
Abstract
Background:
Suicide is a leading cause of death for autistic people, but it is inadequately explained by theories derived in non-autistic populations. Autistic people’s perceptions of the factors underpinning suicidal experiences are vital for guiding conceptual understanding, risk assessment, and policy and clinical practice toward preventing suicide.
Methods:
We recruited 1369 autistic participants for an online survey designed through consultation with autistic people. Participants were 326 cisgender men, 718 cisgender women, and 325 transgender or gender-divergent individuals, ranging from 16 to 89 years old. We asked them to rate the importance of 19 contributing factors to their suicidal thoughts and feelings and to enter their own explanations of additional factors if desired. Alongside thematically analyzing this qualitative data, we examined whether ratings of contributing factors differed by age and gender and whether ratings statistically predicted levels of lifetime suicidality.
Results:
Loneliness, feelings of worthlessness/failure, hopelessness, and mental illness were the highest rated contributing factors to suicidal thoughts and feelings, particularly by autistic women and sex/gender minorities; ratings also differed by age. Qualitative responses indicated the complexity of suicidality, wherein autistic status influenced both the nature of the stressors (e.g., societal stigma) and cognitive-emotional states (e.g., feeling disconnected through feeling different to others) that participants identified. Greater perceived importance of bullying, difficulties accessing support, and past trauma characterized participants with experience of suicide plans or attempts.
Conclusion:
While some of the experiences and mental states identified by participants resembled those identified in non-autistic groups, the psychological profile of autistic participants and their experiences of marginalization appeared to heavily contextualize expressions of hopelessness, burdensomeness, worthlessness, loneliness, and entrapment. Autistic people vary with regard to the factors perceived to underpin suicidality. However, associations between suicidality and the perceived importance of bullying, trauma, and inability to access support highlight the necessity of societal and systemic change to prevent suicide.
Community Brief
Why is this an important issue?
Autistic people are more likely to die by suicide than non-autistic people. To change this, we need to understand why suicidal thoughts and feelings are relatively common in autistic people and why some end their lives.
What was the purpose of this study?
As part of a larger project about suicide prevention, we wanted to hear from autistic people themselves about the factors that contributed to their suicidal thoughts and feelings. Second, we wanted to see if these contributing factors differed across autistic people of different genders and age-groups. Third, we wanted to see if these contributing factors were different in autistic people who had attempted suicide.
What did the researchers do?
We designed an online survey, drawing on feedback from a large group of autistic people. The survey included 19 factors that might contribute to suicidal thoughts and feelings, which were based on existing research and suggestions from autistic people in the design phase. We asked survey participants to rate the importance of these factors and describe additional factors in their own words. Altogether, 1369 autistic people took part.
What were the results and conclusions of the study?
We found that loneliness, hopelessness, feelings of worthlessness or failure, and mental illness were rated as the most important factors contributing to suicidal thoughts and feelings. In their own words, participants said that suicidal thoughts and feelings were caused by the stress of major life events; by the strain of everyday living without support; by instances where they were victimized by others, including professionals; and by societal stigma and constant pressure to mask. Autistic people of different genders and ages differed in the factors that contributed to their suicidal thoughts and feelings. For example, cisgender women and gender-divergent participants rated being unable to access support, difficulties with family/friends, past trauma, and mental illness as more important than did cisgender men. Autistic people who had attempted suicide tended to highlight the importance of past trauma and inability to access support.
What is new or controversial about these findings?
We believe ours is the first study to directly ask autistic people about the factors that contributed to their suicidal experiences. Having a large sample meant we could look for differences related to age and gender. Our findings place responsibility for change on society and systems rather than viewing suicidal thoughts as a kind of sickness or abnormality in autistic people.
What are potential weaknesses in the study?
We cannot confirm that the contributing factors identified by autistic people really did cause their suicidal experiences. Our findings might not be relevant to autistic people with learning disabilities, people of color, or people from other countries.
How will these findings help autistic adults now or in the future?
The findings highlight that society needs to change in order to reduce suicide in autistic people. Specifically, governments must tackle the stigma and abuse that can traumatize autistic people and ensure they have sufficient and appropriate support.
Introduction
Suicide is a leading cause of death for autistic people without learning disabilities (LD 1 ).1,2 Across countries of varying incomes, lifetime prevalence of suicide ideation and attempts is approximately 1 in 10 and 1 in 37 of the general population 3 ; in autistic people without LD their lifetime prevalence is estimated at between 1 in 3 and 1 in 5. 4 While researchers have identified correlates of suicidal thoughts and behavior (STB 2 ) in autistic people (Fig. 1), few factors differentiate those who act on suicidal thoughts. This distinction is vital for preventing early, avoidable deaths since different factors underpin the transition from ideation to action.5–7
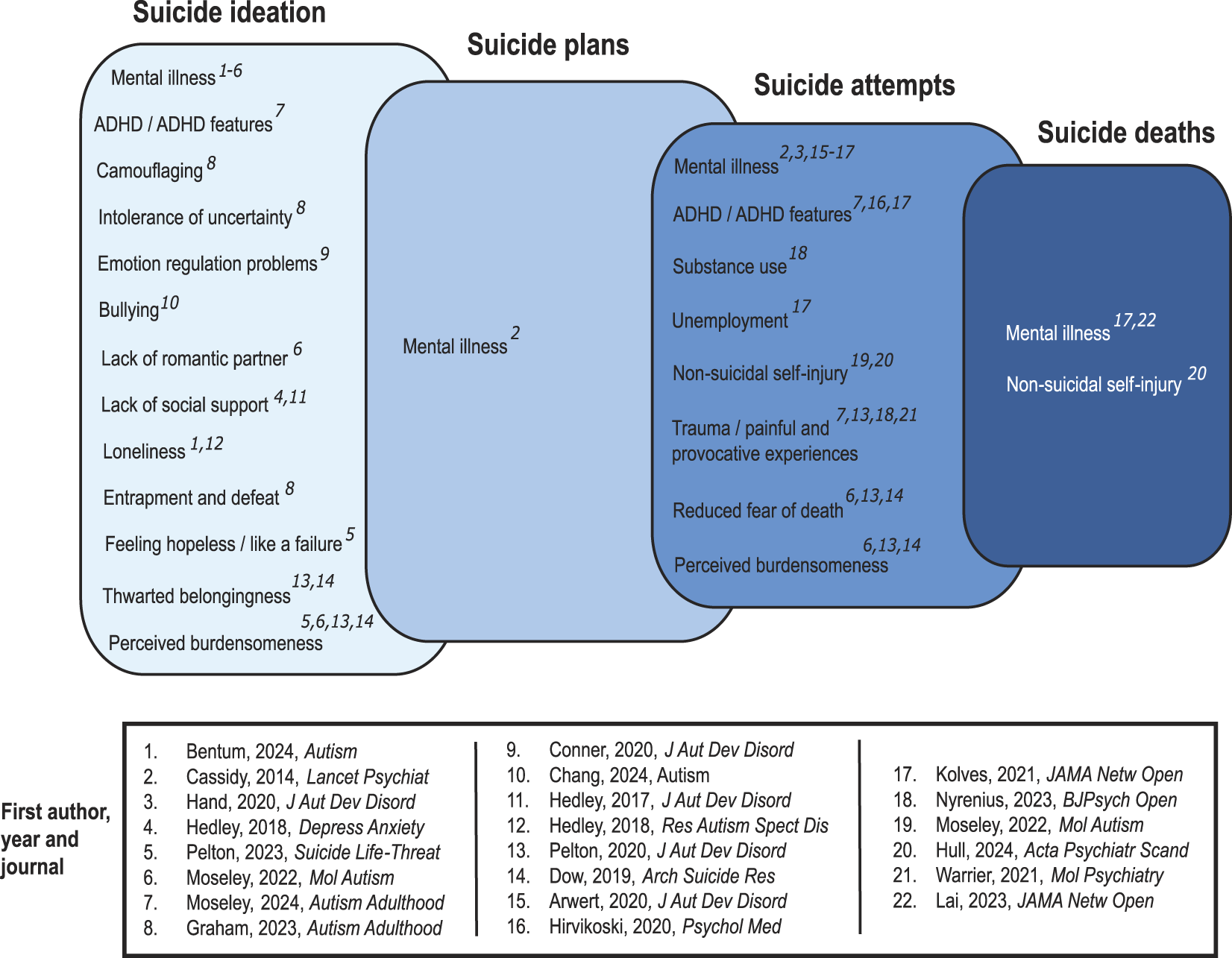
Reported correlates of suicide ideation, plans, attempts, and deaths in autistic people. We have not depicted correlates linked to “suicidality” broadly without distinctions between thoughts and behavior, or correlates whose effects, in the literature, are contradictory.
Psychological theory has guided efforts to understand, predict, and prevent suicide in non-autistic populations. 8 The interpersonal theory of suicide (ITS), 6 for example, has inspired interventions addressing the factors hypothesized to drive suicide ideation (“thwarted belongingness,” meaning loneliness and lack of belonging, and “perceived burdensomeness,” meaning beliefs that one is a burden to others). 9 Critically, it first postulated that different factors, such as reduced fear of death, enable transition from suicidal thoughts to attempts. 6 Suicide prevention in autistic people, however, is hampered by the fact that well-established theories do not necessarily apply or operate equivalently.10–14 There is some evidence that reduced fear of death does, as originally suggested, distinguish autistic people who have attempted suicide.10,12 However, thwarted belongingness only sometimes predicts suicide ideation in autistic people10,12,15 and may operate indirectly through burdensomeness and low mood. 11 Moreover, where perceived burdensomeness was originally linked to suicide ideation, 6 in autistic people it also seems important for suicide attempts.10–12 Beyond theory-derived constructs, other intrapersonal and autism-related factors, such as temperament and cognitive flexibility,1,16–19 likewise fail to consistently predict different degrees of STB in autistic people.
Autistic people’s own perceptions of the causal factors for STB are a vital source of information which is surprisingly absent from present literature. The majority of studies on suicide in autistic people have examined social-psychological constructs defined in non-autistic people.10–15,19–25 This, however, can be problematic, as shown in the case of the Interpersonal Needs Questionnaire (assessing thwarted belongingness and perceived burdensomeness), 26 because measures may not capture constructs as originally conceptualized in non-autistic populations. Autistic people allude indirectly to STB in the context of life changes and adversity,27–30 trauma, 31 barriers to support, 32 meltdowns, 33 masking, 34 burnout, 35 and living undiagnosed 36 —but we lack qualitative approaches that demonstrate how they think about STB and the causal factors underpinning it. Directly exploring the factors that autistic people endorse as important to STB may aid risk assessment and guide intervention, while facilitating conceptual understanding of whether contributing factors differ from those defined in neurotypical populations.
Herein, in a three-part analysis involving autistic participants with varying degrees of STB, we explored factors that these individuals themselves reported as important to STB. In our first quantitative and qualitative analyses, we examined how participants rated the importance of prespecified factors that might contribute to STB, and which factors they themselves identified as important.
In the second, quantitative part of our analyses, we examined whether, much like research and support priorities,37,38 perceived contributing factors to STB differ statistically by sex, gender, and age. Based on extent literature, we predicted that mental and physical illness, trauma, victimization, and unmet needs might be particularly important factors for cisgender women, transgender, and gender-divergent participants39–43 ; that academic strains and gender and/or sexual identity difficulties might be more important for younger participants 44 ; and that employment, housing, legal and financial issues, physical health problems, and bereavement might be more important for older participants. We expected victimization and loneliness to be equally important across age and gender groups, given their ubiquity.10,45–47
In the third quantitative part of our analyses, we returned to the distinction between suicidal thoughts and behaviour by examining whether differences in the perceived importance of contributing factors could statistically predict varying levels of lifetime STB, and particularly distinguish autistic people with experience of suicide attempts. In a data-driven approach without prior hypotheses, we focused on the prespecified contributing factors that had been identified as most important in the first part of these analyses.
Methods
Participants
We advertised our online survey as a call for ideas for suicide prevention (reported elsewhere 48 ), promoting it on Facebook, YouTube, Twitter/X, Instagram, and the website of the charity the Autism Centre of Excellence at Cambridge (ACE; now Autism Action). We set eligibility criteria that required autistic participants to be aged 16 or over. Following the data cleaning process (see Supplementary Data S1), we retained datasets from 1369 participants, all of whom had experience of STB, 3 and 1216 of whom completed the whole survey. Almost 94% resided in the United Kingdom (see Table 1 and Supplementary Data S1).
Sample Characteristics in Relation to Lifetime STB
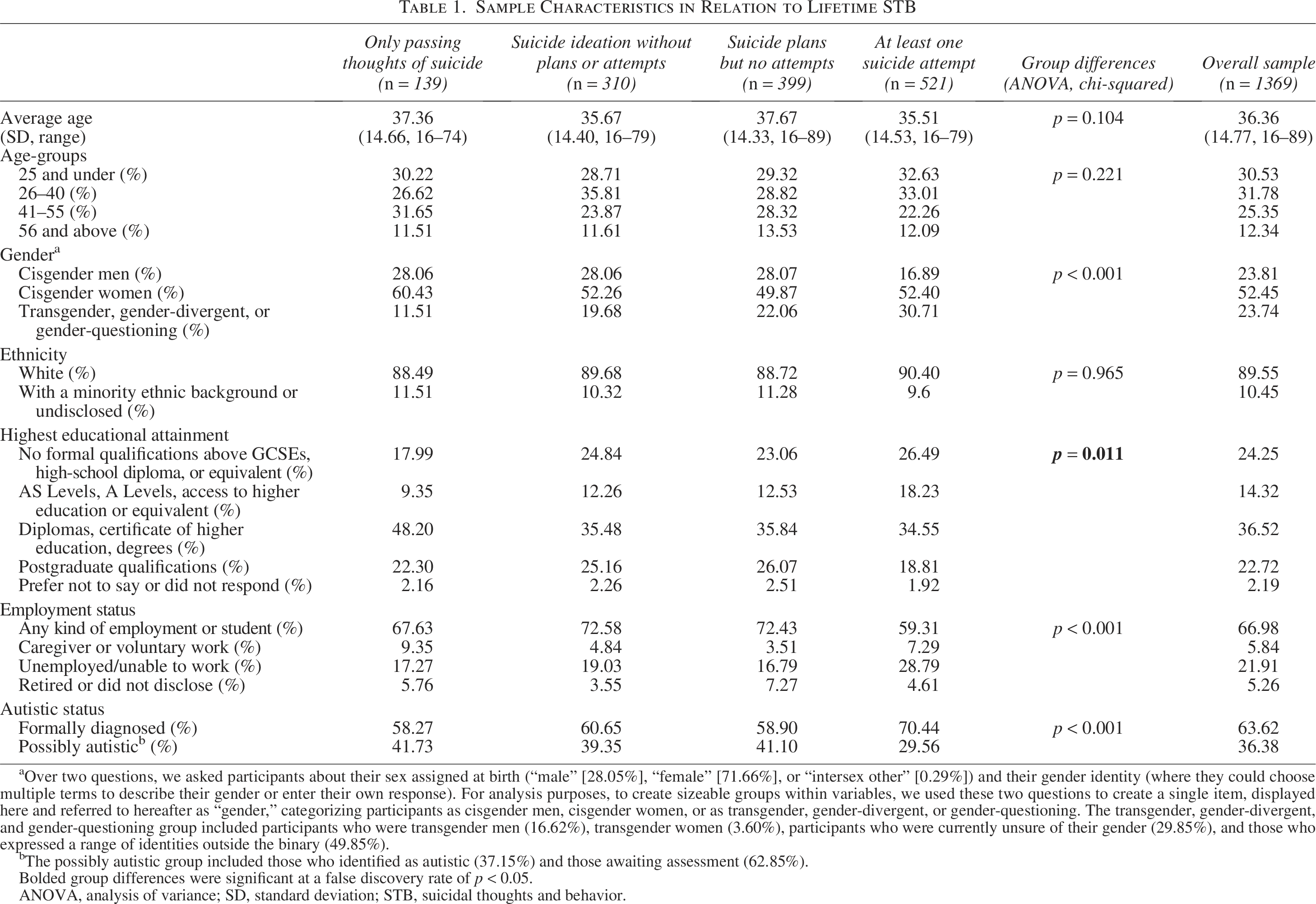
aOver two questions, we asked participants about their sex assigned at birth (“male” [28.05%], “female” [71.66%], or “intersex other” [0.29%]) and their gender identity (where they could choose multiple terms to describe their gender or enter their own response). For analysis purposes, to create sizeable groups within variables, we used these two questions to create a single item, displayed here and referred to hereafter as “gender,” categorizing participants as cisgender men, cisgender women, or as transgender, gender-divergent, or gender-questioning. The transgender, gender-divergent, and gender-questioning group included participants who were transgender men (16.62%), transgender women (3.60%), participants who were currently unsure of their gender (29.85%), and those who expressed a range of identities outside the binary (49.85%).
bThe possibly autistic group included those who identified as autistic (37.15%) and those awaiting assessment (62.85%).
Bolded group differences were significant at a false discovery rate of p < 0.05.
ANOVA, analysis of variance; SD, standard deviation; STB, suicidal thoughts and behavior.
To better understand our participant group, we conducted several initial comparisons. These showed that cisgender women and transgender, gender-divergent, or gender-questioning participants were more likely to have greater lifetime STB; so too were formally diagnosed autistic participants. Differences in the distribution of employment and education categories had less clearly discernible effects.
Materials and procedure
We incorporated suggestions from autistic people and their families in the development of our Qualtrics survey and followed guidance for safely conducting research on sensitive topics. 12 The Cambridge University Psychology Research Ethics Committee approved this survey (PRE.2022.097), and the University of Cambridge sponsored it. Most participants completed the survey within 25 minutes (median completion time was 21.6); unfortunately, we could not reimburse their time.
Through the survey, we began by asking participants demographic questions (e.g., age and gender) and “what [their] mood is like right now” (from 0 = “My mood is very bad,” to 10 = “My mood is very good”). We then asked about lifetime experience of STB (our principal dependent variable). Where a small minority of participants reported never experiencing STB, we forwarded these individuals to a later part in the survey that focused on ideas for suicide prevention (reported elsewhere48,49); these participants were excluded from present analyses. Where participants indicated experience with STB, we asked several follow-up questions to assess the extent of that experience (e.g., number of suicide attempts if relevant), as well as the factors that contributed to suicidal thoughts and feelings (our principal independent variable). Subsequently, we asked participants about their experiences of help-seeking (reported elsewhere 50 ), psychological interventions for STB, app use, and their ideas for suicide prevention. Finally, we asked participants to rate their mood again (with an average difference of −0.03 between the start and end of the study, present mood did not deteriorate significantly for most participants); subsequently, we debriefed participants and provided them with support resources. 12
We derived our key variable of interest, contributing factors to STB, from the question, “Which were the most important factors that contributed to your suicidal thoughts and feelings?” On a scale from “Not at all important/relevant” (0), “Slightly important” (1), “Moderately important” (2), to “Very important” (3), we asked participants to rate 19 prespecified items based on prior research and suggestions from autistic people during the design stage (see Supplementary Data S2). The list included concrete life events or experiences and mental states, some akin to constructs from theories of suicide. Optionally, we invited participants to enter additional factors via free text.
We predicted that contributing factors would differ as a function of gender (categorized as per Table 1) and age. In the second part of our analysis, we operationalized age as a categorical variable within a factorial design (with levels as per Table 1); in the third, regression-based part of the analysis, we treated it as continuous. To examine the effects of these independent variables, we controlled for several possibly confounding variables, including ethnicity (coded as white [0] or ethnic minority [1]); autism diagnostic status (formally diagnosed [1] or possibly autistic [0]); highest educational attainment (no formal qualifications above GCSE (General Certificate of Secondary Education) level or equivalent [1], AS/A-Level or equivalent [2], diploma, certificate of higher education or degree level [3], postgraduate level [4], or undisclosed [0]); and employment status (employed or a student [1]; caregiving or doing voluntary work [2]; unemployed [3]; retired or undisclosed [4]).
For our principal dependent variable of interest, we used a measure of lifetime STB. We assessed this as per one question from the Suicidal Behaviours Questionnaire—Autism Spectrum Conditions (SBQ-ASC 51 ): “Have you ever thought about or attempted to end your life?” We coded response options accordingly: “Never” (excluded from analyses); “I have thought about it briefly, e.g., a passing thought” (1); “I have seriously thought about ending my life, but did not plan how or try to do it” (2); “I have planned to end my life, but did not try to do it” (3); “I have made at least one suicide attempt which I planned in advance” (4); “I have made at least one suicide attempt which was not planned in advance” (also coded 4). The SBQ-ASC was created with and for autistic people. 51 During the validation process, the authors checked that autistic people interpreted these response options as the authors intended (in accordance with the definitions previously provided).
Analysis
We implemented a three-part analysis addressing the following research questions:
Part 1: What do autistic people self-report as the most important factors in suicidal thoughts and feelings?
First, we plotted the average importance of the 19 prespecified contributing factors. We also analyzed qualitative data from participants who provided free-text responses to the question about contributing factors for suicidal thoughts and feelings (n = 510: 111 cisgender men, 278 cisgender women, and 121 transgender, gender-divergent, or gender-questioning participants). We used logistic regression to briefly understand who, among our participants, was most likely to provide qualitative data (see Supplementary Data S3). These analyses indicated that older participants and people with higher levels of lifetime suicidality were more likely to have provided qualitative data. Autistic men were less likely than other gender groups to have provided qualitative data.
R.L.M. and S.J.M. analyzed the qualitative data in an inductive thematic approach, 52 consistently reflexive to their positionality as autistic with experience of STB. Having familiarized themselves with the data, both coded the first 100 quotations and generated agreed codes, which were iteratively refined through coding the remaining data. The authors discussed, refined, and agreed on their interpretations of higher-order themes through development of the thematic table. The whole research team reviewed the analysis and written narrative.
Part 2: Do ratings of importance for contributing factors differ by sex and gender, or age?
Second, we modeled the 19 contributing factors as a within-subject variable in a mixed analysis of variance. For this analysis only, listwise deletion meant that we needed to remove 46 participants who did not respond to every prespecified contributing factor. Some ignored all factors except those deemed “very important/relevant”; although this could indicate that the other, ignored factors were unimportant, we were reluctant to presume this and so removed these participants from this analysis, leaving 1323 datasets included. We modeled age (treated categorically within this factorial analysis, with levels as per Table 1) and gender identity (three levels as per Table 1) as between-subject factors. We controlled for ethnicity, autistic status, educational attainment, and current employment.
We interpreted main effects and interactions with respect to a standard alpha level of p < 0.05. Because of sphericity violations for our within-subject variable, we report Greenhouse–Geisser values; otherwise, we found that the data satisfied assumptions of normality and homogeneity of variance. We investigated significant two-way interactions 4 between contributing factors and age-group or gender with planned univariate tests (using the youngest group and cisgender men as reference categories in simple contrasts). For these, we used all participants who had rated that contributing factor and corrected alpha levels to a false discovery rate (FDR) of p < 0.05.
Part 3: Do ratings of the most important factors in suicidal thoughts and feelings differentiate between individuals with different degrees of STB?
We adopted a broad approach to contributing factors to STB in the first two parts of our analysis. In the third part, we narrowed our focus to only those prespecified factors that were rated as most important in the first part, and examined whether these could predict different degrees of STB in all 1369 participants. For the 9 (of 19) contributing factors with the highest average importance (all over 1.5), we created binary variables indicating whether (1) or not (0) participants had rated that factor as “very important” (a threshold we chose for specificity because these items were frequently endorsed with at least some degree of importance). These factors were: “Academic difficulties/stress,” “Bullying, abuse, harassment or assault” (henceforth “Bullying”), “Difficulties in relationships with family/friends,” “Loneliness or feeling disconnected/alienated from others” (henceforth “Loneliness”), “Feeling worthless or like a failure” (henceforth “Worthlessness”), “Hopelessness,” “Being unable to access support you needed,” “Mental health problems,” and “Trauma from past events” (henceforth “Past trauma”). We confirmed these 9 binary variables were independent (with the Lambda statistic, indicating the absence of multicollinearity) and then included them as predictors in three regression analyses (alpha levels corrected to p = 0.017).
In the first multinomial regression, we included just these 9 binary variables as predictors of group membership in relation to lifetime STB (a dependent variable with four levels: passing thoughts, suicide ideation, suicide plans, and suicide attempts [reference category]). Second, we repeated this analysis including gender, age (treated continuously), and our four covariates. We performed a third binary logistic regression to corroborate and more clearly delineate participants with and without lifetime suicide attempts. Here, we entered contributing factors in the first block of the model, gender and age in the second block, and covariates in the third. Before each analysis, we ensured the data met the assumptions of multinomial or logistic regression with regard to the absence of outliers and multicollinearity in continuous variables, and linearity between these and the logit transformation of the dependent variable (lifetime STB).
Results
Part 1: Factors contributing to suicidal thoughts and feelings
Of prespecified factors, participants rated Mental health problems, Loneliness, Worthlessness, and Hopelessness as most important (Fig. 2A). These and other factors were reflected and enriched in the qualitative data, which demonstrated the multifactorial and complex nature of STB. We interpreted four interrelated themes, some with subthemes and sub-subthemes, in the data (Fig. 2B; thematic table in Supplementary Data S4).
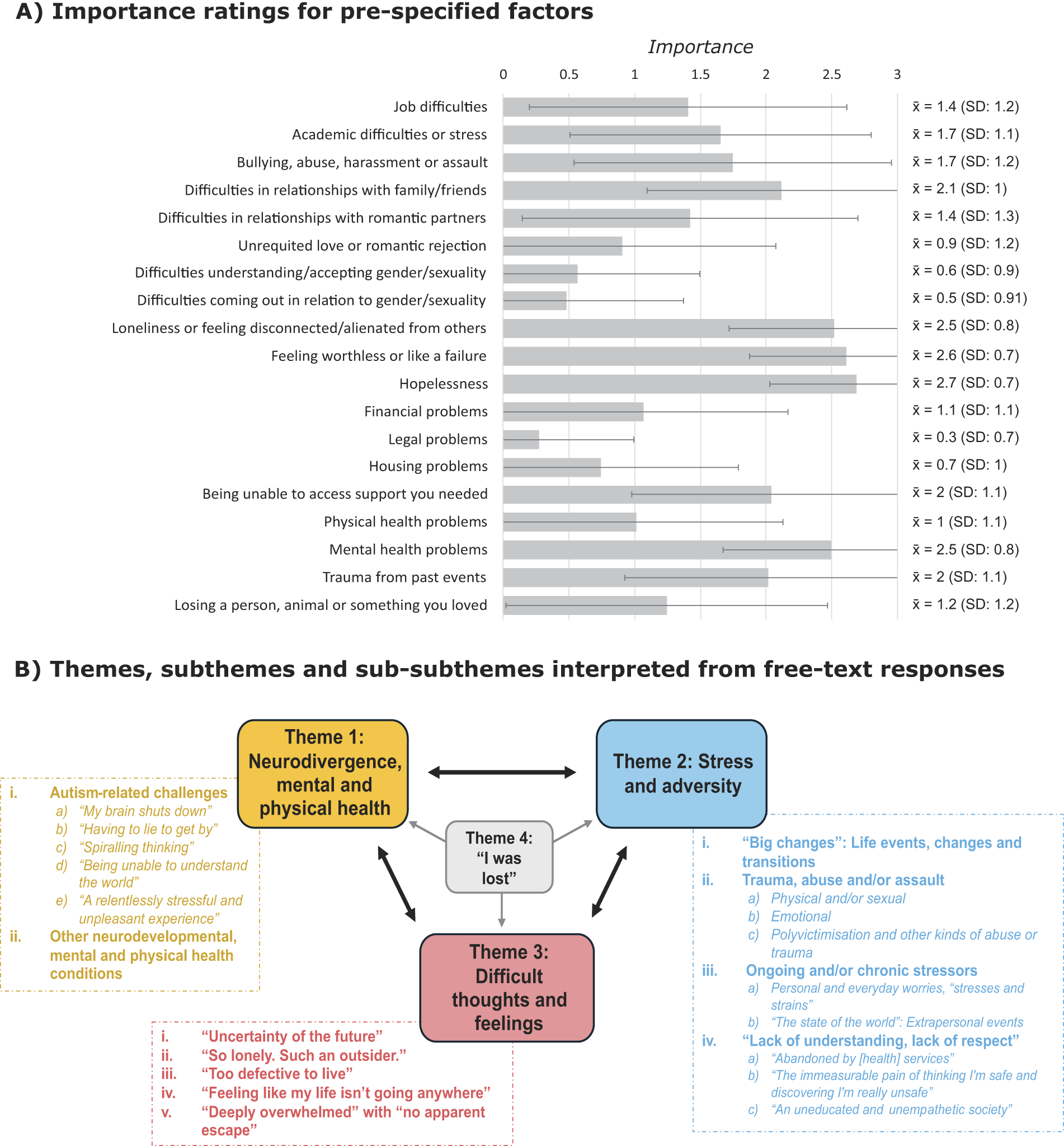
Factors that contributed to suicidal thoughts and feelings: quantitative and qualitative data. Part
Theme 1: Neurodivergence, mental and physical health
Participants frequently alluded to neurodivergence and to mental and physical health conditions in relation to suicidal experiences, as per two subthemes.
Autism-related challenges
Frequent references to specific aspects of being autistic were reflected in five sub-subthemes. In the first, 5 “My brain shuts down,” participants described instances of sensory and emotional challenges, meltdowns, shutdowns, and burnout. Burnout severely affected daily functioning, and some had insufficient support to recover. Sensory pain/discomfort was described in terms of “assault,” “affliction,” and “overload,” and linked to navigating complex, inaccessible environments. Participants described “big,” “intense” and unmanageable emotions, and sensitivity to other people’s emotions. For some participants, emotion nonacceptance was critical:
Even if times are hard, it is not life events, but being angry at myself for not being able to control or manage my low mood that causes suicidal feelings.
In the second sub-subtheme, “Having to lie to get by,” participants pointed out the “emotional exhaustion” and identity confusion associated with masking. “Playing a character” sometimes resulted in others underestimating their needs and/or disbelieving their suicidal feelings. Negative social evaluation and resultant pressure to mask led, for one participant, to a “spiral of despair.”
In the third sub-subtheme, “Spiraling thinking,” participants described thinking patterns that could augment the impact of adversity. These included “worst-case scenario reasoning,” dichotomous thinking in the context of moral unambiguity (“breached my own ethical code”), and “obsessive and intrusive” thoughts, whether focused on self-evaluation or even a parental suicide. Some participants explained that suicidal thoughts could be “a background noise … a rhythm to rumination and loop thinking,” not necessarily related to current events. One participant mentioned suicidal thoughts as a hyper-fixation, while others linked them to being unable to access their interests.
The fourth sub-subtheme, “Being unable to understand the world,” constituted incidents where participants cited their own difficulties communicating, initiating and sustaining contact, and understanding “what is happening in important situations” or “the world in general.” They spoke of resulting estrangement from family, inability to verbalize abuse, and having services “taken away … for ‘not engaging’.”
The fifth sub-subtheme, “A relentlessly stressful and unpleasant experience,” described instances where participants linked suicidal thoughts and feelings to being autistic in a general sense.
Other neurodevelopmental, mental, and physical health conditions
Participants mentioned ADHD and a range of mental (e.g., depression, PTSD [post-traumatic stress disorder], OCD [obsessive compulsive disorder], psychosis) and physical health conditions (e.g., chronic pain and fatigue), which threatened sense of self and made life “more and more difficult to endure.” Other health-related challenges included sleep disruption, gender dysphoria, self-harm, medication side effects and withdrawal effects, and body image distress and disturbance. Some participants linked substance addiction to feelings of loneliness, hopelessness, and suicide attempts.
Theme 2: Stress and adversity
This theme described different stressors related to suicidal thoughts and feelings. While some were ratable prespecified factors in the survey, participants often expanded on the complexity and specificity of events, which were often interrelated with aspects of neurodivergence and/or health (Theme 1), mental states (Theme 3), or being undiagnosed (Theme 4). We interpreted four subthemes as follows:
“Big changes”: Life events, changes, and transitions
This subtheme describes major life events or transitions—some biological (childbirth, menopause) and others social (e.g., leaving home, relationship breakdowns, bereavement). Many described complex, multiple life changes co-occurring.
Trauma, abuse, and/or assault
This subtheme encapsulated three sub-subthemes reflecting different forms of trauma, abuse, and/or assault. The first described instances that were physical and/or (more commonly) sexual. The second described emotional abuse, from “constant criticism” to emotional neglect. The third described instances of poly-victimization and other kinds of abuse and trauma, such as traumatic deaths of loved ones through murder or suicide. One participant expressed that the prespecified item about “relationship difficulties” was not representative of the “trauma” and “sudden collapse of mental and physical health” following a partner’s infidelity, indicating that autistic people may experience trauma from a wider range of factors than non-autistic people.
Ongoing and/or chronic stressors
This subtheme reflected impacts of different kinds of stressors than those listed in the survey. Within it, we interpreted two sub-subthemes:
In Personal and everyday worries, “stresses and strains,” autistic people described feelings of “stress,” “exhaustion,” and “overwhelm” associated with everyday stressors that impacted them particularly severely, such as being a carer or parent; managing multiple roles; conflict with family; financial insecurity; working long hours; and navigating inaccessible systems and environments. The burden of everyday demands was reflected in quotes such as “the weight [of] day-to-day activities or chores such as cooking meals or doing the dishes.”
In “The state of the world”: extra-personal events, participants described feelings of “despair” and “utter powerlessness” at local, national and global events, including the COVID-19 pandemic, politics, the economy, animal welfare and endangerment, climate change, and “injustice.”
“Lack of understanding, lack of respect.”
Many participants cited instances of being misunderstood, dismissed, invalidated, victimized, and/or ostracized, attributing these to lack of understanding and/or disinterest in understanding. We interpreted three common experiences as sub-subthemes:
In the first, “Abandoned by [health] services,” participants described suicidal feelings generated by the absence, inadequacy, and inconsistency of health care, social care, and educational support. Professionals and services were described as underfunded and unequipped to understand, accommodate, and support autistic people. While one participant cited the absence of support while “waiting years” for autism assessment, another expressed the disillusionment of thinking that a diagnosis “would unlock help/support/understanding (it didn’t).”
In the second, “The immeasurable pain of thinking I’m safe and discovering I’m really unsafe,” participants described experiences where professionals or services were uncaring or actively antagonistic. The “demeaning” and “cruel” UK benefits system was frequently mentioned, with one participant feeling “interrogat[ed]” and expressing “sadness for … the way you’re looked upon by others.” Others described being disbelieved or “gaslit” by UK health care services that did not supply the help they wanted. Some participants described instances where victimization was condoned or perpetrated by those in positions of authority.
In the third, “An uneducated and unempathetic society,” participants described “omnipresent stigma,” “constant negative assumptions,” rejection, and victimization from peers, family, colleagues, and society broadly. “Not being believed” or “listened to” were frequently mentioned, as were demanding standards that participants felt they could never meet.
Theme 3: Difficult thoughts and feelings
This theme described the mental states underpinning suicidal thoughts and feelings. Some, like guilt, disappointment/regret, and dissociation, were relatively infrequent, but we interpreted as subthemes five distinct mental states, sometimes co-occurring and accompanied by hopelessness. Interrelatedness between themes was again strongly evident: for example, participants linked sensory pain (Theme 1) to feelings of “massive disconnect,” being “from another world” and being “trapped”; lack of support (Theme 2) to feelings of burdensomeness; trauma, abuse/assault, daily stressors, and antagonistic relationships with services (Theme 2) to feelings of helplessness and entrapment; being late- or undiagnosed (Theme 4) to feeling broken and different.
“Uncertainty of the future.”
Some participants suggested fear of future events contributed to their suicidal thoughts. These events included certain eventualities, such as leaving school, parents’ death, fears of their own death, illness, or old age, and also less certain eventualities, like job loss due to “being unable to keep up with demands.”
“So lonely: Such an outsider.”
Expressing something beyond the prespecified “Loneliness” item, many comments reflected a deeper and pervasive sense of unbelonging, of being unwanted and different from others. While some comments reflected the perceived absence of relationships and people who cared about them (“I’ve…never been loved by an adult human since my nan died”), others expressed feeling disconnected by (or rejected due to) the fundamental, unending, and unsurpassable difference of their neurotype. Feeling like “an alien” and “not fit[ing] into the world” were common expressions.
“Too defective to live.”
Similarly expressing something beyond the “Worthlessness” survey item, this subtheme captured “all-pervasive” feelings of worthlessness and self-hatred, expressed as being “broken,” “inadequate,” “redundant,” “stupid,” “useless,” “bad,” “a failure at life.” Some participants explicitly expressed being burdensome to others, or that they negatively impacted those they loved (“I seemed to hurt people when I was only trying to be good. It felt better to go”). These statements often co-occurred with expressions of loneliness and disconnection (“I remember each time feeling very alone and as though the world was an alien world I could not understand or navigate and I was only being a burden to others or getting myself into pickles”).
“Feeling like my life isn’t going anywhere.”
Some participants expressed a lack of meaning or purpose in their lives (“I have no goal and I am useless”), which was sometimes weighed up against the difficulties of living (“The prospect of having to live my life barely scraping by, with no energy or will left to enjoy anything, seems so completely unappealing”).
“Deeply overwhelmed” with “no apparent escape.”
Participants in this subtheme linked suicidal thoughts, and indeed attempts, to feelings of “overwhelm,” “exhaustion,” and/or being “unable to cope,” a sense of total defeat and entrapment in unbearable circumstances. Suicide was situated by some participants as an (/the only) escape, as a means of “switch[ing] off,” “a reprieve,” “ongoing relief,” or getting “things to stop.” These feelings also occurred in conjunction with the other states (“Feeling as though I don’t fit into this world but knowing I have no choice. I can’t continue to do what’s expected. Feeling that I can’t talk to anybody. Hopelessness”).
Theme 4: “I was lost”
Participants frequently referred to being late- or undiagnosed, sometimes implicitly (e.g., expressing confusion about their differences or difficulties), sometimes by making explicit connections between being undiagnosed and feeling different, “broken” and confused, lacking support, receiving inappropriate support, and/or being victimized. Some participants cited the turmoil of receiving their diagnosis (which, for instance, they felt vindicated the cruelty of others) without any post-diagnostic support.
Part 2: Gender and age differences in factors contributing to suicidal thoughts and feelings
Autistic people rated contributing factors as differentially important in their suicidal experiences (F [13.47, 17608.42] = 32.03, p < 0.001, partial η2 = 0.02). Main effects 6 showed that autistic people of different genders (F [2, 1307] = 17.29, p < 0.001, partial η2 = 0.03) and different ages (F [3, 1307] = 9.34, p < 0.001, partial η2 = 0.02) responded to these items differently. Two-way interactions between contributing factors and gender (F [26.95, 17,608.42] = 12.44, p < 0.001, partial η2 = 0.02), and factors and age-group (F [40.42, 17608.42] = 9.94, p < 0.001, partial η2 = 0.02), reflected that the magnitude of group differences differed across items. A significant three-way interaction involving gender and age-group, due to low numbers, should be cautiously interpreted (see Supplementary Data S5). We display planned comparisons for gender and age in Figure 3, with statistical notations provided in Supplementary Data S6.
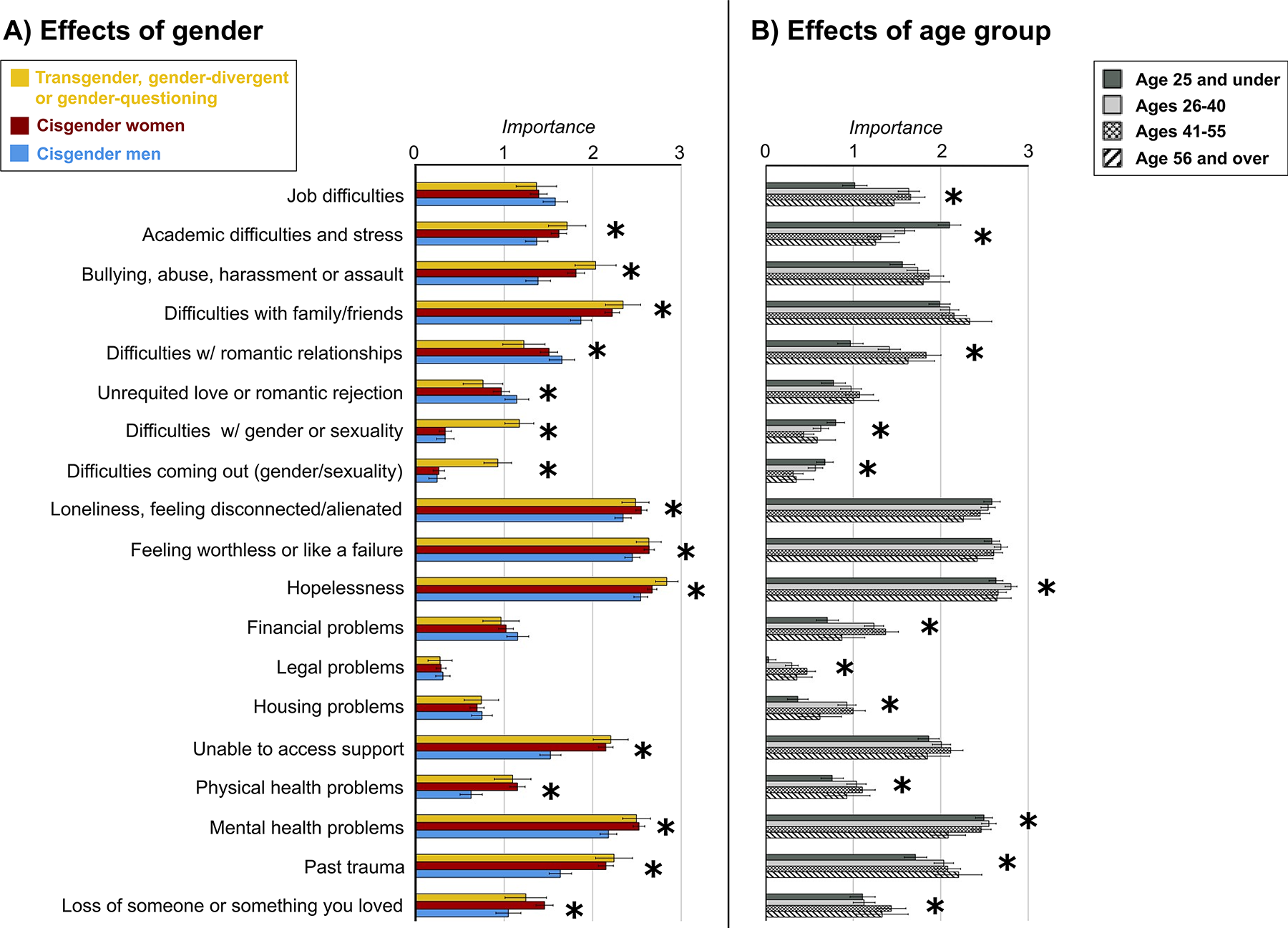
Main effects of gender
In summary, cisgender female and transgender groups perceived Academic difficulties and stress, Bullying, Difficulties with friends/family, Hopelessness, Being unable to access support; Physical health issues; Mental health issues, and Past trauma as more important to their STB than did cisgender men. The transgender group was also differentiated from cisgender men by the importance of items related to gender/sexuality, while cisgender women differed from men in the importance of Loneliness, Worthlessness, and Loss/bereavement. Cisgender men rated Difficulties with romantic relationships and Unrequited love/rejection as more important than the other groups. For age, younger participants tended to rate Academic difficulties and gender/sexuality items as more important than older groups; in contrast, they tended to rate as less important Job difficulties, Difficulties in romantic relationships, Financial, Legal and Housing problems, Physical health problems, and Past trauma. The 26–40 age-group rated Hopelessness as more important than other groups.
Part 3: Contributing factors as predictors of lifetime STB
In the first model, the nine contributing factors predicted 14% of the variance in lifetime STB (χ2[27] = 193.30, p < 0.001; Nagelkerke R2 = 0.14). Variables that significantly differentiated between levels of lifetime STB were high importance of Bullying, Hopelessness, Being unable to get support, Mental health problems, and Past trauma (see Table 2 and Supplementary Data S7 for full statistical notations). Participants who had attempted suicide were distinguished from other groups by their greater likelihood of rating Past trauma and Being unable to get support as very important. The importance of Bullying significantly differentiated between those who attempted suicide versus those with suicide ideation and brief passing thoughts of suicide, but not between individuals with suicide plans and those who had attempted suicide. The importance of Hopelessness and Mental health problems only differentiated between those who had attempted suicide versus those with only passing thoughts of suicide. These associations were unaffected by the inclusion of gender, age, and covariates in the second, adjusted model (Supplementary Data S7).
Multinomial Regression: Significant Relationships Between Perceived Importance of Contributing Factors and Lifetime Suicidality
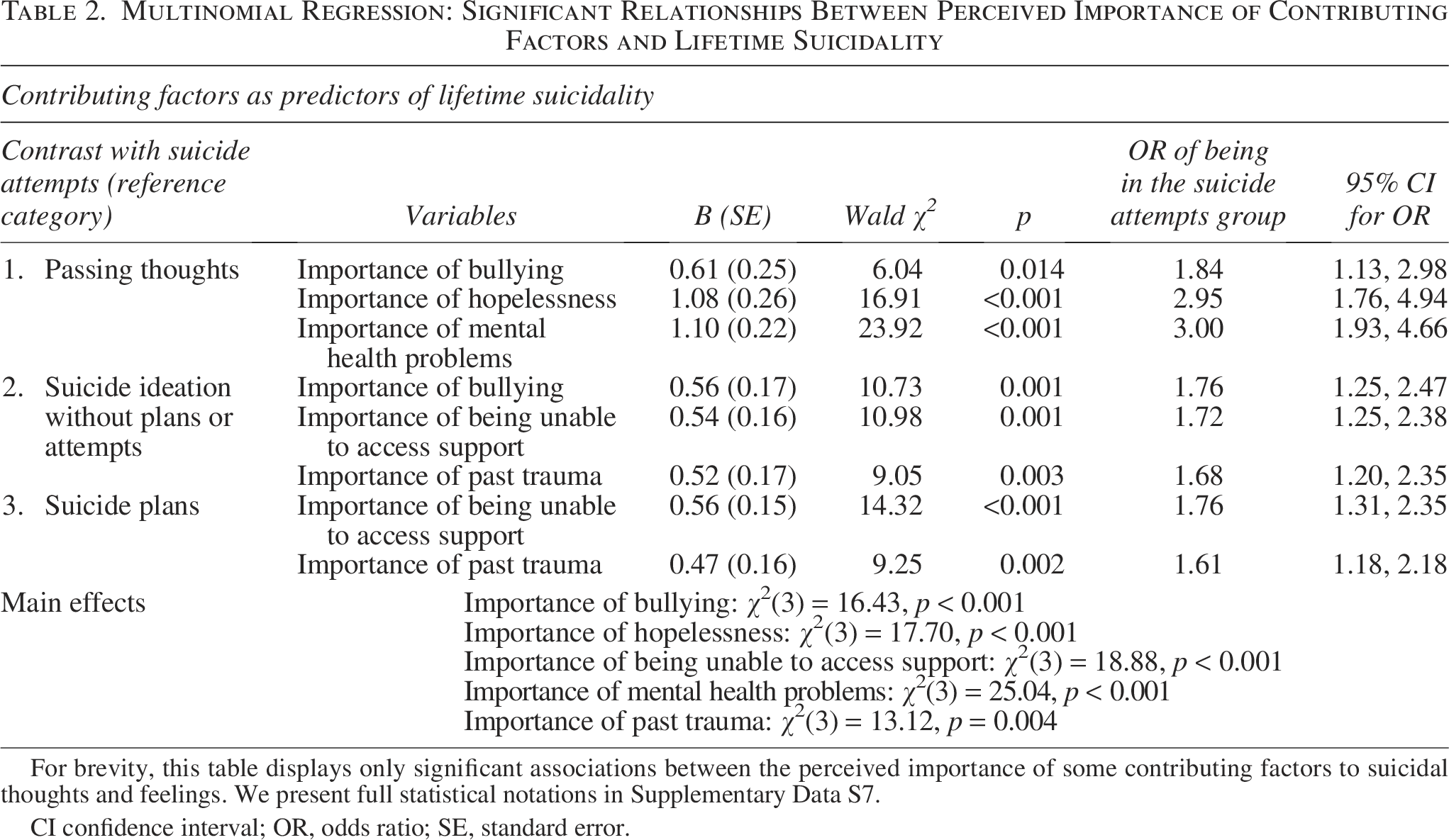
For brevity, this table displays only significant associations between the perceived importance of some contributing factors to suicidal thoughts and feelings. We present full statistical notations in Supplementary Data S7.
CI confidence interval; OR, odds ratio; SE, standard error.
Confirmatory logistic regression corroborated that only the importance of Being unable to access support and Past trauma differentiated between those with and without lifetime suicide attempts (see Supplementary Data S8).
Discussion
Through exploring the self-reported factors underpinning STB, their divergence across age and gender groups, and their ability to discriminate between autistic people with different degrees of lifetime STB, we hoped to advance conceptual understanding of suicide in an autism-specific context. We discuss our findings in light of clinical and policy implications for suicide prevention.
Contributing factors resemble yet apparently diverge from theory-derived constructs
The centrality of mental ill-health, loneliness/social disconnection, feelings of worthlessness/failure, and hopelessness to STB was consistent with previous accounts from autistic people 32 and studies using standardized measures of these constructs in autistic populations.11,12,22,23,53–55 These items also appear supportive of constructs from psychological theory, including thwarted belongingness and perceived burdensomeness, 6 conceptually akin to “loneliness” and “worthlessness” in our quantitative data. Both thwarted belongingness and perceived burdensomeness have been linked to STB in autistic people,10–12,14 but standardized measures to assess them operate differently in autistic and non-autistic people. 26 In that we did not directly assess participant perceptions of thwarted belongingness and perceived burdensomeness (or other constructs from psychological theory), we have limited ability to identify differences in their conceptualization across autistic and non-autistic people. This said, there are clues in our qualitative data that may explain the aforementioned measurement invariance 26 and indicate differential manifestations and experiences of these two constructs.
Thwarted belongingness and perceived burdensomeness 6 appear to be reflected in qualitative subthemes, “‘So lonely…’” and “‘Too defective…’”—albeit with additional elements not apparent in the original constructs and tests designed to measure them. A sense of “disconnection by difference” (where our participants felt that their “alienness” and features such as sensory sensitivities caused a “massive disconnect” from others) is not obvious in the original thwarted belongingness construct. Similarly, a sense of chronic, unfavorable comparison with non-autistic others (“feeling ‘less than’ other people”; “incompatible with the expectations of being alive as a human being”), sometimes occurring in the context of being undiagnosed, is not immediately consistent with typical descriptions of perceived burdensomeness as an acute state. The fact that these states were almost always connected by participants to intrapersonal and/or interpersonal experiences associated with being autistic is also suggestive of differences in the way these states develop and manifest.
Since previous studies cast doubt on the validity of ITS constructs and their assessment tools in autistic populations, 12 these findings are useful in suggesting that these constructs are highly relevant for autistic people but would benefit from recontextualization through an autism-informed, trauma-informed, and minority stress 7 framework. Where autism might, for instance, be interpretated within an ITS framework as one of many “risk factors” (like mental illness) for development of these states, 6 this perspective narrows focus to the pathologized individual, making no demand for social and systemic change. Similarly, the original emphasis on perceptions of unbelonging and burdensomeness fails to engage with the reality of implicit and explicit stigmatization, discrimination, victimization, and ostracism of autistic people.45,56,57 Given the highlighting of societal and systemic gaps, inequities, and injustices as driving factors for STB in both the quantitative and qualitative data, theories and suicide prevention efforts limited to intrapersonal factors and the person’s own interpersonal connections will be less than fully helpful for autistic people.
Beyond the ITS, the qualitative data were supportive of other theoretical approaches relevant for interventions and support. The subtheme “‘Deeply overwhelmed’…” appeared consistent with the integrated motivational-volitional (IMV) model of suicide, 7 which situates suicidal thoughts and intentions in feelings of inescapable defeat and/or humiliation, such as might arise from social rejection and social comparison. There is support for this model in autistic adults, 20 and external entrapment (e.g., pressure to mask) was accompanied and sometimes augmented by internal entrapment (e.g., “sticky” autistic thought processes). 7 Also compatible with the IMV was the subtheme “‘Feeling like my life isn’t going anywhere,’” where participants spoke about the absence of meaning, enjoyment, and purpose to balance out the “difficulty” of living—protective factors, through an IMV lens, which decrease the likelihood of entrapment progressing to suicide ideation. 7 The subtheme is equally consistent with the three-step theory of suicide, which suggests that connections (e.g., to people, goals) tether individuals to living despite psychological pain and hopelessness. 5 Both models widen our perspective beyond the presence of suicidogenic states to the absence of protective factors, such as peer support, 58 which present targets for intervention.
These findings have clinical utility for risk formulation and safety planning with autistic people, highlighting that STB are fluid, complex, and underpinned by inter- and intrapersonal factors co-occurring with external stressors. The interaction of these elements is essential, where, for instance, traumatic and stressful life experiences common to autistic people might be compounded and augmented by their cognitive, emotional, and sensory profile (e.g., ruminative thinking, emotion regulation difficulties), and by isolation. Current UK best practice guidance stresses the importance of full psychosocial assessment to identify risk and protective factors to inform a collaborative safety plan, 59 with additional guidance available for safety planning with autistic people. 60 Clinical intervention for STB in autistic people should be similarly informed by the autistic profile and common experiences of this group, including complex trauma and polyvictimization. Understanding and respecting autistic culture 61 may reduce instances where participants felt unheard or disbelieved in clinical settings.
Contributing factors to suicide differ by gender and age
We were unable to examine intersectional differences in our qualitative data, but these were evident in responses to prespecified contributing factors. Mental and physical illness, victimization, trauma, and inability to access support loomed larger in ratings of autistic women and transgender, gender-divergent, or gender-questioning participants, corroborating poorer health and greater victimization and support barriers in these groups.39–43 The importance of hopelessness, in the transgender group, corroborated their greater levels of lifetime suicidality, and greater importance of conflicts with friends/family might be linked to the stigma these individuals experience across their lives. 40 Autistic women similarly highlighted friend/family differences, corroborating previous suggestions that these stressors might be more numerous and impactful for these individuals. 62 Their greater emphasis on loneliness is consistent with studies reporting greater loneliness in autistic women than men.46,63 Notably, other studies find autistic men equally vulnerable to loneliness,47,64,65 albeit, perhaps, at different points in their lives. 46 The focus of our male sample on romantic relationships may indicate greater distress associated with certain kinds of relationships.
While effects of age on academic difficulties, gender/sexuality difficulties, employment, financial, legal, and housing concerns, physical health, trauma, and bereavement were as expected, the absence of differences in ratings for “bullying” and loneliness confirmed the ubiquity of these issues across the lifespan.45–47 An unexpected finding, the greater importance of hopelessness among the 26–40 age-group, might reflect the decline of autism support and services into adulthood, 38 and/or the continued unfolding of social, economic, and health-related repercussions of earlier life adversity. 66 Our findings underscore the need for care to be age-, gender-, and autism-informed, mindful of additional intersectional identities which confer additional suicide risk.
Differentiating factors between suicidal thoughts and behaviors
Our analysis highlighted five factors which discriminated between participants with different levels of STB. Lower perceived importance of hopelessness and mental illness differentiated those with fleeting suicidal thoughts from all other groups, supporting studies linking mental illness to STB in autistic people.11,12,22,25,53–55,67–69 Greater perceived importance of “bullying,” difficulties accessing support, and past trauma, however, differentiated participants with higher degrees of lifetime suicidality. While we measured perceived importance of life events, thoughts, and feelings which participants might have experienced rather than the extent of exposure to these factors themselves, the findings suggest these factors may have particular significance in the ideation-to-action trajectory for autistic people.
In neurotypical people, suicide plans are important in eroding fear of death and facilitating the transition to action. 70 While participants might have had different interpretations of what constitutes a “plan,” 70 at the very least these reflect a progression from passive to active, intentional suicidal ideation, 70 and possibly greater degrees of mental rehearsal and/or preparatory action. That the importance of bullying distinguished participants with suicide plans and attempts appears supportive of the link between bullying and STB in autistic people (as indeed does our qualitative data).30,71,72 Altogether, this highlights victimization as an essential target for preventing suicidal trajectories.
Greater perceived importance of past trauma and inability to access support were the only variables which predicted suicide attempts. Trauma has been previously linked to suicide attempts in autistic people,10,14,18,73 and was a prominent feature of our qualitative data, wherein it was frequently complex, chronic, interpersonal, and perpetrated by apparent sources of support. Relatedly, in our qualitative data, inability to access support was mentioned recurrently in expressions of hopelessness, isolation, burdensomeness, and helpless entrapment in intolerable circumstances, as mirrored in other studies.32,50,74 While we cannot ascertain participants’ actual experiences, the findings indicate at least that perceiving oneself as unable to access help, and possibly feeling more distressed about this, was associated with higher lifetime suicidality. Given the many diagnosed and undiagnosed autistic adults not in receipt of services or support,38,75 this finding is an urgent call to action for policymakers, corroborating previous recognition that autistic people are a high-risk group who continue to receive insufficient support.76–78
Limitations and future directions for research and policy
Methodological weaknesses include our cross-sectional design: we cannot ratify that “contributing factors,” framed as “predictors” in statistical parlance, causally contributed to or even preceded STB. These analyses show nondirectional associations between varying levels of STB and perceptions of, rather than exposure to, contributing factors. For example, we cannot ascertain if those who did not rate bullying as highly important never experienced it, were less distressed by the experience, and/or perceived other factors to supersede lasting injuries related to bullying.
While we attempted to protect against fraudulent responses, we were unable to validate autism diagnoses or any information provided. We used a single question about lifetime experiences of suicidal thoughts/plans/attempts, asking participants to reflect on their lifetime history with STB. While autistic participants were presumed to interpret the SBQ-ASC similarly to the validation sample in the original study, 51 our use of a single item in this retrospective way, generalizing across the life course, makes it impossible to link contributing factors to specific instances within the ideation-to-action trajectory. Since our question about contributing factors was unstandardized, participants may have had different interpretations of the prespecified factors and/or response options (e.g., what it meant for factors to be “important” vs. “relevant”).
Self-report surveys are unlikely to recruit those individuals who do not want to disclose or seek support for STB. Our highly qualified, female-skewed, and white sample is not necessarily representative of autistic men (underrepresented here), people with LD, and/or ethnic minorities. Our findings are culture-bound: since nationality, culture, and ethnicity shape perceptions of STB, 79 autistic people from other countries might respond differently. We emphasize the importance of longitudinal, lifespan approaches to risk and protective factors in diverse autistic samples, and the value of first-hand accounts for our understanding of STB.
Our final reflections concern the policy implications of this work. In the United Kingdom, recent recognition of suicide risk in autistic people 77 has been accompanied by developing guidance for mental health services 76 and a review of legislation from 2009 that aimed to improve outcomes for autistic people. 78 We welcome these efforts and their focus on broader outcomes across education, employment, and health and social care, since many of the contributing factors our participants highlighted would be completely preventable by strategies such as providing effective support before and after diagnosis, tackling social isolation and societal stigma, and access barriers to employment and education. Despite promising co-developed approaches in health care, employment, and other sectors,80,81 further research is needed to inform national and international policy efforts to prevent the perfect storm of risk factors and ensure that autistic people have equal access to meaningful connections, autonomy, success, enjoyment, and purpose in life.
Conclusions
Affording a window into how autistic people think about suicide, our findings indicate that the self-reported factors underpinning STB in autistic people, while resembling constructs from psychological theory, are heavily contextualized by autistic experiences and the autistic profile. Perceived contributing factors differed by age and gender, but certain factors, like mental illness, loneliness, hopelessness, and feelings of worthlessness and failure, appeared important to all participants. Over and above this, though, we found that the importance of bullying, trauma, and inability to access support appeared to distinguish those with greater degrees of lifetime STB. These findings highlight multiple avenues through which preventative action could prevent the development of suicidal crises, most notably around addressing societal stigma, victimization, and barriers to support.
Footnotes
Acknowledgments
Foremost, we thank each and every participant for their generosity in sharing their experiences. We also thank the autistic people, and family members, and loved ones of autistic people, who reviewed and offered feedback on our survey and communications and promotional material, including members of the Community Advisory Panel of the ACE at Cambridge (now Autism Action); the ambassadors of this charity and outside organizations who aided our recruitment, including Teneo and Edmonds Elder; and the Cambridge University Psychology Research Ethics Committee, who reviewed this work.
Author Disclosure Statement
R.L.M. is a deputy editor at Autism in Adulthood. T.A.P. and J.C. contributed as employees of, and S.B.-C., I.H., and L.O. as trustees of, the ACE at Cambridge (now Autism Action), the charity that initiated the project and funded the online promotion of the survey used in this research. There are otherwise no conflicts of interest to declare for any authors.
Funding Information
The ACE at Cambridge (now Autism Action) funded the online promotion of the survey used in this research. Pro bono support was provided by Teneo and Edmonds Elder to create and circulate communications and promotional materials. E.M.W., T.P., and M.P. receive funding from the ACE at Cambridge for separate research on suicide prevention in autistic people. S.B.-C. received funding from the Wellcome Trust 214322Z18Z. For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Article version arising from this submission. S.B.-C. also received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 777394 for the project AIMS-2-TRIALS. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation program and EFPIA and AUTISM SPEAKS, Autistica, and SFARI. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article, or in the decision to publish the results. S.B.-C. also received funding from the ACE at Cambridge (now Autism Action), SFARI, the Templeton World Charitable Fund, and the MRC. We are grateful to Cambridge University Development and Alumni Relations for anonymous donations. Any views expressed are those of the author(s) and not necessarily those of the funders, (including IHI-JU2). All research at the Department of Psychiatry in the University of Cambridge is supported by the NIHR Cambridge Biomedical Research Centre (NIHR203312) and the NIHR Applied Research Collaboration East of England.
Authorship Confirmation Statement
Conceptualization: S.B.-C., C.L.A., T.A.P., S.C., D.M., I.H., L.O., D.C., J.R., and R.L.M. Formal analysis: R.L.M. and S.J.M. Funding acquisition: S.B.-C. and T.A.P. Investigation: R.L.M. Methodology: S.B.-C., C.L.A., T.A.P., S.C., D.M., I.H., L.O., D.C., J.R., R.L.M., E.M.W., M.P., T.P., and S.J.M. Project administration: R.L.M. Resources: S.B.-C., T.A.P., and R.L.M. Supervision: S.B.-C. and T.A.P. Visualization: R.L.M. Writing—original draft: R.L.M. Writing—reviewing and editing: all authors: R.L.M., S.B.-C., C.L.A., T.A.P., S.C., D.M., I.H., L.O., D.C., J.R., E.M.W., M.P., T.P., S.J.M., T.C., and H.H. The article has been submitted solely to Autism in Adulthood.
Ethics Approval and Consent to Participate
Ethical approval of the study was granted by the Cambridge University Psychology Research Ethics Committee (PRE.2022.097). All participants provided fully informed consent to take part in the study.
Consent for Publication
Consent to publish anonymized data was granted by participants.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Disclaimer
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.