
Abstract
Background
The impact of dietary macronutrient composition on cognitive aging and Alzheimer's disease risk remains inadequately characterized.
Objective
To investigate the associations of carbohydrate, protein, and fat energy ratios with cognitive function and all-cause mortality among older adults in this binational study.
Methods
We analyzed data from the National Health and Nutrition Examination Survey (NHANES, 2011–2014; N = 2510) and the China Health and Nutrition Survey (CHNS, 1997–2006; N = 1600). Cognitive function was assessed using standardized composite z-scores. Associations were evaluated using weighted logistic regression (NHANES) and linear mixed-effects models (CHNS), with restricted cubic splines to examine nonlinearity. Cox models assessed mortality risk in NHANES.
Results
A higher carbohydrate ratio (CRC) exhibited a nonlinear inverse U-shaped association with the risk of cognitive impairment, with a significant threshold effect observed at approximately 48.5% of total energy intake. Moderate protein intake (PRC = 0.125–0.153, representing approximately 15% of energy from protein) was associated with the lowest risk of cognitive impairment in both cohorts. The fat ratio (FRC) demonstrated a complex nonlinear association, with cognitive risk increasing significantly when FRC fell below 33.2%. Lower CRC was associated with reduced all-cause mortality in the U.S. cohort (HRs for the lower quartiles: 0.68–0.72).
Conclusions
Modifiable macronutrient ratios are significantly associated with cognitive health and survival in older adults, with consistent findings across U.S. and Chinese populations. These results support dietary strategies that emphasize moderate carbohydrate intake (below approximately 48.5% of total energy) and balanced protein consumption (approximately 15% of energy) to promote cognitive health.
Keywords
Introduction
Cognition involves key brain functions such as memory, attention, numerical processing, reasoning, executive control, and perception, all of which support the planning, execution, and regulation of daily tasks. 1 Throughout life, cognitive ability generally remains stable during adulthood but begins to decline after the age of 60. 2 With a growing aging population worldwide, age-related cognitive impairment has become increasingly prevalent. In 2019, about 57 million people were affected—a number projected to rise to 153 million by 2050. 3 Despite this significant impact on families and society, there are still no effective treatments that can substantially slow or reverse the progression of cognitive decline or dementia. 4
Recently, a body of nutritional epidemiological research has highlighted the critical role of diet, as a modifiable factor, in interventions aimed at reducing the risk of dementia.5,6 Current research has focused primarily on the impact of food combinations, specific foods, or their constituent nutrients on cognition. 7 However, few studies have examined the effects of the energy contributions of carbohydrates, proteins, and fats—major sources of energy—on cognitive function within the diet, and the conclusions drawn from existing research are inconsistent.8–10 Empirical research has revealed that both excessively low and high carbohydrate intake may exert deleterious effects on human cognitive function, and more importantly, this association is highly dependent on the type of carbohydrates: diets rich in refined or highly processed carbohydrates tend to exacerbate such adverse impacts, while whole grain carbohydrates, as high-quality carbohydrate sources, have been consistently confirmed to be beneficial for brain health and cognitive maintenance. 11 In recent years, the relationship between protein intake and cognitive function has garnered significant attention. Studies have indicated that a high intake of protein may contribute to improved cognitive function in elderly individuals, but there remains no consensus on the recommended levels of protein intake.12,13 Similarly, while preclinical animal studies link high-fat dietary patterns to elevated cognitive decline risk, human epidemiological evidence for this association remains inconsistent and inconclusive. Notably, dietary fats do not exert uniform effects on cognitive function: omega-3 polyunsaturated fatty acids, well-recognized for supporting lifelong cognitive health, highlight the critical role of fat subtype in modulating the fat intake-cognitive outcome relationship. 14 In summary, there is a current dearth of systematic research examining the impact of carbohydrate, protein, and lipid intake on cognitive function.
In summary, the primary objective of this study is to leverage longitudinal and cross-sectional data from both China and the United States for mutual validation, in order to elucidate the specific effects of macronutrient energy ratios—carbohydrates, protein, and fats—on cognitive function and to further clarify their impact on mortality rates. We hypothesize that there exist specific macronutrient energy ratio intervals associated with better cognitive health and lower mortality risk, particularly among older adults.
Methods
Study description and population
The National Health and Nutrition Examination Survey (NHANES) is a biennial cross-sectional survey based on the U.S. general population, designed to assess the overall health and nutritional status of American residents. This comprehensive database includes standardized demographic data, physical examination results, laboratory test indicators, detailed dietary intake information, and health-related survey responses. The survey adopts a multistage probability sampling design to ensure the national representativeness of the sample. For this study, we extracted data from two consecutive cycles of the NHANES (2011–2012 and 2013–2014), and only included participants aged 60 years and older. Participants with incomplete cognitive function assessment data, missing data for any of the macronutrients (carbohydrates, protein, and fat), or incomplete demographic information and chronic disease history records were excluded from the final analysis. The research protocol of this study was approved by the National Center for Health Statistics Research Ethics Review Board, and all included participants provided written informed consent.
The China Health and Nutrition Survey (CHNS) is a long-term prospective cohort study conducted in the general Chinese population, incorporating multiple cross-sectional surveys between 1989 and 2015. 15 This analysis utilized data from 1997 to 2006 to examine the association between macronutrient intake and cognitive performance, as this period provided comprehensive cognitive assessments. The year 1997 was designated as the baseline. The following exclusion criteria were applied to participants aged 55 years or older at baseline: (1) missing dietary data or extreme energy intake (<800 or >4000 kcal/day for men, <500 or >3500 kcal/day for women) to minimize reporting bias 16 ; (2) lack of follow-up data; (3) incomplete cognitive data; (4) missing covariate data at baseline; and (5) diagnosis of mental disorders or inability to cooperate. All participants provided written informed consent covering both baseline assessments and follow-up surveys. The study protocol received ethical approval from the Institutional Review Boards of the University of North Carolina at Chapel Hill and the China Center for Disease Control and Prevention.
Dietary data and assessment of the CRC, PRC, and FRC
For the NHANES data from 2011–2014, we extracted survey data and the first 24-h dietary recall information, which included total carbohydrate, protein, total fat and calorie intake. 17
In the CHNS, dietary intake was assessed using three consecutive 24-h dietary recalls at the individual level and a food inventory weighing method at the household level. 16 Daily energy and nutrient intakes were estimated based on the China Food Composition Database.
In this study, the ratios of carbohydrates to calories (CRC), proteins to calories (PRC), and fats to calories (FRC) were calculated on the basis of the energy yields of carbohydrates, proteins, and fats, respectively. The calculations were as follows: CRC = 4 × Total Carbohydrate Intake/Total Calorie, PRC = 4 × Protein Intake/Total Calorie, and FRC = 9 × Total Fat Intake/Total Calorie. Participants with missing data for CRC, PRC, or FRC were excluded to ensure the integrity and representativeness of the dataset. The participants were subsequently categorized into quartiles (Q1, Q2, Q3, and Q4) on the basis of the quartile results of the CRC, PRC, and FRC.
Assessment of cognitive functioning
In the NHANES, the Consortium to Establish a Registry for Alzheimer's Disease Word Learning Subtest (CERAD-WL) is used to evaluate an individual's ability for both gradual and rapid verbal learning. 18 The CERAD-WL consists of three consecutive learning trials and one delayed recall trial. The maximum score for the CERAD-WL is 40 points (the sum of the three trials, each worth 10 points, plus the delayed recall trial, worth 10 points). The animal fluency test (AFT) examines language category fluency, a component of executive function. Participants are asked to name as many animals as possible within one minute; each animal they name earns them one point. The digit symbol substitution test (DSST) is a comprehensive tool for assessing brain health and is used to evaluate short-term memory, sustained attention, processing speed, and visual scanning.18,19 The participants are required to match 133 numbers with corresponding symbols within two minutes. Each correct match earns one point.
To exclude imbalances in individual cognitive scores, this study uses a composite cognitive function score as the outcome variable, standardizing the results of the DSST, AFT, and CERAD-WL to obtain Z scores, with Z scores less than 1 indicating cognitive impairment. The Z score is calculated via the following formula: Z = (X − M)/σ, where XX is the raw score, MM is the population mean, and σσ is the population standard deviation. 20
Cognitive function in CHNS participants was assessed using the Telephone Interview for Cognitive Status-modified (TICS-m). This instrument comprises three components: immediate and delayed recall of a 10-word list (assessing memory; 20 points), backward counting from 20 (assessing attention/executive function; 2 points), and serial subtraction of 7 from 100 (assessing processing speed; 5 points). The total score ranges from 0 to 27, with higher scores indicating better cognitive function. A global composite Z-score was calculated from the total scores as previously described.
Covariates
This study utilized variables collected through a unified survey as covariates, including age, sex, race, education level, marital status, smoking status, alcohol consumption status, body mass index (BMI), stroke status, depressive symptoms, diabetes status and hypertension status, as risk factors affecting cognitive function on the basis of previous research.21–23 Additionally, the CHNS included the variable of urban or rural residence but did not incorporate depression due to the lack of a standardized assessment. BMI was also used as a categorical variable, with populations defined as normal weight, overweight, and obese at BMI < 25, 25–29.9, and ≥30 kg/m2, respectively.
Statistical analysis
For the NHANES dataset, participants were dichotomized into cognitive impairment and non-impairment groups based on a composite global cognitive Z-score below −1. For continuous variables across different stratification methods, means and standard deviations were calculated, and t tests were used to assess the significance of intergroup differences. For categorical variables, frequency distributions were computed, and chi-square tests were employed to evaluate the significance of intergroup differences. For the NHANES population, weighted logistic regression analysis was conducted to examine the associations and significance levels between CRC, PRC, FRC, and cognitive status. Additionally, restricted cubic spline (RCS) regression was employed to assess potential nonlinear relationships of CRC, PRC, and FRC with cognitive impairment. In contrast, linear mixed models with random intercepts and slopes were utilized in the CHNS cohort to evaluate longitudinal associations between macronutrient intake and cognitive decline. The result was measured via the correlation coefficient R, 95% confidence interval (CI), and p value. Three models were applied for detailed analysis: Model 1 was the unadjusted model; Model 2 was adjusted for age, sex, race, education level, and marital status; and Model 3 was further adjusted for age, sex, race, education level, marital status, BMI, alcohol history, smoking history and disease. We fitted a Cox proportional hazards model to assess the associations of CRC, PRC, and FRC with all-cause mortality outcomes after controlling for covariates. Cox regression analysis was conducted via two models: (1) Model 1, an unadjusted model; (2) Model 2, adjusted for age, sex, race, education level, marital status, BMI, alcohol history, smoking history, diabetes, hypertension, and stroke history. All analyses were conducted via SPSS or R version 4.3.1. A p value of less than 0.05 was considered significant.
Results
Baseline characteristics
We included 2510 and 1600 participants from the NHANES and CHNS databases, respectively, after excluding individuals with missing data on macronutrient intake, cognitive function, or baseline covariates. Figure 1 illustrates the process of data curation.

Data curation process.
Participants from NHANES were stratified into cognitive impairment (n = 1657; weighted age 71; 49.5% female) and non-impairment (n = 853; weighted age 66; 59.0% female) groups based on composite cognitive Z-scores. The groups exhibited a significant difference in global cognitive function (−1.04 ± 1.56 versus 2.84 ± 1.33). Covariates including sex, age, education, and comorbidities differed notably between groups. While only protein intake differed significantly in continuous form, all macronutrients (carbohydrate, protein, fat) showed significant differences when stratified by quartiles. Detailed results are presented in Table 1. Participants from the CHNS cohort were stratified into cognitive impairment (n = 759; mean age 61 ± 7 years; 61.4% female) and non-impairment (n = 841; mean age 62 ± 7 years; 44.2% female) groups based on the composite global cognitive Z-score. The groups exhibited a significant difference in global cognitive function (−0.76 ± 0.49 versus 0.87 ± 0.55, p < 0.001). Covariates including sex, education level, residential location, BMI, smoking history, and alcohol consumption status differed significantly between the two groups (all p < 0.05), whereas no statistically significant between-group differences were observed for age, diabetes, hypertension, or stroke history (all p > 0.05). All macronutrient ratios (CRC, PRC, and FRC) showed statistically significant differences between groups in continuous form (all p < 0.001), and also exhibited significant between-group differences when stratified by quartiles (all p < 0.05). Detailed results are presented in Supplemental Table 1.
Patient demographics and baseline characteristics.

Note: Unweighted: the actual number of study participants included in the analysis without applying sampling weights; Weighted: the population-representative sample size calculated by applying the complex sampling weights of the NHANES survey.
The associations between CRC, PRC, FPC, and cognitive impairment using data from the NHANES
Table 2 provides a detailed examination of the relationships among CRC, PRC, FRC, and cognitive impairment across the three models. With respect to the association between CRC and cognitive impairment, we observed a U-shaped non-linear inverse association, rather than a linear association between elevated CRC and increased risk of cognitive impairment.
The associations between CRC, PRC, FPC and cognitive impairment using data from the NHANES.

Note: Model 1 is a Nonadjusted model. Model 2 adjusted for: Age, Sex, Race, education level, Marital status. Model 3 adjusted for: Age, Sex, Race, education level, Marital status, BMI, Drink history, Smoke history, Hypercholesterolemia, Diabetes, Hypertension, Stroke.
Abbreviation: OR: odds ratio; CI: confidence interval.
Using the first quartile (Q1: 0–0.413) as the reference, Model 1 revealed that elevated CRC levels were associated with an increased risk of cognitive impairment in the third quartile (Q3: 0.485–0.553; OR = 1.55, 95% CI: 1.18–2.02, p = 0.003) and the fourth quartile (Q4: 0.553–1.000; OR = 1.64, 95% CI: 1.21–2.22, p = 0.002). However, after sequential adjustment for covariates, only the third quartile of CRC remained significantly associated with an increased risk of cognitive impairment: an OR of 1.39 (95% CI: 1.04–1.87, p = 0.028) in Model 2, and an OR of 1.46 (95% CI: 1.07–2.01, p = 0.021) in Model 3. No statistically significant association was observed for the fourth quartile of CRC in either of the two adjusted models (Model 2: OR = 1.26, 95% CI: 0.91–1.73, p = 0.161; Model 3: OR = 1.28, 95% CI: 0.90–1.83, p = 0.148).
These findings indicate that CRC exceeding 48.5% of total energy intake is associated with an increased risk of cognitive impairment, with the most pronounced risk observed between 48.5% and 55.3% of total energy intake, rather than a linear dose-response relationship where risk increases incrementally with rising CRC levels.
Regarding the associations of PRC and FRC with cognitive impairment, we observed distinct association patterns for the two macronutrients across the three analytical models, using the first quartile (Q1) as the reference category.
For PRC, Model 1 showed that higher PRC levels were associated with a reduced risk of cognitive impairment, with significant protective effects observed in the second quartile (Q2: 0.125–0.153; OR = 0.66, 95% CI: 0.53–0.84, p = 0.001) and the third quartile (Q3: 0.153–0.183; OR = 0.62, 95% CI: 0.44–0.86, p = 0.006). Following sequential adjustment for covariates, the protective effect remained statistically significant only in the second quartile of PRC, with an OR of 0.68 (95% CI: 0.50–0.92, p = 0.015) in Model 2 and an OR of 0.67 (95% CI: 0.48–0.93, p = 0.021) in Model 3. The third quartile of PRC exhibited a trend toward reduced risk of cognitive impairment in the adjusted models, although this did not reach statistical significance (Model 2: OR = 0.66, 95% CI: 0.43–1.02, p = 0.061; Model 3: OR = 0.64, 95% CI: 0.40–1.03, p = 0.065). In contrast, no significant association was observed for the fourth quartile (Q4: 0.183–1.000) in either of the two adjusted models. These findings indicate that moderate protein intake confers the most pronounced cognitive benefits, with no additional protective effect observed at higher intake levels.
For FRC, Model 1 revealed a significant protective association between higher fat intake and cognitive impairment in the fourth quartile (Q4: 0.401–1.000; OR = 0.67, 95% CI: 0.51–0.89, p = 0.007). In Model 3, this association exhibited a trend toward statistical significance (OR = 0.70, 95% CI: 0.49–1.00, p = 0.052), while no statistically significant association was observed for any quartile in Model 2.
This study further employed a RCS model with four knots to elucidate the associations between CRC, PRC, and FRC and cognitive impairment, as depicted in Figure 2. For CRC, the RCS curve revealed an inverse U-shaped nonlinear association with cognitive impairment risk. The log(OR) of cognitive impairment was approximately 0 (corresponding to OR≈1, no excess risk) when CRC was 0.5; the risk of cognitive impairment increased significantly as CRC rose from 0.485 to 0.553, while no further significant increase in risk was observed when CRC exceeded 0.553, which was fully consistent with the results of the adjusted logistic regression models.

RCS analysis between CRC, FRC, PRC, and cognitive impairment.
For FRC, the RCS curve showed a nonlinear association with cognitive impairment. The log(OR) of cognitive impairment was approximately 0 (OR ≈ 1) when FRC was 0.332; the risk of cognitive impairment increased significantly as FRC decreased below this threshold, while higher FRC above 0.332 was associated with a trend toward reduced cognitive impairment risk.
For PRC, the RCS curve demonstrated that the risk of cognitive impairment was lowest at a PRC level of approximately 0.151, with risk trending upward as PRC deviated from this optimal level. Consistent with the findings from the quartile regression analysis, only the reduction in cognitive risk within the moderate PRC range (0.125–0.153) reached statistical significance in the fully adjusted model. PRC levels above 0.183 showed no statistically significant increase in the risk of cognitive impairment, yet no additional protective benefits were observed relative to moderate intake levels.
The associations between CRC, PRC, FPC, and cognitive scores utilizing data from the CHNS
After adjustment for various covariates, analysis of the association between PRC and overall cognitive impairment revealed that higher PRC levels were associated with increased cognitive function scores. Using the first quartile (Q1: 0–0.086) as reference, the second (Q2: 0.086–0.115), third (Q3: 0.115–0.153), and fourth (Q4: 0.153–1.000) quartiles all showed statistically significant effects (p < 0.05; odds ratios: 0.094, 95% CI: 0.019–0.169; 0.092, 95% CI: 0.015–0.168; 0.133, 95% CI: 0.054–0.212) (Table 3). Furthermore, the fourth quartile of PRC was significantly associated with attention and processing speed scores (p < 0.05; OR: 0.057, 95% CI: 0.004–0.109; OR: 0.382, 95% CI: 0.176–0.588). All PRC quartiles were significantly associated with both immediate and delayed memory (p < 0.05; OR: 0.470, 95% CI: 0.084–0.857; OR: 0.401, 95% CI: 0.008–0.793; OR: 0.464, 95% CI: 0.057–0.871). In contrast, no significant associations were observed between CRC or FRC and attention, processing speed, immediate or delayed memory, or global cognitive scores (Table 3, Supplemental Tables 2–4).
A linear mixed-effects regression analysis of the associations between CRC, PRC, and FPC and global cognition utilizing data from the CHNS.
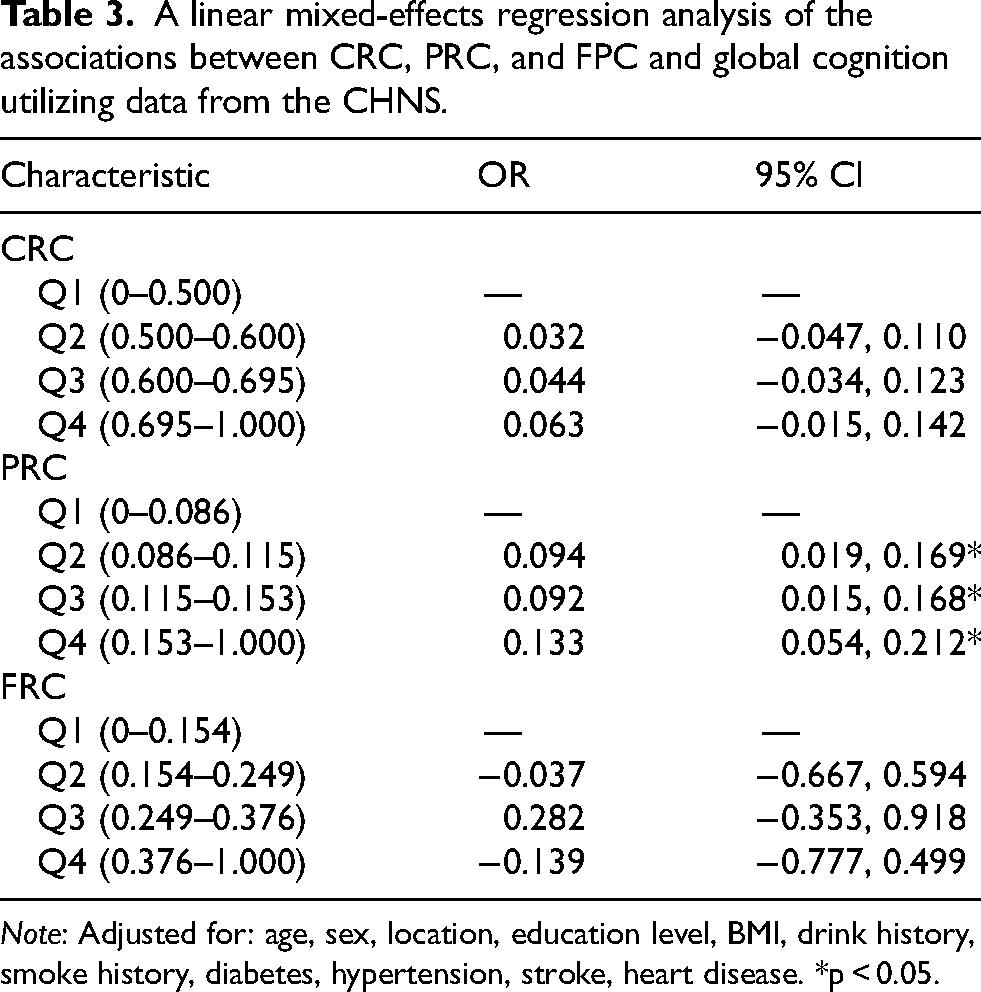
Note: Adjusted for: age, sex, location, education level, BMI, drink history, smoke history, diabetes, hypertension, stroke, heart disease. *p < 0.05.
The relationships among CRC, PRC, FRC, and all-cause mortality using data from the NHANES
During an average follow-up period of 48 months, a total of 477 participants died from various causes. Figure 3 displays the Kaplan–Meier curves for CRC, PRC, and FRC in relation to all-cause mortality, indicating that participants in the highest quartile (Q4) of CRC showed a significant difference in all-cause mortality (p = 0.049); participants in the FRC quartiles did not exhibit differences in either all-cause mortality (p = 0.953). There was no significant difference in all-cause mortality (p = 0.179) among participants in the PRC quartiles.

Kaplan–Meier curves of the survival rates for participants categorized by quartiles of CRC, FRC, and PRC.
Table 4 presents the results of Cox regression analysis, covering the associations between CRC, PRC, FRC and all-cause mortality. We constructed Cox proportional hazards models using the highest quartile (Q4) of each macronutrient ratio as the reference category, with findings consistent with those from the corresponding Kaplan–Meier (KM) curve analysis.
The relationships among CRC, PRC, FRC and all-cause mortality using data from the NHANES.
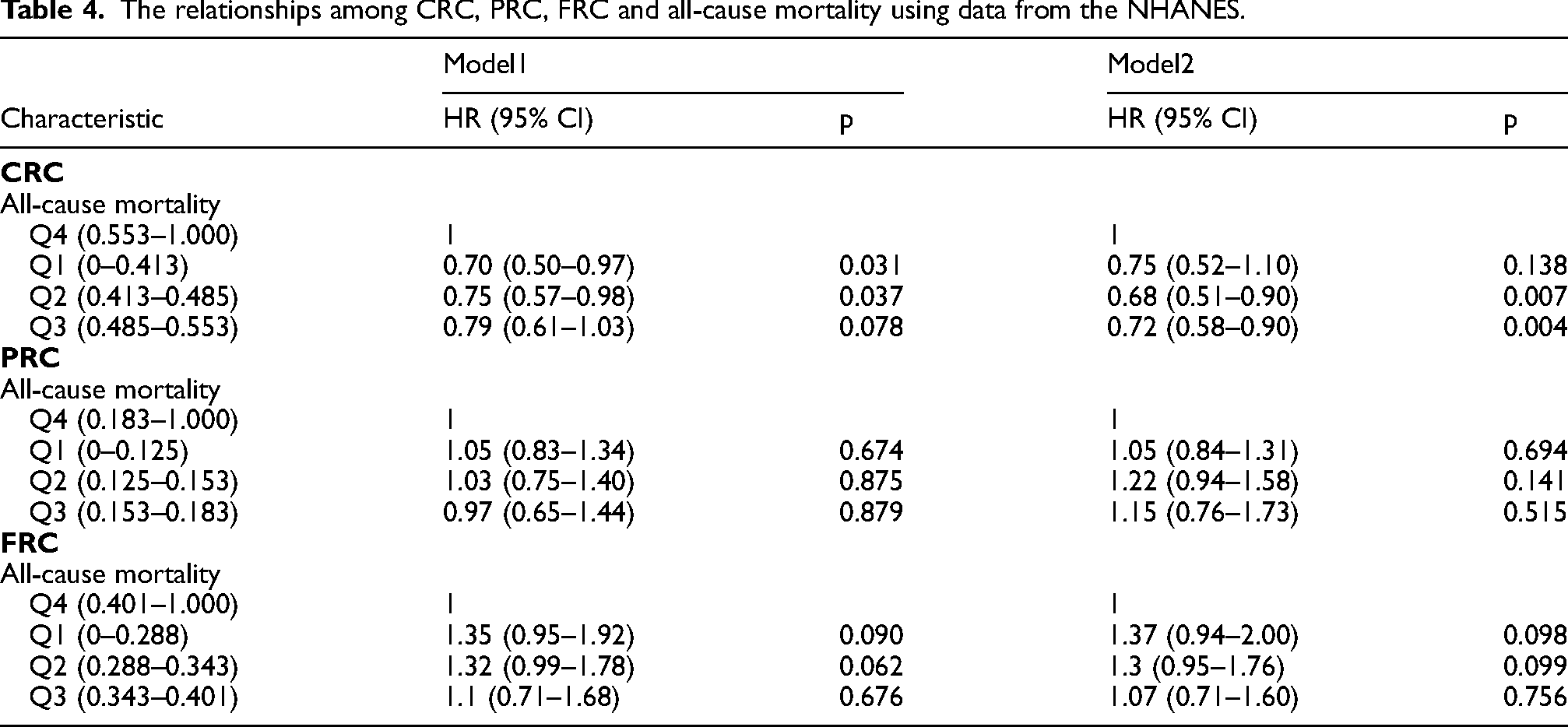
For CRC, Model 1 (unadjusted) showed that the first quartile (HR = 0.70, 95% CI: 0.50–0.97, p = 0.031) and the second quartile (HR = 0.75, 95% CI: 0.57–0.98, p = 0.037) were significantly associated with a reduced risk of all-cause mortality. After full adjustment for all confounding factors in Model 2, the second quartile (HR = 0.68, 95% CI: 0.51–0.90, p = 0.007) and the third quartile (HR = 0.72, 95% CI: 0.58–0.90, p = 0.004) of CRC remained significantly associated with a decreased risk of all-cause mortality.
For PRC, no statistically significant association with all-cause mortality was observed for any quartile in either Model 1 (unadjusted) or Model 2 (fully adjusted) (all p > 0.05), which was consistent with the non-significant difference between groups in the KM curve analysis (p = 0.179).
For FRC, no statistically significant association with all-cause mortality was found for any quartile in either of the two models (all p > 0.05), which was consistent with the non-significant difference between groups in the KM curve analysis (p = 0.953).
Sex-specific associations between macronutrient ratios and cognitive function
We further performed sex-stratified subgroup analyses in the NHANES cohort, as well as tests for interaction between sex and macronutrient energy ratios in the CHNS cohort (Supplemental Tables 5 and 6). In the NHANES cohort, no significant effect modification by sex was observed for the associations of CRC, PRC, and FRC with cognitive impairment (all p for interaction >0.05), with consistent overall trends between men and women. Specifically, elevated CRC was associated with an increased risk of cognitive impairment in both sexes, with statistical significance observed in the fourth quartile (Q4) among men (OR = 1.73, 95% CI 1.08–2.77, p = 0.023) and the third quartile (Q3) among women (OR = 1.81, 95% CI 1.19–2.77, p = 0.006). After sex stratification, no significant associations were detected for PRC across all quartiles in either men or women. Higher FRC exhibited cognitive protective effects in both sexes: a significant dose-dependent reduction in cognitive impairment risk was observed in Q3 and Q4 among men (OR = 0.66, p = 0.047; OR = 0.59, p = 0.015, respectively), while only Q4 reached statistical significance in women (OR = 0.56, 95% CI 0.39–0.82, p = 0.003).
In the prospective CHNS cohort, no significant interactions were found between sex and CRC or FRC (p = 0.601 and 0.485, respectively; all p > 0.05), which was consistent with the null findings for these two macronutrients in the overall population. Notably, the interaction between sex and PRC was of borderline significance (p = 0.051). No significant associations were detected in men, indicating that the longitudinal cognitive benefits associated with higher PRC were predominantly observed in women.
Discussion
In this binational study integrating cross-sectional data from the United States and longitudinal data from China, we elucidated the distinct relationships between dietary macronutrient energy ratios and cognitive health. Our primary findings indicate that a higher CRC is robustly associated with an increased risk of cognitive impairment, while a moderate PRC exerts a significant cognitive protective effect, with no additional benefits or statistically significant cognitive risks observed for higher PRC levels. These associations remained statistically significant after extensive adjustment for demographic, clinical, and lifestyle covariates. Furthermore, restricted cubic spline analyses confirmed non-linear dose-response relationships for all three macronutrients. Finally, survival analysis in the U.S. cohort revealed that lower CRC was associated with reduced all-cause mortality, underscoring the long-term health implications of dietary patterns.
Our finding that elevated CRC is detrimental to cognitive performance aligns with a growing body of evidence. Previous studies have linked high-carbohydrate dietary patterns to an increased risk of AD, particularly in high-risk groups such as elderly women and APOE ε4 allele carriers.24,25 A potential mechanism involves hyperglycemia and insulin resistance induced by excessive sugar intake, which can disrupt cerebral energy metabolism, promote neuroinflammation and oxidative stress, and ultimately accelerate neurodegeneration.26,27 The S-shaped curve derived from our RCS analysis suggests a potential threshold effect, where the risk of cognitive impairment becomes markedly significant once carbohydrate intake exceeds approximately 48.5% of total energy intake. Notably, our analysis focused on total CRC without distinguishing carbohydrate sources, and existing evidence confirms that added sugars and refined carbohydrates—rather than whole-grain carbohydrates—are the key drivers of poor cognitive outcomes; whole-grain carbohydrates have well-validated health benefits and are recommended in global dietary guidelines. Our results on total CRC thus highlight the importance of controlling overall carbohydrate intake, and the cognitive risks of high CRC are likely attributable to the overconsumption of refined carbohydrates in the study cohorts.28,29
A central and innovative finding of our study is that a moderate PRC exerts a significant cognitive protective effect, a pattern consistently observed across both the NHANES and CHNS datasets. We identified a specific “sweet spot” for protein intake (PRC ≈ 0.125–0.153, representing approximately 15% of energy from protein) associated with the lowest risk of cognitive impairment. This finding refines the existing literature, which often reports a more linear inverse association between protein intake and dementia risk.30,31 Our results indicate that insufficient protein intake is suboptimal for cognitive health, whereas higher intake above this optimal range confers no extra cognitive benefits and does not show a statistically significant increase in cognitive impairment risk. Accordingly, considering its benefits for sarcopenia and other age-related conditions, moderate increases in protein intake are feasible for older adults. 32 The underlying mechanisms are likely multifactorial, involving the role of protein in maintaining neuronal integrity, serving as precursors for neurotransmitters, and preserving muscle mass to support an active lifestyle.33,34 This consistent protective effect of moderate PRC across two ethnically and culturally distinct cohorts strengthens the validity of our findings and highlights the importance of adequate protein intake for cognitive health in older adults.
The relationship between the FRC and cognition was complex. Our RCS analysis suggested potential benefits of moderate-to-high FRC, which appears to contradict some studies linking high-fat diets to cognitive deficits. 35 This discrepancy is likely attributable to the critical distinction between fat types, which our analysis could not address. Previous research strongly implicates saturated fats in promoting cognitive decline, whereas unsaturated fats may be protective. 36 The inverse relationship we observed may therefore reflect the benefits of unsaturated fats prevalent in the studied diets. Consequently, our findings regarding FRC should be interpreted with caution, and future research must prioritize analyzing fat quality and sources to draw definitive conclusions.
Finally, our survival analysis extends the clinical relevance of macronutrient intake beyond cognitive health to overall survival. We found that lower CRC was associated with reduced all-cause mortality, aligning with some, though not all, previous studies.37,38 This divergence in the literature may stem from differences in population characteristics and definitions of low-carbohydrate diets. Our results, specific to the U.S. elderly population, suggest that a diet moderately lower in carbohydrates and balanced with adequate protein may be a viable strategy for promoting both cognitive health and longevity.
Sex-stratified subgroup and interaction analyses across the binational U.S.-China cohorts further validated the robustness of the core associations between dietary macronutrients and cognitive health in older adults, while uncovering potential sex-specific characteristics. Overall, sex did not exert a significant modifying effect on the associations of carbohydrate and fat energy ratios with cognitive function, indicating that the cognitive impairment risk of high carbohydrate intake and the potential cognitive protective effect of higher fat intake are consistently present in both older men and women.
The most notable finding of this study is the potential sex difference in the association between protein energy ratio and cognitive function. The interaction between sex and protein energy ratio approached statistical significance in the CHNS cohort, suggesting that the cognitive protective effect of protein may be concentrated in women. This result is supported by plausible biological mechanisms: On one hand, postmenopausal women experience a sharp decline in estrogen levels—a key hormone for maintaining cerebral neurogenesis and counteracting neuroinflammation—whereas adequate protein intake can provide amino acid precursors for neurotransmitters and improve insulin sensitivity; in contrast, men exhibit a more gradual decline in sex hormone levels. 39 On the other hand, women accounted for 61.4% of the cognitive impairment group in the CHNS cohort, and inadequate protein intake is more prevalent among older Chinese women, making the cognitive benefits of protein supplementation more readily observable.
This study has several limitations that warrant consideration. First, the primary analysis of the NHANES data is cross-sectional, precluding causal inference. However, the incorporation of longitudinal data from the CHNS partially mitigates this limitation and strengthens the observed associations. Second, dietary data were self-reported and subject to recall bias. Third, and most critically, our analysis did not differentiate between the quality and sources of macronutrients: we did not stratify carbohydrates by refined/added sugar versus whole-grain sources, fats by saturated/unsaturated subtypes, or proteins by dietary source (e.g., animal versus plant-based). Existing evidence confirms that macronutrient quality is a pivotal factor influencing cognitive and overall health outcomes, and this is a key limitation of our study. Future research should employ prospective cohort designs with repeated dietary assessments and focus on elucidating the effects of macronutrient quality and food sources on cognitive aging and dementia risk across diverse populations.
Conclusion
This multinational study demonstrates that specific, modifiable dietary macronutrient distributions are significantly associated with cognitive function and overall survival in older adults. It identifies a nonlinear optimal range for protein intake and a distinct risk threshold for carbohydrate consumption. These findings support the development of targeted nutritional guidelines and public health strategies advocating for moderate carbohydrate intake and balanced protein consumption to promote cognitive health and longevity. Future research should prioritize prospective study designs and investigate the impact of macronutrient quality to further refine these key recommendations.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261445034 - Supplemental material for Macronutrient energy ratios and cognitive health in older adults: A binational study of nonlinear associations and mortality links
Supplemental material, sj-docx-1-alr-10.1177_25424823261445034 for Macronutrient energy ratios and cognitive health in older adults: A binational study of nonlinear associations and mortality links by Jinbiao Li, Xinkai Zhang, Yu Hu, Yamei Tang, Songhua Xiao and Yongteng Xu in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
The NHANES study protocol was approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board, and the CHNS protocol received ethical clearance from the Institutional Review Boards of the University of North Carolina at Chapel Hill and the Chinese Center for Disease Control and Prevention. All enrolled participants submitted written informed consent before formal data acquisition.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contributions
Please replace this text with the Manuscript Author Contributions sent in the Manuscript metadata/information from Sage Track.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Natural Science Foundation of China (81925031, 81820108026, 82330099), a grant from the Guangzhou Science and Technology Program (202007030001) to Yamei Tang, and grants from the National Natural Science Foundation of China (82304067) and the China Postdoctoral Science Foundation (2020TQ0374, 2020M683095).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.