
Abstract
Anxiety in autism is often misunderstood when compared with neurotypical experiences. It is not as simple as saying, “It’s okay, everyone gets anxious.” Anxiety in autism is not merely a transient experience but often a persistent and pervasive challenge shaped by both neurobiological differences and societal structures. While transient (state) anxiety is common in the general population, many autistic individuals can experience chronic (trait) anxiety, deeply intertwined with sensory sensitivities, social challenges, and the cumulative weight of past traumas. This article examines the complex nature of anxiety in autism, emphasizing how systemic barriers, stigma, and learned coping mechanisms contribute to sustained distress. It explores how societal pressures and internalized responses create self-reinforcing anxiety cycles, supported by psychological and neurobiological mechanisms. The article offers multilevel suggestions—spanning societal, community, professional, research, and individual levels—highlighting the need for inclusive, flexible approaches that account for the diversity of the autistic experience. Addressing both external barriers and internal challenges, these suggestions aim to promote well-being and reduce the burden of anxiety across the autism spectrum.
Community Brief
Why is this topic important?
Anxiety in autism is often misunderstood, especially when compared with the anxiety non-autistic people experience. For many autistics, anxiety can be more intense and constant. It is shaped by both brain differences and social pressures, such as stigma and exclusion. Over time, these pressures make anxiety build up and become difficult to manage. At the same time, autistics have difficulty accessing mental health services to get the support they need. Reasons include high cost, shortage of services, and biases and misunderstandings from health care providers about who benefits from mental health support.
What is the purpose of this article?
This article looks at how social factors and brain differences combine to influence anxiety in autistic individuals. It aims to give a clearer understanding of why anxiety in autism is unique and more complex compared with the anxiety experienced by non-autistic people.
What personal or professional perspectives does the author bring to this topic?
The author brings personal experience as an autistic person with ADHD who deals with social anxiety, sensory issues, and spoken communication challenges, offering a lived understanding of anxiety in autism. The article also draws on the author’s academic research in autism, combining insights from neuroscience, psychology, and disability studies to provide a well-rounded perspective. As an disability advocate, serving on multiple disability boards, the author brings broader insights and has written extensively on autism and disability, promoting greater awareness and change.
What is already known about this topic?
Anxiety is more common in autism than in the general population. Sensory sensitivities, social challenges, and co-occurring conditions such as ADHD and depression can intensify anxiety for autistics. However, most research focuses on anxiety in non-autistics, which doesn’t fully explain the constant, lifelong anxiety many autistic individuals experience.
What does the author recommend?
The author recommends addressing anxiety in autism through several approaches. These include changes in society, improvements in professional care, new research priorities, stronger community support, and practical strategies that individuals can use. These recommendations are not one-size-fits-all. Instead they aim to support the diverse needs of autistics, including autistics with higher support needs. The author also encourages everyday strategies for mental health, to reduce dependence on costly or hard-to-access therapies.
How will these recommendations help autistic adults now or in the future?
These recommendations aim to make mental health support easier to access, inclusive, and affordable. In addition, by promoting everyday strategies to autistics, we not only reduce dependence on expensive professional services but also enable autistics to have more control over their own health, following the disability principle of “Nothing about us, without us.” Mental health is fundamental for a good quality of life and autistics’ need to thrive and not just survive.
Keywords
Introduction
“It’s okay, everyone gets anxious.” This is a thing people say to an autistic to make them feel better. But it’s not that simple. For many autistics, anxiety isn’t a “sometimes thing.” When you already have a persistently high baseline of anxiety, any new stressor just adds to an already overflowing pile.
As an autistic scholar, with attention-deficit/hyperactivity disorder (ADHD), high social anxiety, sensorimotor, and communication challenges, I experience these realities firsthand. Social interactions, for instance, might not be stressful for neurotypicals, but for many autistics like me, the very thought of having to navigate evaluative social situations can be overwhelming. My breath shortens, and my mind goes into analysis paralysis, looping through every possible outcome and word choice to aim for the most succinct response. In the background, I can almost hear the other person’s impatient mental tapping of a foot. My heart races as pressure builds under the weight of this spotlight effect. Regaining composure and recalibrating take time and effort, and in high-stakes interactions, this cognitive overload can sometimes lead to intense anxiety and even meltdowns.
To be sure, everyone experiences anxiety at times, and it’s a normal part of life. However, in everyday conversation, anxiety often refers to its transient form (state anxiety), an adaptive response to challenges or threats.1,2 External pressures or demands can trigger such transient anxiety, which helps individuals prepare for or respond to stressful situations. While both autistics and non-autistics can experience transient anxiety, many autistics contend with anxiety that is chronic and is often deeply intertwined with sensory sensitivities, social challenges, and the cumulative weight of past traumas. This persistent form of anxiety (trait anxiety) often leads to heightened distress and significant impacts on daily functioning.3,4 It’s crucial to understand that while anxiety is universal, the experience of it in autism is often more profound and persistent.
So when someone says, “It’s okay, everyone gets anxious,” they miss the point entirely. It’s not that autistics don’t understand anxiety—we do. My anxiety is often more intense and constant, and comparing it with neurotypical experiences minimizes the struggles involved. This statement, intended to comfort, instead highlights a lack of understanding and empathy. It fails to acknowledge the unique, pervasive nature of anxiety in autism.
This article examines the complex nature of anxiety in autism, emphasizing how societal structures, systemic barriers, and learned coping mechanisms interact to create and sustain distress. While neurobiological factors play a role, anxiety in autism is not solely an intrinsic trait but is also shaped by exclusion, stigma, and institutional constraints. By exploring these interwoven influences, the article highlights the need for interventions that address both external barriers and internalized responses. The article presents a range of recommendations across societal, professional, research, community, and individual levels, recognizing that effective solutions must be flexible and inclusive. Rather than advocating for a one-size-fits-all approach, this framework acknowledges the diverse needs of the autistic community and the importance of systemic change in fostering meaningful support.
Prevalence and Impact of Anxiety in Autism
Anxiety disorders are significantly more common in autism, affecting up to 69% of autistics compared with 18% in the general population.5,6 Aside from anxiety disorders, common diagnoses include generalized anxiety disorder (up to 29% of autistics) and social anxiety disorder (up to 17%). 7
Several factors contribute to this heightened vulnerability. Co-occurring conditions, such as ADHD and depression, further elevate risk. 6 Gender differences are also observed, with autistic females more likely to be diagnosed, potentially due to differences in social expectations and coping strategies. 6 Neurobiologically, heightened amygdala activity in autistics may contribute to exaggerated stress responses, particularly in unpredictable or social environments. 8 Additionally, dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis prolongs physiological arousal and impairs stress adaptability.9,10
The effects of anxiety extend beyond mental distress, impacting employment, daily living, and healthcare access. Anxiety-related challenges—such as difficulty managing interviews, workplace interactions, and cognitive demands—contribute to high turnover, absenteeism, and reduced economic stability.11–13 Outside structured environments, anxiety exacerbates social withdrawal, leading to isolation, avoidance behaviors, and reduced independence.14,15
Sensory sensitivities, affecting up to 90% of autistics, further heighten anxiety. Sensory overload can trigger acute distress, reinforcing avoidance behaviors and limiting participation in daily activities.16,17 Additionally, altered interoception, difficulties perceiving internal bodily states, can hinder emotional regulation, making it harder to identify and manage stress.18,19
While anxiety in autism has clear neurobiological underpinnings, its persistence and impact are shaped by external forces. The following section examines how societal structures and learned coping mechanisms reinforce and sustain anxiety over time.
Social Constructs and Theories Shaping Anxiety in Autism
Anxiety in autism does not arise in isolation; it is reinforced by societal structures, institutional barriers, and psychological mechanisms. 20 Public misconceptions, exclusionary systems, and learned coping strategies create an environment where anxiety is not just heightened but also self-perpetuating.
As Figure 1 illustrates, external pressures such as stigma and exclusion create distress, prompting behavioral adaptations that, over time, reinforce anxiety. Table 1 expands on these interactions, detailing how systemic and psychological mechanisms sustain anxiety cycles. This section examines systemic and social pressures, explores psychological and behavioral responses, and finally, delves into the mechanisms that sustain anxiety. Addressing these constructs is essential for reducing systemic stressors rather than placing the burden on autistics to adapt. 42

This figure outlines how anxiety in autism arises and is sustained over time. Systemic and social pressures
Social, Psychological, and Structural Factors Contributing to Anxiety in Autism

Systemic and social pressures: The foundations of anxiety
Anxiety in autism is reinforced by systemic barriers that sustain chronic stress and exclusion. These pressures manifest at multiple levels: societal stigma fosters bias, systemic barriers restrict access, mental health stigma fuels misconceptions, low expectations limit opportunities, and intersectionality compounds marginalization (Fig. 1A, Table 1A). Together, these forces sustain anxiety cycles by restricting essential resources while reinforcing exclusion and self-doubt.
Societal stigma surrounding mental health 22 and autism perpetuates exclusion by reinforcing harmful stereotypes—such as the misconception that autistics have a narrow range of emotional experiences. 5 These biases contribute to social rejection and create significant barriers to appropriate mental health care, as autistic distress is frequently misinterpreted or dismissed in clinical settings. 45 Many autistics are denied effective treatment because their symptoms do not conform to neurotypical expectations. 5 Paradoxically, autistics with higher support needs are often perceived as not having mental health needs at all, as the focus is often on managing behavioral challenges rather than also considering psychological well-being.45–47
Beyond limiting access to care, stigma has measurable biological effects. Chronic exposure to discrimination dysregulates the autonomic nervous system and HPA axis, heightening physiological anxiety responses.21,44 Mental health stigma further discourages self-advocacy, as seeking help is often framed as a weakness rather than a legitimate need. 22 Thus, stigma does more than drive exclusion; it intensifies anxiety both psychologically and physiologically, reinforcing cycles of distress.
Systemic barriers further entrench social and economic disparities by restricting access to education, employment, and health care. 24 In education, autistic students—particularly those with higher support needs—face low expectations that limit access to mainstream coursework and advanced learning opportunities. 25 Preconceived assumptions about their inability to learn or succeed often create a self-fulfilling prophecy, 48 as exclusion from these opportunities reduces future prospects in higher education and employment.
Similarly, workplace discrimination, inaccessibility, and lack of accommodations result in disproportionately high unemployment and economic instability, exacerbating chronic stress.11,13,31 These barriers extend into health care, where clinician biases and rigid diagnostic frameworks contribute to underdiagnosis of co-occurring conditions and inadequate treatment. 24 Instead of ensuring equitable access, these structural exclusions reinforce cycles of anxiety and economic precarity.
Intersectionality further amplifies these challenges. Autistics of color, women, and those with higher support needs face compounded discrimination, leading to greater exclusion from mental health care, employment, and community support networks.27,28 Biases within both disability and racial justice movements often render these individuals invisible, reinforcing their social isolation and lack of resources. 49 Without structural change, these systemic exclusions continue to deepen cycles of anxiety and distress.
Psychological and behavioral responses: Coping at a cost
Faced with systemic barriers and social exclusion, autistics develop adaptive strategies (Fig. 1B, Table 1B) to navigate environments that are not designed for their needs. 20 While these strategies may provide temporary relief, they often reinforce long-term anxiety and distress.42,43
One consequence of exclusion is internalized ableism, where autistics absorb societal attitudes that devalue their abilities, fostering self-doubt and reluctance to seek accommodations for fear of being perceived as burdensome. 20 Internalized ableism can also complicate intragroup dynamics within the autistic community, where some autistics may unconsciously project these internalized biases onto other autistics they consider as “more disabled.” Research on disability hierarchies shows how ableist standards can lead to stratification within disabled communities suggesting that similar dynamics might occur among autistics. 49 This class hierarchy within autism, based on perceived abilities related to communication, behavioral, and sensory challenges,28,49 perpetuates feelings of inadequacy and exacerbates anxiety among more impacted autistics, reinforcing a cycle of exclusion and heightened distress.
In response to social pressures, many autistics engage in effortful social adaptation, suppressing natural traits to conform to neurotypical expectations. 30 This may involve mimicing social behaviors, forcing eye contact, or masking sensory sensitivities to minimize rejection. 29 “Masking,” a term used to describe the conscious or unconscious suppression of autistic traits to appear more neurotypical, often includes camouflaging social difficulties, hiding sensory discomfort, and imitating conventional social norms. 30 Though these strategies may reduce immediate discrimination, they require significant cognitive effort, leading to exhaustion, identity erosion, and increased anxiety over time. 43 While masking is frequently discussed in the context of autistic women, effortful social adaptation is widespread across genders, with intersectionality amplifying the pressure to conform.
Another significant burden is the constant need for self-advocacy, as autistics must repeatedly justify their needs and request accommodations.20,31 While the Americans with Disabilities Act was designed to ensure access, in practice, autistics must navigate bureaucratic resistance and societal skepticism. 50 Because autism presents differently across individuals, accommodations are often misunderstood, leading to perceptions that they provide unfair advantages rather than necessary support. 31 This skepticism raises the bar for inclusion, reinforcing cycles of anxiety and exclusion. 20
Mechanisms that sustain anxiety
Even as autistics develop coping strategies to navigate societal pressures, deeper cognitive, social, and structural mechanisms ensure that anxiety remains persistent rather than situational. These mechanisms influence how autistics interpret social interactions, sustain exclusion, and reinforce cycles of stress and marginalization (Fig. 1C, Table 1C).
One key factor is negative attribution bias, the tendency to interpret ambiguous social cues—such as a neutral facial expression or delayed response—as rejection or criticism. 32 This cognitive distortion fuels social apprehension, reinforcing avoidance behaviors that deepen isolation. Over time, this self-perpetuating cycle of heightened vigilance, misinterpretation, and withdrawal further entrenches exclusion and distress.
Compounding this is stereotype threat, the fear of confirming negative societal stereotypes about one’s identity group. 33 For autistics, this may manifest as heightened pressure to disprove assumptions of social incompetence or rigidity, leading to excessive self-monitoring and cognitive overload. 20 In academic or social settings, I often find myself hyper-aware not just of my intellectual contributions but also of how my communication style, sensory needs, or even my atypical behaviors might reinforce stereotypes about autism. Unspoken social norms dictate who is taken seriously, creating a constant pressure to navigate and manage perceptions. This continuous effort is mentally exhausting, reinforcing both anxiety and social disengagement.
Another reinforcing mechanism is imposter syndrome, a psychological pattern where individuals experience persistent self-doubt and believe their success is unearned, despite external evidence of competence. 34 Autistics can often receive contradictory messages, expected to be “exceptional” to justify accommodations while simultaneously facing skepticism about their capabilities. This can manifest in autistics feeling as though they must work harder than their neurotypical peers to “prove” their legitimacy, further fueling stress and anxiety. These cognitive burdens are further reinforced by broader structural factors, where invalidation and social exclusion amplify long-term distress.
Structural and social factors
Beyond cognitive mechanisms, structural forces (Fig. 1D, Table 1D) shape autistic anxiety by limiting social capital, reinforcing invalidation, and undermining self-trust. Social capital, the benefits gained through interpersonal networks, is significantly reduced for autistics, particularly those with communication or sensory differences.35,51 Without meaningful social connections, access to emotional support and coping resources is restricted, increasing distress and reinforcing exclusion. 14
Interpersonal invalidation further heightens anxiety. Microaggressions, subtle, often unintentional discriminatory remarks, reinforce stereotypes and dismiss autistic experiences. 37 Comments like “Everyone’s a little autistic” or dismissing autistic distress as an overreaction invalidates lived experiences and contributes to social exclusion and self-doubt.
Similarly, gaslighting—outright dismissal of the autistic’s emotions and perceptions—further erodes self-trust, leading to deep-seated self-doubt. 36 When autistics express distress and are told they are “overreacting” or “too sensitive,” they begin to question their struggles, often feeling the need to suppress their experiences to be taken seriously.
Over time, these social and psychological stressors do not simply take a physiological toll, but they also become embedded in the body, leading to long-term physiological consequences.
Long-term physiological consequences
Autistics experience lifelong cumulative social stress (Fig. 1E, Table 1E), including bullying, exclusion, and lowered autonomy, which compounds anxiety from childhood onward.3,40,52 While these adversities may not fit clinical definitions of trauma, they create persistent stress responses, such as heightened emotional reactivity, chronic anxiety, and avoidance behaviors.39,41
These effects are particularly pronounced for minimally speaking or non-speaking autistics, who make up an estimated 25%–30% of the autistic population. 38 Because traditional diagnostic frameworks frequently rely on verbal self-reporting, their anxiety and mental health needs may go undetected or untreated, reinforcing long-term stress cycles.
Beyond psychological impacts, chronic exposure to stress has physiological consequences, a phenomenon known as allostatic load—where prolonged activation of the body’s stress response disrupts nervous system regulation, immune function, and overall well-being.9,44 Persistent anxiety symptoms, including sleep disturbances, sensory overload, and heightened physiological reactivity, further exacerbate stress sensitivity over time. 21
These cumulative stressors often culminate in autistic burnout, a condition distinct from general burnout. Unlike occupational burnout, which results from work-related stress, autistic burnout arises from chronic social and sensory stress, the relentless effort to navigate inaccessible environments. 43 This prolonged strain may contribute to altered neuroplasticity and emotional dysregulation, increasing long-term mental health challenges. 44 Autistic burnout manifests as extreme exhaustion, withdrawal, reduced cognitive and social functioning, and heightened sensitivity to stressors. 42
The anxiety reinforcement loop and long-term consequences
Together, these mechanisms form a self-reinforcing anxiety loop (Fig. 1F), where external biases shape internalized beliefs, cognitive distortions amplify distress, and avoidance behaviors further solidify exclusion. These cumulative stressors create a feedback loop in which social exclusion, unmet support needs, and persistent distress reinforce one another.
This article has explored the multifaceted nature of anxiety in autism, shaped by societal pressures, neurobiological sensitivities, and learned coping mechanisms. Building on Figure 1, it becomes clear that these factors are not separate but interlocking components that sustain anxiety. External pressures such as stigma and exclusion intensify neurobiological stress responses, while these heightened responses, in turn, make societal barriers harder to navigate—reinforcing the anxiety loop. Addressing one factor in isolation is insufficient; breaking the cycle requires interventions that target both the societal structures that sustain exclusion and the internal stress mechanisms that deepen distress.
The next section explores policy and intervention strategies aimed at disrupting this cycle and reducing anxiety in autistics by addressing root causes rather than placing the burden solely on autistics to adapt.
Recommendations
Disrupting the anxiety reinforcement loop in autism requires a multi-level approach that addresses social, psychological, and neurobiological factors. The following strategies span societal, community, professional, research, and individual levels, as summarized in Table 2.
Multilevel Strategies for Addressing Anxiety in Autism
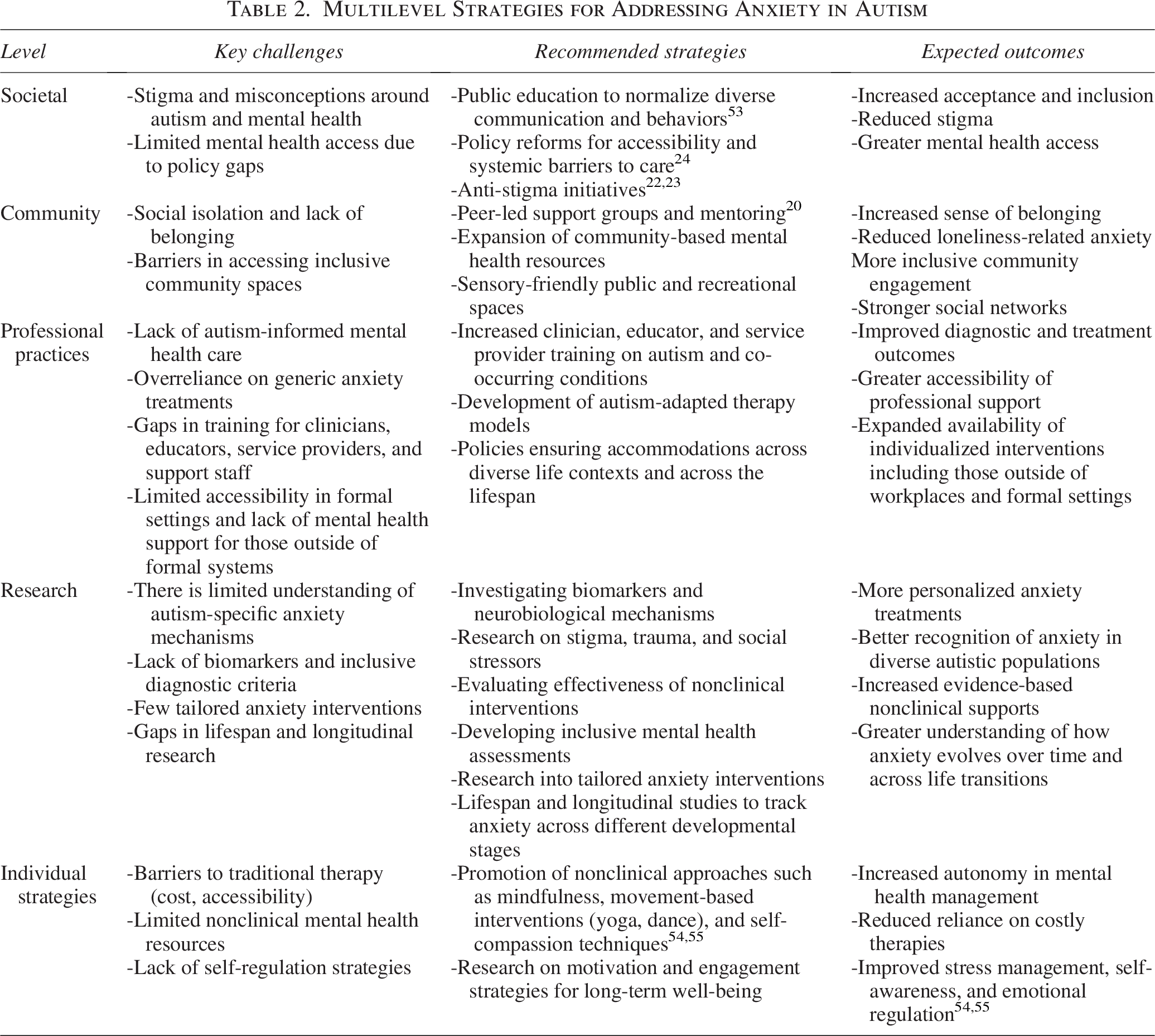
Beyond the recommendations mentioned in Table 2, several key considerations must be emphasized. Mental health services must be available, accessible, affordable, and inclusive of the entire autism spectrum, addressing communication, sensory, and cognitive differences to ensure equitable support. Policies should prevent price gouging in autism-labeled services, particularly in recreational and wellness sectors, and dismantle biases in determining who qualifies for support. Autism research should recognize that designing for the most impacted groups within the autistic community often benefits everyone. This aligns with the principles of universal and inclusive design.
Alongside clinical interventions, sustainable, self-directed approaches such as awe, gratitude, and mindfulness can be effective even in small doses.54,55 Simple, low-cost practices such as nature walks, yoga breathing, and brief moments of reflection offer accessible ways to reduce stress and improve resilience, reducing reliance on expensive therapies.54,55 However, for these approaches to be impactful, autistic voices must be central in shaping mental health frameworks. Recognizing autistics as key stakeholders in their own care is essential, aligning with the disability rights principle of “nothing about us without us.”
From Patching Problems to System Overhaul
While this article proposes strategies for addressing anxiety in autism, important gaps remain. Most anxiety research still focuses on non-autistics; identifying autism-specific biomarkers and underlying neurobiological mechanisms should be a priority. Longitudinal studies tracking anxiety across the lifespan are also essential to develop relevant interventions and supportive policies. Reducing stigma through widespread educational campaigns is critical as increased awareness can lower barriers in education, employment, and health care. Additionally, developing low-cost, accessible, nonclinical approaches remain essential to empower autistics to actively manage their mental well-being. Meaningful progress depends on targeted research, inclusive societal changes, and centering autistic voices in shaping solutions.
We began with, “It’s okay, everyone gets anxious.” But as we’ve explored, anxiety in autism is far more complex. Borrowing from artificial intelligence terminology to frame this reality, it’s not just about fine-tuning surface parameters—it’s about running a full model evaluation. For many autistics, anxiety isn’t just an occasional system alert—it’s a background process running at max capacity, constantly consuming resources, leading to overheating, and at times, triggering a full system shutdown (meltdown). The issue isn’t just with the user, it’s also with the model’s training data; societal structures optimized for a different user population. Instead of expecting autistics alone to constantly overclock their processing power just to function, we need a fundamental shift in the base model’s architecture itself, one that centers universal and inclusive design, and prioritizes sustainable alignment. Only by rewriting the core algorithm of inclusion can we move beyond just managing anxiety to fostering true autistic belonging.