
Abstract
Background
Atrial fibrillation (AF) and dementia frequently coexist in older adults, yet the impact of anticoagulation on cognitive and clinical outcomes in this population remains uncertain.
Objective
To evaluate the effects of anticoagulation on cognitive and clinical outcomes in patients with AF and dementia.
Methods
This retrospective cohort study included 291 patients aged ≥65 years with AF and dementia, treated at a tertiary center between January 2020 and December 2024. Patients were grouped by anticoagulation status. Cognitive, functional outcomes (Mini-Mental State Examination [MMSE], Activities of Daily Living [ADL], Clinical Dementia Rating–Sum of Boxes [CDR-SB]) and clinical endpoints (all-cause mortality, hospitalization, major adverse cardiovascular events, and bleeding) were assessed over a median 28-month follow-up.
Results
Anticoagulated patients were younger (82.8 versus 85.1 years, p = 0.01). Anticoagulation was associated with slower cognitive/functional decline, with medium effect sizes, ΔMMSE mean difference: 2.0 points (95% CI: −3.5 to −0.4; p = 0.048), ΔADL mean difference: 10.9 points (95% CI: −19.6 to −2.3; p = 0.02), ΔCDR-SB mean difference: −1.4 points (95% CI: 0.4 to 2.4; p < 0.01). In multivariable Cox models, anticoagulation reduced hospitalization risk (HR 0.60; 95% CI: 0.43–0.84; p < 0.01) and all-cause mortality (HR 0.59; 95% CI: 0.40–0.88; p = 0.01). Benefits were most pronounced in very mild dementia and Alzheimer's disease.
Conclusions
In this retrospective, confounder-adjusted study, anticoagulation was associated with slower cognitive/functional decline and lower hospitalization/mortality risk in AF and dementia patients. The findings warrant prospective research to investigate whether anticoagulation has disease-modifying effects in early-stage dementia.
Introduction
Atrial fibrillation (AF) and dementia are prevalent comorbidities among older adults, both of which share several cardiovascular risk factors such as hypertension, diabetes mellitus, and heart failure.1,2 However, recent evidence indicates that AF is not only a comorbid condition but also an independent risk factor for cognitive decline and dementia—even in the absence of overt stroke. Several pathophysiological mechanisms have been proposed to explain this association, including silent cerebral infarcts, chronic cerebral hypoperfusion, systemic inflammation, and cerebral micro-emboli.3,4 These mechanisms are thought to contribute to both vascular cognitive impairment and Alzheimer's disease (AD) pathology, making AF patients, particularly vulnerable to cognitive deterioration.
In support of this, Nakase et al. reported that AD or mild cognitive impairment (MCI) patients with AF exhibited significantly worse cognitive function, as measured by the Mini-Mental State Examination (MMSE: 19.4 versus 22.0, p = 0.034), and greater periventricular white matter lesions (6.85 ml versus 4.37 ml, p = 0.007) compared to those with sinus rhythm. These findings suggest that AF-associated cerebrovascular injury may contribute to the accelerated cognitive decline observed in this population. 5
While anticoagulation therapy is the cornerstone of stroke prevention in AF, its role in mitigating cognitive decline and dementia remains a topic of ongoing investigation. Observational studies have proposed that direct oral anticoagulants (DOACs) may offer protective cognitive benefits by reducing micro-embolic events and maintaining adequate cerebral perfusion.6,7 A comprehensive systematic review involving over 600,000 patients found that anticoagulation therapy was associated with a reduced risk of dementia, with DOACs outperforming vitamin K antagonists (VKAs) in several analyses. Notably, the cognitive benefit of warfarin was most pronounced when the time-in-therapeutic-range (TTR) exceeded 70%—a threshold infrequently achieved in real-world settings.3,8
Nevertheless, randomized trials evaluating cognitive outcomes with anticoagulation in AF patients with dementia remain limited. The CAF Trial, a vanguard randomized study comparing dabigatran with warfarin, demonstrated no significant differences in cognitive trajectories over a 2-year period, although both therapies were well managed and no patients developed dementia during follow-up. 9 These findings highlight the complex interaction between anticoagulation, stroke prevention, and cognitive outcomes. In addition, a Spanish registry of older adults with moderate-to-severe dementia reported that anticoagulation did not reduce mortality, and several systematic reviews have reported no consistent cognitive benefit associated with anticoagulation use.10–12 These findings suggest an alternative hypothesis: cognitive decline in dementia may progress predominantly due to underlying neurodegenerative processes, regardless of AF related micro-embolism or anticoagulation status.
Cognitive impairment itself is a recognized predictor of poor prognosis in AF. The ANAFIE Registry demonstrated that patients with MMSE scores ≤23 had significantly higher rates of all-cause and cardiovascular mortality, as well as a greater incidence of adverse clinical events, compared to cognitively intact individuals. 13 Furthermore, the MMSE is widely used for rapid assessment of cognitive function, while the Clinical Dementia Rating–Sum of Boxes (CDR-SB) provides a more detailed evaluation of both cognitive and functional status. When used together with the Activities of Daily Living (ADL) scale, these tools offer a comprehensive assessment of disease progression.14,15
Despite mounting evidence, data regarding the effects of anticoagulation on specific cognitive, functional, and clinical outcomes—including MMSE, ADL, CDR-SB, hospital readmissions, major adverse cardiovascular events, bleeding complications, and mortality—are still limited in patients with both AF and dementia. To address these gaps, this study evaluated the impact of anticoagulation on cognitive, functional, and clinical outcomes in patients with both AF and dementia. We hypothesized that anticoagulation use in AF patients with dementia is associated with slower cognitive and functional decline and improved clinical outcomes.
Methods
Study design and population
This retrospective cohort study included patients aged ≥65 years with diagnosed non-valvular AF and a concurrent diagnosis of dementia. Dementia was classified into the following subtypes: AD, vascular dementia (VaD), mixed dementia, and other forms. Other forms included unknown reason, frontotemporal dementia, Lewy Body disease, Parkinson disease dementia, and mild cognitive impairment, by registered neurologists, psychiatrist or geriatrists following the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5, at the same time, according to the hospital health information system recording. Based on CDR-SB baseline scoring, we divided all the patients into three severity subgroups, 0.5∼4.0: very mild dementia, 4.5∼9.0: mild dementia, 9.5∼18.0: moderate to severe dementia. 16
The study was conducted at a tertiary care center between January 2020 and December 2024. Institutional Review Board approval was obtained (IRB-0066/MEC/N/2024). Eligible patients underwent baseline cognitive and functional assessments, followed by repeat assessments at approximately 12-month intervals.
Exclusion criteria included: Anticoagulation use for <6 months; Malignancy; History of open-heart surgery; Primary psychiatric disorder; Severe functional impairment with the inability to communicate verbally.
Anticoagulation treatment and subgroups
Patients were divided into two groups based on their anticoagulation status: those receiving anticoagulation (either DOACs or warfarin) and those not receiving anticoagulation. Anticoagulant dosing was determined in accordance with the American Heart Association and European Society of Cardiology guidelines for atrial fibrillation.17,18 The study also examined the interaction and relationship between dementia subtypes and the use of DOACs. In addition, clinical parameters, including medical history and background data, were obtained for all patients.
Data collection and outcome measures
Primary endpoints: cognitive and functional change
Cognitive and functional status were assessed using the MMSE, ADL, and the CDR-SB at baseline and at approximately 12-months intervals following the initiation of anticoagulation therapy. Standardized tools included: MMSE, ADL, CDR-SB.
Changes in cognitive and functional status were quantified as delta scores: ΔMMSE (change in MMSE), ΔADL (change in ADL), and ΔCDR-SB (change in CDR-SB), with a lower ΔMMSE, ΔADL and higher ΔCDR-SB indicating greater decline in each measure.
ΔMMSE = MMSE (follow-up) – MMSE (baseline)
ΔADL = ADL (follow-up) – ADL (baseline)
ΔCDR-SB = CDR-SB (follow-up) − CDR-SB (baseline)
Secondary endpoints
We assessed clinical outcomes over a maximum period of 65 months. We assessed survival analysis using Kaplan-Meier survival curves and presented the following clinical events with hazard ratios (HR): 1. All-cause Hospitalization; 2. All-cause mortality; 3. Major adverse cardiovascular events (MACE); 4. Major bleeding events, defined by the International Society on Thrombosis and Haemostasis (ISTH) criteria.
Statistical analysis
Continuous variables were expressed as means ± standard deviations or medians with interquartile ranges. Between-group comparisons for non-normally distributed variables were made using the Kruskal-Wallis test, while paired t-tests were used for normally distributed variables. Post-hoc analyses were performed using Mann-Whitney U tests or one-way ANOVA when appropriate. Categorical variables were analyzed using the Pearson chi-square test.
Longitudinal changes in cognitive and functional scores (MMSE, ADL, and CDR-SB) were evaluated using mixed-effects models to account for repeated measurements over time. Cox proportional hazards models were used to examine time-to-event outcomes. Multivariate models were adjusted for age and relevant clinical comorbidities, including hypertension, diabetes mellitus, congestive heart failure, cerebrovascular disease, coronary artery disease, peripheral artery disease, alcohol use and smoking status, when these variables met criteria for inclusion based on clinical relevance.
To address potential treatment selection bias, analyses within the dementia cohort were supplemented by propensity-score matching to balance baseline characteristics between anticoagulated and non-anticoagulated patients. A 1:1 nearest-neighbor matching algorithm without replacement was used, applying a caliper of 0.1 standard deviations. The variables included in the propensity-score model were age, hypertension, diabetes, congestive heart failure, prior stroke, coronary artery disease, peripheral artery disease, smoking status, and alcohol use. All statistical analyses were conducted using SPSS software, version 27.0.
Missing data, sensitivity analyses, and multiple comparisons
Missing data were <10% for all cognitive measures. Missingness was handled using mixed-model maximum likelihood estimation. Sensitivity analyses excluding patients lost to follow-up produced similar results. A Bonferroni correction was applied for multiple secondary outcomes.
Power considerations
Although formal a priori power calculation was limited by the retrospective design, post hoc estimation indicated approximately 88% power to detect medium effect sizes in ΔMMSE, ΔADL and ΔCDR-SB between groups at α = 0.05.
Results
Patient baseline characteristics
As demonstrated in Figure 1, we screened consecutive patients who visited our memory clinic between January 2020 through December 2024, we initially enrolled 3373 dementia patients. After exclusion criteria, a total of 291 patients with concurrent diagnoses of AF and dementia, free of major psychiatric illness, were included in the final analysis. The median follow-up duration was 28 months. Of these, 208 (71.5%) were on anticoagulation therapy, while 83 (28.5%) were not. As shown in Table 1, the mean age of patients was 83.5 ± 7.5 years. Anticoagulated patients were younger (82.8 ± 6.8 years) compared to non-anticoagulated patients (85.1 ± 8.7 years, p < 0.01). Other baseline characteristics, including gender distribution and the prevalence of cardiovascular risk factors (hypertension, diabetes, dyslipidemia, heart failure, coronary artery disease, and stroke history), CHA2DS2VASc score were similar between the two groups. Baseline CDR-SB severity subgroups were no significant different between with and without anticoagulants. After propensity score matching, there is no significant difference between all of baseline characteristics.

Patient enrollment and selection algorithm. Flowchart illustrating the inclusion and exclusion criteria used to identify the final study cohort of patients with atrial fibrillation and dementia.
Baseline clinical characteristics of all the patients.

Data are presented as mean ± SD, number (%).
CDR-SB: Clinical Dementia Rating Scale-Sum of Boxes. Dementia severity: very mild (0.5–4.0), mild (4.5–9.0), moderate to severe (9.5–18.0).
Significant relationships (p < 0.05) are marked with *.
Cognitive and functional decline
Table 2 and Figure 2 show that patients receiving anticoagulation exhibited significantly less cognitive and functional decline compared to those who were not on anticoagulation. Specifically, the decline in MMSE (ΔMMSE) was milder and slower in the anticoagulated group (−2.2 ± 4.3) compared to the non-anticoagulated group (−4.2 ± 5.2; p = 0.048). Similarly, ADL scores declined less in the anticoagulated group (ΔADL: −7.2 ± 18.0) compared to the non-anticoagulated group (ΔADL: −18.1 ± 30.0; p = 0.02). The progression of CDR-SB (ΔCDR-SB) was also significantly slower in anticoagulated patients (1.3 ± 2.3) compared to non-anticoagulated patients (2.7 ± 3.3; p < 0.01). These associations remained significant after propensity-score matching.
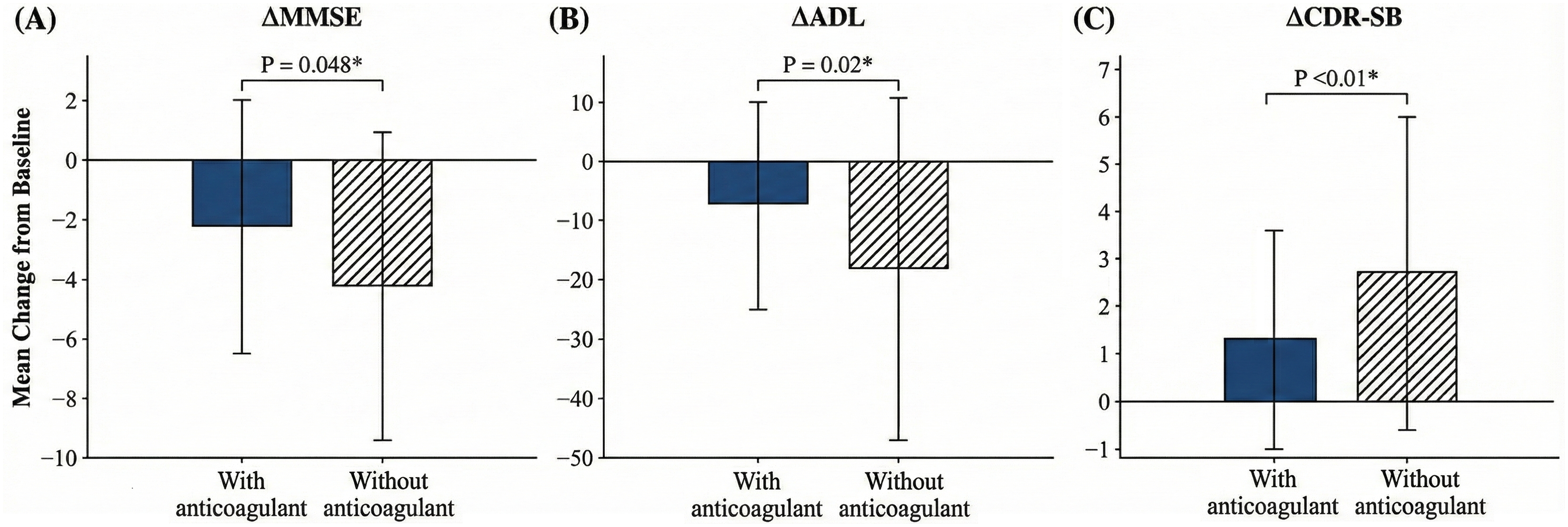
Comparison of ΔMMSE, ΔADL, and ΔCDR-SB between patients with and without anticoagulation.
Comparison of ΔMMSE, ΔADL, and ΔCDR-SB between patients with and without anticoagulation.

Data are presented as mean ± SD.
MMSE: Mini-Mental State Examination; ADL: Activities of Daily Living; CDR-SB: Clinical Dementia Rating Scale-Sum of Boxes.
Significant relationships (p < 0.05) are marked with *.
As demonstrated in Supplementary Table 1, The benefits of anticoagulation were most pronounced in subgroup patients with very mild baseline dementia (CDR-SB 0.5–4), where significant differences were observed in ΔMMSE (p < 0.01), ΔADL (p = 0.04), and ΔCDR-SB (p < 0.01). In subgroup analyses by dementia subtype, AD patients showed the most substantial benefit from anticoagulation, with significant preservation of cognitive function (ΔMMSE) (p = 0.02), functional status (ΔADL) (p = 0.03), and stabilization of CDR-SB (ΔCDR-SB) (p < 0.01). No statistically significant benefit was found in patients with VaD, mixed, or other forms of dementia. Regarding different types of DOACs, only apixaban consistently was associated with significantly slower cognitive and functional decline, including ΔMMSE (p = 0.04), ΔADL (p = 0.02) and ΔCDR-SB (p < 0.01). Subgroup analysis showed that patients on DOACs—specifically apixaban (p < 0.01), rivaroxaban (p = 0.01), and dabigatran (p < 0.01)—experienced significantly less CDR-SB progression (ΔCDR-SB) compared to those not on anticoagulation therapy. Warfarin did not show the same benefit (p = 0.09). Additionally, no significant differences in ΔMMSE, ΔADL, ΔCDR-SB were observed among warfarin, apixaban, rivaroxaban and dabigatran (p = 0.87, p = 0.92, p = 0.88).
Clinical outcomes
Anticoagulation therapy was associated with significantly improved clinical outcomes. As illustrated in Figure 3A, patients receiving anticoagulation demonstrated better overall survival, as shown by the Kaplan–Meier survival analysis (log-rank p < 0.01). Crude and adjusted event rates for all-cause hospitalization and all-cause mortality are summarized in Figure 4, while outcomes for MACE and major bleeding are presented in Supplemental Table 2.

(A) Kaplan–Meier survival analysis comparing survival rates between anticoagulated and non-anticoagulated patients. (B) Multivariate Cox proportional hazards analysis of hospitalization risk in anticoagulated versus non-anticoagulated patients. (C) Multivariate Cox proportional hazards analysis of all-cause mortality between anticoagulated and non-anticoagulated patients.

Cox proportional hazards for the effect of study variables on all-cause mortality and hospitalization.
In multivariate Cox proportional hazards analysis (Figures 3B and 4), anticoagulation use was independently associated with a reduced risk of hospitalization (hazard ratio [HR] = 0.60, 95% confidence interval [CI]: 0.43–0.84; p < 0.01). Furthermore, measures of cognitive and functional decline were also significant predictors of hospitalization risk. Specifically, smaller declines in ΔADL and slower progression in ΔCDR-SB were independently associated with lower hospitalization rates. For each one-point preservation in ADL, the risk of hospitalization decreased (HR = 0.99, 95% CI: 0.98–0.99; p < 0.01). Conversely, each one-point increase in CDR-SB was associated with a higher hospitalization risk (HR = 1.08, 95% CI: 1.01–1.15; p = 0.03).
As shown in Figures 3C and 4, all-cause mortality demonstrated significant reduction in the anticoagulated group (HR = 0.59, 95% CI: 0.40–0.88, p = 0.01). There were no significant differences between the anticoagulation groups in terms of MACE (HR =0.70, 95% CI: 0.37–1.32, p = 0.27) or major bleeding events (HR =1.11, 95% CI: 0.40–3.08, p = 0.85), as presented in Supplemental Table 2. Subgroup analyses for all-cause mortality and hospitalization are presented in Supplemental Figure 1.
In Table 3 and Figure 5, the results of the multivariate Cox regression analysis revealed that greater decline in ADL (ΔADL ≤ −5) and worsening CDR-SB (ΔCDR-SB ≥ 1) were independent predictors of higher hospitalization risk (HR for ΔADL = 1.96, 95% CI: 1.31–2.91, p < 0.01; HR for ΔCDR-SB = 1.60, 95% CI: 1.09–2.35, p = 0.02), especially in patients with very mild dementia at baseline, where the hazard ratios were even higher (HR for ΔADL = 3.53, 95% CI: 1.41–8.82, p < 0.01; HR for ΔCDR-SB = 4.32, 95% CI: 1.79–10.44, p < 0.01).

(A) Multivariate Cox proportional hazards analysis of hospitalization risk associated with significant functional decline (ΔADL ≤ −5). (B) Multivariate Cox proportional hazards analysis of hospitalization risk associated with worsening cognitive and functional progression (ΔCDR-SB ≥ 1).
Age and clinical comorbidities adjusted cox proportional hazards analysis evaluating the association between cognitive and functional decline (ΔADL≤-5, and ΔCDR-SB≥1) and risk of hospitalization.

ADL: Activities of Daily Living; CDR-SB: Clinical Dementia Rating Scale-Sum of Boxes; Dementia severity: very mild (0.5–4.0), mild (4.5–9.0), moderate to severe (9.5–18.0); AD: Alzheimer's disease; VaD: vascular dementia, Mixed: Alzheimer's disease mixed with vascular dementia; others: unknown reason, frontotemporal dementia, Lewy Body disease, Parkinson disease dementia, and mild cognitive impairment; CI: confidence interval; HR: hazard ratio.
Significant relationships (p < 0.05) are marked with *.
Discussion
This retrospective cohort study provides real-world evidence that anticoagulation in patients with both AF and dementia is associated with a slower progression of cognitive and functional decline, as assessed by MMSE, ADL, and CDR-SB scores. These benefits translated into reduced all-cause hospitalization and all-cause mortality. The effects were particularly pronounced in patients with very mild dementia and those diagnosed with AD, suggesting that early intervention in the cognitive disease process may yield the greatest benefits.
Although the between-group differences in ΔMMSE (≈2 points, −2.2 versus −4.2), ΔADL (≈10 points, −7.2 versus −18.1), and ΔCDR-SB (≈1.5 points, 1.3 versus 2.7) reached statistical significance, these numerical changes may not necessarily represent major clinical deterioration within a single year. However, in the context of a progressive neurodegenerative condition, even modest declines can accumulate and contribute to loss of independence, increased hospitalization risk, and transition to institutional care. Importantly, our multivariate analysis demonstrated that worsening ADL (ΔADL ≈-5 points) and CDR-SB (ΔCDR-SB ≈1 point) were independently associated with higher hospitalization rates, supporting the clinical relevance of these measures. Nonetheless, because this is an observational study, our findings reflect associations rather than causal relationships, and should be interpreted with appropriate caution.
The neuroprotective role of anticoagulation in AF has been previously hypothesized, with proposed mechanisms including the prevention of silent cerebral infarctions, maintenance of cerebral perfusion, and reduction in microembolic burden.3,19 Our findings extend this hypothesis by demonstrating that these benefits may vary by dementia subtype. Patients with AD showed the most significant benefit from anticoagulation, while those with VaD or mixed dementia did not demonstrate statistically meaningful improvements. This may be due to the multifactorial pathology of VaD, characterized by extensive cerebrovascular damage and impaired autoregulation, which may limit the efficacy of anticoagulation in altering disease progression. In contrast, microvascular dysfunction in early AD plays a contributory, but not dominant role, offering a therapeutic window for intervention.1,20 Moreover, the association between coagulation factors and cognitive decline further supports the hypothesis of a procoagulant state in AD. 20 Given that AD is the most prevalent form of dementia globally, this observation holds substantial clinical relevance. 21
Our analysis suggests that anticoagulation is most effective when initiated early in the dementia course, potentially by reducing the burden of silent cerebral infarcts and improving cerebral perfusion, both of which are known to contribute to cognitive decline in AF patients. These results align with large-scale studies that have reported that early initiation of oral anticoagulants in patients with AF may help preserve cognitive function.6,22 Nevertheless, causal inference cannot be drawn due to the observational nature of our study, and improvements may partly reflect baseline differences in frailty, vascular burden, or clinician prescribing patterns.
The subgroup of patients using apixaban showed a significantly slower decline in MMSE, ADL, and CDR-SB scores. In contrast, no significant differences in MMSE or ADL decline were observed in the dabigatran, rivaroxaban, and warfarin groups. This difference may be related to the higher frequency of apixaban use in our study, with most patients receiving a reduced dose. Apixaban might also offer the most favorable risk-benefit profile among DOACs for older adults, including those with typical geriatric conditions. 23 Otherwise, our subgroup analysis by anticoagulant type indicates that DOACs—especially apixaban and dabigatran, followed by rivaroxaban—were associated with significantly slower progression in CDR-SB scores (p-values: apixaban <0.01, dabigatran <0.01, rivaroxaban = 0.01). In contrast, the warfarin group did not reach statistical significance (p = 0.09). These findings are consistent with prior studies suggesting that DOACs have more predictable pharmacokinetics, fewer drug and dietary interactions, and a better safety profile than warfarin.8,24 However, because between-agent differences were not statistically significant in direct comparison, these findings should be interpreted cautiously and may partly reflect confounding by indication.
Our results also compare favorably with prior randomized trials. The CAF and GIRAF trials did not demonstrate significant cognitive differences between dabigatran and warfarin over two years. However, those trials enrolled cognitively intact individuals, and the short follow-up duration may have limited their ability to detect meaningful change.9,25 Our study, which included patients with established dementia and longer follow-up, may offer a more clinically relevant assessment of anticoagulation's impact in this population. Additionally, findings from the CardioCHUVI-FA registry in Spain reported significant differences in embolic and bleeding outcomes, but not in all-cause mortality, in an older population (age ≥85 years). 12 Our cohort, with a younger mean age of 83, showed the most benefit among patients with very mild AD, suggesting that age, dementia subtype and stage may significantly influence the therapeutic response to anticoagulation.
Conversely, other real-world data suggest that in patients with advanced dementia, anticoagulation may increase the risk of serious bleeding while providing only modest reduction in mortality. 26 These findings reinforce the concept that progressive neurodegeneration may outweigh any vascular benefits in later disease stages. Collectively, variations in baseline characteristics, dementia severity, anticoagulant selection, and follow-up duration across studies may account for the observed differences in outcomes.
In this study, anticoagulation use, functional and cognitive status emerged as strong predictors of hospitalization. Greater deterioration in ADL and CDR-SB scores was independently associated with higher rates of hospital readmission. Additionally, anticoagulation was linked to increased survival rates, as demonstrated by the Kaplan-Meier survival curve. These findings underscore the critical importance of maintaining functional and cognitive independence, not only for preserving quality of life but also for reducing healthcare resource utilization. Anticoagulation may play a role in this by stabilizing function and delaying the need for institutional care, which carries significant implications for both caregivers and public health system.27,28 Importantly, the observed cognitive and functional benefits from anticoagulation appeared to be independent of major bleeding complications, further supporting the safety of anticoagulation in dementia patients when appropriately monitored.
The decision to initiate anticoagulation in patients with dementia is inherently complex, requiring a balance between bleeding risk, life expectancy, and quality of life. 26 Our findings suggest that in carefully selected individuals, particularly those with mild AD and relatively preserved cognitive function, anticoagulation may offer benefits beyond stroke prevention. These include stabilization of cognitive, functional decline, reduced all-cause mortality and reduced hospital admissions, without a proportional increase in adverse events. For certain dementia patients with AF and borderline ischemic stroke risk (CHA2DS2-VASc score of 1 for men or 2 for women), or for those with subclinical AF, earlier and more aggressive initiation of anticoagulation may be justified to achieve better clinical outcomes and preserve cognitive function. These results further support the potential role of anticoagulation as a disease-modifying strategy in this high-risk population.
Despite these strengths, confounding by indication and reverse causation must be acknowledged. Clinicians may preferentially prescribe anticoagulation to younger, healthier, or more functionally independent patients, which could exaggerate the apparent benefit. Conversely, patients who deteriorated more rapidly may have been withheld anticoagulation due to frailty or bleeding concerns. Although we adjusted for age, multiple comorbidities, residual confounding likely persists.
Limitation
External validity is an important limitation. Our single-center design and relatively homogenous population may not fully represent broader clinical settings and limits the generalizability of the findings. This study is limited by its retrospective design, the modest sample size introduces potential sources of bias, potential for residual confounding, and lack of standardized longitudinal imaging or biomarker data to elucidate mechanisms. The duration of follow-up, although sufficient to detect cognitive trends, may not fully capture long-term effects on dementia progression or mortality. Furthermore, adherence to anticoagulation, time-in-therapeutic range (for warfarin), and potential drug-drug interactions were not evaluated in detail.
Future directions
Future research should include prospective, multicenter studies and randomized controlled trials with standardized cognitive assessments, neuroimaging, adjudicated clinical outcomes, and detailed medication adherence data. Studies focusing on early AD, mild cognitive impairment, or subclinical AF may clarify the optimal timing of anticoagulation to maximize cognitive benefit.
Conclusion
Anticoagulation in patients with AF and dementia, especially those with very mild AD, has been associated with reduced cognitive and functional decline and lower hospitalization rates. Early initiation of anticoagulation in cognitively vulnerable patients with AF may improve clinical outcome, suggesting that anticoagulation may serve a potential disease-modifying role in dementia. Further randomized controlled trials are needed to confirm these findings and to optimize anticoagulation strategies in this high-risk population.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261433532 - Supplemental material for Impact of anticoagulation on cognitive decline and clinical outcomes in patients with atrial fibrillation and dementia: A retrospective cohort study
Supplemental material, sj-docx-1-alr-10.1177_25424823261433532 for Impact of anticoagulation on cognitive decline and clinical outcomes in patients with atrial fibrillation and dementia: A retrospective cohort study by Yun Du, Weng-Chio Tam, Man-Fong Chu, Sio-Mui Wong, Kuok-Wun Lam, Tat-Kuong Tong, Mei-Hong Wong, Chon-Hou Chan, Weng-Hong Pun, Mario Evora, U-Po Lam and Iek-Long Lo in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors thank Macau cardiology association, Association of diagnosis and therapeutic intervention of Macau.
Ethical considerations
This study was approved by the Medical Ethical Committee of Centro Hospitalar Conde de São Januário Hospital(0066/MEC/N/2024).
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used in the study are available upon reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.