
Abstract
Background
Alzheimer's disease (AD) and related dementias (ADRD) are a rapidly growing cause of morbidity and mortality in the United States, yet little is known about how these conditions are understood within American Indian (AI) communities. Limited alignment between biomedical models and community conceptualizations may hinder culturally appropriate care and research engagement.
Objective
This study aimed to explore how aging and dementia are conceptualized among older adults in a Pueblo community, with the goal of informing culturally congruent dementia care, education, and research practices.
Methods
In partnership with a local health and wellness center and tribal government, semi-structured interviews and questionnaires were administered to 32 older AI adults in a Pueblo community in New Mexico. Data were analyzed using thematic qualitative methods to identify perspectives on aging and dementia.
Results
Dementia was described as memory loss, diminished independence, or altered sense of self. Explanations of causation extended beyond biomedical models to encompass lifestyle, psychological, historical, and environmental factors.
Conclusions
Findings underscore the importance of understanding community-specific distinctions between “normal” and “abnormal” aging. Culturally grounded approaches that build trust, reduce uncertainty, and support open dialogue are essential for developing meaningful dementia education, assessment, and care that are community-driven and culturally responsive.
Keywords
Introduction
Alzheimer's disease (AD) and Alzheimer's disease–related dementias (ADRD) are progressive neurodegenerative conditions that undermine functional abilities and independence in older adults. They represent a major public health challenge, affecting not only those diagnosed but also their families and communities. American Indian (AI) peoples face disproportionate health risks, including heightened vulnerability to AD/ADRD. 1 Chronic stress driven by such social inequality, and the unequal social and physical environments it creates, may directly increase dementia risk among marginalized groups like AI peoples. 2 These longstanding inequities also contribute to higher rates of chronic conditions, such as cardiovascular disease and diabetes, which further elevate dementia risk. Therefore, as the AI population in the United States continues to age, concerns about dementia are increasing—this underscores the urgent need for research that captures cultural perspectives on dementia to support effective clinical communication and recommendations.
There are 574 federally recognized American Indian and Alaska Native (AI/AN) tribes which come from diverse regions and have distinct cultural traditions and lifestyles. 3 Despite each tribes’ uniqueness, there is a shared historical legacy of colonialism and contemporary discrimination. These shared histories of trauma, continued discrimination, and ongoing barriers to healthcare have contributed to significant health disparities, including an increased AD/ADRD burden for AI peoples.4–5 Pueblo peoples are Indigenous communities of the United States Southwest, particularly in present-day New Mexico, whose histories are deeply shaped by centuries of Spanish and later United States colonialism, including missionization, land dispossession, and policies of cultural suppression. Despite these disruptions, Pueblo communities have maintained strong cultural continuity, including place-based lifeways, communal governance, and enduring traditions that continue to shape health beliefs, intergenerational relationships, and approaches to wellness and aging today.
Research with AI elders emphasizes that wellness and aging are understood holistically, encompassing balance among physical, mental, emotional, and spiritual domains, and deeply rooted in social and familial relationships. 6 Elders often describe wellness as “being in balance” and highlight agency, independence, and the ability to contribute meaningfully to one's community as key to health and well-being. When illness or cognitive decline threatens that balance or autonomy, it can profoundly affect elders’ sense of wellness and identity. 7
Structural barriers, such as the limited availability of specialized dementia services in rural regions, chronic underfunding of the Indian Health Service (IHS), and high turnover among healthcare providers, are particularly challenging for older adults experiencing cognitive decline, who may struggle to navigate fragmented and resource-limited systems.8–9 At the policy level, American Indian elders are often rendered “invisible” in federal, state, and tribal decision-making processes. 9 This invisibility, combined with inadequate data systems and inconsistent tribal consultation, limits advocacy and resource allocation for elder health services, including dementia care. Although Medicaid expansion under the Affordable Care Act (ACA) improved reimbursement and care access in some regions, gaps in implementation, bureaucratic barriers, and cultural incongruities persist. As a result, many elders continue to face structural obstacles to care continuity and experience mistrust toward medical systems. Furthermore, current models of care often fail to align with community health beliefs and communication practices and may offer recommendations that are impractical within specific cultural or geographic contexts, leading to frustration, reduced trust, and decreased engagement. Acknowledging these challenges is essential to fully understand community perspectives and to develop dementia care that is culturally responsive and sustainable.
Research documenting how AI peoples navigate their experiences of culture and biological meaning of illness can help medical practitioners understand healthcare seeking behaviors, potential responses to biomedical treatment, and care management plans. To date there is very little information on how to provide personalized clinical care, effective treatment planning, or lower AI peoples’ risk for developing AD/ADRD. Miscommunication between Western medical providers and AI communities is a substantial barrier in dementia diagnosis and care. It is well-established that culture influences individual and family understandings of illness, including causal theories, treatment options, emotional experiences, healthcare seeking behaviors, models of decision making, and care practices. 10 Many AI communities conceptualize declining cognitive abilities as a part of the normal aging process or as a result of sociocultural and lifestyle factors.11–12 These understandings are unique from the biological model adopted and used by Western medical teams and can contribute to misunderstandings between patient-providers. Some existing barriers to effective dementia care stem from these miscommunications: patients may be uncomfortable sharing their viewpoints and become discouraged if their worldviews and circumstances are not taken into consideration in a treatment plan. This discouragement may exacerbate the long-standing distrust present in medical systems and subsequently lower engagement in care and with follow up appointments. In addition to many of the existing logistical barriers (e.g., long wait times, cost, distance, unreliability) preventing adequate care for AI communities, culturally incongruent care can hinder effective communication and potentially worsen relationships between AI communities and the medical system. 13
Investigating cultural beliefs through collaboration with communities can help researchers and clinicians to build trust and can inform shared decision-making processes to promote effective disease prevention and treatment. Without this collaboration, it would not be possible to improve mechanisms for diagnosis and care and ultimately would be impossible to achieve health equity. 12
The current study aimed to evaluate perceived positives of aging, general dementia meaning, and theories of dementia causation in an Indigenous Pueblo community in rural Southwestern United States.
Methods
Participants and recruitment
A community-based cohort was recruited from a rural Pueblo community in the Southwestern United States. Approval for the study was received from the local tribal Government. The study was then approved by the University of New Mexico (UNM) Health Science Center Institutional Review Board (IRB) and the study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We partnered with the Pueblo's Health and Wellness Department and a community health worker (CHW), who aided with recruitment through flyering, community presentations, and word of mouth. CHW was a community member fluent in the local native language, who provided input in interview design, and was trained on cognitive screening measures and semi-structured interview procedures. Inclusion criteria were broad in order to facilitate a representative sample: participants were required to be between 50 and 95 years of age and identify as American Indian. Data were captured using pencil-and-paper, and were physically stored in Tribal Health and Wellness offices. The study team entered these data with REDCap electronic data capture tools, securely hosted at UNM.
Study activities
Participants were seen individually by the CHW to provide demographic information, completed questionnaires regarding cultural identity and social supports, and were administered brief cognitive screening measures. These cognitive screening measures were a part of the larger study and were not used for this study. A semi-structured interview assessing interest in AD biomarker testing disclosure was developed from a similar study and was expanded to also capture explanatory models of dementia, and community gaps in dementia care. 14 The interview revisions and validation were completed by experts in dementia and Pueblo community members: neurologists, a neuropsychologist, a speech-language pathologist, a communications expert, and the director of the Health and Wellness and Community Health Workers of the Pueblo Community. Study staff were fluent in the local native language and provided the option of conducting the assessment in their native language, but 100% of participants chose to complete the interview and assessment in English.
Qualitative data analysis
Inductive thematic analysis was employed as the best qualitative methodology for data analysis. Each interview was audio-recorded, transcribed, and entered into REDCap. A subset of transcripts (n = 5) was initially reviewed by multiple researchers (SR, TG, KE, NH), and categories and subthemes were identified through inductive coding, allowing themes to emerge from the data rather than being predetermined. A structured codebook was then developed, including detailed definitions and illustrative examples to ensure consistency across coders. The codebook was iteratively refined through team discussion, incorporating feedback and critique to enhance clarity and analytic rigor.
The analysis was guided by a reflexive, team-based thematic analysis process, with themes organized around three primary domains: (1) positive aspects of aging in the community; (2) understandings of dementia and age-related cognitive changes; and (3) causal beliefs about dementia onset. A multi-step coding process was conducted using NVivo12 (Lumivero, 2017). Two independent coders (KE, NH) read transcripts multiple times to ensure familiarity and systematically applied codes to the data.
To enhance reliability, coding consistency was assessed using Cohen's kappa coefficient. Initial agreement ranged from moderate to substantial; following retraining and iterative discussion, coders re-coded the data and achieved substantial agreement across all three domains (κ = 0.63, 0.67, 0.70). Ongoing triangulation and consensus discussions among the research team further supported the credibility and trustworthiness of the findings.
Results
Table 1 presents the participant characteristics. Participants were mostly female (65.6%), with the average age of 68.2 ± 11.1years. The majority of participants had attended some college (59.4%). The average household income was $42,074, which is below the national average of $77,700. 15 All participants identified as non-Hispanic AI members of the tribal community where the interviews took place. No study participants were excluded from analysis.
Participant demographic characteristics.
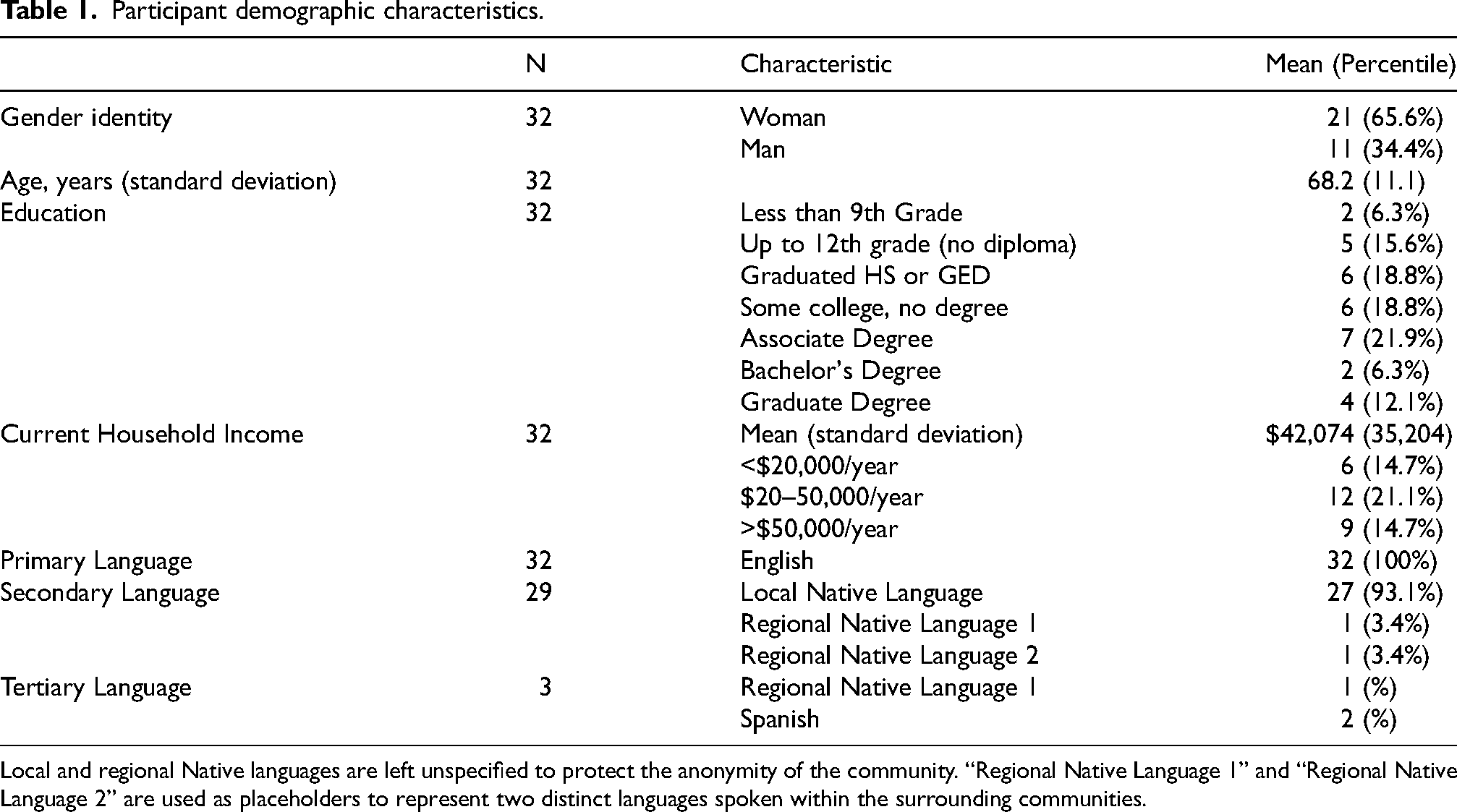
Local and regional Native languages are left unspecified to protect the anonymity of the community. “Regional Native Language 1” and “Regional Native Language 2” are used as placeholders to represent two distinct languages spoken within the surrounding communities.
Interview themes and subthemes
Question 1: what are the positive aspects of aging in your community?
Participants were first asked to describe the positive aspects of aging within their community. We deliberately placed this question at the beginning of the semi-structured interview, prior to introducing any discussion of dementia, in order to foreground strengths and optimism. Starting with a focus on the value and meaning of aging allowed us to capture how community members conceptualize this stage of life beyond the lens of illness or decline. Their responses offered a richer and more holistic understanding of aging as experienced within their cultural and social context.
From these interviews, we identified recurring themes, which were systematically organized and refined into a codebook. Each theme was supported by complete ideas and illustrative examples, ensuring that the analysis reflected the perspectives shared by participants. To further synthesize these findings, we created a visual representation (Figure 1) in the form of a mind map. Figure 1 highlights the diversity and frequency of themes and illustrates their interconnections, using shortened titles to those in the Codebook for easier visualization. Though only the most prominent themes will be discussed, it is important to consider the variety of themes discussed.

Mind map illustrating themes and subthemes identified for positives of aging. Size of theme or subtheme relates to relative frequency theme was identified.
Aging allows one to inherit or deepen one's traditional role and relationship with their culture
When asked about the positive aspects of aging, participants positively described inheriting traditional roles associated with being an elder in their community. In our codebook, we described Traditional Role as Being Rooted in Traditional Culture, Passing on Wisdom to a Younger Generation, Acting as a Role Model or Leader in their Community, or Feeling more Connected or Involved with their Sense of Spirituality or Religion. An individual's relationship with culture, language, and spirituality were among the traditional elements described as deepening as one ages. “Always look to the clan elders, the uncles, for advice— to listen, to encourage, to support.” Male in his 60s [A positive to aging is] “Trying to keep the knowledge alive about our home, [Pueblo] culture here. Passing it on. That's probably the best- strongest I've seen.” Male in his 60s
Aging allows for more time (taking one's time and socialization)
Another important theme was an appreciation for taking one's time, not only in daily activities but in decision-making practices. Participants described increased free time that they could spend being active in their community and with family and friends. Additionally, some participants said they felt as though they trusted themselves and made more deliberate choices in their older age. “I try to think more in depth. I try to analyze things and not make such quick decisions.” Female in her 80s “Well you get to have more flexibility in your daily schedule and you are able to retire from work and spend more time with family. But what I realize is that an individual who is older and retire, you can also find yourself very busy in the community.” Female in her 70s
Uncertainty towards positives of aging
While some participants described a general gratitude for still being alive, there were others who described aging as a challenging stage and did not describe any positives associated with getting older. “I don't know. I don't see any.” Male in his 50s “I don't know about that, I don't know what to say. Just getting older, you don't realize.” Male in his 70s
Question 2: what does dementia mean to you?
Participants were asked an open-ended question about what the term “dementia” meant to them. This was intentionally posed before providing any formal description or educational information about dementia or its causes. Our aim was to capture participants’ own understandings of the term as representatives of their community, thereby gaining insight into the community's definition and conceptualization of dementia. Following the interview questions presented in this manuscript, participants were then given a brief educational overview of how dementia is defined in Western science and what is currently known about its causes. This information was shared to address any questions and ensure ethical engagement, but only after responses were collected, so as not to influence or shape participants’ initial perspectives. Figure 2 highlights the scope of themes discussed and illustrates their interconnections, using shortened titles for easier visualization. Most significant themes are discussed below.
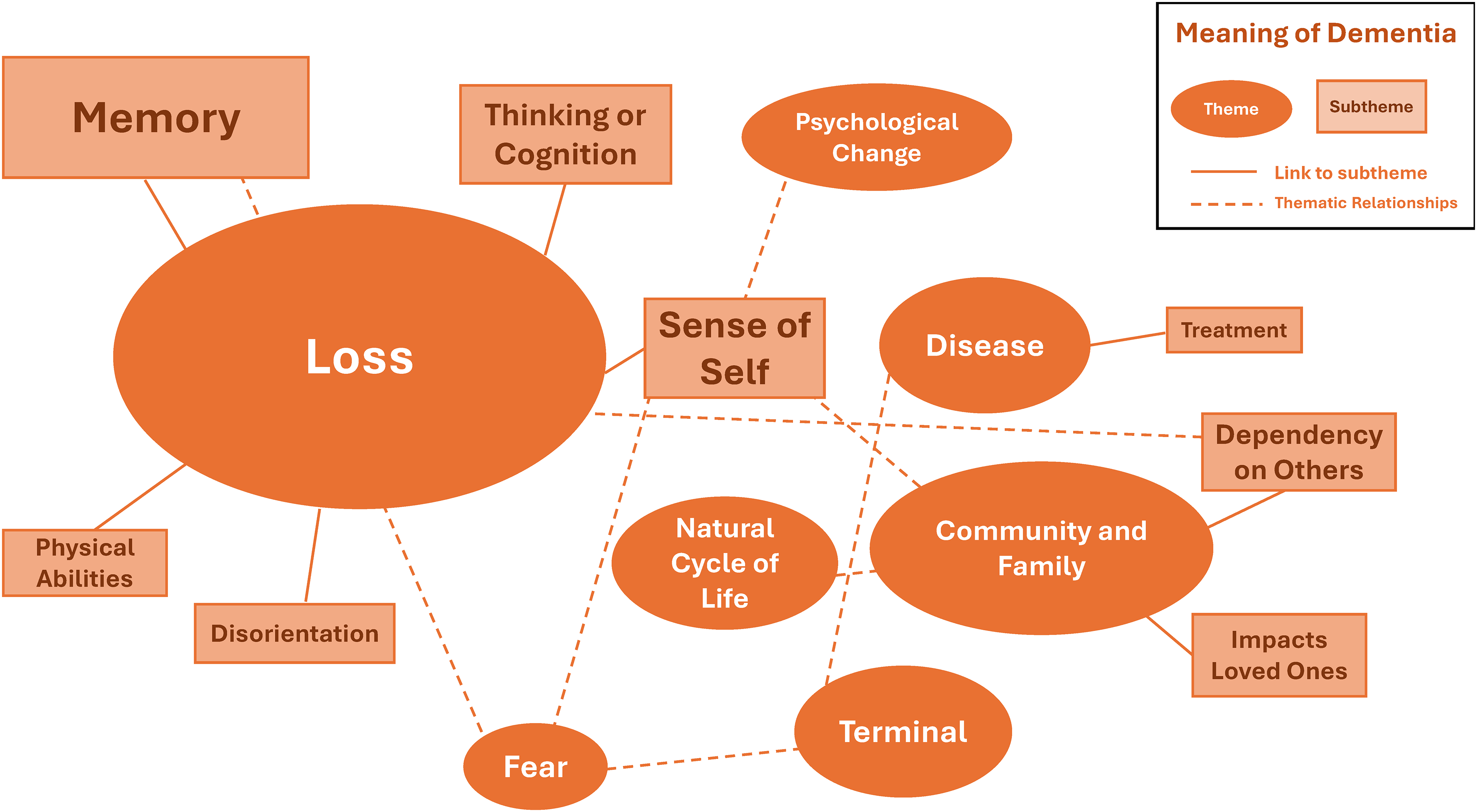
Mind map illustrating themes and subthemes identified for dementia meaning. Size of theme or subtheme relates to relative frequency theme was identified.
Dementia means loss
Participants were asked if they knew of the term “dementia”, and what it meant to them. Almost one third of participants (31.25%) described being uncertain about the term, which is a significant finding in and of itself. There were others who were more confident in their understanding of the term, and the majority of these participants described dementia as loss: loss of memory, thinking, independence, or sense of self. “Not remembering something in the past or present. Like your personal information, you have to go back and maybe relate to people in your household to remind you.” Female in her 70s “I think it's, I probably can't remember the whole definition but I think it was a form of cognitive thinking that starts to become limited. Forgetfulness, I think they mentioned that it was a disease.” Female in her 70s “It means that an individual loses some ability in thinking, rationalizing, being themselves. Um, losing memory, losing skills, losing the ability to do anything for themselves.” Female in her 50s
Fear was also described several times in conjunction with these understandings: The idea of losing yourself and your memories to AD was described as fearful, as was the concern for loved ones becoming disoriented and lost. “Loss of memory. Well it's almost like a scary topic because if you have that you're going to forget your children's names, your grandchildren's birthdays.” Male in his 60s “Family members think about people wander off and get lost. They wander off on their own.” Female in her 70s
Dementia involves the community and the family
Understandings of dementia and caregiving practices are interdependently woven together, as care practices can influence perceptions of the disease itself. Individuals’ perceptions of dementia may be influenced by personal or secondhand knowledge of caregiving for elders with cognitive decline. Many participants discussed care practices after being asked about the meaning of dementia or aging. Some participants described that older adults needed to adjust one's way of life to be more reliant on family to help manage their care as they age. “There's one or more people in the family who would like to step forward and make sacrifices of their own to help out elders of their family. I did that.” Male in his 60s “As a family, we've all had a family meeting and decided when mom and dad would get to a certain age, who will be responsible. And with my siblings, we all share the responsibilities. We did that with my mother and now my father…we all agreed we would never put them in a home and that we would take care of them.” Female in her 50s
One participant discussed dementia in the context of negative healthcare experiences they have had. When providers fail to meet patients’ needs, they may inadvertently increase mistrust and reduce patients’ engagement in appointments and follow-up care. “My provider would always deflect the question and I’d keep pressing her and she didn’t satisfy my question. I want to know something about my doctor before I give them my answers. I want to know who I’m talking to and what makes them qualified to meet with me.” Male in his 60s
Question 3: what do you think causes dementia?
Similar to the previous question, it is important to note that participants were asked about their causal understandings of dementia before receiving any educational information from the research team. This follow-up question was only posed if participants indicated in Question 2 (“What does dementia mean to you?”) that they had some knowledge of the term. Those who responded “I don’t know” (31.25%) were not asked this question. Consequently, the findings presented here reflect the responses of 68.75% of the sample, who may represent individuals with greater familiarity or knowledge of dementia and therefore may not fully reflect the views of the broader community. Figure 3 presents the most common themes identified, along with their interconnections, using shortened titles to facilitate visualization. Though not all themes are discussed below, these themes were depicted in the Figure to highlight diversity of responses.
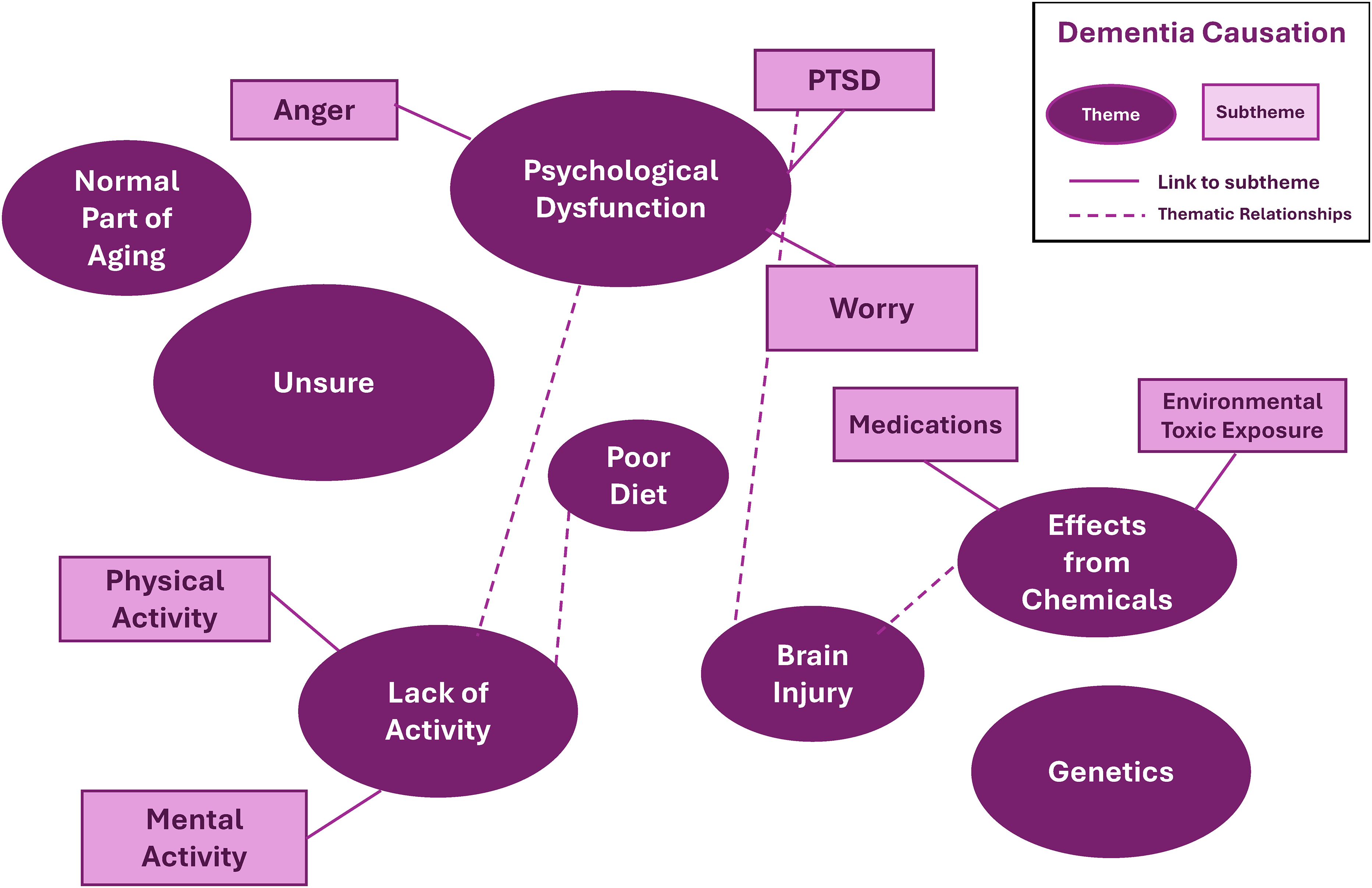
Mind map illustrating themes and subthemes identified for theories of causation. Size of theme or subtheme relates to relative frequency theme was identified.
Most participants described knowing what dementia meant (68.75%), and these participants were asked for their understanding of the cause of dementia. Many participants said they were not sure what could cause dementia. Others described dementia as a normal part of aging while a few mentioned “DNA” (deoxyribonucleic acid) or hereditary influences. Overall, there was greater emphasis on social and environmental factors driving dementia risk, than on physiological biomedical factors.
Poor diet, lack of exercise, or lack of engagement cause dementia
A large proportion of participants thought dementia was connected to lifestyle factors; specifically, they related dementia to changes in diet, lack of exercise, or decreased engagement. “I think that the brain, like anything else, is also a muscle and if you don't use your muscles enough, then sometimes that muscle might deteriorate. And just like your physical abilities, you also need to exercise your mental abilities.” Female in her 70s
“I guess just not doing anything. Just being, what- uh, not being interested in anything I guess. Not wanting to do anything.”
Female in her 80s “I believe it's twofold, one that it's passed on by DNA. I also believe that it's um nutrition, that as I got older and I moved from having home cooked meals to like the ready to eat stuff.” Male in his 60s
Dementia stems from psychological distress
Additionally, many participants discussed the potential causal factor of strong emotions or stress. Some described the relationship between unresolved grief or traumatic events contributing to one's risk for dementia. “The causes I would- I didn't- It comes with age or maybe stress. Probably emotional stress.” Male in his 50s “I would say it can be caused by sometimes traumatic events in your life. You tend to hold things back, not want to remember, and I guess it just triggers how you grew up or lived your life.” Female in her 50s
Dementia is a result of effects from chemicals
A few community members said that dementia was a side effect of possible medications. Others talked about the past military effects on the land, and how toxins or poisons left in the land can circulate our food and water systems, potentially contributing to diseases such as dementia. These discussions were tied with comments about poor encounters with practitioners or large organizations, like the military or mining companies and indicated a general mistrust of these systems. “…During your lifetime people ingest medicine, whatever it may be, over the counter and there are side effects. And people don't ask what those side effects are, they just think ok it's going to help me and they don't wonder what those side effects are.” Male in his 60s “It has a lot to do with our environment…like in the water, you need it to water our crops, you consume the crops and that goes into our body.” Female in her 60s
Discussion
The current study provides insight into explanatory models of dementia for a Southwest Pueblo community. Participants identified many strengths pertaining to how individuals age in their community, such as the valued role of Elders, an emphasis on passing down wisdom, and increased time with family. Although some were unsure of the formal definition of dementia, many participants accurately described the various types of loss that accompany ADRDs. Additionally, participants reported a broad range of perceived causes of dementia, spanning biological explanations, exposure to chemical pollutants, and life course factors. Many participants described multiple causes simultaneously, creating an interconnected web of causation rather than a single, linear explanation. Importantly, the ways in which these causes were framed also reflected broader hesitation to trust Western systems of knowledge and care.
Understanding the positives (and negatives) of aging in context
Across interviews, participants described both the meaningful benefits and the significant challenges associated with aging. Overall, most participants described the positives of aging in terms of developing new or deepened connections with their traditional cultural identity, spirituality, and family. For some, aging was viewed as a time to share wisdom, teach younger generations, and strengthen ties to language, land, and community traditions. These experiences were described as sources of pride and purpose.
However, even though the interview question focused on positives, many participants also spoke about the converse—the losses, barriers, and absences that shape their experiences of aging. A few participants described little to no positives of aging and were not able to identify many resources in their communities. Several participants noted that previous generations seemed busier and had more defined cultural roles, and that this shift toward social isolation and reduced cognitive engagement may increase dementia risk. This could be influenced, in part, by the difficulties arising from the SARS-CoV2 (COVID-19) pandemic: senior centers and community resources were closed, leading to the loss of important cultural and social hubs, and communities are still navigating this recovery. Furthermore, Indigenous communities have documented disparities in healthcare resource access, with fluctuating and unreliable access to specialized and emergency services. 16 Feelings of isolation heightened during the pandemic, combined with increased difficulty obtaining medical services, underscore how aging can be experienced as not only frustrating and isolating, but also as a reflection of broader systemic inequities that shape elders’ opportunities for care, connection, and wellbeing.
A spectrum of caregiving beliefs
Many perspectives of dementia and aging were tied to participant discussions of family caregiving practices. In many AI communities, informal and family caregiving is the primary or sole form. 17 This is in part from necessity due to the barriers faced by Indigenous communities to access Western medical resources, but also influenced by cultural emphasis on familiar interdependence and cultural values of reciprocity and respect.17–18 While many individuals have found caregiving rewarding, it is also important to consider the various stressors: psychological changes, strains of family relations, or the negative effects on personal career choices.18–19 At the interpersonal and community levels, Jaramillo and authors found that wellness among AI elders is sustained through strong kinship networks, intergenerational caregiving, and collective resilience. 13 Family and community relationships provide meaning and motivation to stay well, yet caregiving responsibilities and grief associated with loss can also act as stressors. Although all participants were older adults, they described a wide range of experiences with caregiving—both in providing care to relatives and in receiving care themselves. Their perspectives also reflected strong and sometimes divergent views, ranging from the belief that caregiving should remain solely a family responsibility to openness toward outside assistance or placement in care facilities. These differences underscore the diversity towards caregiving perspectives that exist in a single community alone. For healthcare providers, this highlights the importance of considering each individual's unique circumstances, cultural values, and family dynamics when discussing care management. Adopting a shared decision-making approach that centers the elder's preferences can help ensure care aligns with both personal and cultural priorities.
Uncertainty of the term “dementia” and fear of the disease
Findings from this study underscore the critical need for psychoeducation and culturally responsive education about dementia within Indigenous communities. Nearly one-third of participants expressed uncertainty about the meaning of the term dementia, highlighting a significant gap in shared understanding of the condition and how it is conceptualized in Western medical contexts. This lack of clarity has important implications for researchers and healthcare providers, as it may affect individuals’ willingness to seek care, their ability to describe symptoms, and their trust in the diagnostic process. Among participants who felt more confident in their understanding, dementia was most often described in terms of loss—loss of memory, independence, thinking, or sense of self. These views were consistently accompanied by expressions of fear: fear of losing one's identity and autonomy, and fear of becoming a burden on family members. Such narratives reveal the profound emotional weight attached to dementia and point to the need for approaches that attend not only to cognitive decline but also to the lived, affective experiences of patients and families. Collectively, these findings suggest that education and communication around dementia must move beyond technical definitions. Interventions should prioritize psychoeducation that validates concerns and fears, provides culturally grounded explanations, and creates opportunities for dialogue about what dementia means across cultural contexts.
Differences in understandings of dementia causation between community participants and the Western medical system
Participants demonstrated considerable wisdom in their understandings of dementia, identifying a range of causes that in many ways align with Western medical perspectives, including lack of exercise, poor diet, limited social engagement, and the effects of poor mental health. At the same time, several participants described dementia as a natural part of the cycle of life, echoing findings from other Indigenous communities where aging and cognitive decline are conceptualized as expected life transitions rather than pathological conditions. 20 There was overall a greater emphasis placed on social and environmental factors (i.e., psychological and lifestyle causes) than on biomedical factors (such as genetics and brain injury), which is in line with previous research on AI perspectives of dementia. 21
Within Western medicine, AD is primarily defined by the accumulation of amyloid plaques—abnormal clumps of protein fragments that build up between nerve cells—and tau tangles, which are twisted strands of another protein that form inside neurons and disrupt their function. 22 These changes interfere with communication between brain cells and ultimately contribute to cell death and brain atrophy, though the origins and exact sequence of these processes are still being investigated. Importantly, other dementias are also associated with related pathological processes, including abnormal protein aggregation and neurodegeneration, though the specific proteins and patterns differ. Notably, no participants described AD or other dementias in terms of these or similar biological mechanisms, suggesting that incorporating such information in accessible ways may be an important component of psychoeducation. To enhance impact, dementia education could be integrated into existing community health initiatives—such as ongoing diabetes prevention efforts by the local health department—and also addressed directly by medical providers and research groups, thereby embedding dementia awareness into both community and clinical contexts.
Theories of causation highlighting mistrust
A few elders identified genetics or DNA as potential causes of dementia, while others emphasized the role of medication side effects and environmental pollutants. Some community members specifically described dementia as a side effect of medications in conjunction with poor experiences with healthcare providers—a perspective that may reflect experiences of mistrust, including poor communication with providers and the absence of relationships in which patients felt comfortable asking questions or raising concerns. Others highlighted the lingering impacts of military activity on the land, including toxins or poisons that contaminate food and water systems. In the Southwest United States, American Indian communities living near abandoned uranium mines face potential exposure to mixed-metal contamination, which can alter messenger RNA (mRNA) expression and increase cardiovascular burden—therefore contributing to dementia risk. 23 Integrating these environmental concerns into understandings of dementia underscores the long history of governmental and commercial land abuses, which continue to shape perceptions of health and disease. This connection between environmental trauma and illness may also extend to relationships with Western medical providers and treatments, reinforcing mistrust rooted in historical violations of Indigenous communities.
Study limitations
This study was limited by the use of a community sample composed of individuals who elected to participate in a university-based research study. As such, the findings may not fully capture the perspectives of community members who have less trust in medical or research systems. To help mitigate this, we collaborated with local CHWs who facilitated interviews in participants’ preferred language. Nonetheless, the relatively high proportion of participants who expressed uncertainty about the meaning or causes of dementia suggests that the responses may not be representative of the broader community, but instead reflect the views of a more informed or engaged subset. Importantly, this research highlights the perspectives of a single AI community, with its own distinctive history and cultural traditions. While these findings reinforce the importance of culturally competent care that integrates both Western and traditional approaches, they should not be generalized or homogenized across all AI/AN groups.
Recommendations for future clinical, community, and research efforts
These findings suggest a variety of clinical, population health, and research pathways. Clinically, treatment planning should involve shared decision-making that includes the individual, their family, and providers who are knowledgeable about community resources. A theme from this research was the importance some participants placed on not rushing in their older years; therefore allowing patients time to consider their options may be essential for respectful and effective care. Findings from the research suggest that assessing loneliness, a risk factor in aging, should be prioritized. 24 Evaluating activities of daily living may also require adaptation, as measures that assume individual autonomy may not fully capture functioning within communities where interdependence is central. Responses to treatment are likely to vary based on cultural values: in this Pueblo community, medicalized interventions may be approached with caution, while lifestyle-based strategies such as diet, exercise, and social engagement may be more readily accepted. When pharmacological treatment is considered, additional time may be needed to explain benefits and potential side effects. Psychological care may also be strengthened by involving family members or offering community-based support groups, ensuring that treatment aligns with both cultural practices and individual preferences.
Caregiver needs are another critical consideration. Although caregiving can be deeply rewarding, it also carries significant challenges. Supports such as respite care, counseling, and skill-building programs, when tailored to community contexts, may help alleviate these burdens. In this Pueblo community, one participant described that he was part of a program which allowed him to receive compensation for his caregiving duties. This type of caregiving compensation preserves elders’ valued familiar and cultural roles by increasing participation in social events and creating opportunities to share wisdom to their family. Such approaches not only provide monetary support for community-member-caregivers but also affirm the dignity and cultural significance of the elders’ roles. Integrating cultural frameworks of wellness—such as the Relational Worldview, which emphasizes balance between body, mind, spirit, and context—may offer pathways to culturally congruent dementia prevention and care. 6
In terms of population health, a dementia education that validates community perspectives, addresses uncertainty and fear, and creates dialogue about dementia's meaning is essential. Integrating dementia education into trusted health initiatives (e.g., diabetes prevention programs) may not only increase familiarity with the term across multiple timepoints but also situate dementia as a condition interconnected with other health concerns, reinforcing its relevance within broader health education.
Future research in this area should prioritize community-engaged projects that examine how dementia education can be meaningfully integrated into existing health department programs, building on trusted infrastructures to reach a wide audience. In addition to broad public health efforts, research on support groups may provide valuable insight into whether these spaces serve as effective sites of connection, coping, and education for individuals diagnosed with dementia and their families. Expanding on this, further work is also needed with Indigenous caregivers, drawing from prior studies to better understand culturally specific caregiving practices and support needs for the community. 25 Finally, our team intends to extend this line of inquiry by investigating approaches to AD biomarker disclosure, with particular focus on how such sensitive information can be communicated in ways that are culturally responsive, supportive, and ethically responsible—fostering understanding while minimizing potential harm.
Conclusion
These findings highlight the value of gaining deeper community insights into the meaning of dementia and the explanatory models of its causes. In this Southwest Pueblo community, participants described perspectives that both align with and diverge from Western medical frameworks, offering a much richer understanding of the population to be treated. Participants described the role of elders as valued and emphasized intergenerational connection and cultural continuity. Dementia was described in terms of loss and dependence on family, accompanied by uncertainty about the term itself and fear of its consequences. Explanations of causation extended beyond biomedical models to include lifestyle, psychological, and environmental factors, rooted in the broader context of historical and structural influences that continue to shape healthcare today. The significance of this research lies in its potential to reshape how dementia is approached in Indigenous communities: ensuring that prevention and treatment strategies validate local knowledge, address fears and uncertainties, and recognize caregiving and social support as central to wellbeing. More broadly, it demonstrates how centering community voices can generate richer, more meaningful approaches to care and research.
Footnotes
Acknowledgements
We want to recognize the approval and support of the tribal Governor and the Tribal Council. We sincerely thank the Pueblo people for welcoming us and participating and guiding the research. In addition to the community members and skate-holders that are authors on this publication (Malanie Garcia, Alfonso Cheromiah, Madison Nez), we also want to specifically thank Roseanne Pasqual for supporting this effort.
Ethical considerations
Approval for the study was received from the local tribal Government. The study was then approved by the University of New Mexico (UNM) Health Science Center Institutional Review Board (IRB) and the study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Participants were providing consent information verbally via consent documentation prior to any study participation.
Consent for publication
This manuscript has been approved for publication by the Pueblo Government.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health (P20GM103451), the New Mexico Alzheimer's Disease Research Center, funded by the National Institute of Aging (P20AG068077, P30AG086404), and the UNM HSC Clinical And Translational Science Center (UL1TR001449), funded by the National Center for Advancing Translational Sciences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available as they are owned by the Tribe represented in the study, but requests from the Pueblo government to see the data can be made by contacting the corresponding author.