C. Nishizawa for helpful support.
Ethical considerations
This study was approved by the Ethics Committee of Shinshu University School of Medicine and the Ethics Committee of Niigata University.
Consent to participate
The patient provided written informed consent for participation in the study.
Consent for publication
Not applicable.
Author contribution(s)
Funding
This study was supported in part by the program for dementia research and development, AMED, under Grant Number JP23dk0207066h0001, JP24dk0207066h0002, JP25dk0207066h0003, and JP25dk0207060.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available on request from the corresponding author.