
Abstract
Background:
Autistic adults face a paradox: they have a greater risk of developing mental health difficulties, while also experiencing increased barriers to accessing mental health care. Research on reducing these barriers has previously focused on physical adjustments such as providing quiet waiting rooms, and cognitive adaptations such as using unambiguous language. Approaches to building the therapeutic relationship have been under-researched.
Methods:
The researchers interviewed 12 UK-based late-diagnosed White autistic females about experiences of therapy that they identified as being particularly positive. The study adopted a critical realist and neuro-affirmative stance, with an insider researcher position. The researchers developed common themes and subthemes through reflexive thematic analysis.
Findings:
Three themes were developed from the interviews and incorporated eight subthemes. Theme 1: “Providing and delivering beneficial therapy for autistic clients” included “sourcing therapy” and “autistic expectations of positive therapy.” Theme 2: “Features of a positive therapeutic relationship from an autistic perspective” included “building trust and rapport,” “equitable power dynamics,” and “reciprocity and a collaborative approach.” Theme 3: “Understanding autism and using adaptation strategies” included “adaptation strategies,” “understanding autism,” and “positive autism.”
Conclusions:
While physical and cognitive adaptations improve the accessibility of therapeutic interventions, therapists must also focus on adapting the therapeutic relationship with autistic clients, particularly with an enhanced focus on power dynamics and collaborative approaches. All participants described positive experiences of connection when their therapists shared relevant insights and experiences to build common ground. Recognizing less stereotypical presentations of autism and exploring internalized ableism in both the therapist and client improved the positive experience of therapy.
Community Brief
Why is this an important issue?
Autistic people have identified mental health as a major issue, with only a small percentage of those wanting support being able to access it.
Previous research has recommended adjustments to the physical environment and adjustments for thinking and processing styles, but therapists need more information about building positive therapeutic relationships with autistic clients.
What was the purpose of this study?
This study sought to identify best practices in therapy by listening to the experiences of autistic adults who felt that they had received particularly positive support. By focusing on a smaller subgroup of autistic people, late-diagnosed autistic females, we aimed to identify commonalities to provide specific recommendations to therapists.
What did the researchers do?
We interviewed 12 late-diagnosed White autistic females about their experiences of therapy that felt particularly positive. We compared their answers and developed common ideas.
The researchers offered interviews in a variety of formats to cater to autistic communication differences, either live via video link or live chat, or over more extended periods via email or voice messages. Eleven of the 12 participants chose email interviews.
What were the results and conclusions of the study?
We analyzed the interview answers and developed them into three main themes. Theme 1: “Providing and delivering beneficial therapy for autistic clients” includes the subthemes “sourcing therapy” and “autistic expectations of positive therapy.” Theme 2: “Features of a positive therapeutic relationship from an autistic perspective” includes the subthemes “building trust and rapport,” “equitable power dynamics,” and “reciprocity and a collaborative approach.” Theme 3: “Understanding autism and using adaptation strategies” includes the subthemes “adaptation strategies,” “understanding autism,” and “positive autism.”
What is new or controversial about these findings?
Participants described wanting therapy to feel challenging but also to provide a nonjudgmental and validating space. They emphasized a need for an enhanced focus on collaboration and appreciated therapists who were willing to share some of their own insights and experiences to build common ground. This study also suggests that therapists needed more information about autism and its wider presentation, and should recognize and challenge internalized biases and ableism within themselves and their clients.
What are potential weaknesses in the study?
This study was limited to a UK population and only looked at late-diagnosed White autistic females. Further work needs to be done to explore the experiences of the wider autistic population, including other minority groups, those with learning disabilities, and those who do not communicate with speech.
How will these findings help autistic adults now or in the future?
Improving therapists’ knowledge of autism and appropriate therapeutic adaptations can improve therapy outcomes and reduce health care inequalities within the autistic population. Offering multiple communication formats for participation in scientific research promotes accessibility, allowing a greater number of autistic individuals to contribute to future studies.
Introduction
Autism is associated with a greater risk of mental health difficulties,1,2 including significantly elevated risk for suicide. 3 Despite this, autistic adults experience significant barriers to accessing mental health care, including insufficient capacity within services, 4 difficulties with communication leading to misunderstandings, 5 and an underestimation of the severity of need. 6 Diagnostic overshadowing can result in misdiagnosis and delays in the provision of appropriate support for co-occurring mental health difficulties. 7 Brede et al. 8 suggest that current mental health services lack the flexibility needed to adequately support autistic clients and need to be tailored, with an understanding of the impact of an individual’s autism on their mental health, to prevent the possibility of causing further harm. There are concerns, especially within the autistic community, that some therapies are felt to pathologize autism and autistic behaviors or reflect outdated, stereotypical, and ableist views of autism.9,10 Mental health professionals report less confidence in treating autistic clients due to a lack of training and misconceptions about autism,11–14 which may be associated with therapist anti-autistic bias, both intentional and unintentional, that is particularly damaging to client self-esteem. 15 A qualitative study by Dabbs et al. suggests that the effects of these biases are also seen in therapist training establishments, where autistic students report having greater barriers to admission and lower retention rates, reducing autistic representation within mental health professions. 16
Adapting therapy for autistic clients
As reflected in previous studies,17,18 there is growing awareness that adaptations relating to the physical environment, structure of appointments, and cognitive needs of the client may support autistic people to better access mental health care. In the United Kingdom, there is a legal requirement for public sector organizations, such as the National Health Service (NHS), to make reasonable adjustments to ensure that services are accessible to disabled people, including those with autism spectrum disorders, under the Equality Act (2010). 19 In addition to adaptations to the way care is delivered, research suggests that mental health interventions may also need adaptation in terms of their content to allow for autism-specific risk factors and mechanisms behind mental health difficulties. 20 For example, autistic social anxiety may be based on accurate experiences of stigma and discrimination, and so exposure-based exercises and expectations regarding outcomes from therapy may need to be adapted for the autistic population. 21 It is also essential that interventions be carefully considered to ensure that they are aimed at reducing comorbidities such as anxiety and depression rather than suppressing core autistic characteristics. 22 There is early empirical work looking at autism-adapted therapies, for example, Personalised Anxiety Treatment—Autism (PAT-A), 23 which has refined existing treatment packages and developed bespoke modules specific to the needs and experiences of autistic people. Overall, the evidence base is limited regarding the effectiveness of mental health interventions for autistic people, with a systematic review concluding “very low” certainty that existing approaches, including autism-adapted interventions, can improve mental health in autistic people, underlining the importance of further research. 24
Adapting therapeutic relationships for autistic clients
One area that has been relatively overlooked within mental health care for autistic adults is the centrality of relationship building to mental health interventions and the possible need to adapt this process to support autistic communication styles.25–27 Albaum et al. (2022) state that “Given the inherent social communication challenges … it is critical to consider therapist factors that may contribute to establishing and maintaining alliance… .”
A key aspect of psychological therapy is the development of a therapeutic relationship between a therapist and their client. 28 A strong therapeutic relationship has been known for many years to influence positive outcomes in therapy across a range of therapy modalities and populations. 29 However, the training that therapists receive to build this therapeutic relationship is based on neurotypical (NT) communication styles and may not always translate well to autistic individuals. 30 In a systematic review of therapeutic process factors in mental health treatment for autistic youth, Albaum et al. (2023) found that strong working relationships are not only possible but appear to be an important contributor to both engagement in treatment and improved mental health outcomes, although discrepancies were noted based on who rated the relationship (therapist or client), possibly highlighting a disconnect in the perception of the therapeutic relationship between therapist and client. 26 The therapeutic relationship is grounded in the core conditions of Rogerian person-centered therapy of congruence, unconditional positive regard, and empathy. 31 While the therapist may intend to communicate these conditions, the client must also perceive them, and autistic differences in social communication may alter the perception of these core conditions.
These differences in social communication may occur at different levels. At an emotional-cognitive level, the autistic individual may show traits of alexithymia, which is highly prevalent in the autistic community32,33 and may mean that the individual presents with difficulties in understanding and communicating emotions within the therapeutic relationship. At an interpersonal level, communication between the client and therapist may be hampered by the “double-empathy problem” 34 where interaction and communication difficulties between autistic and non-autistic people are mutual rather than stemming from deficits in the autistic person alone. These difficulties arise from differences in social cues and communication styles between different groups, and are equally relevant to the therapeutic relationship as they are to other types of relationships. At a broader contextual level, the double-empathy problem may be exacerbated by what Shaw et al. 35 have called a “triple-empathy problem.” This relates to additional barriers resulting from the specific language, communication styles, and culture into which health care professionals have been socialized; these can alienate both autistic and non-autistic patients, but when combined with the double-empathy problem may have a particularly high impact for autistic people entering into a therapeutic relationship with a therapist. Lastly, we should consider that certain subgroups of autistic people may experience specific barriers to communication within the therapy room. For example, among late-diagnosed women, individuals commonly report “masking” autistic traits to attempt to “fit in” with NT styles of interaction.36,37 Masking may be a key factor affecting a client’s identity, life story, and challenges—and therefore potentially the themes they might bring to therapy—while also possibly affecting the relational dynamics in the therapy room. It is unclear the extent to which masking and many other subtle barriers to communication may impact the development of the therapeutic relationship.
Previous qualitative research has highlighted the importance of the therapeutic relationship from an autistic perspective. For instance, Darazsdi and Bialka (2023) found that while expressions from therapists of both implicit and explicit bias were extremely damaging to the mental health and self-esteem of autistic clients, one strong therapeutic relationship was felt to be capable of reversing the damage of many negative experiences. 15 Similarly, O’Brien et al (2024) found that creating a therapeutic relationship based on feelings of human connection, a willingness to be flexible and accommodating, and a focus on strengths rather than deficits took time and patience, but resulted in feelings of a “safe space,” which facilitated a positive experience. 27 Hume’s Interpretive Interactionist study highlights the importance of person-centered relationships. 25 It discusses the overlap between effective relational approaches for autistic and non-autistic clients, finding that while the same conditions of congruence, empathy, and unconditional personal regard were required, these needed to be demonstrated at enhanced levels with autistic clients. Self-disclosure was suggested to have a greater importance in demonstrating authenticity with explicit expressions of genuine emotion supporting an enhanced experience of both empathy and unconditional positive regard; participants also discussed a desire to explore positives and to talk about interests, hopes, and dreams rather than being entirely focused on problems or difficulties.
Rationale
There has been an increase in the United Kingdom of 787% in autism diagnosis over 20 years (1998–2018), with the greatest increase being among adult females. 38 The late diagnosis of autistic females can be associated with elevated mental health needs, 39 and since therapeutic relationship formation and priorities may vary by gender, 40 the perspectives of a late-diagnosed female participant base may differ from those of previous studies. This indicates a need to investigate the experience of therapy and therapeutic relationships in this rapidly increasing population.
Aims
This research aimed to explore the experiences of therapy and building a therapeutic relationship from a late-diagnosed female perspective. It was felt that taking the positive perspective of exploring what has been beneficial rather than emphasizing negative experiences would provide greater opportunities to identify best practices and to give specific, actionable recommendations for therapists. The overarching research question asked how therapists have contributed to positive experiences of therapy and therapeutic relationships, from the perspective of autistic adults, specifically late-diagnosed females.
Methods
The University of Essex Online Ethics Committee granted ethical approval (Ref. no. 5746 4099 3412 7589 464) for this study as part of a student dissertation.
This study used a qualitative interview design and was analyzed using Braun and Clarke’s reflexive thematic analysis. 41 The primary researcher (Z.M.) approached the data from a critical realist stance and the position of an insider researcher. This insider position impacts both the questions asked and the interpretation of the data; the reflexive nature of Braun and Clarke’s methods allows for this subjectivity to be openly explored and used to develop more complex interpretations.
The authors approach autism from a neuro-affirmative stance of autistic differences rather than deficits. All suggestions and recommendations are directed toward helping therapists overcome barriers to effective communication with autistic clients.
Participants
Participants were females who self-reported having been diagnosed with autism as adults (aged 18 or older) and had accessed therapy or counseling for mental health support in the United Kingdom that they had considered a positive experience. We recruited participants via Facebook, Reddit, and in-person networks, leading to initial interviews with five participants. On reviewing the data, the researchers identified new discussion points and novel codes; the study was readvertised, and seven additional participants were recruited. The researchers determined that the final data set was sufficient, with no novel codes in the last interview.
All participants were White British, of whom three had dual nationalities. The average age of participants was 43 years (SD = 9 years) and the average age at diagnosis was 41 years (SD = 9 years). Six participants had accessed therapy through the NHS, and six had accessed therapy privately. In the NHS, local mental health services can be accessed through referral from primary care, and in some cases through self-referral, for instance, to NHS Talking Therapies; therapists would typically be allocated by the service. Alternatively, the client may be able to follow the “right to choose” pathway in the NHS and select their preferred NHS or partner service. Participants discussed their positive experiences in relation to 10 different modalities of therapy; these modalities were self-reported by the participants. Other modalities were discussed by some participants in comparison with the main therapy. A summary of key participant information is given in Table 1.
Summary of Participant Information
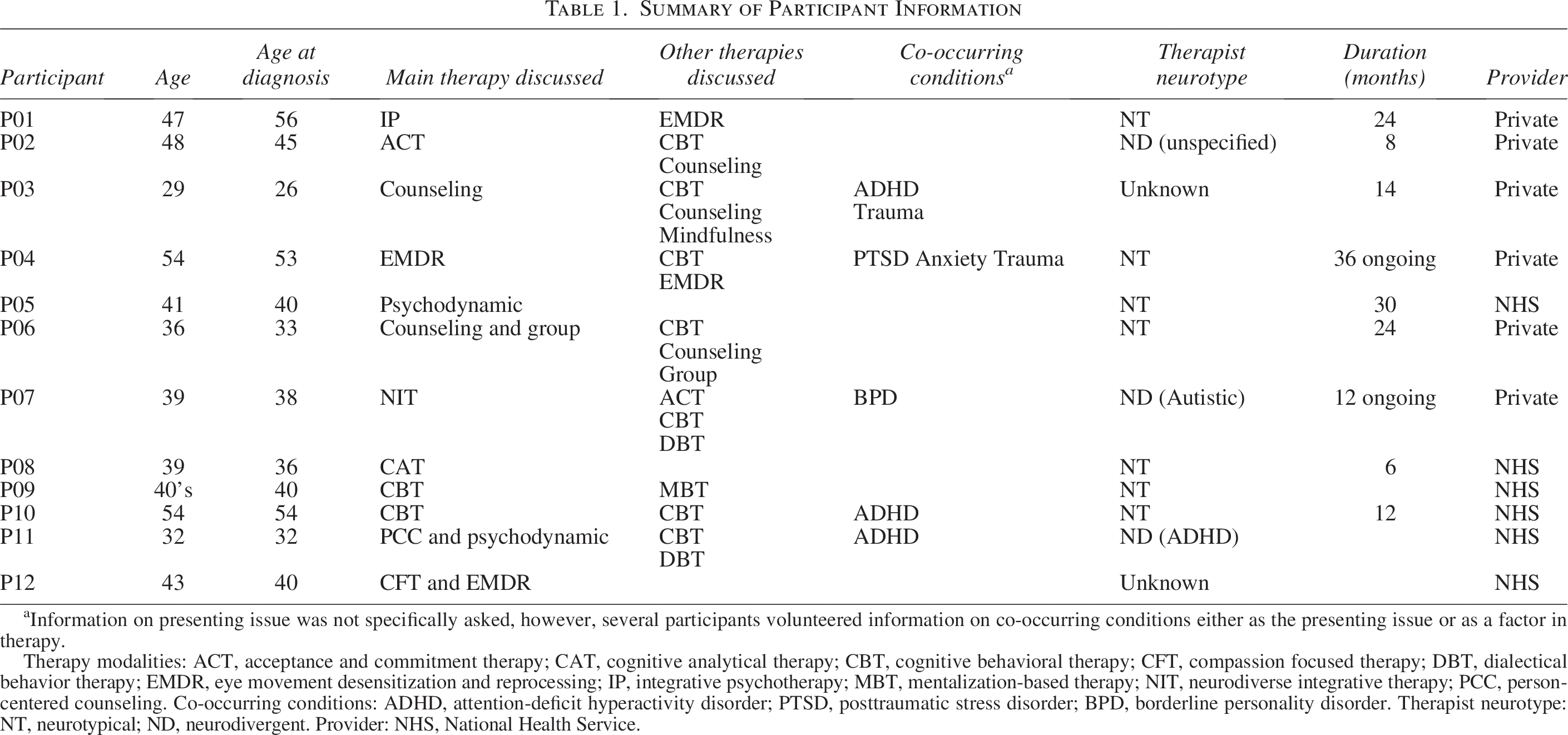
Information on presenting issue was not specifically asked, however, several participants volunteered information on co-occurring conditions either as the presenting issue or as a factor in therapy.
Therapy modalities: ACT, acceptance and commitment therapy; CAT, cognitive analytical therapy; CBT, cognitive behavioral therapy; CFT, compassion focused therapy; DBT, dialectical behavior therapy; EMDR, eye movement desensitization and reprocessing; IP, integrative psychotherapy; MBT, mentalization-based therapy; NIT, neurodiverse integrative therapy; PCC, person-centered counseling. Co-occurring conditions: ADHD, attention-deficit hyperactivity disorder; PTSD, posttraumatic stress disorder; BPD, borderline personality disorder. Therapist neurotype: NT, neurotypical; ND, neurodivergent. Provider: NHS, National Health Service.
Procedure
After providing written informed consent, participants took part in a structured interview that was offered in multiple formats to allow for differences in preferred communication methods and processing styles: asynchronous text (emails), asynchronous verbal (voice message emails), synchronous text (chat function interviews), and synchronous verbal (video interview). Eleven participants requested email interviews, and one participant requested a video call interview; this was conducted and recorded on Zoom and transcribed using Auris AI.
The interviews included three broad categories of questions relating to demographics and background information, positive perceptions and experiences of therapy, and the effects of autism on therapy. The initial four participants were not told how many emails would be required. Following feedback that a fixed number would be helpful, the researchers restructured the questions into six numbered emails using the same content but with more formal organization. This allowed participants to know exactly how many exchanges they would complete. Any follow-up questions to check for clarity were included at the beginning of the subsequent email.
Email 1. Demographics and background information about the participant.
Email 2. Information about the type of therapy and the therapist.
Email 3. Questions about what was particularly positive in their therapy and the development of a positive therapeutic relationship.
Email 4. Questions around the building of rapport in therapy.
Email 5. Experiences and perceptions of empathy within therapy.
Email 6. Anything further that the participant wished to add, the participant's advice to therapists, and feedback on the interview process.
Each email contained three to five individual questions or prompts, with any follow-up questions included in the first paragraph of the following email. The same questions and prompts were used in the verbal interview over video call.
Data analysis
The researchers analyzed interview transcripts using techniques based on Braun and Clarke’s reflexive thematic analysis. 41
The reflexive thematic analysis involved a six-stage process:
Familiarization with the data. Each email thread was continuously reviewed throughout the conversation to personalize the interview process. After completion, the emails were printed, reread, and annotated with summarizing notes and reflective memos. Coding. Transcripts were coded manually on hard copy to enhance reflection and identify subtleties of meaning. Semantic coding highlighted important sections, followed by more latent coding. Each transcript was coded in isolation to avoid generalizing ideas and codes too early. Generating initial themes. Initial codes were grouped into “condensed codes” and then combined to show shared meanings, concepts, or core ideas and structured into initial thematic maps. Reviewing and developing themes. Z.M. (student researcher) and A.C.W. (supervisor) collaboratively refined different iterations of thematic maps and assessed these for alignment with original data and research objectives. Refining, defining, and naming themes. Theme and code names were adjusted for clarity and flow between concepts through collaborative discussion between Z.M. and A.C.W. Participants were invited to review the final thematic map, and three responded positively with no changes or clarifications suggested. Writing up. Representative quotations were selected to exemplify each subtheme while avoiding repetition of ideas.
Results
The thematic analysis generated three themes comprising eight subthemes (shown in Fig. 1). An expanded mind map showing the condensed and combined codes and how these form each subtheme is available as Supplementary Data.
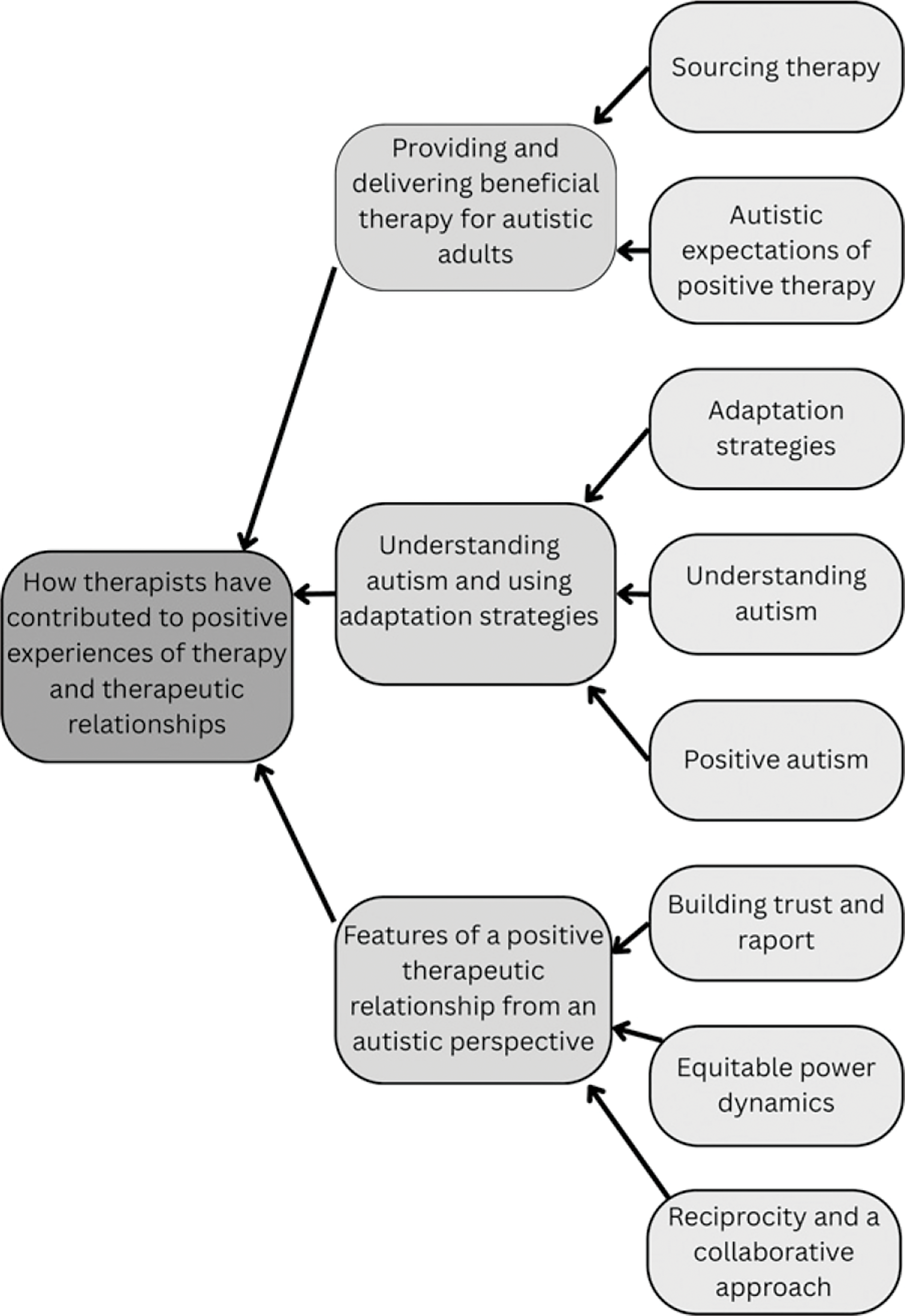
Mind map of themes and subthemes.
Note that participants' quotes are mainly taken from emails (rather than transcriptions); the original spelling, punctuation, and grammar have not been altered or corrected.
Theme 1: Providing and delivering beneficial therapy for autistic adults
This theme provides an overview of the participants’ preferences when sourcing a therapist and their expectations and criteria (including but not limited to the therapist’s specialist mental health knowledge) for deciding that a particular therapeutic intervention felt “positive.”
Sourcing therapy
Participants explained that their reasons for seeking therapy were for support with mental health difficulties (such as anxiety and trauma) rather than autism. They acknowledged that autism was a context for therapy, but not a focus of it.
[P12] “The therapy […] isn’t just based on my autism […] I have anxiety (social and generalised), and lots of other reasons for therapy.”
[P02] “We’ve talked about unmasking but that and post diagnostic stuff hasn’t been the focus of the therapy. We’ve had talks about it in the context of specific issues we’ve been talking about.”
Where options were available when sourcing therapy, participants explained that they wanted the therapist to commit to adapting the therapeutic process to their specific needs as a neurodivergent person.
[P10] “Being willing to adjust whatever modality they’re using to my needs as a neurodivergent person, rather than hammering along the standard protocol no matter what.”
[P08] “She tailored resources to me & it was obvious she had taken time to do this.”
Participants valued having choice and autonomy during the process of sourcing therapy so that they could be more confident the therapy would align with their needs and preferences as an autistic person.
[P03] “A therapist who I found privately through the counselling directory … you can sort of search certain tags or characteristics. So I specifically look for someone with experience with autism.”
[P02] “I wanted ND (neurodiversity) affirming therapy. My therapist is neurodivergent so I knew they would be affirming.”
The downside of this positive neuro-affirming therapy is that it was often only available through private providers, which comes with financial barriers.
[P04] “I feel this was very positive and I felt so understood and validated. Unfortunately I couldn’t afford to carry this on.”
Autistic expectations of positive therapy
Several participants said that for therapy to feel positive it needed to include aspects of achieving results or making progress toward specific goals.
[P10] “For me, positive therapy means making progress towards not needing therapy, rather than simply expressing issues/problems/concerns and feeling heard.”
[P03] “Positive therapy for me is also, it is challenging. She does challenge me, She gets me to think deeply about what I am going to feel and my experiences. Its not just a case of me talking and I’ve had much more shallow therapy experiences in the past.”
For other participants, a key ingredient of positive therapy was having a safe space to explore emotions and receive validation. Participants reported that in therapy they discussed identity confusion, experiences of emotional disconnection, and feeling judged or made to feel “silly or belittled” by historical invalidation. In contrast to these past experiences, 8 of the 12 participants explicitly mentioned the positive effects of feeling validated in therapy.
[P04] “It felt really positive to have a place and time to go and just talk… it was completely non-judgmental and a welcoming environment where I felt accepted … I didn’t always want to talk about traumatic things that have happened. Even if I was paying just to go to a completely accepting and validating place to talk where they didn’t judge - that felt the most positive for me I think.”
Positive therapy for many participants also meant showing curiosity about and celebrating positive experiences and achievements rather than only focusing on difficulties.
[P11] “Taking a genuine interest in my life, celebrating the positives with me, but equally sitting with me and supporting me through the difficult times.”
Theme 2: Features of a positive therapeutic relationship from an autistic perspective
Theme 2 explored the areas that participants highlighted as being of particular importance in creating and maintaining a positive therapeutic relationship for them and examples of how they experienced these relationships.
Building trust and rapport
Therapists being patient, reliable and consistent, perhaps at enhanced levels for autistic clients, helped to build trust. Participants shared that building a trusting relationship helped them see that they mattered and gave them skills that transferred to other relationships.
[P05] “It was a slow build and I needed many months to feel fully comfortable with her […] Her willingness to be patient and encouraging was very helpful in making me feel that I mattered […] I never felt shamed or that she was exhausted with me.”
[P08] “She was always on time for appointments & did what she said she would!”
[P07] “I have had the odd breakthrough moment but mostly for me, it’s the showing up repeatedly, especially when I am ill and not particularly nice to work with (I come out of those patches with stronger relationships if they’re handled well).”
Participants acknowledged that building a rapport with an autistic client can be difficult and can take extra time, although some participants found that the therapeutic relationship developed more quickly. It was helpful for participants to see common ground in terms of shared experiences and shared interests with professionals, which gave them some evidence that the professional was likely to have some understanding of what they were going through.
[P07] “After several months, I felt like a couple of staff members did understand a bit more but not all of them. I was definitely more likely to gravitate towards the ones who had shared a bit more about their own personal experiences during the programme because yes, ‘they got it.’”
Equitable power dynamics
Participants valued having some shared ownership and control over therapy to help them build an empathic and empowering relationship with the therapist.
[P06] “[Not] someone with a ‘strict headmistress’ style if you get what I mean - that don’t come across as approachable or understanding, too clinical.”
The process of relationship building was felt to require explicit well-explained boundaries and consistent transparency.
[P01] “To build rapport I need honesty, transparency, detailed explanation and patience while I question that as much as I need to.”
Several participants described the outcome of building this relationship as sharing some characteristics with friendship.
[P08] “It felt like talking to a friend but I was still aware of her professional boundaries. I felt we had a strong connection.”
Reciprocity and a collaborative approach
Many of the participants mentioned feeling a personal connection, of not just feeling known but of feeling like they knew the therapist. Notably, all participants mentioned some form of appropriate therapist self-disclosure or the sharing of experiences and common ground as being particularly positive.
[P11] “For them to share a bit about themselves too so that I can get to know them as a person a little before sharing so much of myself.”
[P06] “He would sometimes share insights from his own life, nothing too deep or overstepping boundaries, but enough to show that he related and made him seem more genuine.”
While participants noted that some of their therapists already had a good understanding of autism, this appeared less essential than an openness and interest in learning and a willingness to learn alongside the client.
[P01] “She’s open about not knowing something or wondering whether x or y.”
[P10] “During the year-long therapy I had in 2020–21, I discovered I’m autistic […]. My therapist embarked on the voyage of discovery with me - although they were primarily CBT-focused we worked out together which aspects of CBT were useful for me and they borrowed techniques from other modalities when appropriate.”
Participants highlighted that the benefit of an open, collaborative approach was that they shared responsibility for therapy and were empowered to work together on any difficulties in the therapy process.
[P01] “It feels collaborative. That’s also how we work through misunderstandings as there is the assumption that she might not know and we are there working it out together.”
Theme 3: Understanding autism and using adaptation strategies
Theme 3 encompasses particularly positive approaches that participants had experienced, specifically related to higher levels of autism understanding from therapists, including adaptations and attitudes that were found to be either particularly helpful or desirable.
Understanding autism presentation
Participants pointed out the need to understand the heterogeneity of autism and the expression of autism across the different contexts of a person’s life.
[P03] “Understand that every neurodivergent person is different and that there is no one thing that is true for all autistic people, certainly not for all autistic women. Make sure you have an understanding of the fact that being autistic will affect every aspect of that person’s life. It will just manifest very differently depending on who that person is and their experiences.”
[P02] “Respect autistic people as being reliable narrators of their experience.”
Pathologizing autism
Participants highlighted the pitfalls of viewing autism through a neurotypical lens that might tend to pathologize autism. They stated that it was important for the therapists to reflect on their own biases, and to support their clients to reflect on their internalized biases too. Participants explained that the outcome of this would be reduced misunderstanding of autistic behaviors.
[P10] “He consistently picked up on the aspects of myself I saw as negative because they didn’t conform to NT norms and gently reminded me that those aspects weren’t negative or ‘bad’, just different.”
[P02] “If a therapist is NT they need to recognize their own inevitable internalised ableism and work to dismantle that.”
[P04] “It isn’t my thoughts or anxiety, for example, that make supermarkets or loud places overwhelming, it’s because I’m Autistic and it’s upsetting when therapists don’t seem to understand that part.”
Positive autism
Rather than pathologizing and medicalizing autism, participants wanted to be able to build positive autistic identities within therapy and be authentically autistic.
[P03] “They will remind me that [autism] affects aspects of my life that I wouldn’t have thought that it does, and so I feel completely accepted and understood as an autistic person in that room, and that it’s completely acceptable for me to be the autistic person that I am.”
Adaptation strategies
Participants highlighted several key supports that are likely to be useful for therapists adapting the therapy process to autistic clients, for example, giving extra processing time.
[P01] “She also gives plenty of space and time for me to think and process. I never feel rushed. Minutes can pass by with me staring off somewhere trying to burrow down into something and she just waits until I ask her for help.”
Some limited contact outside of therapy was an important adaptation for some participants. This was either before a session to make a plan for an upcoming session, or after a session to allow processing time to extract the key point from a discussion.
[P02] “That made me feel that I’d be safe opening up more […]. Initially I did this by sending her emails before sessions about what I wanted to talk about because I found it too hard to verbalize.”
Participants appreciated clear and direct communication of the acceptance of autistic behaviors such as self-regulation (stimming) and sensory differences.
[P02] “In the beginning I was often dissociated and very stimmy in sessions and this was met with complete acceptance which was a new experience and built trust massively.”
Participants stated that it was important to acknowledge that transitions can be difficult for autistic people, both after sessions and after therapy ends. Transitions relating to video call sessions may be particularly difficult and may benefit from a planned activity to ease the transition.
[P11] “What I found most difficult about this was literally putting the lid down on my laptop at the end of a session, which sometimes had been really challenging, and just being in my own house, without any change of scenery/walk/drive/to help me mentally move out of the therapy session and back into everyday life.”
Several participants mentioned the importance of carefully managing the ending of therapy. Practical suggestions included having other support options pointed out to them and the invitation to rejoin therapy in the future.
[P06] “When my therapy ended he said […] that If i needed help again in future I could contact them and he would work with me again.”
[P03] “Make sure that you’re not just sending them off into the world with the assumption that they’re going to be fine.”
Discussion
This study investigated positive therapeutic experiences within a group of late-diagnosed autistic females and developed three themes: “Providing and delivering beneficial therapy for autistic clients,” “Features of a positive therapeutic relationship from an autistic perspective,” and “Understanding autism and using adaptation strategies.”
Participants discussed their positive experiences across a range of 10 different therapy modalities, demonstrating that diverse therapeutic approaches can meet the needs of autistic clients. One of the key points was that while therapy was not autism-specific, standard protocols often require adjustment and flexibility to maximize benefits for autistic clients. Encouragingly, six participants discussed positive experiences within a public sector health service, and while two participants had specifically selected neurodivergent therapists through private practices, the majority described positive interventions and adaptations achieved with non-autistic therapists.
Positive therapy
When asked what made them define their therapy experience as positive, participants responded that positive therapeutic interventions had to include an element of challenge and progress. They also identified a desire to celebrate positives within therapy rather than to focus exclusively on difficulties, suggesting that identity development may be an important feature of therapy and supporting research by Taylor et al. (2023) that strengths-based approaches are valuable in boosting well-being for autistic clients. 42
Barriers to therapy
Barriers exist in the sourcing of therapy due to limited choice within public sector health services and the financial burden of private services. Therapists may also be reluctant to take on autistic clients due to a lack of confidence or lack of training,12,43 or may view this work as outside their sphere of competent practice. Health care systems must increase their awareness and understanding of autism, particularly in mental health provision. This study highlights that participants who could access private therapy actively sought neuro-affirming therapists, an important consideration for service design and therapist training.
Positive therapeutic relationships
Participants recognized therapist attributes such as curiosity and acceptance as highly positive, which should be reassuring to therapists who enact these traits with their full range of clients. These results complement the discussion by Hume 25 of the importance of the fundamental skills of the therapist in relationship building with their autistic clients, and the need for an enhanced level of the core Rogerian conditions—congruence, empathy, and unconditional regard—for autistic clients.
Participants expressed a strong desire not only to feel that the therapist knew them well but also that they had a sense of knowing the therapist. Therapists sharing limited personal information, sometimes referred to as “therapist self-disclosure,” was consistently mentioned as a positive aspect of therapy, supporting findings from both Hume 25 and O’Brien. 27 Research links therapist self-disclosure to positive outcomes in therapy in the wider population.44–46 However, therapists may feel uncomfortable using self-disclosure due to insufficient training and inconsistent guidelines. 44 Andrade 47 suggests that anecdotal communication styles, such as disclosing personal stories and similar experiences, represent a cultural communication difference. Neurodivergent and some collectivist cultures may use this to show engagement and empathy, while other cultures may misconstrue it as oversharing. Participants described these anecdotal conversations as showing connection, care, and creating a feeling of a “genuine relationship.” While we acknowledge that this will not be appropriate in all forms of therapy, disclosures of personal stories, experiences, and interests may provide an important communication style adjustment where suitable.
Collaboration and authenticity
This study emphasizes the need for an enhanced focus on reciprocity and collaborative approaches with autistic clients to create more equitable power dynamics. Due to differences in social communication styles and past social experiences, autistic people may have a reduced interest in social status and an increased sensitivity and distrust toward hierarchical relationships, which may feel difficult to identify or judge the validity of. 48 Participants particularly valued collaboration, ownership, and control within the therapeutic relationship. For this population, further exploration of relational equity as a therapeutic skill is needed.
The relationship with the therapist and the experience of having a nonjudgmental, validating, and safe space where they felt accepted as their authentic selves were extremely important. Participants described being authentic or unmasked in therapy as cathartic and essential for therapeutic engagement; for some, the therapeutic space was used as a place to explore their own internalized biases and to recognize and deconstruct unconscious camouflaging. Late-diagnosed autistic adults have often learned to rely on camouflaging or masking behaviors. Research links these behaviors to poorer mental health outcomes, reduced sense of self, exhaustion, and feelings of isolation.36,49–52 Recognition of the detrimental effects of these camouflaging behaviors is needed to avoid confusing increased masking with positive progress within therapy 53 and to support positive identity development within therapy.
Adaptations
In their interviews, participants specifically mentioned adaptations to support language processing, sensory regulation, predictability, and increased cognitive processing time. This finding reinforces the well-documented need for physical and cognitive adaptations. Progress may need to be slower to allow for increased processing times within sessions,18,54 and therapists may need to adjust expectations around the pace of relational development and progress. At an organizational level, recognition is needed that flexibility, including around the number or length of sessions, is needed to prevent what Moore et al. (2024) have described as “clinicians feel[ing] constrained when attempting to work flexibly within an inflexible system.” 18 Some participants felt reluctant to use sensory regulation behaviors such as taking shoes off or being able to move around, fearing they “might seem weird.” This highlights the need for explicit, therapist-led conversations around adaptation and sensory regulation to create psychologically safe environments supportive of authentic identity expression.
The heterogeneity of autism means that any adaptation strategies need to be assessed individually in each therapeutic relationship. At the systemic level, services need a greater understanding of autism in general and a recognition of the potential for diagnostic overshadowing. As participants emphasized, there needs to be more focus on preventing the pathologizing of autistic behaviors, such as atypical eye contact, responses relating to sensory issues, or atypical self-regulatory behaviors, and more focus on the positive mental health outcomes the individual desires from therapy, underpinned by a capacity to be authentically themselves.
Limitations and recommendations for future research
As a qualitative research study, the results of this project are not intended to be generalizable to the autistic population as a whole. The findings and examples given should be evaluated for their particular relevance to specific contexts rather than applied universally. This study was specifically focused on the UK population and may not be transferable to other areas where therapy is accessed differently. Some participants disclosed other co-occurring conditions such as attention-deficit/hyperactivity disorder, posttraumatic stress disorder, and borderline personality disorder. While co-occurring conditions are often the rule rather than the exception with autism, these may affect individuals’ needs and experiences in distinct ways compared with the wider autistic population. All participants were females older than 30 years, White British (or dual nationality including British), and had been recently diagnosed (in the last 5 years); as such, these findings may not reflect the experience of other groups of autistic people. Exploring the specific experiences of other groups will illuminate shared needs from therapy and distinct adaptations that may be required. 55 Males in general are less likely to access therapy, 56 so work focused on autistic males may be beneficial, as would focusing on autistic people with learning disabilities, for whom the therapeutic evidence base is poor and who experience significant inequalities in access to health care. 4
The use of asynchronous interview techniques appeared to be particularly beneficial for the participants involved in this study, and all but one participant chose this interview format. For instance, one participant stated, “I much preferred to undertake an email interview than over the phone or via Zoom.” Another participant saw this form of interview as potentially beneficial in other contexts too: “I would definitely like to have this as an offer for other services as well. … This makes participation accessible without the overwhelm and anxiety that goes into having to access new spaces and people.” While asynchronous techniques may risk losing nonverbal cues, this is outweighed in this population by providing participants with the additional processing time needed to provide a more accurate representation of their experiences. The option to use this format may increase the range of respondents and increase accessibility for participants with social communication difficulties.
Our findings indicate the potential importance of the therapeutic relationship in outcomes for therapeutic interventions, and so it may be helpful to examine satisfaction with the therapeutic relationship as a mediator of outcomes in future studies to test interventions. While questionnaire measures exist for therapeutic relationships, future studies may look at adapting these for the autistic population based on elements uncovered in this research.
Conclusion
This study used qualitative techniques to explore the experiences of 12 late-diagnosed autistic females who described therapeutic interventions that had felt particularly positive. It was encouraging to see that both private and public sector interventions and both neurodivergent and non-neurodivergent therapists were discussed as providing particularly beneficial and positive experiences. Physical and cognitive adaptations for autistic clients have been previously researched, and this study supports existing findings that these adaptations increase accessibility when tailored to the individual.17,18 However, the importance of the therapeutic relationship for autistic people has been less researched. Results showed that positive experiences of therapy are founded on the universal “core conditions” of therapy (empathy, congruence, and unconditional positive regard), which do not differ for autistic people, but may benefit from being especially clear, transparent, and explicitly communicated. Participants explained how this helped manage power dynamics and promoted a collaborative approach. Notably, all participants described their therapists being able to develop common ground with them through appropriate sharing of relevant insights, experiences, and interests, and that this particularly supported positive therapeutic relationships. Participants also explained how their positive experiences of therapy relied on therapists having a good understanding of autism, including the less stereotypical presentations, and the ability to recognize and challenge internalized ableism both in themselves and in their clients. In highlighting a diverse range of positive experiences of therapy, we hope this study draws attention to aspects of therapy that will be familiar to clinicians and are well-received by autistic people, as a means of amplifying current good practice and improving mental health outcomes for autistic people.
Footnotes
Authorship Confirmation Statement
Conceptualization: Z.M. and A.C.W. Methodology: Z.M. and A.C.W. Investigation: Z.M. Formal analysis: Z.M. and A.C.W. Writing—original draft: Z.M. Writing—reviewing and editing: Z.M. and A.C.W. Supervision: A.C.W. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.