
Abstract
Background
There is strong desire for the return of individual results, including biomarker testing, among participants in Alzheimer's disease and related dementias (ADRD) studies. However, it is not known whether participants accurately understand the utility, limitations, benefits and risks of biomarker disclosure, nor how they weigh these factors to inform their decision to undergo testing and learn results. Furthermore, little is known about how factors like participant race or diagnosis influence a desire to learn biomarker results.
Objective
This mixed-methods study explored how clinically and racially diverse participant-care partner dyads perceive and plan to use AD biomarker testing in the context of research studies.
Methods
57 participants (Age: M = 74.28 ± 5.98; Race: n = 22 Black, n = 35 White; Diagnosis: n = 23 with mild cognitive impairment; n = 34 cognitively healthy) and care partners were recruited from AD studies wherein the participant completed amyloid-β and tau positron emission tomography without receiving results. Each completed an independent interview about their perspectives on learning the participant's results.
Results
Responses suggested strong interest in learning results, driven by perceived benefits (e.g., informing treatment, lifestyle changes, and social support). Risks were rarely discussed, though some respondents cited concerns about psychological burdens of a positive result. Few nuanced differences in perceived risks or benefits were observed across race and diagnosis.
Conclusions
The decision to learn the results of biomarker testing is motivated by highly varied perceived benefits and minimal consideration of risks. Testing should be preceded by individualized counseling that carefully reviews potential benefits and risks.
Introduction
Alzheimer's disease (AD) represents a profound global challenge to public health and caregiving systems, with an exponentially growing impact. The prevalence of dementia-Alzheimer's type (DAT), the form of dementia caused by AD, is expected to surge dramatically by 2060 with projections of 13.8 million cases in individuals 65 and older. 1 Increasing prevalence of AD and limited treatments for the cognitive and behavioral sequalae highlight the urgent need for earlier identification of those with the disease. Biomarkers found in cerebrospinal fluid, plasma, and via neuroimaging modalities like positron emission tomography (PET) now allow the measurement of abnormal amyloid-β (Aβ) and tau protein levels—the hallmark pathological characteristics of AD—not only before a person passes away, but years before onset of symptoms.2–4 Early detection of biomarker positivity offers a crucial opportunity to intervene and potentially delay disease and/or symptom progression by enabling individuals to access treatments and clinical trials, adopt healthier lifestyles, and mitigate lifestyle risk factors for DAT.5–7
Biomarker testing occurs frequently in research settings, often as part of determining eligibility for specific trials or to otherwise characterize participants.8,9 Until recently, researchers rarely shared individual results with research participants; however, there is currently a growing demand to do so. 9 There has also been greater clinical translation of biomarkers in recent years–a shift that has been accelerated by the Centers for Medicare & Medicaid Services approval of Medicare coverage for serial positron emission tomography (PET) scans for Aβ 10 and approval of anti-Aβ medications. Moreover, the emergence of direct-to-consumer blood-based biomarker tests 11 has further transformed the landscape, such that individuals may soon be able to access these assessments without consultation from their medical providers.
Though the development and implementation of biomarker testing represent an exciting advancement for AD research and clinical care, the ethics of disclosing this information to participants and patients are complex. There is, to date, no standard set of guidelines regarding when and how AD biomarker status should be communicated, despite the potential impact on the individual's well-being, familial relationships, and broader societal implications. The limited data on post-disclosure outcomes suggest that learning a positive AD biomarker result has relatively minimal effects on anxiety, depression, or distress,12–14 and that learning a negative AD biomarker result can offer emotional relief. 15 However, fears about anticipatory grief, anxiety, or suicidality may still restrict interest in testing or learning results. Patients and participants may also be concerned about social discrimination and stigma based on their results. 16 Additionally, individuals may worry about the potential for medical, insurance, employment, or housing discrimination following testing. 16 The Genetic Information Nondiscrimination Act has been implemented to prohibit discrimination by employers and health insurers based on genetic information, but no federal protections currently exist for individuals with elevated AD biomarkers.6,9 These concerns can impact recruitment into AD biomarker research and clinical trials in which biomarker testing is involved 17 or even care-seeking behaviors, with mistrust and access concerns acting as formidable barriers, particularly among African Americans.18,19 It is also important to consider that the aforementioned risks of learning and sharing biomarker results—distress, stigma, and medicolegal discrimination—are already experienced at disproportionate rates by minoritized racial-ethnic groups. To date, few studies have evaluated how beliefs about the utility/benefits and risks of testing impact interest, particularly among diverse older adults and their care partners.20–23
The rationale for offering biomarker results is multi-faceted. In research settings, returning results can promote autonomy, transparency, and trust-building between researchers and participants, fostering a supportive and collaborative relationship.6,24,25 Individuals involved in AD research express interest in receiving research results, and the lack of disclosure is considered a potential barrier to willingness to participate in research. 19 Additionally, providing individuals with AD biomarker results empowers them to make informed decisions and positive changes in various aspects of their lives. This includes adopting a brain-healthy diet and engaging in regular exercise associated with cognitive health. 6 Furthermore, armed with knowledge about their biomarker status, individuals may proactively plan for the future by appointing a legally authorized representative, exploring alternative or assisted living arrangements, and engaging in other advanced planning. 25 The multifaceted impact of AD biomarker results extends beyond awareness, encouraging individuals to take concrete actions that enhance their current and future health.
Given the complexity of potential risks and benefits and the potential for disproportionate risk among those from diverse backgrounds, it is critical to evaluate diverse perspectives on AD biomarker testing. Little is known about how familiar community-dwelling older adults and their loved ones are with the complex benefits and risks mentioned above, nor how they weigh these in decisions about whether to get tested for AD biomarkers. The present study aimed to leverage mixed methods to examine perspectives on the impact, benefits, and risks of AD biomarker testing among participants and their current or future care partners. Additionally, we explored differences in beliefs by race and in cognitively normal individuals and those with amnestic mild cognitive impairment (MCI).
Methods
Participants
Participants aged 65 and older were recruited from ongoing research studies conducted through the Research Program on Cognition and Neuromodulation Based Interventions and/or the Michigan Alzheimer's Disease Research Center (MADRC). During their involvement in these studies, participants completed the National Alzheimer's Coordinating Center (NACC) Uniform Data Set-3 (UDS-3) 26 and additional neuropsychological tests. Using the NACC criteria, participants were diagnosed as cognitively healthy older adults (HOA) or with mild cognitive impairment. 27 Participants with a history of severe mental illness, substance use disorder, current moderate-to-severe anxiety or depression, or other significant neurological illness or injury were not eligible to take part.
Unlike the limited extant literature on perspectives of AD biomarker testing that involved respondents considering hypothetical biomarker testing, we aimed to survey individuals for whom this decision was less hypothetical; we therefore included participants who had either already undergone or were scheduled to undergo PET Aβ and tau scans through prior research involvement. At the time of completing these scans, participants were told that they would not receive their results (as this was not a clinical or research standard at the time of parent study development). Individuals who previously underwent and learned the result of AD biomarker testing in prior research or clinical settings were not eligible, as we were specifically interested in the perspectives of individuals who had not previously considered this decision.
Procedures
After completing parent studies, participants were recruited into the present study: the Sharing Alzheimer's Risk Estimates in Diverse Communities (SHARED) study. All participants were required to identify a study partner, defined as the person currently serving as a caregiver or the person who would likely serve in this role if needed in the future. Study partners included adults aged 18 years and older who were cognitively healthy as determined by either recent cognitive evaluation or cognitive screening with the Montreal Cognitive Assessment prior to study involvement. Study partners were required to know the participant for at least five years and to have regular written virtual or in-person contact with the participant. Like participants, study partners were required to have stable mental health without a history of severe mental illness, neurologic, or substance use disorder.
All procedures were approved by the Institutional Review Board of the Medical School at the University of Michigan and in accord with the Helsinki Declaration of 1975. Given that participants included those with MCI, the study team assessed decisional capacity for research participation during the consenting process. Only those who were able to demonstrate capacity and provide consent, or those with a legally authorized representative for research who provided consent (with assent from the participant) were included. Interviews were conducted in person or via secure video-conference visit between October 2019 and November 2020. Participants and study partners were interviewed separately to minimize dependence of responses.
Measures
Disclosure needs assessment interview
Dyad members completed semi-structured interviews with a trained study team member. The interview involved both open-ended qualitative questions and fixed-response survey-style items. The latter quantitative items are summarized in a prior paper. 21 Questions explored interest in and perspectives about receiving the participant's PET Aβ and tau biomarker results and associated information about Alzheimer's disease etiologic diagnosis and risk for DAT. Items queried perceived meaning of elevated and not-elevated biomarker results, as well as utility/benefits and deterrents/risks of PET biomarker results. Additionally, participants described how they would cope if biomarker results were indicative of increased risk for DAT. Prompt questions are listed in Table 1. Interviews were recorded digitally, then manually transcribed and de-identified.
Interview items with demonstrative responses and assigned codes.

Analyses
Qualitative coding was initiated by independent line-by-line open coding on five transcripts. Preliminary codes were defined through several consensus meetings with the analysis team, comprising faculty content experts, a faculty qualitative research consultant, and research staff. Sample responses to interview items and their codes are described in Table 1. The final codebook included three categories (perceived risks of knowing biomarker results, perceived benefits of learning biomarker results, and coping strategies for an elevated result), each capturing multiple specific themes. Theme frequencies (Table 2) represent the number of participants or study partners who provided a response that aligned with each specific theme, not the number of times a theme was mentioned.
Themes endorsed by participants and study partners, by race of respondent.

*significant difference between frequency of theme endorsement by race at p < 0.05. N/A: chi-squared test not applicable because of exactly equal frequency of theme endorsement between groups.
After finalizing the codebook, the gold standard coder (ML) and secondary coder (AB) used Dedoose (Version 9), 28 to code the remaining transcripts. The third independent rater (ARF) resolved any coding disagreements between the primary and secondary coder. Dedoose was used to calculate inter-rater reliability, resulting in a Kappa coefficient of 0.98. We used chi-square tests to evaluate differences in theme endorsement among participants by race (Black versus white) and diagnosis (HOA versus MCI). We used the same approach to compare frequency of theme endorsement among study partners.
Results
As described in Table 3, the total sample included 57 participants (n = 22 Black; n = 35 White; age = 74.28 ± 5.98, education = 16.33 ± 2.75) and their respective care partners (n = 19 Black; n = 38 White; Mage = 66.93 ± 10.92, Medu = 16.18 ± 2.49). Twenty-four participants were diagnosed with MCI (42.1%) and the remaining 33 were HOA (57.9%).
Demographic characteristics of the sample (n = 57 dyads).

*significant at p < 0.05
Perceived vulnerability to AD and relationship to interest in biomarker results (all respondents)
The majority of respondents relayed concerns about the participant's personal vulnerability to DAT, often based on the participant's family history or subjective memory complaints. This perceived vulnerability was listed as a key motivator for wanting to receive biomarker information for most respondents (72% participants; 58% study partners). In contrast, approximately half of the participants and study partners (51% of each) described wanting biomarker information to help augment their general, not personal, knowledge about AD and DAT.
Perceived benefits and utility of learning AD biomarker results (all respondents)
Many participants discussed the clarity provided by biomarker disclosure as a significant benefit and tool for planning for the future, though confusion persisted regarding nomenclature and what a test actually reveals (etiological versus clinical or phenotypic diagnosis). For example, when asked about potential benefits, one participant responded that “Having a diagnosis of Alzheimer's dementia would give some definition to what to expect, although the timeline of Alzheimer's dementia is varied in between individuals.” As depicted in Figure 1, all respondents listed at least one specific action they would take based on learning the participant's biomarker results, including planning for the future (81% participants; 74% study partners), making a specific clinical decision (e.g., anti-Aβ medication use; 63% participants; 61% study partners), making lifestyle changes such as diet or exercise (56% participants; 53% study partners), and seeking social support from or sharing results with family (56% participants; 74% study partners).
Frequency of endorsement of perceived benefits of biomarker disclosure in total sample (n = 57 dyads).
Perceived risks of learning AD biomarker results (all respondents)
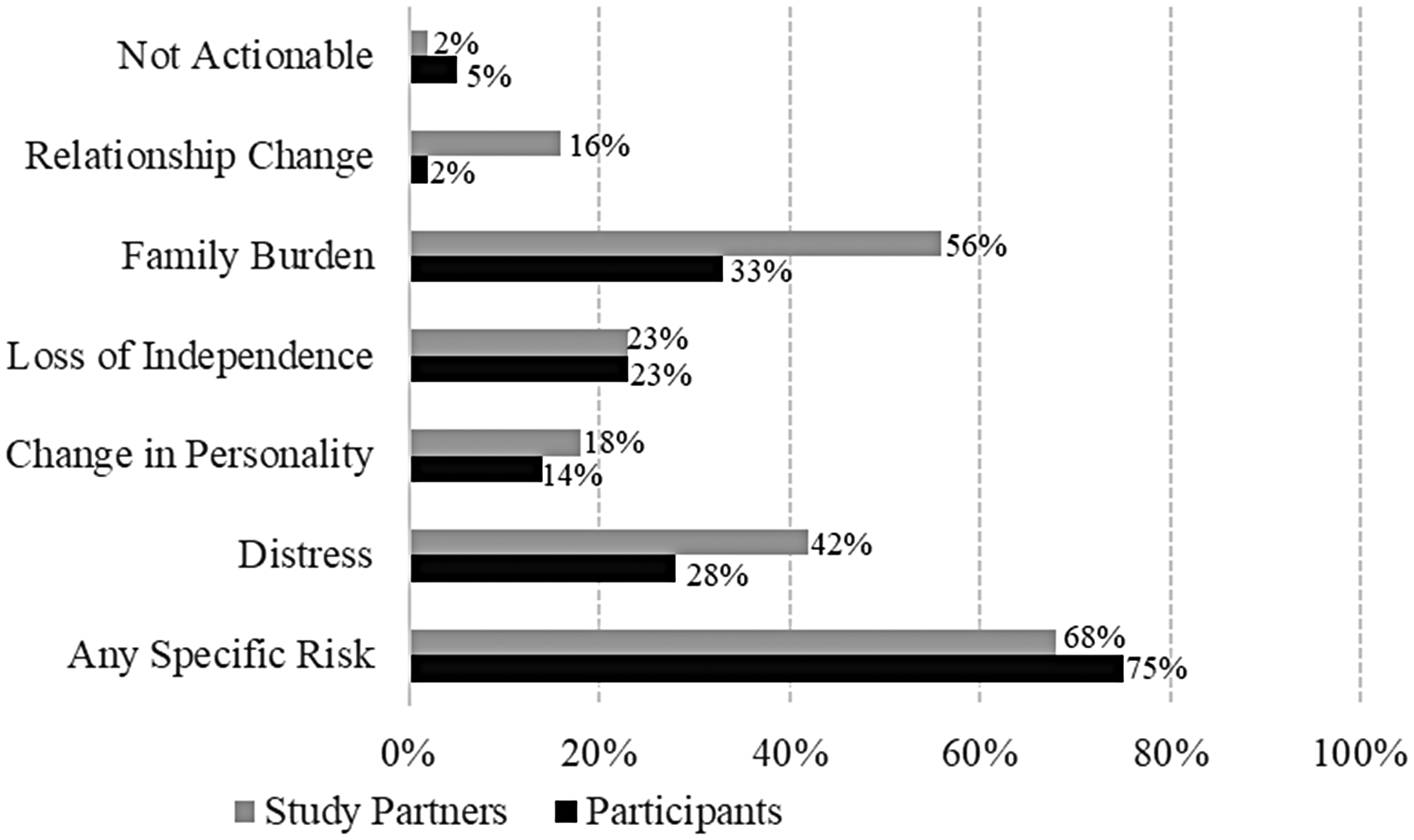
The endorsement of perceived risks was significantly more limited than discussion of benefits. As depicted in Figure 2, the most frequently reported risks of learning the participant's biomarker results included concerns about the potential burden of an elevated result on family (33% participants; 56% study partners) and on the participant's psychological health (28%; 42%). Participants were also apprehensive about a loss of rights or independence if found to be biomarker positive (23%; 12%). Risks commonly discussed in the literature, such as information not being ‘actionable’, were rarely mentioned by respondents (5% participants, 2% study partners). Of note, among the 68% of participants and 75% of study partners who described some concern about risks or limitations of biomarker testing, all expressed a desire to still learn the participant's results. Participants clarified that, while some risks or barriers to disclosure existed, they were far outweighed by desire to know: “I mean, if I had to say a reason it would just be the worry that would be associated with it, but- I would say I would want to know.” Conversely, some participants denied any concerns about risks or limitations to learning one's results: “There is absolutely no reason that I can think of that I wouldn’t want to know…I’d much rather have the information on the front end, than be surprised down the line.”

Frequency of endorsement of perceived risks of biomarker disclosure in the total sample (n = 57 dyads).

Frequency of endorsement of coping responses following biomarker disclosure in the total sample (n = 57 dyads).
Potential coping with elevated biomarker results (all respondents)
Participants and study partners alike reported a strong sense of ability to cope with learning biomarker results, even if elevated (Figure 3). Fifty-eight percent of participants and 60% of study partners provided responses alluding to general resilience. Others took an action-oriented approach, citing how they would cope by leveraging results to guide risk-reducing behavior: “I would want [to know], first of all, if there was any way in which it [dementia] could be prevented. Which I don’t think, but at least the process slowed down. So, is there any physical things that I could do? Alter my physical activity? Is there any nutritional things I could do? Is there any medical interventions that could be taken? I would seek out information from an Alzheimer's organization, I think that would be the primary thing. And direction from- And I would talk to my PCP. And I guess I would utilize the internet.” More than half of participants (56%) and almost three-quarters of study partners (74%) reported that they would rely on support from loved ones following disclosure. A small percentage of respondents (9% participants; 4% study partners) described faith or spirituality as a source of strength after learning their results.
Differences in biomarker disclosure decision theme endorsement by race (Table 2)
Among participants, there were few differences in the discussion of specific risks of disclosure based on race. Only concern about the participant experiencing post-disclosure distress differed between racial groups, with 46% of Black participants discussing this theme compared to 17% of White participants (p = 0.03). Regarding perceived benefits of disclosure, more White study partners (71%) described wanting results to inform clinical care, compared to Black study partners (42%; p = 0.046). There were no differences in anticipated post-disclosure coping by race among participants or study partners. Table 4.
Differences in themes endorsed by participants and study partners, by participant diagnosis.

*significant difference between frequency of theme endorsement by participant diagnosis at p < 0.05. N/A: chi-squared test not applicable because of exactly equal frequency of theme endorsement between groups.
Differences in biomarker disclosure decision theme endorsement by participant diagnosis (Table 4)
There were no differences in the frequency of risks discussed by cognitively healthy participants versus those with MCI, nor in their respective study partners. When considering potential benefits of learning the participant's biomarker results, more cognitively healthy participants (91%) cited advanced planning as a motivator for learning AD biomarker results, compared to participants with MCI (67%). There were no differences in discussion of benefits among study partners of those who were cognitively healthy versus those with MCI. Similarly, there were no group differences in anticipated coping with positive biomarker results in participants or study partners based on participant diagnosis.
Discussion
This study investigated perceptions of testing for and learning results from AD biomarker testing among cognitively healthy and symptomatic participants and their care partners. Consistent with prior literature,12,17 our findings demonstrate that participants and study partners alike emphasize benefits of learning research-based biomarker results including using this information to guide changes in lifestyle (e.g., diet, exercise, cognitive training), advanced care planning (e.g., planning living arrangements, drafting a will, assigning a durable power of attorney, informing their physician, and managing finances) or clinical care (e.g., seeking specialty care or anti-Aβ therapies). This finding underscores that early biomarker testing may drive both proactive health management and personalized medicine.5–7,15,23 Although these broad benefits should be considered as part of an informed decision about undergoing biomarker testing, so must the limitations of testing and additional barriers to accessing both testing itself and the potential benefits of testing. For instance, many Aβ positive participants will be unable to realize the perceived benefit of anti-Aβ therapies due to high costs, logistical barriers (e.g., access to a medical center with infusion and imaging resources), or disqualification due to comorbid medical conditions. Researchers and clinicians have a responsibility to educate the community and their patients/participants regarding these contextual factors prior to offering testing, as removal of these benefits could affect the decision to test.
In contrast to the strong and heterogeneous benefits described by participants and their care partners, few risks or deterrents to testing were recognized or discussed in our sample. While some anticipation of psychological distress was described, other risks like stigma and medicolegal discrimination were largely ignored. This stark finding mirrors results from our previously published quantitative data that demonstrate that over 80% of participants and care partners denied any significant risks of undergoing biomarker testing. 21 Lack of knowledge about the potential risks of testing limits patients’ and participants’ ability to make an informed decision about the procedure or take action to mitigate risks. For example, a participant with concerns about post-testing distress may engage in mental health treatment in preparation for testing. Conversely, a participant with concerns about housing or long-term insurance discrimination based on an elevated biomarker result may elect to apply for these services before testing is completed. With sufficient warning about the potential for stigma or discrimination, participants found to be at-risk for DAT based on biomarker results may be more cognizant of accidental data sharing. Therefore, by not providing pre- and post-test counseling that clarifies both benefits and risks, researchers and clinicians are not only violating multiple ethical principles, including respect for participant autonomy, and protection from potential harm.
While few, the nuanced differences in perceived risks, benefits, and coping ability by diagnosis or race highlight that the risk-to-benefit ratio of undergoing biomarker testing is not equal across all participants and situations. For example, while race-based differences in themes endorsed were few, Black participants were more concerned about psychological distress and loss of independence compared to White participants. Furthermore, White participants and care partners focused more on planning and health-related changes in the context of higher perceived resilience and self-efficacy compared to Black participants and care partners, respectively. It is possible that the desire among Black participants to avoid negative outcomes may reflect the burden of disparities and experiences of discrimination already disproportionately affecting this group; in contrast, it may reflect a known disparity in health knowledge, including about AD biomarkers, in minoritized communities. Furthermore, it is well-established that Black older adults experience a range of psychosocial and environmental stressors (e.g., neighborhood disadvantage,29,30 discrimination and stigma 31 ) that contribute to higher chronic distress. It is possible that Black participants’ significantly higher concern regarding negative psychological sequelae of learning a positive biomarker result reflects an overall heavier and longer-standing burden of distress secondary to contextual and interpersonal factors. It is imperative that future protocols for educating patients about and offering results of AD biomarker testing consider these sociocultural factors and are adapted for the needs of individual patients.
Participants with MCI were also more concerned about loss of rights and independence based on results. This concern is not unfounded; in the absence of legal protections, there is potential risk of medicolegal, employment, housing, and other discrimination based on biomarker status. As relative risks and benefits are not universal across clinical stage, pre-disclosure counseling and educational materials must be tailored to those with and without cognitive impairment, and must take into account critical sociodemographic factors (e.g., financial stability, healthcare access, employment status) to support informed decision making for all. 5
The post-disclosure anxieties anticipated by respondents highlight the importance of post-disclosure support, 32 including availability of psychological counseling, caregiver preparation, advanced planning services, and pathways to specialty care. While pragmatic limitations in expertise, time, and funding undoubtedly exist in the research context, investigators plan funding applications to include the resources required for a thoughtful disclosure protocol that includes follow-up and safety assessment. Nonetheless, researchers cannot fulfill all needs of participants following biomarker testing, raising a larger issue of insufficient capacity for mental health and dementia-related care in the community. As research-based testing increases in parallel with implementation of blood biomarkers in primary care settings (with direct-to-consumer testing on the horizon), the number of patients needing monitoring, treatment, and advanced care planning is expected to increase exponentially. Most counseling and other specialty care services are currently housed at academic medical centers or large hospital systems that are inaccessible or unaffordable to many patients and already overburdened. Wait times to access specialty care are estimated to be 12 months with confirmed biomarker positivity (and over 50 months with only a positive cognitive screen). 33 Furthermore, prior literature suggests that, despite having greater risk of developing DAT, Black patients wait longer for a diagnosis and are less likely to seek specialty care and treatment as compared to White patients.23,34,35 This may be in part due to greater perceived stigma from and poorer trust in medical providers at larger institutions. 23 There remains a critical need to increase capacity for dementia and mental health care at federally qualified health centers and other community-based organizations. The diverse post-disclosure needs of participants also call for a more interdisciplinary approach to returning individual results, including the incorporation of social work and care navigation.
Finally, there is a need for effective community education to address the knowledge gaps we identified regarding AD biomarker testing. This curriculum must include broad information clarifying the differences between AD and other dementias, utility and limitation of testing, and potential risks and benefits. Such education is crucial for informed decision-making and advocacy efforts. Broad availability of biomarker testing has the potential to address the known disparities in how early, accurately, and frequently participants from minoritized backgrounds are diagnosed and treated, but only if all communities are aware of and can make informed decisions about testing, and have access to the necessary services to leverage test results towards treatments and advance planning.
Limitations and future directions
Our study excluded individuals with significant mental health conditions, which could affect the generalizability of our findings. Reasoning around and, therefore, interest in biomarker testing could differ in those with significant psychiatric history. On the one hand, participants with mental health conditions could seek to avoid the potential distress induced by an etiologic diagnosis of a disease without a known cure; on the other, participants with greater anxiety may seek information early as a means of coping. This population is also likely to react differently to return of biomarker results. While prior studies (including our own) have predominantly focused on those without significant current mental health conditions, some research has included broader groups. As blood-based biomarker testing becomes more accessible in primary care and direct-to-consumer settings, it is likely that a more diverse population, including those managing these conditions, will seek testing. It is therefore critical to understand pre- and post-disclosure needs, and how shared decision-making should be adapted to balance safety, autonomy, beneficence, and non-maleficence.
While results did not support significant variation in responses by race, it is important to note that our participants did not differ significantly on many social determinants that drive racialization and disparities (i.e., education level, healthcare access, insurance status, and healthcare access). Additionally, we recognize that categorical race-based comparisons may mask the massive heterogeneity within racialized groups. Broader investigation of testing and disclosure preferences and needs is essential with a sample that includes a wider range of education, income, healthcare access, health literacy, and ethnic/cultural backgrounds. This study did not include races or ethnicities outside those identifying as Non-Hispanic White and Non-Hispanic Black or African American and consisted of a highly educated sample across both racial groups, which may limit the generalizability of the findings. Futures studies must use community-engaged approaches to evaluate the needs of other diverse communities particularly those with varying educational and socioeconomic profiles, to develop culturally informed practice guidelines.
This study aimed to explore various perspectives of AD biomarker disclosure among Black and White participants with and without MCI, and their care partners. Across race and diagnosis, results indicate strong interest in and perceived benefit of receiving AD biomarker risk information, despite relatively minor concerns or barriers associated with testing and learning results. Participants, regardless of their cognitive status, demonstrated a readiness to use biomarker results for proactive health management, highlighting the value of personalized information in guiding clinical care and lifestyle changes. However, the study also underscores the need for culturally sensitive and comprehensive support services to address the psychological and social implications of biomarker disclosure. Furthermore, this research lays the foundation for future research to expand in sample diversity and employ mixed methods approaches to capture a more nuanced understanding of the long-term implications and effectiveness of disclosure practices, ultimately enhancing protocols to better support individuals navigating the complexities of AD diagnosis and treatment.
Footnotes
Acknowledgements
The authors would like to acknowledge the contributions, time, and effort of the participants and families who took part in this study.
ORCID iDs
Ethical considerations
The Institutional Review Board of the Medical School at the University of Michigan approved our mixed-method surveys and interviews (approval: HUM00160276) on March 19, 2019. All participants were provided with a written consent form that was described, section-by-section, by a trained study team member. Using a standardized decision-making capacity assessment tool, study staff asked questions to ensure that all participants were able to understand the study procedures, purpose, potential risks and benefits, and alternatives. Participants then provided written consent for study procedures and publication of anonymized responses and data. No photos or images were taken as part of this study.
Consent to participate
All participants were provided with a written consent form that was described, section-by-section, by a trained study team member. Using a standardized decision-making capacity assessment tool, study staff asked questions to ensure that all participants were able to understand the study procedures, purpose, potential risks and benefits, and alternatives. Participants then provided written consent for study procedures and publication of anonymized responses and data. No photos or images were taken as part of this study.
Consent for publication
All participants provided written informed consent to conduct the study and publish their de-identified responses and results. No photos or images were taken as part of this study.
Author contribution(s)
Funding
This work was supported by funding from the National Institute on Aging and American Federation for Aging Research (NIA/AFAR R03-AG063222 [PI: Rahman-Filipiak]). Additional support was provided by funding from the National Institute on Aging (R01AG058724 [PI: Hampstead]; R35AG072262 [PI: Hampstead]; P30 AG072931 [PI: Paulson]; and K23AG070044 [PI: Rahman-Filipiak]).
National Institute on Aging, (grant number K23AG070044, P30 AG072931 , R01AG058724, R03-AG063222 , R35AG072262).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.