
Abstract
Background:
This study empirically tests whether an imbalance between self-compassion and compassion for others influences mental health outcomes in autistic and non-autistic adults. The main hypothesis is that autistic individuals, compared with non-autistic individuals, may exhibit a greater “self–other imbalance,” which is characterized by low self-compassion and particularly high compassion for others.
Methods:
This paper describes two empirical studies (N = 677 in Study 1, N = 404 in Study 2). Participants included autistic adults (N = 290 in Study 1, N = 201 in Study 2) and non-autistic adults (N = 387 in Study 1, N = 203 in Study 2). Participants completed demographic questions and measures of autistic traits, self-compassion, compassion for others, anxiety, and depression. Data were analyzed to identify patterns of self–other imbalance and its association with mental health symptoms.
Results:
Findings of this cross-sectional study indicate that autistic adults, particularly females, exhibit a high self–other imbalance. This tendency was associated with increased symptoms of anxiety and depression, independently predicted these symptoms, and mediated the relationship between autistic traits and anxiety/depression.
Conclusions:
This study is the first to investigate both self- and other-compassion in autistic people. Enhancing our understanding of compassion in autism can inform the development of targeted psychological interventions, potentially improving the mental health and quality of life of autistic people.
Community Brief
Why is this an important issue?
Research suggests compassion-based approaches could help support autistic people with their mental health. This article looks specifically at self-compassion and compassion for others, and how these factors may influence anxiety and depression.
What was the purpose of this study?
This study explores the way we divide our compassion between ourselves and others. The main idea is that when people allocate low levels of compassion toward oneself and high levels of compassion toward others, it can negatively affect their mental health. This study introduces the concept of self–other imbalance, the balance between compassion toward oneself and others, and explores how it can affect the mental health of autistic and non-autistic people. This study also looked at whether autistic adults are more likely to experience this imbalance compared with non-autistic people.
What did the researcher do?
Two studies explored whether an imbalance between self-compassion and compassion for others affects mental health in both autistic and non-autistic adults. The studies included both autistic and non-autistic adults, who answered questions about their self-compassion, compassion for others, autistic traits, anxiety, and depression. The data were then analyzed to see if self–other imbalance was linked to mental health symptoms.
What were the results of the study?
The results from the studies suggest that self–other imbalance is more common in autistic adults, particularly in autistic women, and this imbalance is linked to higher levels of anxiety and depression.
What do these findings add to what was already known?
Autistic adults display compassion tendencies that may inadvertently contribute to mental health challenges. If autistic people have a different compassion profile compared with neurotypical people, there is a need to recognize these patterns to develop autism-friendly interventions.
What are potential weaknesses in the study?
The study used self-report questionnaires, which may be subject to biases. Also, because the study collected data at one point in time, it is difficult to understand which factor is causing the other. To understand this better, future research would need to track these patterns over time. The study results may not apply broadly because the participants came from a limited group, with little diversity in factors such as sex and ethnicity.
How will these findings help autistic adults now or in the future?
Understanding how autistic people experience compassion can help researchers and therapists develop better support strategies. By recognizing the challenges autistic people face, future mental health treatments can be more targeted toward any specific challenges and needs, which can lead to more effective well-being support and improved mental health.
Background
Autism presents a distinct neurodevelopmental profile, 1 including unique cognitive and emotional experiences.2,3 Traditional mental health models may not fully capture these experiences,4,5 highlighting the need for autism-specific hypotheses to improve understanding and interventions. This article explores self–other imbalance, the balance between self-compassion and compassion for others, as a potential predictor of mental health in autistic and non-autistic adults. It is hypothesized that autistic individuals experience greater imbalance (i.e., hyper-other-compassion and hypo-self-compassion), contributing to poorer mental health.
Defining compassion and its role in mental health
There are currently several definitions of compassion, a common thread in all of them is that they are rooted in caring motives that require a range of competencies for their enactment. 6 Compassion for others is defined as the humane quality of comprehending the suffering of others and having the desire to take action. 7 Self-compassion, then, is about comprehending our own suffering and having the desire to act. 8 Viewed from this perspective, self-compassion is the redirection of compassion inward, involving treating oneself with the same compassion offered to others. 7
Self-compassion benefits well-being, improving health behavior regulation, 9 emotion regulation, 10 happiness, and resilience, 11 while reducing stress, anxiety, and depression. 12 Studies indicate that self-compassion negatively correlates with mental health symptoms in autistic adults.13–19 One longitudinal study found that lower self-compassion predicted higher anxiety and depression at the 6- and 12-month follow-ups. 18 In addition, a 5-week self-compassion program for autistic adults 14 improved well-being while reducing anxiety and depression. These findings support the potential of compassion-based interventions to improve mental health in autistic populations.
Compassion for others is linked to prosocial behaviors, social connectedness, and improved mental health.20–22 Compassion toward others is related to, but distinct from, empathy. Much like compassion, empathy is viewed as a multidimensional construct comprising cognitive and affective components. 23 Cognitive empathy involves understanding another person’s emotions and perspective, 24 whereas affective empathy entails emotionally sharing those emotions. 25 One noticeable difference between empathy and compassion is that a drive to alleviate suffering through actions is seen as a core feature of compassion but not empathy.6,8
Goetz and colleagues 26 argued that empathy simply involves vicariously experiencing another’s emotions, whereas compassion stands as an independent emotion that has distinct appraisal processes attuned to undeserved suffering. Specifically, based on evolutionary theory and empirical evidence, the authors argued that compassion has evolved as a distinct affective experience with a primary function to facilitate cooperation and protect the weak and those who suffer. This definition suggests that compassion might be more closely linked to principled moral judgments, including fairness, equity, and justice.
Although both empathy and compassion involve understanding and responding to others’ emotions, 23 they serve different functions. Empathy allows one to feel another’s emotions, 25 while compassion motivates action to reduce suffering.6,8 Empathy can lead to compassion, but not always, since people can empathize without acting (e.g., feeling another’s pain but not helping), and compassion can exist without empathy (e.g., acting without deep emotional resonance). Thus, empathy can play some role in generating and experiencing compassion, but compassion does not reduce to an empathic state of mirrored distress, fear, or sadness. The two constructs therefore differ in phenomenology, display behaviors, and autonomic profiles,8,26 and neuroscientific evidence points toward distinct brain activations in response to compassion and empathy training. 27
Baron-Cohen28,29 argued that autistic people lack cognitive empathy or “theory of mind,” that is, the ability to infer others’ mental states and predict behavior. However, research suggests alexithymia, a difficulty identifying and understanding emotions in oneself and others, rather than autism itself, may underlie autistic challenges in recognizing emotions.30,31 Milton’s “double-empathy problem” 32 further challenges the empathy hypothesis, arguing that empathy deficits do not lie solely within the autistic individual, and when individuals from different neurotypes interact, misunderstandings and communication barriers can arise on both sides. Research shows that while autistic individuals may have reduced cognitive empathy and alexithymia, their affective empathy remains intact or even heightened. 33
Gilbert’s 34 three-system model explains how compassion regulates emotional well-being by balancing the threat, drive, and soothing systems. The threat system detects and responds to threats both real and perceived, the drive system motivates resource seeking, and the soothing system promotes contentment and safety. Compassion activates the soothing system and plays a crucial role in regulating the other two systems, especially in mitigating the overactivation of the threat system. 35 In therapy, fostering compassion can shift individuals from a threat-focused mindset to one where the soothing system is more regularly engaged. 36
Buddhist teachings view self- and other-compassion as inseparable, with the notion of a separate self-considered a delusion (termed “wrong view”).37,38 However, empirical research often examines them separately. Findings on their relationship remain mixed; some studies report a weak correlation between self- and other-compassion,39,40 others a moderate one, 41 and some none at all. 7 According to Strauss et al., 42 these inconsistencies may reflect partial independence between the constructs, definitional ambiguities, measurement shortcomings, or limitations inherent to correlational designs.
Imbalance versus harmony
This study introduces self–other imbalance, where the allocation of compassion resources between the self and others can influence well-being. Specifically, a disparity in terms of low allocation toward the self and high allocation toward others can lead to poorer mental health. This idea aligns with Neff’s view that people are often more compassionate toward others than themselves. 43 It also aligns with Gilbert’s model, 34 although suggesting that an overactive soothing system directed outward (but not inward) could fail to regulate the threat system effectively, leading to distress.
Other similar ideas for measuring and investigating self- and other-compassion have recently been put forward. Sahdra and colleagues 41 proposed the idea of “self–other harmony,” which measures the within-person correlation between self- and other-compassion. An individual is considered to have high harmony when an increase in self-compassion is accompanied by a corresponding increase in compassion for others, and vice versa, whereas for individuals with low harmony, there would be no correlation or a negative correlation. The authors argued that self-compassion could be considered a blessing for those with high harmony, but inactive or unhelpful for those with low harmony. 41
Self–other harmony differs from self–other imbalance both conceptually and statistically. Sahdra et al. analyzed harmony by examining within-person correlations, whereas this study measures imbalance using the standardized difference (D-score) between self-compassion and compassion for others. Self–other harmony assumes that well-being improves when both forms of compassion increase or decrease together. In contrast, self–other imbalance emphasizes how excessive compassion for others at the expense of self can be problematic, regardless of whether the two constructs correlate. By capturing disparity rather than fluctuation, self–other imbalance offers a more direct measure of how individuals distribute compassion, making it a more straightforward metric for identifying problematic compassion tendencies.
Sahdra and colleagues 41 argued that an increase in self-compassion accompanied by a reduction in compassion for others means a lack of harmony, and that increasing self-compassion in this situation would be seemingly unhelpful. However, this reasoning is flawed from a clinical perspective. For individuals at the extreme end of the compassion continuum, increasing self-compassion may naturally reduce compassion for others or even necessitate it. The goal in therapy is not to reduce compassion for others, but to change the client’s relationship with it and balance it with self-compassion. Working with the client to reduce problematic patterns (as is the case in the self–other imbalance model) may provide compassion relief—an alleviation of the pressure created by compassion imbalance.
This distinction between harmony and imbalance has clinical significance in relation to how change is conceptualized in therapy. Harmony focuses on increasing synchronization, implying that well-being is tied to whether these two constructs move together. Imbalance is about relative prioritization, for example, encouraging those with extreme self-sacrificing tendencies to develop self-compassion while maintaining compassion for others. Indeed, self–other harmony appears to require a more stable and adaptive emotional profile, which may not be particularly suitable for autistic populations who are known to have challenges with emotion regulation. 44 The self–other imbalance model therefore focuses on the distribution of compassion resources and how prioritizing others at one’s own expense can contribute to mental distress. Because of this focus, imbalance research offers more direct therapeutic applications and a clearer interpretative framework. Therapy should focus on addressing harmful imbalances—particularly when excessive compassion for others comes at the cost of self-compassion—rather than simply ensuring that both move in tandem, as the harmony model suggests.
The self–other imbalance hypothesis of autism
While research on self- and other-compassion in autistic people remains limited, existing studies suggest that autistic adults tend to report lower self-compassion compared with non-autistic individuals.16,18 Galvin and Richards 16 proposed that increased inward hostility in autistic people is likely to have started early in childhood and be associated with attachment processes and sustained adverse experiences across the lifespan, including increased trauma exposure, bullying, the need to camouflage one’s autistic traits, and nonacceptance from others. Beyond these individual experiences, broader sociocultural factors, including minority stress and ableism, may contribute to lower self-compassion.45,46
In the case of compassion for others, although experiencing past adversity is generally associated with negative outcomes, it has actually been linked with an increase in compassion for others. 47 The post-trauma development of compassion and the factors that might predict this trajectory are poorly understood, but in the case of autistic individuals, it is possible that they are more easily able to mentally put themselves in another’s shoes and/or that they have a strengthened willingness to extend needed resources to disadvantaged others. Goetz et al. 26 described compassion as rooted in principled moral judgments, and autistic individuals may be predisposed toward the higher end of the compassion continuum when it comes to disadvantaged others. Indeed, it is now well documented that autistic individuals possess strong moral inclinations, engage in deep thoughts and emotions, and exhibit a strong commitment to fairness and justice.48,49 Kapp 49 stated that autism may predispose individuals toward moral intuitions across dimensions such as care, loyalty, authority, sanctity, and particularly fairness.
Given these patterns, autistic people may be more susceptible to high imbalance. Thus, the self–other imbalance hypothesis of autism states that, on average, autistic people will display a highly imbalanced profile, characterized by high compassion for others and low compassion for self. Imbalance will also be present in non-autistic people, as people in the general population often report higher compassion for others than for themselves (as shown in the work of Neff and colleagues).7,50 However, this discrepancy is expected to be higher in autistic individuals.
Study 1 Hypotheses
Autistic individuals will report lower self-compassion than non-autistic people.
Autistic individuals will report higher compassion for others than non-autistic people.
Higher self–other imbalance will be more common in autistic individuals.
Self–other imbalance will positively correlate with autistic traits, anxiety, and depression.
Anxiety and depression will vary by compassion profile, with those having high self-compassion relative to their compassion for others reporting the lowest symptoms and those with low self-compassion and high compassion for others reporting the highest symptoms.
Autistic traits will indirectly relate to anxiety and depression through self–other imbalance.
Study 1 methods
Participants
The University of Warwick’s Humanities and Social Sciences Research Ethics Committee approved this study. All participants provided informed consent online. Autistic and non-autistic participants were recruited on Prolific (www.prolific.co) using the following prescreening criteria: (1) autism diagnosis, (2) no intellectual disability, (3) age 18+, (4) UK residency, and (5) equal females and males within groups. Autism status was verified through Prolific’s prescreening and on the day self-reports.
Two attention-check questions (e.g., “select disagree for this question”) were included, and participants failing both were excluded. Each participant received £1.50, with an average completion time of 8 minutes (£11.25/h). Of 730 initial participants, 32 failed attention checks, and 21 had inconsistent autism status between prescreening and self-reported data, leaving a final sample of 677 adults: 290 autistic (age range = 18–64 years [M = 33.14, SD = 10.45]) and 387 non-autistic (age range = 18–65 years [M = 36.74, SD = 10.94]). Table 1 details demographics.
Demographic Information in Study 1
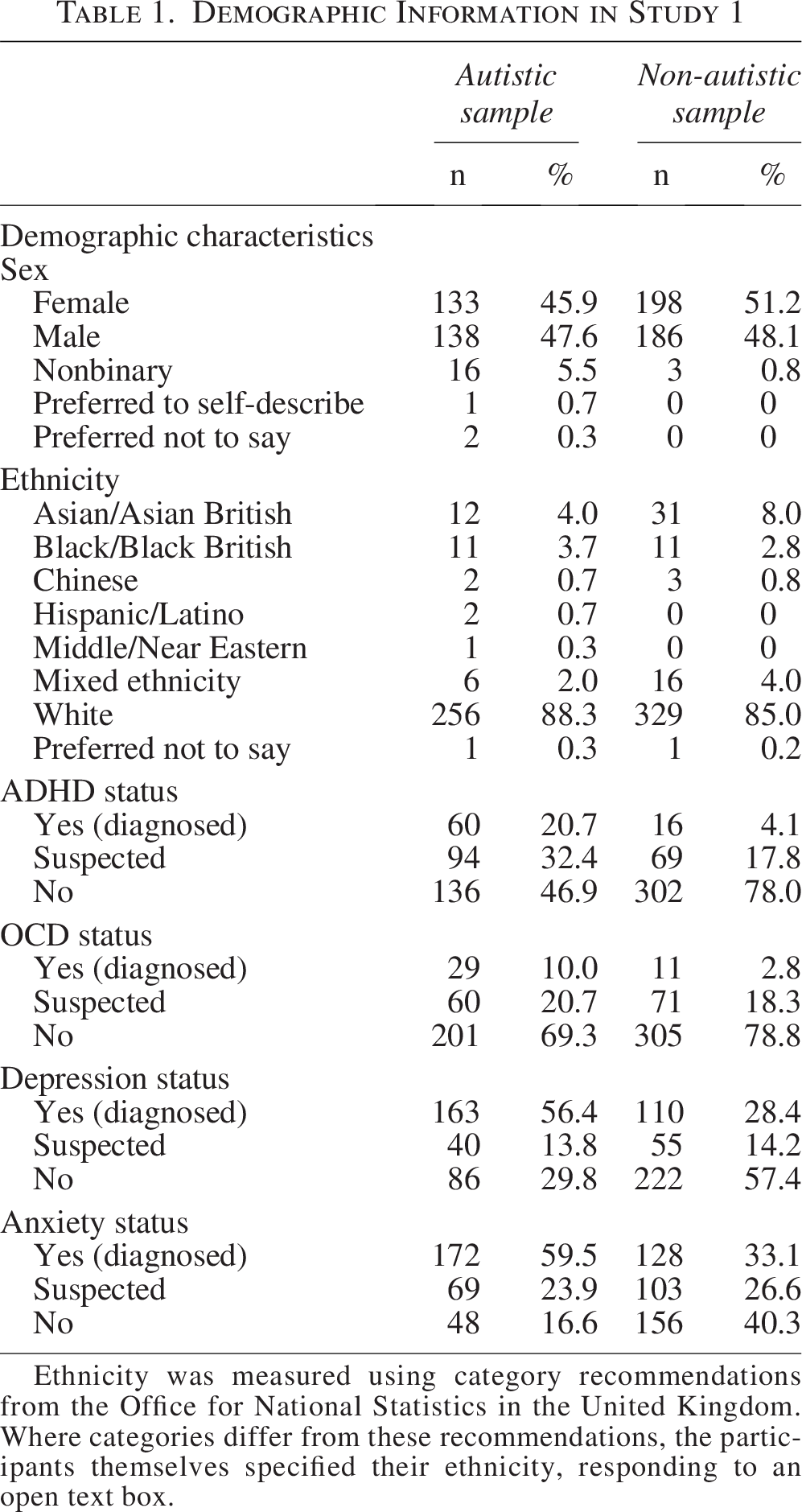
Ethnicity was measured using category recommendations from the Office for National Statistics in the United Kingdom. Where categories differ from these recommendations, the participants themselves specified their ethnicity, responding to an open text box.
Measures
Participants reported their sex, age, ethnicity, and whether they had been diagnosed with or suspected autism, anxiety, depression, obsessive compulsive disoder (OCD), or attention deficit hyperactivity disorder (ADHD). Autistic traits were assessed using the 10-item Autism Spectrum Quotient (AQ-10). 51 The AQ-10 uses a 4-point scale from 1 (almost never) to 4 (almost always). Items are scored 0 (absence of autistic trait) or 1 (presence of autistic trait), producing a total score ranging from 0 to 10, with higher scores indicating more autistic traits. Developed from the AQ-50, the AQ-10 includes the 10 most predictive items for autism diagnosis and shows good validity as a brief screening instrument. 52 It was selected for its brevity and strong correlation with the AQ-50 (r = 0.92). 51 Internal consistency in the current study was α = 0.709.
Self-compassion was measured using the Self-Compassion Scale Short-Form (SCS-SF), 53 a 12-item scale with a 5-point response ranging from 1 (almost never) to 5 (almost always). The total score is calculated by averaging the items after reverse-scoring negatively worded items. The SCS-SF has a high correlation (r = 0.98) with the original 26-item version. Internal consistency: α = 0.850.
Compassion for others was measured with the Compassionate Love for Humanity Scale Short-Form (CLHS-SF), 54 a 9-item scale (1 = not at all true of me, 7 = very true of me). Items are averaged to calculate a total score. The CLHS-SF overcomes some content shortcomings of the longer version of the scale, 55 which includes items more focused on empathy, kindness, and altruism (i.e., constructs separate from compassion). Internal consistency: α = 0.944.
Anxiety was measured using the Generalized Anxiety Disorder-7 (GAD-7) scale, 56 a 7-item scale (0 = not at all, 3 = nearly every day), which assesses the frequency of anxiety symptoms over the past 2 weeks. The GAD-7 is validated for both autistic and general populations.57,58 Internal consistency: α = 0.919.
Depression was measured with the Patient Health Questionnaire-9 (PHQ-9), 59 a 9-item scale (0 = not at all, 3 = nearly every day). Higher scores indicate more severe depression. PHQ-9 is a reliable and valid measure of depression severity in both autistic and general populations.58,60 Internal consistency: α = 0.901.
Analysis
Statistical analyses were performed using IBM SPSS version 29. Self–other imbalance was assessed using a standardized difference score (D-score):
This calculation is used to center the difference around zero and ensure that the resulting score is interpretable in terms of relative balance between the two variables. The D-score therefore captures relative prioritization rather than absolute levels of self- and other-compassion.
For the purpose of investigating patterns of compassion allocation, the approach taken here is similar to statistical approaches used previously in cognitive theories of autism.37,38 Specifically, participants were classified into five compassion types based on D-score percentiles:
Individuals in whom self-compassion is higher than other-compassion. For shorthand, S > O (or Type S). Individuals in whom other-compassion is higher than self-compassion. For shorthand, O > S (or Type O). Individuals in whom compassion for self and others are both equal. For shorthand, S = O (or balanced, Type B). Individuals with High Type S, for shorthand S ≫ O (High Type S), would display hyper-self-compassion and hypo-other-compassion. Individuals with High Type O, for shorthand O ≫ S (High Type O), would display hyper-other-compassion and hypo-self-compassion.
Participants in the bottom 20 percentiles were classified as High Type S, the top 20 percentiles as High Type O, the middle 40th–60th percentiles as Type B, the 20th–40th as Type S, and the 60th–80th as Type O. The self–other imbalance hypothesis of autism predicts more autistic participants in Type O and High Type O groups. Using percentile cutoffs (e.g., top/bottom 20%) is common in psychopathology research to identify individuals at the end of a distribution who may have qualitatively different psychological experiences. 61 Using 20% thresholds for the extreme groups (High Type S and High Type O) captures those with the most pronounced imbalances, while the middle groups (Type S, Type O, Type B) reflect more moderate variations. This five-profile structure ensures that the classification reflects meaningful variation without being overly complex, with the nuanced gradations of self–other imbalance better captured. This approach also acknowledges that the self–other imbalance exists on a spectrum—some people lean more toward self-compassion, some more toward compassion for others, and others may be severely imbalanced in either direction.
Independent t-tests compared autistic and non-autistic participants on AQ, SCS-SF, CLHS-SF, GAD-7, and PHQ-9. Pearson’s correlations examined relationships between D-score and autistic traits, anxiety, and depression. Analysis of variance (ANOVA) with Bonferroni post hoc tests assessed anxiety and depression differences across compassion profiles. Finally, mediation analyses (PROCESS tool, 62 model 4, 10,000 bootstrapped resamples) tested indirect effects of autistic traits on anxiety/depression through self–other imbalance.
Study 1 results
Table 2 presents means, standard deviations, and group comparisons for the main study variables.
Descriptive Statistics and Comparisons for the Main Study Variables (Study 1)
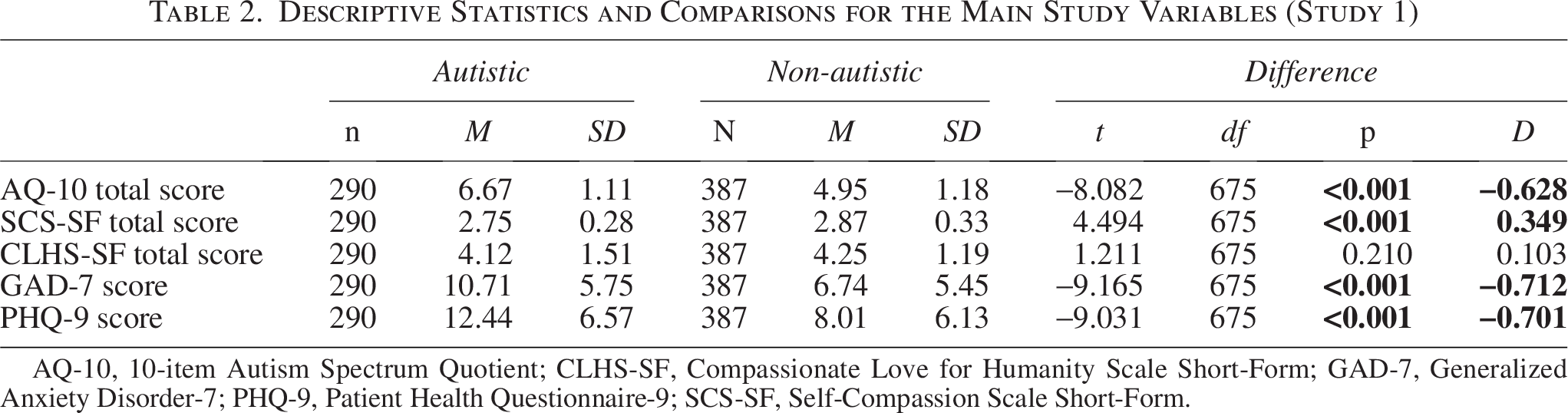
AQ-10, 10-item Autism Spectrum Quotient; CLHS-SF, Compassionate Love for Humanity Scale Short-Form; GAD-7, Generalized Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9; SCS-SF, Self-Compassion Scale Short-Form.
Hypotheses 1 and 2: Levels of self-compassion and compassion for others
Autistic participants reported significantly lower self-compassion than non-autistic participants (Cohen’s D = 0.35, p < 0.001), supporting hypothesis 1. However, there was no significant difference in compassion for others (Cohen’s D = 0.10, p = 0.21), contradicting hypothesis 2.
Hypothesis 3: Compassion profiles
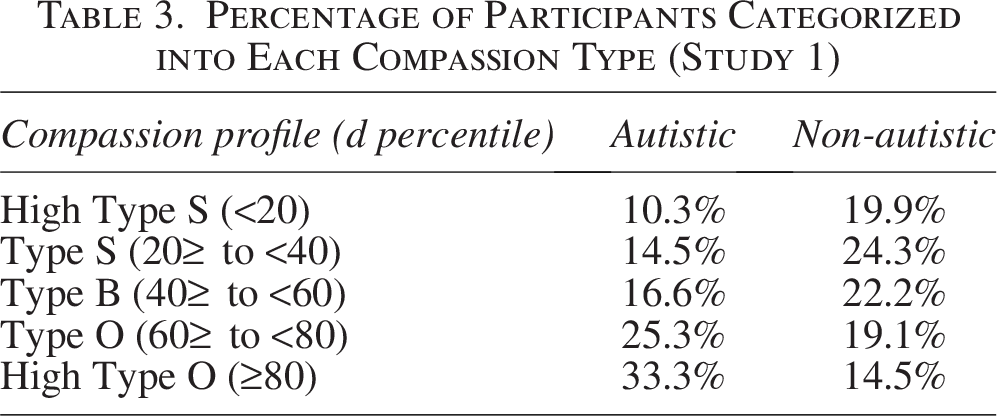
More autistic participants were classified as Type O (25.3% vs. 19.1% of non-autistic participants) and High Type O (33.3% vs. 14.5%) (χ2 = 16.60, p < 0.001), supporting hypothesis 3. See Table 3 for details.
Percentage of Participants Categorized into Each Compassion Type (Study 1)
Hypothesis 4: Correlation between D-score and autistic traits, anxiety, and depression
D-score was positively correlated with autistic traits (r = 0.175, p < 0.001), anxiety (r = 0.333, p < 0.001), and depression (r = 0.291, p < 0.001), supporting hypothesis 4.
Hypothesis 5: Anxiety and depression by compassion profile
ANOVA revealed a significant effect of compassion profile on anxiety, F(4, 672) = 7.62, p < 0.001, and depression, F(4, 672) = 5.09, p < 0.001. Bonferroni post hoc showed that anxiety scores were lowest for High Type S (M = 5.61, SD = 5.73) and increased across the profiles, reaching their highest at High Type O (M = 14.29, SD = 4.14). The same pattern appeared for depression, with the lowest scores in High Type S (M = 8.89, SD = 7.03), increasing across all the profiles, and reaching its highest in High Type O (M = 16.14, SD = 6.62). These findings support hypothesis 5.
Hypothesis 6: Indirect effect of autistic traits on anxiety/depression through D-score
Mediation analyses revealed a significant indirect effect of autistic traits on anxiety and depression through self–other imbalance. For anxiety, the indirect effect (beta = 0.135, BCa 95% CI [0.019, 0.254]) explained 17.78% of the total effect, and the direct effect remained significant (beta = 0.623, BCa 95% CI [0.275, 0.971], p = <.001). For depression, the indirect effect (beta = 0.132, BCa 95% CI [0.020, 0.255]) explained 13.58% of the total effect, and the direct effect remained significant (beta = 0.840, BCa 95% CI [0.443, 1.238], p < 0.001). These findings support hypothesis 6.
Study 2 Rationale and Hypotheses
Study 2 aimed to do the following:
Explore sex differences in self–other imbalance. Address potential methodological issues from Study 1. Determine whether self–other imbalance explains unique variance in mental health outcomes that is not explained by self- or other-compassion independently.
Sex differences in self–other imbalance
High self–other imbalance is expected to increase mental health symptoms regardless of sex or autism status. However, it is proposed that an increased risk of imbalance could be determined by these factors. Sex has been found to moderate the association between compassion (for self and others) and anxiety and depressive symptoms.63,64 Research suggests females typically report lower self-compassion and higher compassion for others than males.39,65,66 This may be due to female socialization, which can emphasize caregiving and prioritizing others’ needs. 66 For autistic females, masking pressures are known to contribute to higher rates of internalizing mental health conditions,67–69 and may amplify imbalanced tendencies. Conversely, males typically report higher self-compassion and lower compassion for others,39,65,66 which may be influenced by societal expectations of self-reliance and emotional restraint.70,71 Prior research suggests that autistic females may be particularly prone to low self-compassion compared with autistic males, non-autistic females, and non-autistic males, 16 making them more likely to fall into Type O or High Type O categories.
Conceptualization and assessment challenges
It is important to note that conceptualizations and assessment methods are just as problematic in compassion research as in empathy research. In empathy research, this has been referred to as neurotypical gatekeeping 72 and almost certainly exists in compassion research too. For instance, established measures such as the CLHS-SF may not be fully applicable to autistic individuals. Items such as “I feel a selfless caring for most of mankind” and “If a person (a stranger) is troubled, I usually feel extreme tenderness and caring” may be interpreted differently by autistic people. The first item, with its reference to “most of mankind,” suggests it is referring to the neurotypical majority and may therefore be confounded for autistic people, and, relatedly, the second item may be responded to very differently if it explicitly referred to an autistic (or neurodiverse) stranger. To address this, Study 2 involved adapting the CLHS-SF to change the target population of the “other” (i.e., to reference an “autistic stranger” rather than a generic stranger).
Another limitation in self-compassion studies is the lack of consideration for participants’ prior experiences with self-compassion techniques, whether self-guided or clinician-led. Such experiences likely shape self-compassion levels and how self-compassion relates to mental health. Study 2 accounted for this by including questions about previous exposure to self-compassion practices.
Hypotheses
A higher proportion of autistic females will be classified as Type O or High Type O than other groups.
Adapting the target population on the CLHS-SF will significantly increase scores in the autistic sample.
Self–other imbalance will independently predict anxiety and depression.
Study 2 methods
Participants
Recruitment mirrored Study 1, with participants paid £1.50 through Prolific. The average completion time was again 8 minutes. Participants completed a consent form online. Since Study 2 examined sex differences, only biologically male or female participants (per prescreening data) were invited to take part. Focusing on sex rather than gender identity allows direct comparisons with previous studies on compassion and mental health risks in males versus females.16–19,64–66 In addition, the use of a binary variable (male/female) ensures meaningful and adequately powered statistical comparisons.
After exclusions (19 failed attention checks, 17 inconsistent autism diagnosis information), the final sample included 404 participants: 201 autistic (age range = 18–65 years [M = 33.95, SD = 10.69]) and 203 non-autistic (age range = 18–65 years [M = 33.24, SD = 11.453]). See Table 4 for demographics.
Demographic Information in Study 2
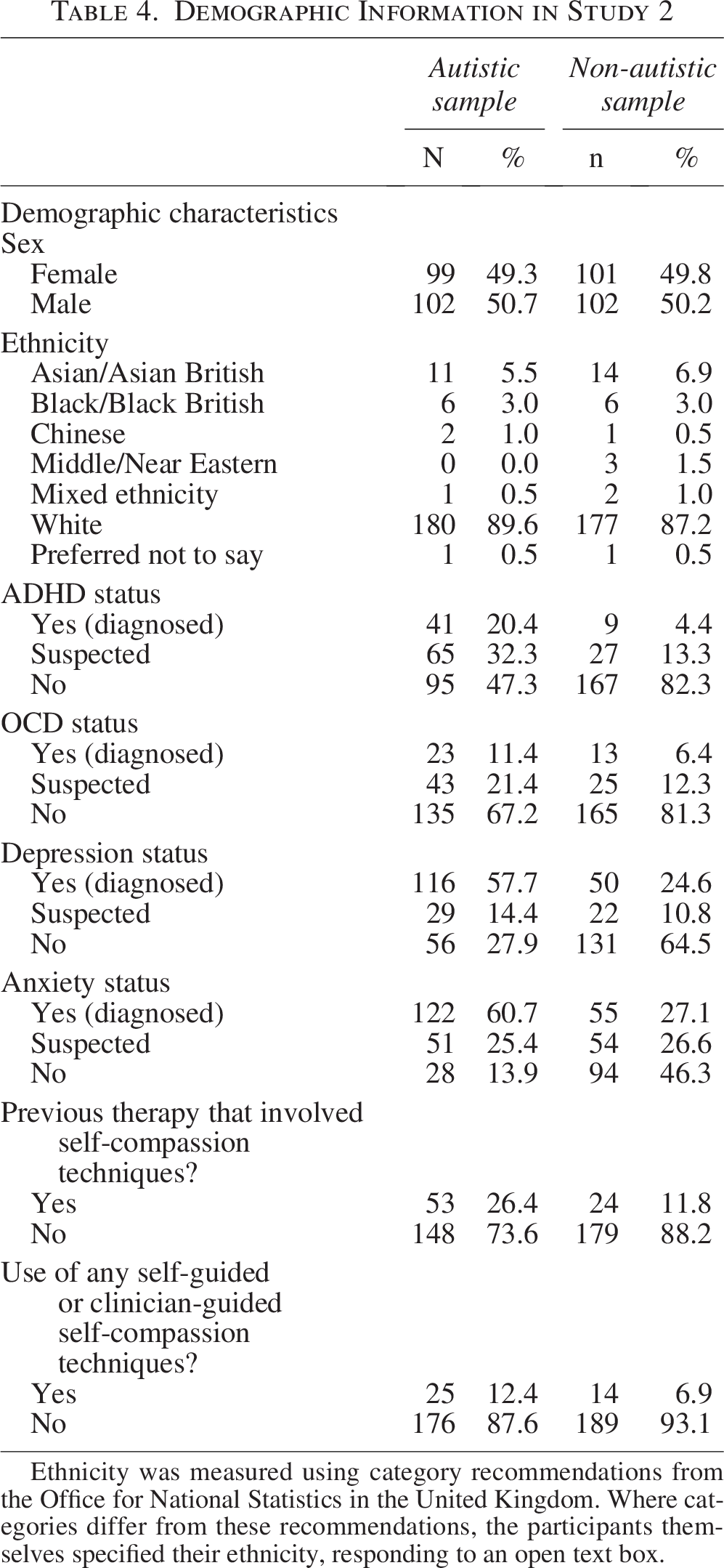
Ethnicity was measured using category recommendations from the Office for National Statistics in the United Kingdom. Where categories differ from these recommendations, the participants themselves specified their ethnicity, responding to an open text box.
Materials
Participants completed the AQ-10, SCS-SF, CLHS-SF, GAD-7, and PHQ-9. Internal consistency in Study 2 was as follows: AQ-10 α = 0.817, SCS-SF α = 0.872, CLHS-SF α = 0.946, GAD-7 α = 0.930, and PHQ-9 α = 0.910.
Study 2 involved administering both the original and an adapted CLHS-SF to the autistic sample. The original scale assesses feelings toward a stranger, whereas the adapted version specifies “an autistic stranger,” while item content remained unchanged to maintain psychometric integrity. For example:
“If a person (a stranger) is troubled, I usually feel extreme tenderness and caring”→“If an autistic person (a stranger) is troubled, I usually feel extreme tenderness and caring.” “If I encounter a stranger who needs help, I would do almost anything I could to help him or her”→“If I encounter an autistic stranger who needs help, I would do almost anything I could to help him or her.”
To confirm validity of the adapted scale, items were reviewed by an independent reviewer to ensure that adaptations retained the original meaning and relevance. Reliability testing of the adapted CLHS-SF showed it had strong internal consistency (α = 0.968). Convergent validity was supported by a high correlation between the adapted and original scale scores: r(201) = 0.892, p < 0.001. The original scale and the adapted scale also correlated similarly with outcomes: SCS-SF (original: r = 0.123, p = 0.014; adapted: r = 0.131, p = 0.010), GAD-7 (original: r = −0.047, p = 0.342; adapted = r = −0.071, p = 0.151), and PHQ-9 (original: r = −0.079, p = 0.112; adapted r = −0.038, p = 0.441). This suggests discriminant validity and indicates that the adapted and original scales were measuring the same construct.
Participants also answered: “Have you ever had any form of psychological therapy that involved self-compassion techniques?” (Yes/No) and “Do you currently use any self-compassion techniques in your life (self-guided or clinician-guided)?” (Yes/No).
Analysis
Independent t-tests compared groups on the main study variables. Participants were assigned to compassion profiles based on D-score percentiles, with analyses stratified by autism diagnosis and sex. Pearson’s correlations examined relationships, and Fisher’s r-to-z tests assessed sex differences in correlation strength. A paired t-test compared autistic participants’ score on the adapted versus original CLHS-SF, while an independent t-test compared the autistic groups’ adapted scores with the non-autistic groups’ original CLHS-SF score. Multiple regression analyses tested whether self–other imbalance (D-score) independently predicted anxiety (model 1) and depression (model 2), controlling for self-compassion, compassion for others, and prior exposure to self-compassion techniques.
Study 2 results
Table 5 presents the means, standard deviations, and comparisons for the main study variables.
Descriptive Statistics and Comparisons for the Main Study Variables (Study 2)
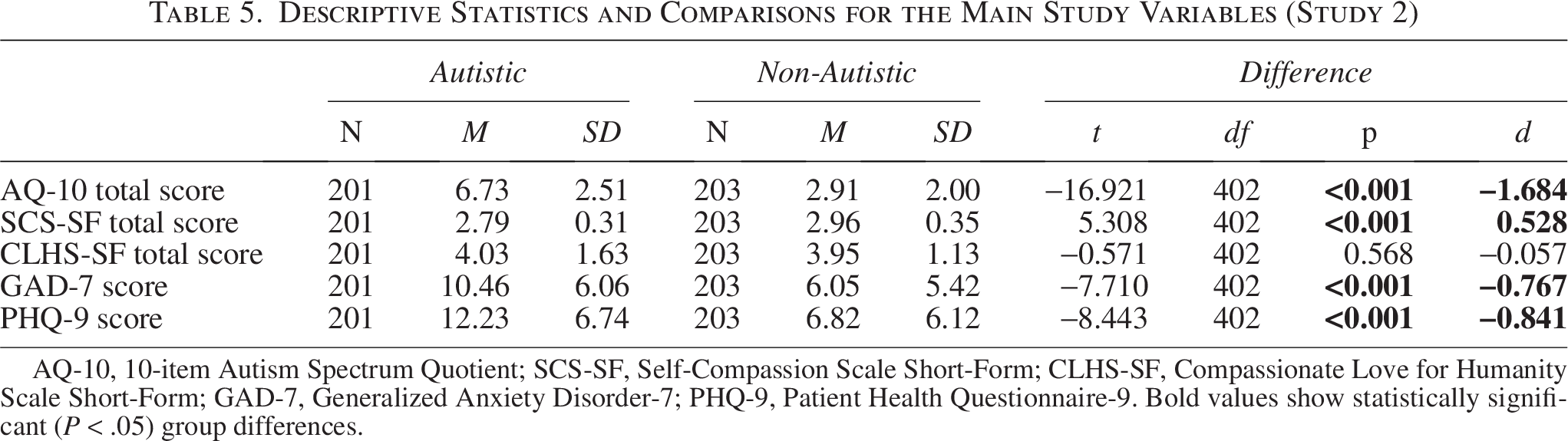
AQ-10, 10-item Autism Spectrum Quotient; SCS-SF, Self-Compassion Scale Short-Form; CLHS-SF, Compassionate Love for Humanity Scale Short-Form; GAD-7, Generalized Anxiety Disorder-7; PHQ-9, Patient Health Questionnaire-9. Bold values show statistically significant (P < .05) group differences.
Supporting hypothesis 7, a higher proportion of autistic females were categorized as High Type O (36.4%), followed by autistic males (18.6%), non-autistic females (17.8%), and non-autistic males (8.8%). More autistic males were classified as Type O or High Type O (combined 44.3%) compared with non-autistic males (combined 20.6%). Non-autistic females also had a higher percentage of Type O or High Type O classifications (combined 42.6%) than non-autistic males (combined 20.6%) (Table 6).
Percentages for Each Compassion Profile Stratified by Autism Diagnosis and Sex

Controlling for prior self-compassion experience, D-score correlated positively with autistic traits (rpartial = 0.169, p < 0.001), anxiety (rpartial = 0.406, p < 0.001), and depression (rpartial = 0.307, p < 0.001), thus replicating the findings of Study 1. Fisher’s r-to-z tests revealed no significant differences between autistic and non-autistic samples in correlations between D-score and autistic traits (z = 0.02, p = 0.984), D-score and anxiety (z = −0.41, p = 0.681), or D-score and depression (z = −0.41, p = 0.681). Similarly, males and females showed no significant differences in these relationships: D-score and autistic traits (z = −1.35, p = 0.177), D-score and anxiety (z = −1.31, p = 0.190), and D-score and depression (z = −1.00, p = 0.317).
Table 5 shows that autistic participants reported significantly lower self-compassion than non-autistic participants (Cohen’s D = −1.68, p < 0.001). However, as in Study 1, no significant difference in compassion for others was found using the original CLHS-SF scale (Cohen’s D = −0.06, p = 0.568). With the adapted CLHS-SF, autistic participants reported significantly higher scores (M = 4.66, SD = 1.62) than their scores on the original scale (M = 4.03, SD = 1.63) (paired t[200] = 8.954, p < 0.001) and the non-autistic participants’ original scale scores (M = 3.95, SD = 1.13) (independent t(402) = 4.396, p < 0.001), supporting hypothesis 8.
Recalculating D-scores with the adapted scale increased Type O and High Type O classifications among autistic participants: Autistic females: Type O +5.6%, High Type O +6%; Autistic males: Type O +3.2%, High Type O +2.4% (using the percentages reported in Table 6 as baseline).
Multiple regression analyses confirmed that self–other imbalance (D-score) independently predicted unique variance in anxiety and depression, supporting hypothesis 9. Model 1 explained 26.8% of the variance in anxiety (p < 0.001), and model 2 explained 18.0% of the variance in depression (p < 0.001). In both models, D-score emerged as the strongest predictor (see Table 7).
Multiple Regression for Anxiety (Model 1) and Depression (Model 2)
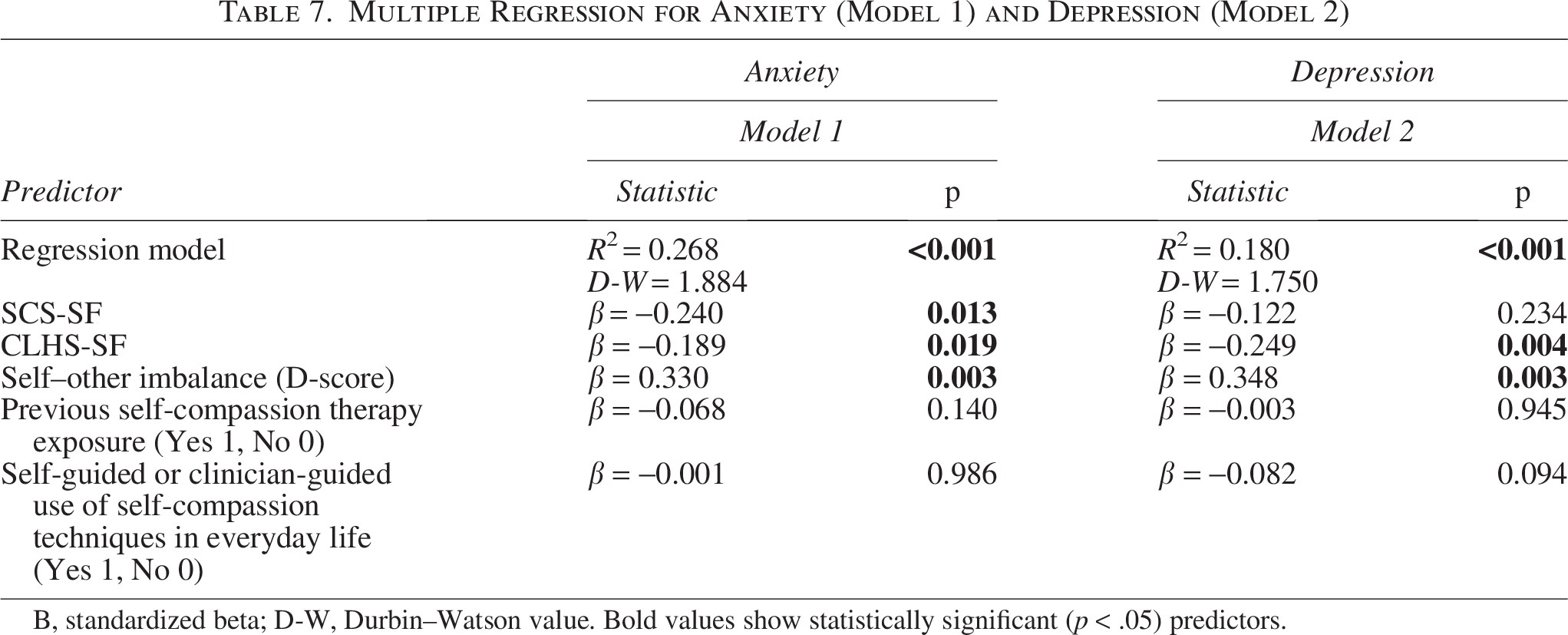
Β, standardized beta; D-W, Durbin–Watson value. Bold values show statistically significant (p < .05) predictors.
Discussion
This study is the first empirical investigation into the self–other imbalance hypothesis of autism. The findings suggest that an increased imbalance, favoring other-compassion over self-compassion, may be a distinguishing feature of autistic cognition in adulthood. Study 1 showed that self–other imbalance was correlated positively with autistic traits, anxiety, and depression, supporting the idea that an overemphasis on compassion for others at the expense of self-compassion may contribute to poorer mental health. The compassion profile analysis further reinforced this notion, as individuals with low self-compassion and high compassion for others reported the highest levels of anxiety and depression. In addition, the results of mediation analysis provided some initial evidence that self–other imbalance may act as a pathway through which autistic traits contribute to mental health difficulties. Building on these insights, Study 2 showed that the self–other imbalance may be more common in autistic females, is an independent predictor of anxiety and depression, and that by modifying the target “other” on the CLHS-SF, we can yield different results in a theory-consistent direction.
The study highlights self–other imbalance as a potentially important factor for mental health. It is possible that high self–other imbalance functions as a cognitive–emotional mechanism underlying social and mental health challenges in autistic populations. In particular, the findings could help explain why autistic people often report feeling emotionally exhausted in neurotypical social settings.13,69 Indeed, there is preliminary evidence from interviews with autistic adults showing that incidents of self-criticism mostly occur during social situations. 14 Autistic people may prioritize social harmony at great personal cost, feeling obligated to prioritize others’ needs over their own. Without self-compassion to balance outward compassion, individuals may suppress personal distress to maintain relationships, 17 struggle to recognize emotional exhaustion, 44 and experience guilt when attempting self-care or setting boundaries. 13
A higher imbalance in autistic females may stem from both societal expectations and unique autistic experiences. Society generally expects women to be nurturing and prioritize others’ needs over their own. 66 Autistic females, despite their neurodiversity, may still internalize these expectations. Indeed, an increased tendency for autistic females to mask to fit in socially has been linked with lower self-compassion, 17 and may be related to self–other imbalance. Furthermore, research suggests that autistic females are more attuned to social cues and expectations than autistic males, 73 even if they too find them challenging. This heightened awareness may drive autistic females to focus on others’ emotions and well-being while neglecting their own needs and feelings in the process.
The differences observed between the original and adapted CLHS-SF provide some initial support for the idea that when autistic individuals relate to the experiences or struggles of similar others, their levels of compassion may exceed those displayed by neurotypical individuals. It is well documented in human psychology and social group dynamics that we tend to show greater connection toward those who share similarities with us, whether in terms of personality traits, experiences, or identities.74,75 While this phenomenon is not unique to autism, it may be more pronounced in autistic individuals due to the challenges they face in interacting socially with different neurotypes and their reported stronger connections with those of the same neurotype.76,77
This finding also highlights the methodological and conceptual challenges of researching compassion in autism. As this article advocates for more research in this area, it is important to remain open to revising assumptions about compassion, how it is measured, and understood. This will ensure that research avoids potentially stigmatizing assumptions and truly captures the complexities of compassion in autistic populations. Indeed, if autistic individuals lack empathy, as some have suggested,28,29 it might be an easy jump to suggest they also lack compassion. However, the double-empathy problem 32 may extend to a “double-compassion problem,” where communication barriers and misunderstandings hinder mutual compassion between neurotypes. Compassion requires both understanding another’s suffering and wanting to do something about it.7,8 The cognitive component of understanding is of particular relevance here and is possibly disrupted (in both directions) in the relations of autistic and non-autistic people.
Like the double-empathy theory, a double-compassion theory would argue that compassion difficulties should not be seen as an autistic deficit but as a two-way issue shaped by differing expectations and communication styles. Indeed, autistic expressions of compassion may differ from non-autistic expressions of compassion. Non-autistic people may expect compassion to be expressed through socially typical gestures, such as verbal reassurance or physical comfort. In contrast, autistic people may express compassion differently, for example, offering practical solutions rather than emotional validation. This difference might lead non-autistic individuals to perceive autistic people as lacking compassion, even when they care deeply and have a desire to help. Similarly, autistic individuals may struggle to interpret or accept compassion from neurotypical individuals if it is expressed in a way that feels overwhelming, intrusive, or insincere.
A broader implication is the need to shift societal perceptions of compassion, encouraging neurotypical individuals to recognize different compassion styles and promote autistic expressions of care. Fostering mutual understanding of differing compassion styles—both in autistic and non-autistic individuals—could help bridge the gap, improving relationships and mental well-being. Future research should explore (1) whether and how autistic and non-autistic individuals differ in expressing compassion, (2) how autistic individuals perceive and interpret compassion from others, and (3) how clinicians and the public can be trained to recognize and validate diverse compassion styles.
Compassion-focused therapy (CFT) 34 could provide a useful framework for developing autism-friendly interventions to address self–other imbalance. CFT is designed to help individuals regulate emotions by cultivating compassion across the three flows of compassion—self-compassion, compassion for others, and the ability to receive compassion from others. Research in non-autistic populations shows that CFT enhances psychological well-being, improves self-acceptance, and reduces anxiety and depression. 78 Techniques such as compassionate imagery, soothing rhythm breathing, chair work, and compassionate letter writing can help individuals challenge self-punishing thought patterns, reduce shame-based responses, and establish healthier emotional boundaries.79–81 Despite its effectiveness in non-autistic populations, researchers are yet to examine the potential for CFT to reduce mental health symptoms in autistic individuals. Given the distinct cognitive, emotional, and social processing differences in autism,1–3 CFT may require adaptation and autism-specific protocols to better suit autistic needs. 82
Limitations and future directions
This study focused on autistic and general adult populations, but future research should examine other groups. This includes children and adolescents, to investigate whether self–other imbalance emerges early in development or changes over the lifespan. Understanding the developmental trajectory of compassion in autistic individuals could inform early interventions and support strategies, potentially mitigating longer-term mental health challenges.
Limitations include the use of cross-sectional data for mediation and a predominantly White sample, which limits the interpretation and generalizability of results. The study did not include self-diagnosed autistic individuals and treated sex as a binary variable (male/female) to ensure adequate statistical power. Future research with larger samples should include self-diagnosed individuals and explore how gender identity, not just sex, influences self–other imbalance. This is important given the gender diversity found in autistic populations. 83
Self-report measures, although common in psychological research, may be subject to biases, particularly in autistic individuals who may find it challenging to accurately convey their internal states. The AQ-10 was chosen for its brevity, but research has criticized it as a measure of autistic traits. 84 This could potentially reduce the reliability of the mediation models, in which it was used as a predictor variable. While some steps were taken to ensure the psychometric integrity of the adapted CHLS-SF, further use would require a full validation study. While the steps taken in this study indicated that the scale measured the intended construct, the results in relation to this scale should be interpreted with caution. Furthermore, although the SCS-SF and CLHS-SF have been validated for use in clinical populations, they have not been validated specifically in autistic populations.
Finally, although standardized difference scores derived from SCS-SF and CLHS-SF were adequate for theoretical testing in this study, their practicality in research and clinical settings is limited. The nature of standardized D-scores, where group means are always zero, restricts conventional comparisons (e.g., t-tests). Examining “compassion profiles” and score distributions provides some insight, but it is far from ideal. The next step in this project is the development and validation of a dedicated scale to measure self–other imbalance more directly.
Conclusion
Autistic people may have compassionate tendencies that can inadvertently have negative effects on their mental health. The self–other imbalance framework may be useful to investigate these tendencies and could inform the design of autism-friendly psychological interventions. This is the first study to explore self- and other-compassion in autistic people. The findings show that self–other imbalance may be increased in autistic adults, particularly in females, and serves as a predictor for symptoms of anxiety and depression. Future research should build on these findings by developing direct measures of self–other imbalance and exploring its long-term impacts across different stages of life.
Footnotes
Authorship Confirmation Statement
J.G. designed the studies, collected and analyzed the data, and drafted the article. The article has been submitted solely to Autism in Adulthood.