
Abstract
Background:
Alexithymia—a trait characterized by difficulties in emotion processing—is of high interest in the autism field. However, the lack of validated alexithymia measures for autistic individuals limits progress. This study aimed to address this gap by examining the psychometric properties of the Perth Alexithymia Questionnaire (PAQ) across autistic and non-autistic samples. Using the PAQ, we investigated how alexithymia manifests in autistic individuals and its links with poor mental health outcomes (anxiety).
Methods:
Autistic individuals (who reported having a diagnosis from a health professional; n = 244) and non-autistic individuals (n = 383; age range: 16–62 years) completed the PAQ and a trait anxiety questionnaire online. We conducted confirmatory factor analysis, item response theory (IRT), and moderated nonlinear factor analyses to investigate the psychometric properties of the PAQ and alexithymia differences between autistic and non-autistic individuals. Regression analyses investigated the relationships between alexithymia and anxiety and whether these relationships differ for autistic or non-autistic populations.
Results:
As operationalized by the PAQ, alexithymia manifested similarly in autistic and non-autistic individuals, comprising a general alexithymia factor and five subfactors: positively and negatively valenced difficulties identifying feelings, positively and negatively valenced difficulties describing feelings, and externally oriented thinking. All factors exhibited good to excellent classical test theory and IRT-derived reliability. The PAQ did not meaningfully bias scores for autistic individuals, who reported greater alexithymia across all its components. Alexithymia predicted greater anxiety, with nuances regarding externally oriented thinking particularly for autistic individuals.
Conclusions:
For the first time, our study illustrates that all facets of alexithymia can be validly and comprehensively assessed in autistic populations. As measured via the PAQ, alexithymia manifests similarly across autistic and non-autistic individuals, and on average, autistic individuals have greater challenges across all aspects of alexithymia. The PAQ, therefore, represents a critical assessment advancement for the field, providing a foundation for future work on alexithymia and autism.
Community Brief
Why is this an important issue?
Many autistic individuals report struggling to focus on, identify, and describe their feelings, an experience known as alexithymia. People experiencing alexithymia may have challenges managing their emotions and can face mental health difficulties (e.g., anxiety). We do not know why autistic individuals are more likely to experience alexithymia. However, some researchers point to the different communication and emotional styles used by autistic and non-autistic individuals. To help autistic individuals experiencing alexithymia, it is crucial to assess it accurately. Until this study, there was no valid way of comprehensively assessing alexithymia in autistic individuals.
What was the purpose of this study?
This study wanted to know (1) whether alexithymia in autistic individuals involved difficulties attending to, identifying, and describing positive (e.g., happiness) and negative (e.g., sadness) feelings; (2) whether a commonly used alexithymia questionnaire, the Perth Alexithymia Questionnaire (PAQ), accurately measures alexithymia in autistic individuals; (3) whether autistic individuals experience greater alexithymia than non-autistic individuals; and (4) whether individuals with more alexithymia experience greater anxiety.
What did the researchers do?
We recruited 244 autistic and 383 non-autistic individuals online through a website called Prolific, who then completed the PAQ and an anxiety questionnaire. To be included as an autistic participant, individuals had to report having a formal autism diagnosis from a health professional (excluding individuals who self-identified as autistic but did not have a formal diagnosis). We then used advanced statistical analyses to answer what we wanted to know.
What were the results of the study?
The PAQ accurately and fairly assessed alexithymia in autistic individuals. Alexithymia includes multiple characteristics, including difficulties paying attention to feelings, identifying positive or negative feelings, and describing positive or negative feelings. The PAQ also does not bias scores for autistic individuals. Lastly, while autistic individuals, on average, reported experiencing more alexithymia than non-autistic individuals, this was not true for all autistic individuals.
Individuals with greater alexithymia experience greater anxiety. Interestingly, we found some evidence that autistic individuals with alexithymia may avoid focusing on their emotions to reduce their anxiety.
What do these findings add to what was already known?
There is now a valid measure of alexithymia for autistic individuals. Additionally, the findings help us better understand how alexithymia presents in autistic individuals and the impact of alexithymia on anxiety.
What are potential weaknesses in the study?
One limitation of our study is that we recruited individuals online. We were unable to verify whether autistic individuals had an autism diagnosis or not, and we excluded self-identifying autistic individuals. As such, we do not know how alexithymia presents or what it may impact in these autistic individuals.
How will these findings help autistic adults now or in the future?
We now have a way to assess alexithymia in autistic individuals. Practitioners can use the PAQ to identify which autistic clients may benefit from support around their alexithymia. Additionally, as the PAQ is freely available, autistic adults can access it to see if they experience high levels of alexithymia. In the future, more research will uncover the best ways to support autistic individuals experiencing alexithymia.
Keywords
Introduction
To react adaptively to the outside world, it is crucial to be aware of one’s own perceptions and, particularly, one’s own feelings. Alexithymia is a trait involving a set of emotion-processing difficulties that hinders one’s emotional awareness. It was first coined in the 1970s based on observations of patients with psychosomatic disorders, 1 and alexithymia has since been identified as a risk factor for a wide array of emotion-based psychopathologies, including depression, anxiety, eating disorders, nonsuicidal self-injury, substance use, and personality disorders.2–4 These links with psychopathologies appear to be partly due to the impact that alexithymia has on emotion regulation.5,6 Recent advancements have emphasized that we must explore and assess distinct processes to understand alexithymia.
As defined in the attention-appraisal model of alexithymia,7,8 alexithymia is multidimensional, comprising three interrelated facets: difficulties identifying one’s feelings (DIF), difficulties describing one’s feelings (DDF), and an externally oriented thinking style (EOT), whereby an individual has difficulty focusing on their feelings. 9 Thus, people with high alexithymia rarely attend to their emotions, and when they are, they have difficulty accurately appraising what those emotional states are (e.g., experiencing their emotions in a more undifferentiated way, such as being unsure whether an unpleasant emotion is sadness, anger, or fear). In line with brain studies suggesting that we process negatively and positively valenced emotions differently,10–12 alexithymia can manifest across both negative and positive emotional valence domains. 8
Alexithymia is a dimensional trait, with 10% of the general population having elevated levels of alexithymia 13 and clinical populations reporting much higher rates.3,14,15 Alexithymia is emerging as an important area of research in numerous clinical populations, including prominently in the autism field. While alexithymia is not a core characteristic of autism, approximately 50% of autistic individuals report experiencing high levels of alexithymia. 16 The alexithymia hypothesis of autism 17 posits that many socio-emotional challenges faced by autistic individuals may be driven by alexithymia, including differences in eye gaze 18 and empathic brain responses. 19 Furthermore, alexithymia in autistic individuals has been associated with poorer mental health outcomes, including greater prevalence of internalizing difficulties, such as depression 20 and heightened anxiety. 21 Indeed, studies have suggested that alexithymia, at least partly, explains emotional difficulties experienced by autistic individuals.20–24
The mechanisms leading to alexithymia are not well understood in neurotypical individuals, 9 let alone in autistic individuals. However, conceptually, both ability and avoidance mechanisms are hypothesized to play an important role. 25 For example, individuals may vary in their theoretical understanding of emotions or how well-developed the cognitive structures are. 26 Thus, this can dictate one’s ability to process emotions at a high level. Equally, people can differ in how much they avoid processing their emotions, often as an avoidant coping response to overwhelming emotional states. 27 Thus, this use of experiential avoidance of emotions can also dictate alexithymia levels.
From a developmental perspective, alexithymia is often attributed, at least in part, to environmental factors, such as caregivers bonding with children 28 or being encouraged to understand and share emotions. 26 Accordingly, children are more likely to experience high alexithymia if they are not provided the opportunity to receive appropriate emotional feedback. However, what constitutes appropriate emotional meaning and expression may differ for autistic and non-autistic individuals. The double empathy problem29,30 highlights that communication difficulties between autistic and non-autistic individuals are bidirectional and can stem from mutual misunderstandings. In this context, alexithymia-related difficulties in autistic individuals may be viewed as a reflection of divergent communication styles and emotional socialization. Social pressure to conform to neurotypical norms of emotional behavior—such as expectations around eye contact, tone, or verbal affect—can lead to emotional suppression and distress.31,32 Repeated criticism or invalidation can undermine emotional confidence and clarity, especially when emotional expression diverges from conventional expectations.
Moreover, internalized stigma and repeated social misunderstandings may contribute to the development of avoidant emotional coping strategies, 33 further complicating emotional expression. Autistic individuals may begin to question the legitimacy of their emotional experiences, particularly when those experiences are dismissed or misunderstood. 34 As emotional processing is shaped heavily by social context, 35 alexithymia in autism may be better understood as a relational outcome rather than an intrinsic limitation.
Research consistently shows that alexithymia is linked to emotion-related mental health symptoms such as anxiety and occurs more frequently in autistic than non-autistic individuals. These patterns may reflect the cumulative effects of miscommunication, social pressures, and cultural expectations. To offer more effective support, it is essential to deepen our understanding of how alexithymia develops and manifests in autistic individuals. Emotional communication differences, invalidating social experiences, and other contextual factors likely contribute to significant variability in emotional processing. 36 Despite this, progress is hindered by the lack of a comprehensive, validated, autism-sensitive measure of alexithymia.
Assessing alexithymia in autistic individuals
The capacity to understand and accurately measure alexithymia in autistic individuals is critical. To date, there has been a lack of psychometric tools validated to assess alexithymia in autistic individuals. Traditionally, the most widely used tool in the alexithymia field had been the 20-item Toronto Alexithymia Scale (TAS-20), 37 a self-report tool introduced in the 1990s. However, recent psychometric data have highlighted several significant psychometric issues in the TAS-20 that are present across clinical and non-clinical populations. Most prominently, its EOT items have unacceptably poor reliability, restricting the capacity to capture this aspect of alexithymia (Cronbach’s α = 0.50–0.60). 38 Importantly, the TAS-20 has been shown to have discriminant validity problems due to being confounded with measures of distress (i.e., substantial variance in the TAS-20 measures how distressed people currently are, rather than their alexithymia levels),39–43 a particularly notable limitation in autistic population.
While the TAS-20 has been frequently used in research contexts to operationalize alexithymia in autism, 16 its psychometrics have rarely been examined in autistic samples. To the best of our knowledge, there is one exception, 44 which examined the psychometric properties of the TAS-20 in a sample of 743 autistic adults. Those results highlighted significant problems with the TAS-20’s validity, with confirmatory factor analysis (CFA) of all 20 items indicating unacceptable model fit. The study suggested that 60% of the TAS-20 items (i.e., 12 of the 20 items) needed to be removed due to psychometric problems, including all eight items designed to assess the EOT facet of alexithymia. This effort resulted in the proposal of a reduced 8-item score from the TAS-20, called the General Alexithymia Factor Score (GAFS-8), as one option to assess alexithymia in autistic populations. 44 However, several issues ultimately limit the utility of this GAFS-8 score. Most prominently, the elimination of all EOT items means that the alexithymia construct is not captured in its entirety, with EOT being viewed as an essential part of the alexithymia construct by most theorists.8,9,45 The alexithymia construct is also well established as being multidimensional, and thus facet-level assessment is important for comprehensive assessments, 9 which cannot be implemented with the GAFS-8. The GAFS-8 also retains several of the items from the TAS-20 that are confounded with how distressed respondents currently are, and which have content that may inappropriately overlap with sensory sensitivity experiences in autistic individuals (e.g., “I have physical sensations that even doctors don’t understand”). Lastly, the GAFS-8 is an unofficial scoring process derived from the TAS-20 and thus requires the full TAS-20 to be accessed and administered. However, the TAS-20 is a copyrighted instrument that requires payment of a licensing fee to access and use, 35 therefore reducing its accessibility to many populations (e.g., those from disadvantaged socio-economic backgrounds). Overall, in the context of autism, these limitations highlight the pressing need for freely accessible, comprehensive, and valid alexithymia tools to be established for use with autistic populations.
The Perth Alexithymia Questionnaire
One promising option for assessing alexithymia in autism is the Perth Alexithymia Questionnaire (PAQ). 46 The PAQ is a freely available 24-item self-report measure recently introduced to provide comprehensive and robust alexithymia assessments across adults and adolescents. It was designed to assess the DIF, DDF, and EOT facets of alexithymia. A novel feature of the PAQ, in line with recent trends in the broader emotion field, 47 is that it attempts to assess alexithymia across positive and negative emotional valence domains separately. In total, five subscales can be derived from the PAQ: Negative-Difficulty Identifying Feelings (N-DIF; e.g., “When I’m feeling bad, I can’t tell whether I’m sad, angry, or scared”), Positive-Difficulty Identifying Feelings (P-DIF; e.g., “When I’m feeling good, I can’t make sense of those feelings”), Negative-Difficulty Describing Feelings (N-DDF; e.g., “When I’m feeling bad, I can’t find the right words to describe those feelings”), Positive-Difficulty Describing Feelings (P-DDF; e.g., “When I’m feeling good, I can’t talk about those feelings in much depth or detail”), and General-Externally Oriented Thinking (G-EOT; e.g., “I tend to ignore how I feel”). The valence-specific DIF and DDF subscales have the same item content (except for the valence-specific terms) to allow direct comparisons. All items can also be summed into theoretically meaningful composite scores, including a total score as an overall marker of alexithymia.
The psychometric properties of the PAQ have been tested across a range of non-clinical and clinical samples, different age cohorts, and different language versions and cultural groups, with reports of consistently high validity and reliability metrics. Factor analyses support a 5-factor model, with lower-order factors corresponding to the five intended subscales.48–54 When tested, support has also been found for a bifactor model, which includes a “general alexithymia” factor alongside the five narrow subscale factors,46,52 with all these subscales and composite scores displaying high reliability,53,54 including in autistic individuals. 55 Such findings are consistent with the conceptual multidimensional status of the alexithymia construct. 8 The PAQ has also shown a range of expected relationships with theoretically relevant constructs, including emotion dysregulation and psychopathology symptoms43,56–58 and importantly shows good discriminant validity against markers of distress. 42 Of relevance to the value of assessing both the negative and positive valence domains, studies with the PAQ in neurotypical samples have found that processing difficulties for negative and positive emotions can explain unique variance in the prediction of psychopathology.59,60
Differential item functioning in autistic samples
While these described patterns for the PAQ are promising, there are presently no studies focused on the psychometric performance of the PAQ in autistic samples. Moreover, the relative lack of factor analytic studies of any alexithymia measures in autistic samples means that, more broadly, it is unclear how alexithymia manifests in the autistic population. This can be examined directly via measurement invariance (or differential item functioning) testing of the factor structure of alexithymia measures, in turn informing not only the validity of the measure but also an understanding of the latent structure of the construct (i.e., does the alexithymia construct manifest similarly across autistic and non-autistic individuals).
Measurement non-invariance or differential item functioning occurs when responses on items are driven by factors (e.g., autistic diagnosis) other than the underlying construct of interest (i.e., alexithymia) and indicate potential biases. 61 Items may show uniform differential item functioning (i.e., individuals’ responses to an item are systematically increased/reduced regardless of their true underlying ability; differences in item intercepts; akin to scalar invariance) or non-uniform differential item functioning (i.e., items relate differently to the underlying construct for different groups; differences in item factor loadings; akin to metric invariance).
One valuable and contemporary methodology for examining the psychometric properties of the PAQ and how alexithymia manifests across autistic and non-autistic individuals is Moderated Non-Linear Factor Analysis (MNLFA). 62 MNLFA assesses differential item functioning and latent construct differences due to individual characteristics, whether continuous (e.g., age) or categorical (e.g., autistic diagnostic status), by combining the strengths of older approaches, such as multiple groups modelling and multiple-indicator multiple-causes (MIMIC) modelling. 60 MNLFA can also examine interaction/moderation effects, which is particularly useful when assessing biases that may only occur in subgroups, such as autistic females who may not fit in a male-gendered representation of autism, 63 which has led to late/missing diagnoses and suppression of their autistic characteristics. 64 Additionally, MNLFA can statistically control for differing demographic variables across groups and may show greater power when some group samples are smaller than others. 65
Lastly, MNLFA allows a direct examination into whether alexithymia manifests differently in autistic individuals compared to non-autistic individuals. This includes not only mean differences (i.e., a latent construct is more common or at a higher level in one group) but also variance differences (i.e., a latent construct varies more in one group) and covariance differences (i.e., two latent constructs are more distinct in one group). Given the importance of considering the heterogeneity of individuals on the autism spectrum,66,67 the difference in variance between autistic and non-autistic individuals could help to identify whether this heterogeneity exists for alexithymia.
The present study
The primary aim of this study is to examine the psychometric properties (e.g., latent structure, validity, and classical test theory and item response theory-derived reliability) of the PAQ across autistic and non-autistic populations. In so doing, we also aimed to use the PAQ to understand more about how alexithymia manifests in autistic populations and, replicating previous autism research, its links with poor mental health outcomes (anxiety). As part of this, we directly examined the measurement invariance (and differential item functioning) of the PAQ across autistic and non-autistic individuals, and thus the consistency of the latent structure of the alexithymia construct. Testing these hypotheses is essential for advancing the understanding of alexithymia, ensuring that the tools used are accurate and unbiased for all individuals.
Methods
Participants and procedures
Participants completed a battery of questionnaires online through Qualtrics, including the PAQ 46 and the trait version of the State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA). 68 An autistic sample was recruited through the online platform Prolific 69 and consisted of 298 participants. To be eligible for the autistic sample, individuals had to report having a formal autism diagnosis from a health professional. Individuals who reported self-identifying as autistic without a formal diagnosis or who were in the process of an assessment were not included in either the autistic or non-autistic sample. To provide greater confidence in our sample, it should be noted that the autistic participants on average scored above the clinical cut-off (i.e., 148) on the Comprehensive Autistic Trait Inventory (mean [M] = 154.57, standard deviation [SD] = 25.97), a well-validated measure of autistic traits.70,71 A non-autistic sample comprised 406 university students who reported not having an autism diagnosis or self-identifying as autistic. The demographic statistics for the two samples are presented in Table 1.
Demographic Statistics for the Autistic and Non-Autistic Samples
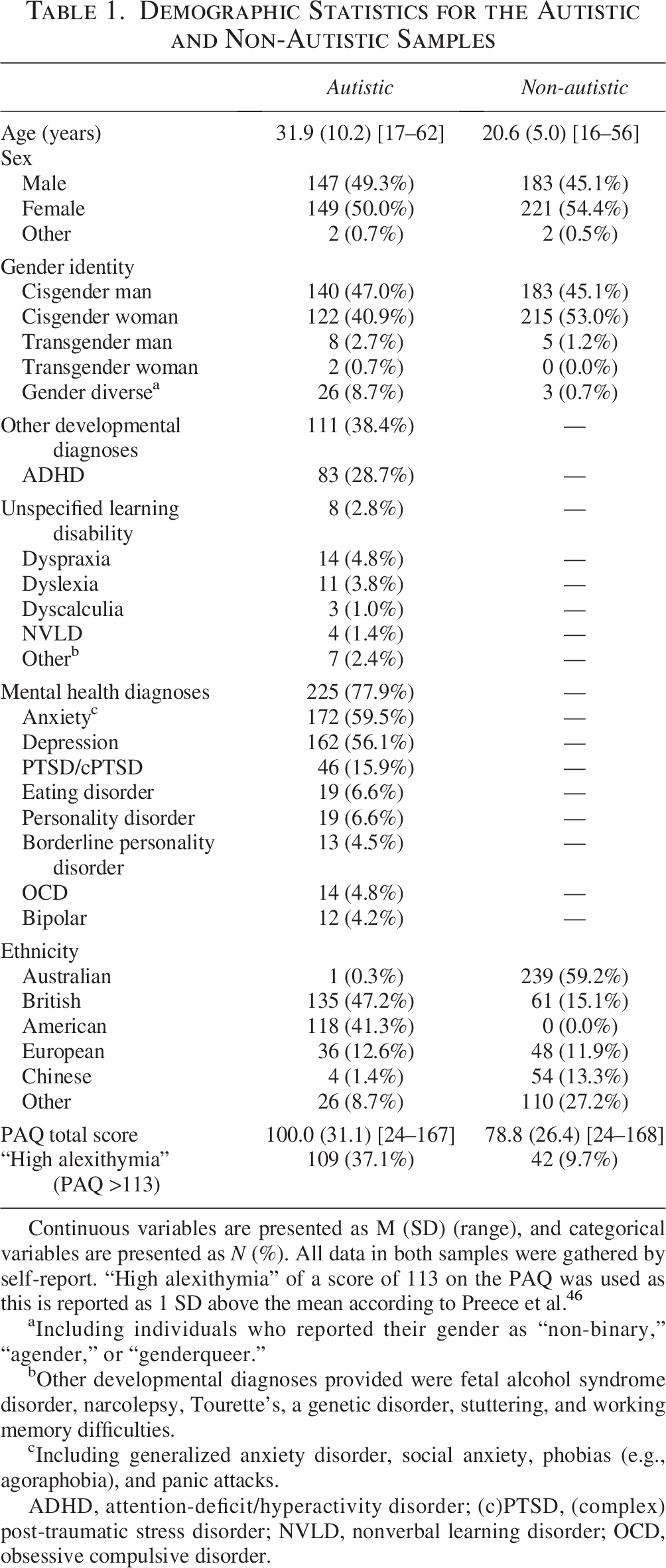
Continuous variables are presented as M (SD) (range), and categorical variables are presented as N (%). All data in both samples were gathered by self-report. “High alexithymia” of a score of 113 on the PAQ was used as this is reported as 1 SD above the mean according to Preece et al. 46
Including individuals who reported their gender as “non-binary,” “agender,” or “genderqueer.”
Other developmental diagnoses provided were fetal alcohol syndrome disorder, narcolepsy, Tourette’s, a genetic disorder, stuttering, and working memory difficulties.
Including generalized anxiety disorder, social anxiety, phobias (e.g., agoraphobia), and panic attacks.
ADHD, attention-deficit/hyperactivity disorder; (c)PTSD, (complex) post-traumatic stress disorder; NVLD, nonverbal learning disorder; OCD, obsessive compulsive disorder.
The autistic sample reported co-occurring neurodevelopmental diagnoses and mental health diagnoses (see Table 1); these questions were not provided for the non-autistic sample due to a methodological error. Overall, both samples came predominantly from Western countries (e.g., the United States of America, Britain, Europe, and Australia) without significant diversity (i.e., only 0.93% were Australian First Nation Peoples, compared with ∼3% of the general Australian population). We did not record data on socioeconomic status and educational attainment levels.
The final sample consisted of 627 participants (244 autistic individuals, 383 non-autistic individuals), after removing 7 participants who only provided demographic information, 42 participants who self-reported that their data were invalid, and 11 participants who completed the questionnaire too quickly for attentive responding (less than 2 seconds per item). Lastly, to meet statistical assumptions, we did not include gender-diverse people in the analyses due to inadequate sample size for this group. We refer to gender hereafter as only encompassing cis-male and cis-female individuals.
Participants provided informed consent digitally, and the study was designed according to the principles of the Declaration of Helsinki and obtained ethical approval from the University of Western Australia’s ethics board.
Materials
Perth Alexithymia Questionnaire (PAQ)
The PAQ 46 is a 24-item measure of alexithymia. The scale uses a 7-point Likert scale with higher scores indicating higher levels of alexithymia. Five subscales can be extracted: N-DIF, P-DIF, N-DDF, P-DDF, and G-EOT. Various composite scores, including a total score, can also be derived.
State-Trait Inventory for Cognitive and Somatic Anxiety
The Trait version of the STICSA 68 is a 21-item questionnaire that assesses respondents’ levels of anxiety. The scale uses a 4-point Likert scale with higher scores indicating higher anxiety. The items relate to the cognitions and somatic experiences commonly associated with anxiety. The STICSA has not been assessed for measurement invariance in an autistic sample, although previous research has highlighted its validity for assessing anxiety in autistic adults. 72 In the present study, the STICSA showed adequate internal consistency reliability (α = 0.92).
Statistical analyses
Statistical analyses were completed using Mplus (version 8.5) for the CFA and MNLFA of the PAQ and R (version 4.2.1) for the data visualization, item response theory (IRT) models, Johnson–Neyman regions of significance, and analyses exploring the relationships between alexithymia and anxiety. The robust maximum likelihood estimator based on a Pearson covariance matrix was used for the factor analyses. The sample size in the present study provided sufficient power. 73
Factor structure and classical test theory and IRT-derived reliability
CFAs were conducted on five theoretically driven models to assess the factor structure of the PAQ and therefore the latent structure of the alexithymia construct, in the autistic and non-autistic samples separately (Fig. 1). Model 1 was a unidimensional model, where all 24 items were specified to load on a “general alexithymia” factor. Model 2 had two factors representing the attention and appraisal stages of emotion valuation. Model 3 had three factors representing the difficulties identifying feelings, difficulties describing feelings, and EOT facets of alexithymia, but did not differentiate between valence domains. Model 4 was another three-factor model that represented valence-specific appraisals but did not differentiate between the DIF and DDF parts of appraisal, whereby two factors were negative difficulties appraising feelings (N-DAF) and positive difficulties appraising feelings (P-DAF) and the third factor was EOT (G-EOT). Model 5 was a five-factor model that represented the intended subscale structure of the PAQ, differentiating between the components of alexithymia and the valence domains, with N-DIF, P-DIF, N-DDF, P-DDF, and G-EOT factors. Lastly, Model 5b was a bifactor variant of Model 5, whereby items were loaded onto a general alexithymia factor and the specific factors suggested in Model 5.

Diagrammatic representation of the models investigated via confirmatory factor analysis. Figure taken from Preece et al. 7 Squares indicate item numbers, and ellipses indicate latent factors. Item error terms are not displayed. DAF, difficulty appraising feelings; DDF, difficulties describing feelings; DIF, difficulties identifying feelings; EOT, externally oriented thinking; G-, general factors (i.e., both valences); gen alexi, general alexithymia; N-, negatively valenced factors; P-, positively valenced factors.
Acceptable model fit was evaluated using standard criteria for the comparative fit index (≥0.90), the Tucker–Lewis Index (TLI ≥0.90), the root mean square error of approximation (RMSEA <0.08), and the standardized root mean residual (≤0.08).74–76 The Akaike Information Criterion, Bayesian information criterion (BIC), and sample-size adjusted BIC were also used to directly compare and investigate the most parsimonious model (lower values indicating greater fit and parsimony). 77
Model-based indices of the bifactor model 78 were calculated to examine the extent of multi-dimensionality in the PAQ and the PAQ’s reliability. Model-based indices included explained common variance of the general factor (ECV), total Omega (ω) Omega Hierarchical (ωH), and Subscale Omega Hierarchical (ωHS). The interpretation of these indices was based on guidelines from the literature.79–81 Lastly, to examine the PAQ’s reliability across the breadth of alexithymia levels, a series of graded response IRT models 82 were conducted on each PAQ scale separately for both the autistic and non-autistic samples.
Measurement invariance
While MNLFA simultaneously examines differential item functioning and latent construct differences, we focus first on the parameters related to measurement invariance before moving on to examining the parameters related to latent construct differences. Multidimensional MNLFAs were conducted using the best-fitting models to directly assess the compatibility of the PAQ’s structure and item functioning across the autistic and non-autistic samples while controlling and examining moderating effects of age and gender. We followed the suggested steps to conduct the MNLFAs. 62 An iterative approach was used to evaluate differential item functioning, where each item was sequentially assessed for possible differential item functioning. Likelihood ratio tests, 83 with the Benjamini–Hochberg procedure to control for false discovery rates, 84 were used to identify the items with differential item functioning. This procedure provides conservative results, thus identifying items that may not provide meaningful differential item functioning. 85 Accordingly, to determine whether the differential item functioning showed meaningful differences, we calculated McFadden’s R2 (R2McF) to provide an effect size of the differential item functioning. According to COSMIN guidelines, R2McF >0.02 indicates meaningful differential item functioning. 86
Alexithymia differences
After examining the MNLFA parameters involving differential item functioning, the MNLFA parameters involving the alexithymia profile of autism were investigated. This included examining the effect of autism diagnostic status on the means, variances, and covariances of alexithymia dimensions (while controlling for and examining the moderating effect of age and gender). Simple main effect analyses and Johnson–Neyman regions of significance were conducted when significant moderation effects were identified.
Alexithymia and anxiety
To explore the relationships between alexithymia and anxiety, bivariate and multiple regression analyses were conducted. Latent scores were taken from the previously conducted MNLFA to obtain scores of general alexithymia and alexithymia facets. Anxiety level (i.e., STICSA score) was the outcome in each regression analysis. We conducted bivariate regressions with autism spectrum disorder (ASD) diagnosis status, total alexithymia, and alexithymia components to investigate their total effects on anxiety before conducting multiple regressions to investigate unique effects across the alexithymia facets. Additionally, to explore whether these relationships differed in autistic and non-autistic individuals, moderation regressions were also conducted, whereby autism diagnosis status was the moderator.
Results
Factor structure and reliability
CFAs revealed that of the first-order correlated models, Model 5, which reflected the intended five-subscale structure of the PAQ, was the best-fitting model in both samples (Table 2). All items loaded >0.40 on their intended subscale factor in both samples (Supplementary Table S1). The bifactor variant of Model 5 (Model 5b) also fits the data well, indicating that a general alexithymia factor was tenable in both samples.
Model Fit Indices of the Examined Models Within the Autistic and Non-Autistic Samples
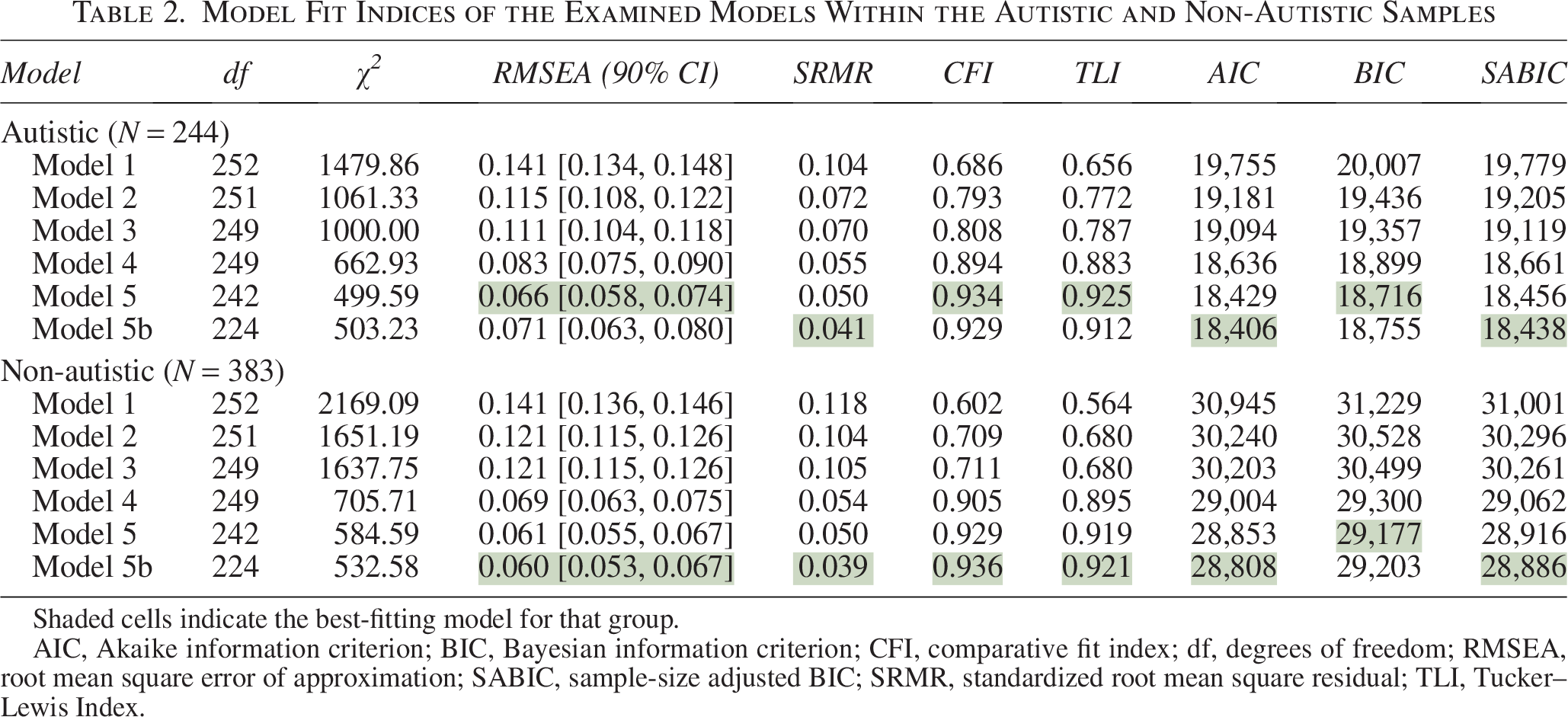
Shaded cells indicate the best-fitting model for that group.
AIC, Akaike information criterion; BIC, Bayesian information criterion; CFI, comparative fit index; df, degrees of freedom; RMSEA, root mean square error of approximation; SABIC, sample-size adjusted BIC; SRMR, standardized root mean square residual; TLI, Tucker–Lewis Index.
In terms of multidimensionality, the model-based indices (Supplementary Table S1) on the bifactor model indicated that the PAQ provides a multi-dimensional measure of alexithymia in both autistic and non-autistic individuals; percent of uncontaminated correlations (PUC) = 0.81 and ECVAutistic = 0.64 and ECVNon-autistic = 0.53. However, the general alexithymia factor showed good reliability (ω = 0.98 and 0.96), with most of this systematic variance accounted for by general alexithymia and not the subscales (ωH = 0.86 and 0.82), thus suggesting that the total scores may be considered essentially unidimensional.59–61 In line with the multidimensionality nature of the PAQ, the subscales provided additional value above the general alexithymia score (ωHS = 0.22–0.50).
Conditional reliability estimates indicated very good reliability (≥.80) for the total scale across people with various levels of severity — from low (θ>−3) to high (θ>+3) scores for both autistic and non-autistic individuals. In addition, conditional reliability estimates indicated good reliability (≥.80) for all the subscales from low (θ >−2) to high (θ>+2) scores (Supplementary Fig. S1). Overall, these results suggest that the factor structure of the PAQ appears to show utility in capturing alexithymia at both the general (i.e., total score) and facet (i.e., subscale) level in autistic and non-autistic individuals, with these factors showing reliability across a range of score severity.
Differential item functioning of the PAQ
Demographic information (Table 1) identified likely differences in age and gender between the two groups. These differences can be statistically controlled when included in MNLFA. As the first-order correlated and bifactor versions of Model 5 both demonstrated good performance and are theoretically meaningful, MNLFAs were investigated for Model 5′s first-order and bifactor structures.
First-order model
The first-order factor structure (i.e., Model 5) showed no significant differences in PAQ item functioning based on autism status for the majority (22) of the 24 items. Autistic individuals were less likely to endorse difficulties talking about their negative feelings in depth (item 7 from the N-DDF subscale) or difficulties paying attention to their emotions (item 9 from the G-EOT subscale), regardless of their underlying N-DDF or G-EOT (Supplementary Table S3). Two other items also differed in their functioning based on age or sex. While there were some statistically significant differential item functioning due to autism status, age, and gender, the total effect of this differential item functioning was not meaningful, R2McF < 0.01.
Bifactor model
Once the PAQ general factor was considered (i.e., in the bifactor model), only item 15 showed differential item functioning due to autism status. The results indicated non-uniform differential item functioning, whereby item 15 was a greater predictor of overall alexithymia for autistic individuals (B = 0.35, p = 0.001) and a worse predictor of G-EOT (B = −0.30, p = 0.016) than for non-autistic individuals. As with the first-order factor results, males and older individuals reported greater responses to item 15 than females and younger individuals, regardless of their underlying alexithymia and G-EOT levels (Supplementary Table S3). While there were some statistically significant differential item functioning due to autism status, age, and gender, the total effect of this differential item functioning was not meaningful, R2McF < 0.01.
Alexithymia differences
Mean differences
Figure 2 provides the factor scores from the bifactor and 5-factor first-order models. Regarding the relationship between autism diagnosis and alexithymia subscales (taken from the first-order model), after controlling for gender and age, there was a medium-sized difference 87 in all alexithymia subscales between the autistic and non-autistic groups (Cohen’s d = 0.48–0.77; see Supplementary Table S4), with the autistic group having higher levels. Gender moderated the difference between autistic and non-autistic individuals on N-DIF (B = 0.36, p < 0.05) and N-DDF (B = 0.34, p < 0.05). Simple main effect analyses identified that autistic females reported a medium- to large-sized difference in N-DIF (B = 0.79, p < 0.001) and N-DDF (B = 0.87, p < 0.001) compared with non-autistic females. Contrastingly, autistic males reported a medium-sized difference in N-DIF (B = 0.51, p = 0.001) and N-DDF (B = 0.63, p < 0.001) compared with non-autistic males. Overall, autistic individuals report greater difficulties across all facets and valence domains of alexithymia.
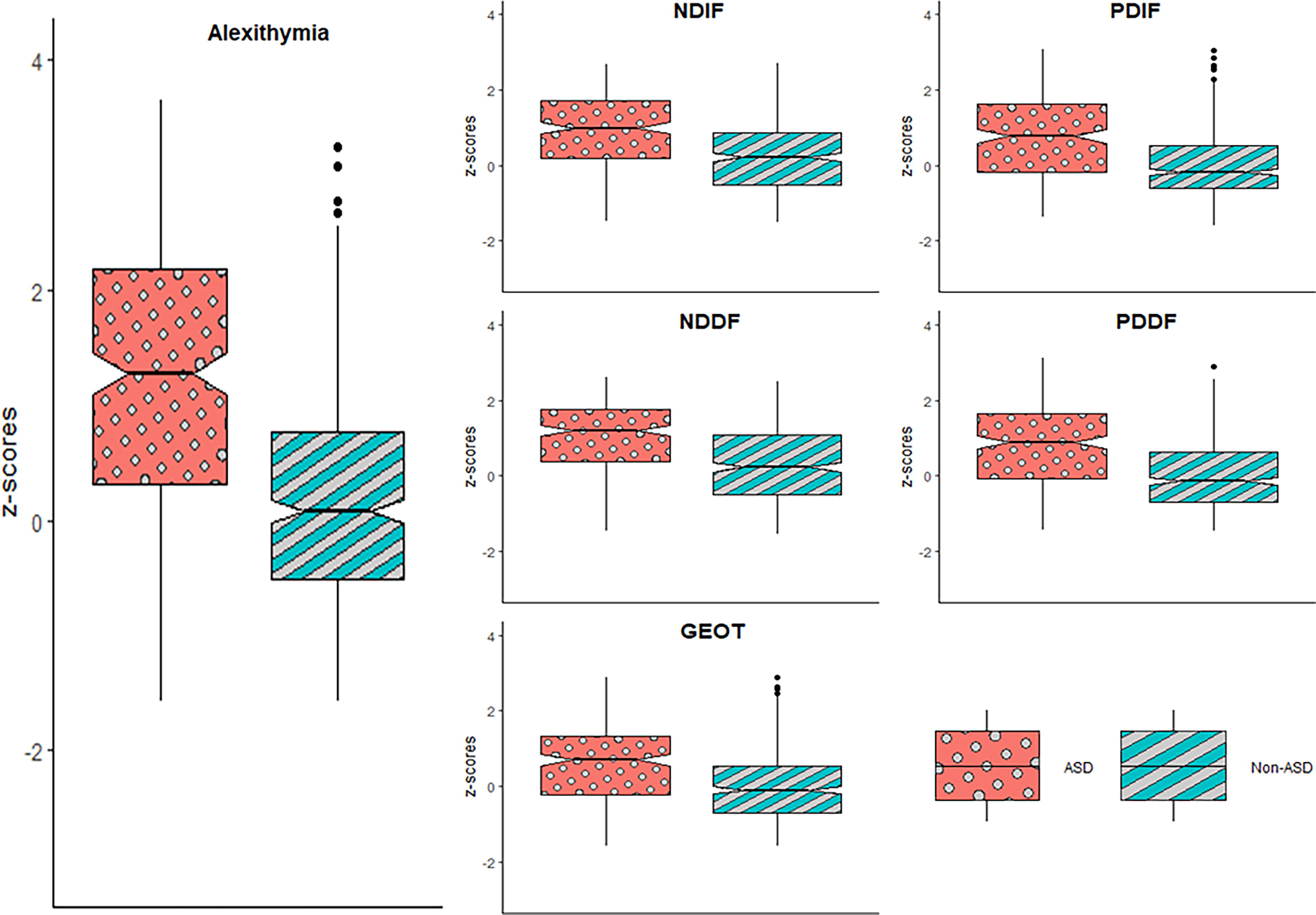
Alexithymia and alexithymia’s subcomponent scores for autistic and non-autistic individuals. The alexithymia scores are taken from the bifactor MNLFA, while the subscale scores are taken from the first-order MNLFA. Dots indicate outliers. GEOT, general externally oriented thinking; NDDF, difficulties describing negative feelings; NDIF, difficulties identifying negative feelings; PDDF, difficulties describing positive feelings; PDIF, difficulties identifying positive feelings.
As expected, given that all subscales suggested similar differences, the bifactor model found differences between autistic and non-autistic individuals on overall alexithymia scores. Autistic individuals reported significantly more overall alexithymia than non-autistic individuals (Cohen’s d = 1.1, p < 0.001). Additionally, this difference in alexithymia was moderated by age, whereby the older the individuals, the greater the difference between autistic and non-autistic (B = 0.03, p < 0.05). Simple main effect analyses suggested no effect of age in autistic individuals (B = 0.01, p = 0.173). In contrast, older non-autistic individuals reported less alexithymia than younger non-autistic individuals (B = −0.03, p = 0.031). Johnson–Neyman regions of significance analysis revealed that across all ages recorded, autistic individuals reported greater overall alexithymia than non-autistic individuals. In the bifactor model, there were no differences in the specific factors once the general alexithymia factor was accounted for, further supporting that the general alexithymia factor accounts for substantial variance.
Variance and covariance differences
The results revealed greater alexithymia heterogeneity in the autistic sample than in the non-autistic sample. The variance of the general alexithymia factor in the autistic sample was 1.73, compared with 1.00 in the non-autistic sample (p < 0.001). However, there were no significant differences in variability between the two samples for the subscales (in the first-order and bifactor models). The greater variance in the general alexithymia factor suggests greater heterogeneity of overall alexithymia in the autistic population than in the non-autistic population. Lastly, autistic diagnosis status did not influence the co-variance between any factors (for both the first-order and bifactor models), suggesting that the relationships between alexithymia facets (subscales) are similar for autistic and non-autistic individuals.
Alexithymia and anxiety
Using bivariate and multiple regressions, we examined the influence of alexithymia and autism diagnosis on anxiety levels (one non-autistic individual did not complete the anxiety questionnaire). A total anxiety score was used as the pattern of bivariate correlations was the same when investigating somatic or cognitive anxiety symptoms (Supplementary Table S5). The general alexithymia score was taken from the bifactor MNLFA alexithymia score, while the subfactors were taken from the first-order MNLFA scores. All models passed assumptions of independence of residuals (Durbin–Watson test statistics), homoscedasticity (Breusch–Pagan test), and outliers/influential observations (students residuals and Cook’s distance). General alexithymia, all alexithymia subfactors, and autism diagnosis were all related to greater levels of anxiety (Supplementary Table S5).
Once controlling for the effects of alexithymia, age, and gender, individuals with an autism diagnosis reported 0.27 standard deviations more anxiety than those without the diagnosis (B = 3.16, p = 0.006). Individuals reporting greater general alexithymia reported greater anxiety (B = 3.90, β = 0.39, p < 0.001), controlling for autism diagnosis, age, and gender. Additionally, the relationship between alexithymia and anxiety did not differ for autistic and non-autistic individuals (i.e., no significant interaction effect of autism diagnosis, B = −0.81, p = 0.315).
When investigating the influence of the alexithymia factors, the assumption of multi-collinearity was violated (i.e., VIF >10), reflecting high correlations between each valence domain’s DIF and DDF facets. Therefore, the scores within each valence domain for DIF and DDF were summed together to assess valence-specific difficulties appraising feelings (i.e., N-DAF and P-DAF scores), which are also theoretically informed composite scores from the standard PAQ scoring, as DIF and DDF both conceptually correspond to the appraisal stage of emotion processing. 46 The results from the multiple regression (Supplementary Table S6) suggested that N-DAF (β = 0.38; p < 0.001) and P-DAF (β = 0.31; p < 0.001) both uniquely increased levels of anxiety after controlling for the effects of autism diagnosis (βsemi-standardized = 0.34; p < 0.001) and G-EOT (β = −0.28; p < 0.001). Interestingly, a negative suppression effect 88 was found for G-EOT. The results suggested that G-EOT was related to lower anxiety levels after controlling for difficulties appraising feelings and ASD diagnosis (and the covariates), which is the opposite direction when not controlling for difficulties appraising feelings.
Moderation analyses revealed that ASD diagnosis did not moderate the relationships between anxiety and N-DAF (B = 0.00, p = 0.999) or P-DAF (B = −0.34, p = 0.409). Contrastingly, the relationship between G-EOT and anxiety (i.e., the negative suppression) is stronger in autistic individuals than in non-autistic individuals (B = −1.65, p = 0.042). The moderation effect was not spurious due to a quadratic effect (i.e., no statistically significant quadratic effect of G-EOT on anxiety, B = 0.39, p = 0.240). 89 Simple main effect analyses revealed that both autistic (B = −4.86, β = −0.43, p < 0.001) and non-autistic individuals (B = −1.92, β = −0.16, p = 0.010) report reduced anxiety with greater G-EOT after controlling for their difficulties appraising feelings.
Discussion
The present study sought to establish the validity of assessing alexithymia in the autistic population via a psychometric study of the PAQ. Moreover, we used the PAQ to explore how alexithymia manifests across autistic and non-autistic individuals and what impact alexithymia has on mental health outcomes (anxiety) for autistic individuals. Overall, we found that the PAQ performed well across both autistic and non-autistic individuals, producing a valid measure of the multidimensional alexithymia construct. Our results highlight that on average alexithymia is substantially elevated in autistic individuals, and is linked to increased mental health problems, thus meaningfully advancing our understanding of the alexithymia construct in autism.
The latent structure of alexithymia in the autistic population
We found the same theoretically congruent factor structure for the PAQ across the autistic and non-autistic samples, thus replicating past work on the PAQ outside of autistic samples.46,49–54 The PAQ was well represented by five specific factors (i.e., difficulty identifying negative feelings, difficulty identifying positive feelings, difficulty describing negative feelings, difficulty describing positive feelings, and EOT). These findings highlight the broad utility of considering the different facets of alexithymia, as well as the negative and positive emotional valence domains when assessing alexithymia in autistic individuals. There was also strong evidence for a “general alexithymia” factor in the bifactor model, thus supporting the extraction of a total score from the PAQ and the coherent multidimensional nature of the alexithymia construct.46,48,90 All subscales and the total score had high reliability across the breadth of alexithymia scores. Importantly, while a small number of items had statistically significant differential item functioning (i.e., items 7, 9, and 15), none of these items had meaningful differences in item functioning across the autistic and non-autistic samples. This indicates that the structure of the alexithymia construct, as measured by the PAQ, manifests similarly across autistic and non-autistic samples, thus enabling confident comparisons. Accordingly, we recommend using all 24 items of the PAQ when assessing alexithymia in autism, with the flexibility of using the full array of total, composite, and subscale scores.
This contrasts with the only previous psychometric examination of another alexithymia measure in an autistic sample, 44 which found the TAS-20 to be unsuitable for use with autistic individuals in its standard form, resulting in the proposal of the GAFS-8, which does not include any EOT items and allows for no facet-level subscales. Our positive results with the PAQ suggest that those past findings are likely specific to measurement issues with the TAS-20 (e.g., TAS-20 psychometric issues have also been identified in non-autistic samples)38,39 rather than broader issues with the validity of the alexithymia construct in autistic individuals. Indeed, our results highlight the importance of EOT through the factor analyses, suggesting that it is a component of alexithymia and that EOT relates more strongly with anxiety in autistic compared to non-autistic samples. Our study makes a substantial novel contribution in providing the PAQ as the first comprehensive alexithymia tool successfully validated for use in autistic populations that can assess across the full breadth of the construct (i.e., DIF, DDF, EOT). In so doing, our study provides initial evidence that theoretical models of alexithymia that position DIF, DDF, and EOT as key interrelated components of the construct (e.g., the attention-appraisal model) 7 can be relevant in autistic samples. That said, this is a single study, and there is an important need for future research to continue testing the generalizability and replicability of our findings. Moving forward, our data suggest the PAQ provides an essential measurement foundation for the field, now enabling alexithymia to be confidently operationalized in a manner that does not unduly bias scores for autistic individuals.
Alexithymia differences
Upon this measurement foundation, we also sought to use the PAQ to understand more about alexithymia in autistic individuals. We comprehensively investigated whether alexithymia manifests differently (e.g., mean, variance, and covariance differences) between autistic and non-autistic individuals. Our finding that autistic people generally report greater alexithymia is consistent with most previous research,16,55 with autistic individuals reporting similar levels of difficulties across all alexithymia components and valence domains. Thus, on average, focusing attention on emotions (i.e., EOT) and accurately appraising those emotions (i.e., DIF and DDF) all appear more challenging for autistic individuals. Interestingly, gender moderated some differences, highlighting that autistic females in particular report greater difficulties with appraising negative feelings (but not positive feelings) than non-autistic females. This valence differentiation further highlights the importance of investigating valence-specificity in alexithymia.
That said, we also found greater heterogeneity in alexithymia levels among the autistic sample than the non-autistic sample. Similarly, heightened levels of heterogeneity have also been observed in the autistic population for other emotional skills, such as empathy. 56 Indeed, emotional processing and expression can vary significantly among individuals, 36 influenced by personal, contextual, social, and cultural factors. As such, these mean differences in alexithymia are likely not generalizable to all autistic individuals, and not all autistic individuals will have high alexithymia. 17 Accordingly, there is a need for future research to understand what mechanisms may contribute to this greater alexithymia heterogeneity in autistic populations so that support can be better personalized. Alexithymia research outside of autistic samples has begun examining the presence of potential alexithymia subtypes, 59 and this may be a fruitful area of study in the autism context. Additional moderating variables may also help to explain this heterogeneity. For example, in our study, we found demographic variables moderated differences, with greater differences in females and younger individuals. Other potential moderating factors, interoception 91 and emotion regulation abilities 92 could be good areas of investigation.
Environmentally, risk factors for developing alexithymia include environments that invalidate emotions and where it is unsafe to express emotions. 93 This is particularly true for some autistic individuals who may experience greater levels of stigma. 94 Additionally, some autistic individuals report attempting to conform to neurotypical norms by suppressing their autistic traits, leading to emotional challenges. 95 As such, one possible explanation of the greater heterogeneity of alexithymia in autistic populations is that some autistic individuals might have greater exposure to these environmental factors, with these negative experiences driving greater attempts to disengage from or avoid emotions. 96 It will be vital for future research to investigate the impact of these environmental factors on how autistic individuals experience alexithymia.
Lastly, we did not find any co-variance differences, indicating that the positive relationships between alexithymia components are not significantly different between autistic and non-autistic individuals. As such, individuals (autistic and non-autistic) that report difficulties in one alexithymia component are likely to report difficulties across the other alexithymia components. Given the high correlation between valence-specific difficulties identifying and describing feelings, particularly when not including a general alexithymia factor, summing the DIF and DDF elements can provide conceptually clear valence-specific difficulties appraising feelings scores (as used in our investigation with anxiety, and aligned with the close conceptual mapping of DIF and DDF onto the appraisal stage of emotion processing) 25 for both autistic and non-autistic individuals. Lastly, these results suggest that the valence-specificity of difficulties identifying and describing feelings may be similarly distinct across these two groups.
Understanding more about alexithymia in autism will be essential, as our findings also show that alexithymia is linked with poor mental health outcomes (anxiety) in autistic individuals. In this respect, our results replicated previous research investigating alexithymia’s influence on mental health in autistic individuals.20–24 This is consistent with theorizing that alexithymia may be one risk factor for emotion-based psychopathologies (e.g., due to its impact on emotion regulation).6,25 Alexithymia was robustly associated with greater levels of anxiety, even after controlling for autism diagnosis status. Regarding the components of alexithymia, individuals exhibiting greater difficulties appraising negative and positive feelings and EOT reported greater anxiety symptoms. However, a negative suppression occurred when effects caused by difficulties appraising feelings were controlled for in the relationship between EOT and anxiety; for individuals with the same levels of appraising difficulties, those who report less attention to their emotions (i.e., more EOT) report fewer anxiety symptoms. Furthermore, this effect was greater in autistic individuals than in non-autistic individuals.
The stronger relationship between EOT and anxiety in autistic individuals, once controlling for difficulties appraising emotions, may arise from the broader social and contextual factors experienced by autistic individuals. There are indications that the development of alexithymia in autism may be driven by miscommunication between autistic and non-autistic emotional expressions. The pressure to conform to neurotypical emotional expression norms can create anxiety and stress in autistic individuals,97,98 particularly from the fear of being misunderstood. 34 Consequently, one possibility is that autistic individuals may stop focusing on their own emotional experiences to make it easier to conform to these neurotypical norms, potentially alleviating anxious feelings. However, further research will be needed to assess the replicability of these findings and the associated long-term impacts. For instance, this reduced attention may increase the difficulties one has in appraising one’s emotions, ultimately leading to greater anxiety in the long run.
In terms of practical implications, our results highlight the utility of assessing alexithymia amongst autistic individuals to better understand mental health risks. Our findings also support that targeting alexithymia in treatment may be helpful for many autistic individuals (alexithymia treatment approaches do exist 25 ), perhaps helping to address the high rate of emotional disorders often observed in autistic populations. 99 However, more work is needed to understand the link between alexithymia and anxiety. Future research can now extend our findings by investigating potential socio-cultural factors (e.g., stigma and misunderstanding of autistic perspectives), autistic traits (e.g., communication differences and sensory sensitivities), and other mental health factors (e.g., depression) to better understand these complexities and provide greater nuance to the alexithymia hypothesis of autism. 17
Limitations and future directions
While the current article provides meaningful contributions to the field, some limitations should be noted. First, the PAQ is a self-report questionnaire, which may exclude participants with significant levels of co-occurring intellectual disability. Accordingly, and due to our online sample, there should be caution in generalizing the current findings to autistic individuals less likely to be recruited online, such as individuals with an intellectual disability. 100 Second, there are limits regarding the generalizability of the results. The current samples were from Western Countries, and future studies in different cultural groups will be important to establish the generalizability of these findings across cultures. 49 The autistic sample also came from an online sample that reported having an official autism diagnosis. We did not verify the participants’ diagnoses (e.g., by asking for proof or conducting an autism assessment), and we did not include individuals who self-identify as autistic (even if in the process of an assessment). We acknowledge the legitimacy of self-identification, particularly in the context of structural barriers to formal diagnosis, such as long waitlists, financial limitations, or gender and cultural diagnostic biases. 101 While online recruitment of autistic individuals is common,102–111 future research will be needed to extend on the current results within clinical settings (i.e., where verification of an autism diagnosis is more viable) and to individuals who self-identify as autistic.
Conclusions
Our study provides the first successful psychometric validation of a measure of all alexithymia facets in autistic individuals. Our data highlight that, as assessed via the PAQ, the multidimensional alexithymia construct is valid across autistic and non-autistic samples, with autistic individuals, on average, having significantly higher levels of alexithymia. These findings underscore the importance of assessing and addressing alexithymia in autistic samples, given the robust links between alexithymia and poor mental health outcomes. Moving forward, our results with the PAQ now provide a psychometric foundation to enable such work within the field.
Authorship Confirmation Statement
J.D.B.: Conceptualization, methodology, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, and funding acquisition. I.J.: Conceptualization, methodology, writing—original draft, and writing—review and editing. M.U.: Writing—review and editing. A.W.: Writing—review and editing. J.J.G.: Writing—review and editing. A.C.S.: Writing—review and editing. D.A.P.: Conceptualization, methodology, investigation, writing—original draft, writing—review and editing, and supervision. The article has been submitted solely to Autism in Adulthood.
Data Access Statement
Data are available on the Open Science Framework repository (https://osf.io/qe7fj/?view_only=da271bc5b0d24502a0bffb267130de87).
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The authors acknowledge the support provided by an Australian Government Research Training Program Stipend to J.D.B.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.