
Abstract
Given the dearth of research on adulthood in autism prior to the last decade, we need methods to accelerate progress. One area of interest is mental health, but studies focusing on isolated methods or limited sets of constructs are unlikely to rapidly identify the many contributors to autistic adult mental health outcomes. We argue that adopting a multimethod, dimensional approach will more rapidly speed progress. One framework designed to encourage this approach is the National Institute of Mental Health’s Research Diagnostic Criteria (RDoC) initiative. In this article, we describe the utility of the RDoC and considerations for the design of an RDoC-inspired autism study. We demonstrate this via an example focused on suicide because suicide is one serious and well-documented sequelae of poor mental health. This article begins with a brief overview of the significance of suicide to autism. Then, the article outlines key aspects of the RDoC, including consideration of the following: dimensional processes, development, different units of analysis (methods), content domains, and environmental influences. We describe the University of Pittsburgh Autism Center of Excellence as project context; it adds an example of how RDoC can work and concepts to consider when designing an RDoC-inspired autism study. Specific methods and constructs are highlighted that may lead to improved understanding of suicide and mental health in autistic adults, and ultimately to more tailored interventions and supports.
Community Brief
Why is this topic important?
Mental health, and suicide in particular, are high priorities for adult autism research. A slow pace of research is unacceptable for topics such as suicide, given the high rates of suicide deaths in autism. Current research focuses on a small set of variables, which is unlikely to adequately improve our understanding of adult mental health. To speed up our progress, we need new methods and a comprehensive approach to mental health research. We detail new ways to speed up research progress in autistic mental health.
What is the purpose of this article?
In this article, we argue that the National Institute of Mental Health’s Research Diagnostic Criteria (RDoC) initiative may provide an example for designing research studies that can lead to faster progress. We describe the University of Pittsburgh Autism Center of Excellence (Pitt ACE) as an example of how RDoC can work and concepts to consider when designing an RDoC-inspired autism study. Although the Pitt ACE focuses on many aspects of mental health, we describe its suicide emphasis for illustrative purposes and because suicide is one serious well-documented outcome of poor mental health.
What does this article tell us?
This article begins with a brief overview of why suicide research is so relevant to autism and currently used methods. Then, we describe the RDoC approach partnering with the community. We include a discussion of ensuring fit of RDoC to autism via a research approach that integrates input from autistic adults. RDoC emphasizes the value of: (1) studying dimensional processes instead of focusing on categories, (2) using multiple methods ranging from biological through self-report, (3) considering content domains that span negative and positive emotions and responses to negative and positive events, cognitive and social processes, sensory and regulatory processes, and development, and 4) environmental influences. Each aspect of RDoC is considered with examples of how each is applied in the Pitt ACE and why they may be beneficial. We also include promising methods and understudied topics to consider related to suicide. An example from a single participant’s data and experiences illustrates the value of integrating information from multiple methods and concepts. A supplement with the complete Pitt ACE methods includes information on safety protocols, strategies to promote a positive participant experience, and measures that may be useful for others planning studies on autistic adult mental health.
How will this help autistic adults now and in the future?
Autistic adults cannot afford for the pace of research to be slow, especially on topics such as suicide. This article shows how researchers can design studies that will yield more information more quickly. Including a broad range of methods and concepts can identify new areas for prevention and intervention related to suicide. This article also highlights several topics that have received limited attention in adult mental health research. The hope is that the Pitt ACE results, as well as other research inspired by these methods, may provide new avenues for mental health treatment and support for autistic people.
Given the dearth of adult autism research, 1 we need methods to accelerate progress. Studies using isolated methods or limited constructs are unlikely to rapidly identify the many contributors to adult outcomes. We argue that adopting a multimethod, dimensional approach for complex issues such as mental health will speed progress. One framework that encourages this approach is the National Institute of Mental Health (NIMH)’s Research Diagnostic Criteria (RDoC). 2 In this article, we describe RDoC with a project example from the University of Pittsburgh Autism Center of Excellence (Pitt ACE; P50MH130957). We describe its suicide emphasis because suicide is one serious well-documented sequelae of poor mental health.
Suicide Risk in Autism
Autistic adults are more likely to die of suicide than non-autistic peers.3–5 A Denmark nation-wide study found that autistic people aged 10+ were over three times more likely to have a suicide attempt and to die by suicide compared with the non-autistic population. 6 Recent meta-analyses reveal that 15%–24% of autistic adults report suicidal behaviors or attempts in their lifetime.7,8 Over one-third of autistic adults have suicidal thoughts in their lifetime.7,8 However, the prevalence rates of suicidal thoughts and behaviors (STB) in autism vary widely.9,10 Rates differ by demographic factors (e.g., age, sex), methodological factors, recruitment strategies (e.g., clinic-, population-based), and geographic location.3,5,7,9,11,12
Recent reviews and meta-analyses summarize current understanding of risk and protective factors for STB in autism.7,12–16 Some risk factors identified in the general population are also associated with STB in autism (e.g., thwarted belongingness, perceived burdensomeness, loneliness, co-occurring psychiatric conditions, limited access to mental health care, lack of employment). There are additional STB risk factors more specific to autistic people (e.g., masking, or hiding one’s autistic traits to appear more neurotypical; autistic burnout).10,17,18 Emerging work indicates associations between STB and cognitive and emotional characteristics common in autism (e.g., alexithymia, low self-esteem, and emotion dysregulation). 12 There is mixed support for the role of autism characteristics, childhood adversity, and socioeconomic status (SES). Finally, research on protective factors is very limited and inconclusive, with some indication of a positive effect of social support.12,15
Method Gaps in Suicide Research in Autism
While suicide research in autism is increasing, limited research focuses on biological and psychophysiological correlates of STB in autism. Some autism studies indicate an association between STB and biochemical parameters 19 and neurobiological mechanisms such as delayed prefrontal reactivity during cognitive tasks. 20 More biological/psychophysiological research could help identify mechanistic aspects of suicide in autism. In non-autistic populations, biological studies delineated multiple categories of people who are likely to attempt suicide, including people with preserved executive control who plan their attempts carefully versus more impulsive attempters whose executive control is not as preserved. 21 These individuals likely require different approaches to intervention. Work on brain mechanisms has informed the development of multiple interventions for STB from pharmacologies, including recent game-changing interest in ketamine, 22 to brain stimulation approaches 23 and chronotherapeutic methods. 24
Suicide prevention and intervention research for autistic people is similarly nascent, although there is recent interest in this area. As an important starting point to guide suicide risk evaluations and safety planning, researchers examined the feasibility and efficacy of adapting safety plans for autistic people. 25 Furthermore, a recent study found that Dialectical Behavior Therapy reduced STB in autistic people, 11 which is promising given its established and widespread use. To date, prevention and intervention efforts primarily rely on clinical knowledge and pull from approaches used in non-autistic samples, likely due to the lack of research on STB in autism.
Valid measurement is a barrier to suicide research in autism. Questionnaires of suicidality designed for non-autistic individuals have different psychometric properties in autistic individuals. 26 Furthermore, autistic adults report difficulties with vagueness of Likert response options, questions about if they would “someday” do something, nonliteral language (e.g., saying you are “blue” to assess depression), comparing their thoughts or behavior with others, and how contexts may change responses.26–28 There may also be important considerations regarding assessment methods. One study found that nearly one in five autistic adolescents endorsed suicidal thoughts via self-report but not via a clinician-administered interview, indicating the need for a multimethod assessment. 29
The majority of STB research in autism has relied upon single methods (typically self-report) in online-recruited convenience samples, small clinic-based samples, or medical records in large population-based samples. Overuse of convenience samples risks generalization from biased samples that are largely composed of participants who are female, high education level and SES, and diagnosed as adults. 7 Clinic-based samples are often restricted to collecting a small set of predictors. The use of large-scale medical or death records limits the use of many known predictors and excludes individuals without diagnosed autism or access to health care. 30 Lastly, most research focused on categorical (presence or absence of STB) rather than a continuum of suicide risk, which may miss (or not allow us to measure relative salience of) key factors associated with suicidality and mental health.
The RDoC Initiative
Suicide is multidetermined, arising from a complex interplay of factors. As such, an emphasis on categorical risk factors is unlikely to be sufficiently informative. For example, identification of demographic and psychiatric diagnosis risk factors led to minimal improvement in the prevention of suicide in the general population. 31 The dynamic nature of suicide requires an approach that goes beyond single methods or cross-sectional designs.
RDoC is a framework led by the NIMH (Fig. 1). 2 Beginning in 2009, experts in different content areas met to develop an organizing structure with guidelines and suggestions based on available empirical evidence. RDoC is dynamic; it can be updated as scientific findings progress, as well as modified for specific questions.
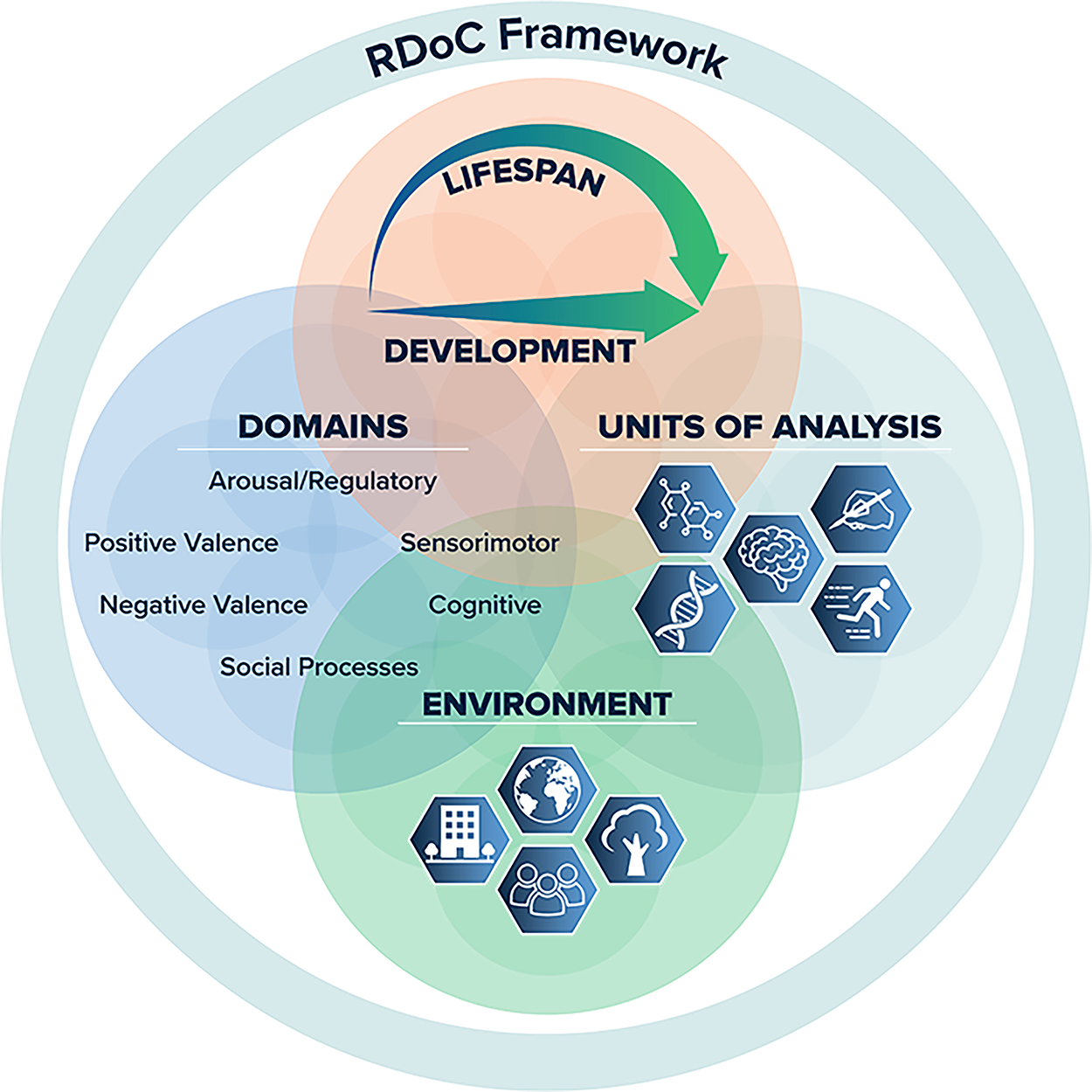
Research Domain Criteria (RDoC) Framework reproduced from https://www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/about-rdoc where more descriptive information on the figure can also be found.
RDoC intended to address limitations in categorical diagnostic boundaries and concern over a focus on diagnostic symptoms as defined by the Diagnostic and Statistical Manual of Mental Disorders. 32 A diagnosis-focused approach may not reflect underlying biological processes. Furthermore, a single mental health condition (e.g., major depression) likely evolves from multiple neurobiological and psychosocial mechanisms, some of which may be shared with other conditions. RDoC is therefore focused on dimensional mental health processes versus categories (diagnoses). It emphasizes translational and integrative research. The ultimate goal is to support better precision medicine and perhaps more refined ways of defining mental health concerns.
RDoC outlines Units of Analysis or methods, including genes, molecules, cells, circuits, physiology, behavior, self-report, and paradigms. RDoC outlines Domains, including negative valence systems, positive valence systems, cognitive systems, social processes, arousal and regulatory systems, and sensorimotor systems added later (Table 1 for definitions). Within each domain, examples are given of possible measures and paradigms across different units of analysis to form a matrix. Finally, RDoC suggests consideration of both Development and Environment (Table 2). These RDoC pillars are explained in more detail below in the context of examples from an RDoC-inspired autism study.
Research Domain Criteria Matrix Example: Domains and Units of Analysis in the Pitt ACE Including Promising Constructs and Methods for Autism Suicide-Focused Research
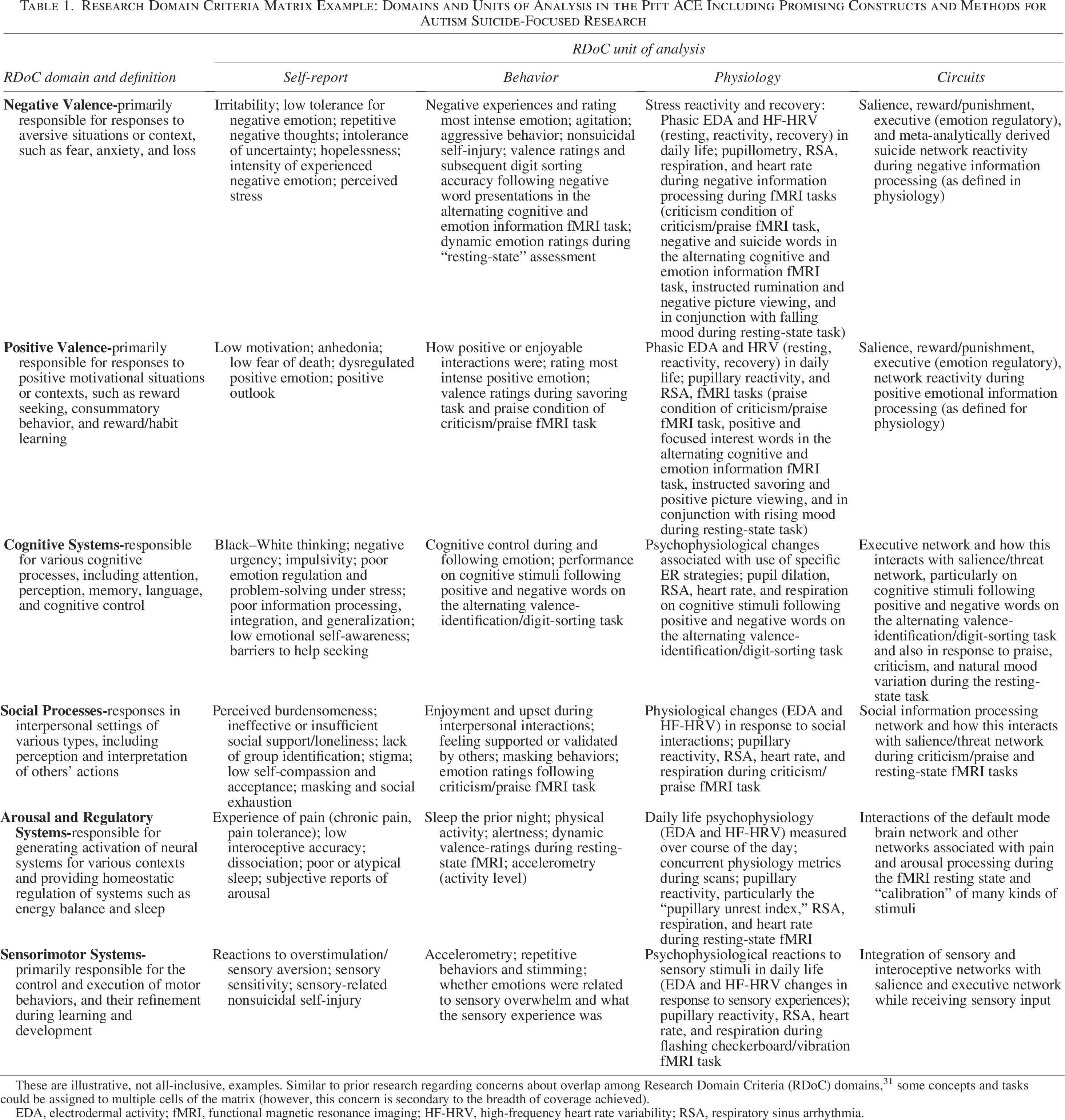
These are illustrative, not all-inclusive, examples. Similar to prior research regarding concerns about overlap among Research Domain Criteria (RDoC) domains, 31 some concepts and tasks could be assigned to multiple cells of the matrix (however, this concern is secondary to the breadth of coverage achieved).
EDA, electrodermal activity; fMRI, functional magnetic resonance imaging; HF-HRV, high-frequency heart rate variability; RSA, respiratory sinus arrhythmia.
Research Domain Criteria’s Focus on Dimensional Processes, Development, and the Environment: Pitt ACE Methods and Construct Examples
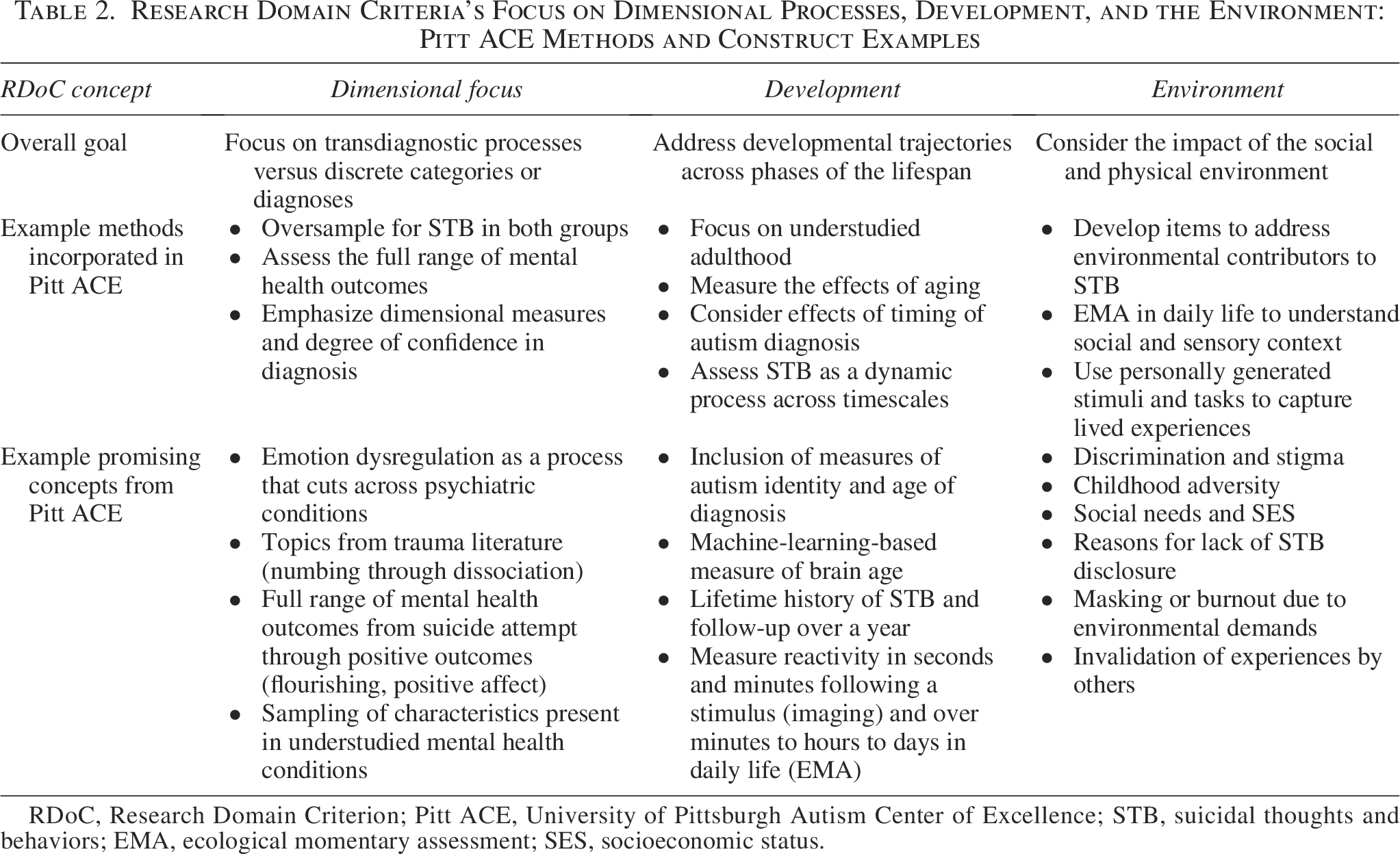
RDoC, Research Domain Criterion; Pitt ACE, University of Pittsburgh Autism Center of Excellence; STB, suicidal thoughts and behaviors; EMA, ecological momentary assessment; SES, socioeconomic status.
Applications of RDoC Outside of Autism
A summary of the first decade of progress related to RDoC noted over 1000 articles from 17 specific RDoC funding announcements 33 ; this does not take into account research with different funding sources. RDoC led to alternative conceptualizations and designs, such as recruiting based on a particular characteristic as opposed to a diagnosis and an emphasis on mind–body connections.
Because deaths continue to rise despite decades of suicide prevention research, some suicide researchers suggested considering whether alternative frameworks, such as RDoC, might identify novel risk factors for suicide. Glenn et al. 31 conducted a meta-analysis of suicide studies to determine how they map onto the RDoC. They found that most studies focused on categorical predictors with limited consideration of RDoC constructs related to suicidality. Critically, Glenn et al. 31 concluded (pp. 85):
“In line with findings from prior meta-analyses,34,35 this review found that the effect size for any single predictor (or domain) was relatively small, especially after accounting for publication bias. This highlights the need for research to identify novel risk factors for suicide (e.g., factors related to understudied RDoC domains, like Positive Valence Systems), as well as empirically informed ways to combine factors to improve risk prediction.”
In autism, an emphasis on mental health diagnoses may be even more problematic, given that the majority of autistic people meet the criteria for multiple mental health diagnoses when administered structured psychiatric interviews 36 and differential diagnosis from autism is unreliable. 37 Integrating different units of analysis is also essential given a push from autistic adults to include their own perspective (self-report) combined with a need for objective indicators, not biased by a desire to hide suicide plans or lack of insight. 31
Applying the RDoC Framework: Key Points and Examples from the Pitt ACE Study
The Pitt ACE is a research study designed to advance research on adult mental health and suicide using an RDoC framework. We first provide a brief overview of the different study components for project context. Next, we consider how to ensure RDoC’s relevance to autism. Then, we discuss each core RDoC tenet with Pitt ACE examples to illustrate how RDoC can be applied, including transferable lessons that include specific methods and constructs that are important to consider related to suicide/mental health research in autistic adults.
Pitt ACE project context
The Pitt ACE includes three components, each of which emphasizes a different unit of analysis and taps all RDoC domains in different ways, offering examples of different approaches to embed RDoC into research on suicide/mental health in autism. Full method details are in the Supplementary Data to support their use in other studies.
Component 1 (self-report) is developing dimensional self-report questionnaires of suicide risk in autistic people (The Pittsbur). Rather than including direct questions about intent and plans, the new measure intends to capture the propensity for suicide risk by considering a broad range of factors that may make someone more or less likely to have STB (using RDoC as a conceptual model). We follow the Patient-Reported Outcome Measures System (PROMIS® 38 ) measure development standards (see Supplementary Data S1). Repeated completion of the measure by our Pitt ACE cohort within the context of a longitudinal design will identify suicide risk trajectories.
In Component 2 (behavior and physiology), participants wear two ambulatory physiological sensors during waking hours (at least 12 hours/day) for 14 days. Concurrently, participants complete eight brief ecological momentary assessment (EMA) surveys per day; up to half are triggered by changes in physiology, with the remaining surveys arriving at random intervals. These data will characterize proximal risk STB processes in a temporally sensitive manner, such as how emotional reactivity, context, and patterns of physiological arousal predict near-term (e.g., hourly and daily) within-person STB increases.
Component 3 (circuits) is testing a neural mechanistic model to understand why autistic people often report strong emotional reactions but may not show them in conventional ways (e.g., flat facial affect, not asking for help). We examine neural responses to emotional and sensory stimuli and ask participants about their reactions to their individual neuroimaging data. In addition to structural and diffusion-weighted images (magnetic resonance imaging, MRI), participants complete functional neuroimaging (fMRI) tasks. Imaging data will then be connected to self-report measures of mental health and STB using computational modeling.
Key point 1: Ensure RDoC’s relevance to autism and that methods are autism affirming
We included autistic adults when considering how to apply RDoC in the Pitt ACE design. Autistic adults are part of the team as investigators, consultants, and staff. Our participatory group of autistic adults, the Pittsburgh Adult Autism Research Community Collaborative, meets 10 times/year to guide all community engagement, dissemination, and procedures. As such, autistic adults are integrated at all stages of the center to ensure that our research is grounded in lived experience and is meaningful to the autistic community.39,40 Examples of autistic partners’ input include conceptualization, measure selection, and how to support participant well-being in a demanding and potentially emotionally draining study (Supplementary Data S1 provides details).
Key point 2: Embody RDoC’s dimensional emphasis
RDoC moves away from a focus on mental health diagnoses or traditional symptoms (Table 2). Focusing on categorical diagnoses is insufficiently specific (e.g., not everyone who is depressed experiences suicidal thoughts), STB are present transdiagnostically, and there are discrepancies within autism; that is, reported rates of depression 41 that are lower than the reported rates of STB.
So, how can one focus on a specific population (autistic people) and still embody RDoC’s dimensional emphasis? First, the project can remain centered on a dimensional process by recruiting for a wide range of the construct of interest. For example, we oversample for recent STB in both autistic and non-autistic adults and we are inclusive of those who have never experienced any STB.
Second, one can situate the topic within other potentially related transdiagnostic processes. For example, we assess mental health conditions that include elevated rates of suicide, including those that are understudied in autism (e.g., personality disorders). We include transdiagnostic emotional constructs such as emotion dysregulation because it is elevated in autism and associated with many mental health outcomes, including suicidality.14,42 We consider processes implicated in trauma but less studied in autism, for example, numbing and dissociation.2,43 It is also important to consider the full dimension of mental health inclusive of positive well-being indicators, such as positive affect and life satisfaction.
Finally, we acknowledge the limits of categorical approaches and explore opportunities to address this. Often diagnosis of mental health conditions in autism varies depending on the measure used, reflected by the wide published rates (e.g., anxiety ranging from 1.5% to 54%; depressive conditions from 2.5% to 47%). 44 Thus, we derive a novel “certainty” index from dimensional measures.45,46 Advantages of this method over traditional approaches include its focus on a person’s individual pattern of mental health concerns rather than simple diagnostic criteria counts, and it quantifies the degree of confidence associated with a diagnosis in probabilistic terms (0%−100%).
Key point 3: Consider different units of analysis
RDoC provides links to examples of specific methods that map onto different units of analysis and possible paradigms (www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/units). The idea of different units of analysis is similar to the long-held notion of the value of multimethod assessment. In terms of mental health, emotion is considered a multicomponent process, including behavior, neural activity, physiological arousal, and subjective experience. 47 Consideration of one form of information likely provides an incomplete understanding of how difficulties arise and therefore limits ideas on how to provide support. Our overall approach to ensuring multiple units of analysis is to enroll a core cohort that completes deep phenotyping plus the three study components that emphasize a different primary unit of analysis (Table 1).
Self-report
We obtain self-report via traditional interviews and existing questionnaires (Supplementary Data lists measures). Given concerns regarding the validity and psychometric soundness of many self-report measures in autism,48,49 it is important to draw first from those that have been modified for, developed for, or validated in autism. There may be instances when nothing exists; in our case, we aimed to develop a self-report of processes that contribute to suicide risk in autism as part of our self-report focus. This involves a systematic and iterative process to ensure content coverage and develop optimal wording (Supplementary Data S1 and see prior50–54 ). Through the measure development process, we will learn which types of items are most strongly linked to suicidality in autism. EMA can also be an ideal method to capture RDoC self-report in daily life. Although EMA can use standardized questionnaires, often it is a small set of questions developed for a specific study. If not standardized, it is helpful to develop them in partnership with autistic adults, as we did to ensure mutual understanding in the meaning of the questions. Finally, self-report can be embedded within other modalities—for example, participants continually rate their emotion during a resting-state imaging task.
Physiology
RDoC uses physiology to refer to measures that are well-established (e.g., heart rate, cortisol) but not directly related to circuits. Several aspects of physiology associate with emotion; for instance, both parasympathetic and sympathetic activities are linked to self-regulation transdiagnostically.55–57 There is also previous work demonstrating an association between parasympathetic58,59 and sympathetic 60 measures of physiological arousal and emotion dysregulation in autistic children. To assess physiology, participants in the Pitt ACE wear two ambulatory physiological sensors during waking hours. One sensor is worn on the chest to measure electrocardiogram, which provides information on parasympathetic activity (high-frequency heart rate variability, HF-HRV). The other sensor is worn on the foot to assess electrodermal activity, a measure of sympathetic activity. We find that this is both feasible and acceptable, with high rates of compliance that are similar to non-autistic adults. It is also feasible to obtain measures of physiology during neuroimaging; for example, using standard MRI equipment, we collect respiration and pulse plethysmography during MRI scans, which allows derivation of HF-HRV. 61
Behavior
The behavior domain emphasizes observations and tasks. These can be collected passively; for example, from pupillary motility we can derive the well-established Pupillary Unrest Index, a measure of variability in pupil diameter representing momentary fatigue. 62 This provides an opportunity to understand if autistic adults have higher resting fatigue and how this may associate with burnout. Another passive example is accelerometry, which measures movement/physical activity; we obtain this via both our chest and ankle sensors. In addition, we measure behavior via performance during structured tasks (paradigms). Response to paradigms is the crux of functional MRI. Consistent with our goal of measuring reactivity to emotional stimuli, we include five tasks (multimodal sensory stimulation, reactivity to criticism, and emotional words and pictures, as well as instructed rumination and savoring; see Supplementary Data S1), with some providing additional opportunities to measure behavior via performance metrics and valence ratings. Although there are some established paradigms for measuring RDoC domains (www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/units/paradigms), we instead selected tasks to enhance relevance to autistic and suicidal adults (e.g., suicide relevant, sensory, and personally generated stimuli relevant to intense interests). Finally, RDoC includes a list of “elements” (concepts) under behavior (www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/units/behaviors). Many of these can be assessed via EMA (i.e., rumination, affective states, sensory reactivity), as we are doing. Table 1 and the Supplementary Data provide further examples.
Circuits
RDoC circuits can be measured via neuroimaging, animal models, or functional neuroimaging. Many forms of neuroimaging are utilized to understand STB in the general literature as summarized in prior reviews/meta-analyses (i.e., STB,63–65 emotion dysregulation,66–68 ) However, there are no other STB-focused neuroimaging studies with autistic people, and this is an important RDoC unit of analysis to consider. In our study, we obtain a high resolution T1-weighted structural image, diffusion-weighted images, and fMRI with eye-tracking. We selected tasks based on publications suggesting that they elicit activity in circuits of interest (i.e., salience, executive, sensation networks) and those identified more recently via suicide research (Table 1). Thus, our planned analyses are at the circuit/network level and our automated processing stream extracts network-wise indices.
Cells, molecules, and genes
It is rarely possible to include all RDoC units of analysis in a single project; indeed, the Pitt ACE does not measure cells, molecules, or genes. Nonetheless, basic science provides an important foundational basis related to mental health. For example, there is research suggesting gene-by-environment interactions such as genetic susceptibilities to experience more negative outcomes following stress or adversity, and genetic and cellular changes that may occur following adversity.69,70 Understanding these processes will be important for a complete understanding of risk and resilience. Furthermore, there is emerging evidence to suggest overlap between genes implicated in suicide and in autism, which may also imply biological pathways that confer risk.69,71,72 Researchers who include cellular and molecular units of analysis should partner with autistic adults in the design of their study, especially ensuring that they understand concerns regarding the possibility for misuse of genetic information. Maintaining focus on questions that could lead to better supportive and personalized care would be critical.
Key point 4: Consider different major domains
RDoC offers domains intended to capture major systems of emotion, cognition, motivation, and social behavior (Table 1), as well as subconstructs within each domain and examples of paradigms and measures for each (www.nimh.nih.gov/research/research-funded-by-nimh/rdoc/definitions-of-the-rdoc-domains-and-constructs). It may be helpful to consider supplementing RDoC’s predefined suggestions to include autism-relevant concepts, with the support of autistic partners. For example, there are other aspects of social processes that we felt might have an even stronger relationship to suicidality (e.g., thwarted belonging), and social processes not described by RDoC that are pertinent for autism (e.g., autistic burnout). We provide examples (Table 1) with relevance to suicide (and mental health) in autism across the six RDoC domains and four different units of analysis.
It is not necessary to include every RDoC domain in an RDoC-informed study. Nonetheless, this is helpful when focusing on a topic such as suicide in autism, which has limited empirical data to draw upon. Focusing on only a narrow set of constructs identified in prior empirical or theoretical work may result in missing the discovery of potentially important concepts. Therefore, we ensured that each RDoC domain is measured in each Pitt ACE component. Later analyses will help refine and narrow constructs with the most relevance to suicidality in autism.
There are many options to measure domains. We used the RDoC domains as a factor in the conceptual model for our new measure development. This model is then used to support item generation, by developing facets within each RDoC domain. For example, we developed items related to negative valence, social processes, etc. that may capture variability in suicide risk. Importantly, we do not expect this to replicate the RDoC domains but are hopeful that the broad content coverage will result in the discovery of novel and sensitive items. An additional option is to develop a small set of questions to cover each domain; for example, we did this for the content of the EMA surveys. Finally, the selection of our neuroimaging tasks is structured to include paradigms that map onto the domains and planned analyses of brain networks thought to underlie domains (Table 1; Supplementary Data S1).
Key point 5: Consider environmental influences
RDoC encourages consideration of environment but provides limited guidance. RDoC mentions the social and physical environment, early childhood stressors, how one’s behavior impacts their environment, and that environmental influences can include both risk and protective factors. Such environmental features are generally understudied in autism, although aspects of the neurodiversity movement are shifting the dialogue to a greater focus on how society plays a role in contributing to disability. 73 To identify additional environmental and contextual factors, we drew from themes related to mental health from qualitative interviews with autistic adults.74,75 Therefore, we included concepts such as reluctance to share suicidal thoughts due to fear of consequences or that no one will believe them. Because autistic adults report that sensory and emotion dysregulation is often entangled, 75 we explore the role of exhaustion resulting from sensory input in the environment.
We also emphasize environmental factors associated with suicide in non-autistic samples, such as discrimination76,77 and trauma,78,79 which are generally understudied in autism. Autistic people are a marginalized group that frequently experiences discrimination in daily life.80–82 Autistic people are at much higher risk for trauma, including physical and sexual abuse and neglect, as well as nontraditional trauma.83,84 Similarly, social needs (e.g., food or housing insecurity) are linked to mental health in non-autism research.85–87 Many autistic adults are unemployed and have a limited income,88,89 factors linked to depression. 90 We include metrics of childhood SES in addition to current employment, income, use of federal assistance programs, and subjective SES, where individuals place themselves ranked on an SES ladder. Subjective SES relates more strongly with psychological well-being than objective SES in the general population. 91 This approach may be particularly relevant in autism, given that many adults live with support people and it can be an arbitrary decision to choose household versus individual indicators of SES.
It is also helpful to consider environment at the level of one’s daily experiences. EMA is a promising method for elucidating real-time contextual patterns related to mental health outcomes in autistic adults.92–94 While EMA could assess some of the above concepts (e.g., discrimination), we use EMA to identify patterns of emotional reactivity and recovery and the utilization and effectiveness of a variety of emotion regulation strategies in response to environmental (contextual) triggers, such as social/nonsocial situations, sensory, and daily life events. We combine EMA with passive and continuous assessment of physiology to characterize the contextual precipitants and components of experiences in daily life across multiple response systems. This will allow us to link these components to near-term events (including STB, use of masking). Prior studies of emotion regulation and physiological arousal in autism almost exclusively used laboratory paradigms and cross-sectional methods, which limits our ability to capture how these processes unfold across various environmental contexts and experiences. Emotional reactivity to social situations in autistic adults may be elevated but varies based on context, particularly social factors such as familiarity. 95
Environmental influences can also be probed via tasks that integrate standard RDoC assessments with autism- and person-specific stimuli. Pitt ACE participants generate prompts for positive, negative, and neutral stimuli that they encounter in daily life (i.e., criticism, praise, words with negative or positive meaning, and things that are most interesting to them). Sensory processing is directly measured via a task that provides sensory input. These tasks during fMRI may provide insight into how one’s neural responses vary based on stimuli that have real-world meaning and better capture one’s lived environment.
Key point 6: Consider development
RDoC suggests consideration of development but does not provide guidance. The Pitt ACE is focused on the understudied-in-autism period of adulthood 1 through the lens of developmental constructs important to mental health, such as timing of the autism diagnosis (given increased mental health concerns among adult-diagnosed 96 ). It may be important to consider both specific developmental periods across the life course and how they intersect with autism identity.
We consider aging. It is generally unknown how the brain changes across adulthood in autism. We apply a machine learning model 97 that contextualizes whole-brain structural information from our Pitt ACE sample against structural information from a large normative participant cohort to generate a prediction of the participant’s chronological age. Discrepancies between chronological and predicted brain age may indicate disruption or accelerated aging, allowing us to then see how this relates to STB. Future work is needed to explore the intersection between mental health and aging.
It is also critical to move away from time-invariant studies of suicide risk (i.e., those that describe risk in a static way at one point in time). Suicide risk is inherently dynamic, fluctuating considerably within and across days, often with rapid onset and short duration.98,99 Therefore, we assess different timescales related to suicidality. For example, we obtain a full lifetime history of STB via interview. 100 We also characterize current experiences and behavior that may relate to suicidality. Our EMA protocol includes eight surveys/day over 2 weeks, providing a timescale spanning minutes to days. We characterize neural reactivity in the seconds after stimuli are presented. Finally, interviews and questionnaires are repeated after 6 and 12 months to track changes longitudinally. Together, this enables us to understand the development of suicidality with attention to fluctuation over different timescales.
The Value of Integrating
Translational research is a pillar of RDoC. It provides an opportunity to integrate data across domains and units of analysis, which is faster and provides more insights than considering each in isolation in succession. In the Pitt ACE, data can be pooled for integrative analyses (Supplementary Data has examples of different analytical approaches). Many tangible outcomes can result from this approach, such as: (a) connecting a biological causal mechanism to lived experiences and longitudinal outcomes, (b) validating a feasible questionnaire against physiologically triggered self-reports in daily life, and (c) examining how subgroups of individuals with similar patterns of emotion dysregulation in daily life differ in terms of clinical features, neural circuits, and suicide risk trajectories. Integrating neurobiological information (physiology and neural reactivity) with self-report and behavioral data can provide a clearer mechanistic account of how suicidality develops. Through integration, we can test a “bottom-up” framework for how neural reactivity may lead to emotion dysregulation in daily life, and how intersectionality of processes results in suicidality. Finally, pooling data across units of analysis and domains supports the identification of relative contributions of different factors and the strongest predictors of suicidality for autistic adults, possibly uncovering connections not previously considered.
Ultimately, the goal of research is to improve quality of life for autistic people, so it should yield clinically actionable and informative information. Integration across units of analysis and domains enables this, such as identifying physiological patterns that precede a behavior to provide opportunities for biofeedback or just-in-time interventions. Understanding how one’s brain responds to certain stimuli can provide the context for experiences. For example, understanding if brain networks for regulatory control shut down following criticism can provide relief for those who do not understand why they feel “paralyzed” in stressful situations. Understanding whether neural responses are increased or decreased is important for identifying the most suitable psychosocial strategies.
Illustrative example
We illustrate with one participant’s data that an RDoC approach combining multiple units of analysis and domains can yield insights that are more comprehensive than if considered individually. The participant (“Sam”) reviewed and agreed with the conceptualization.
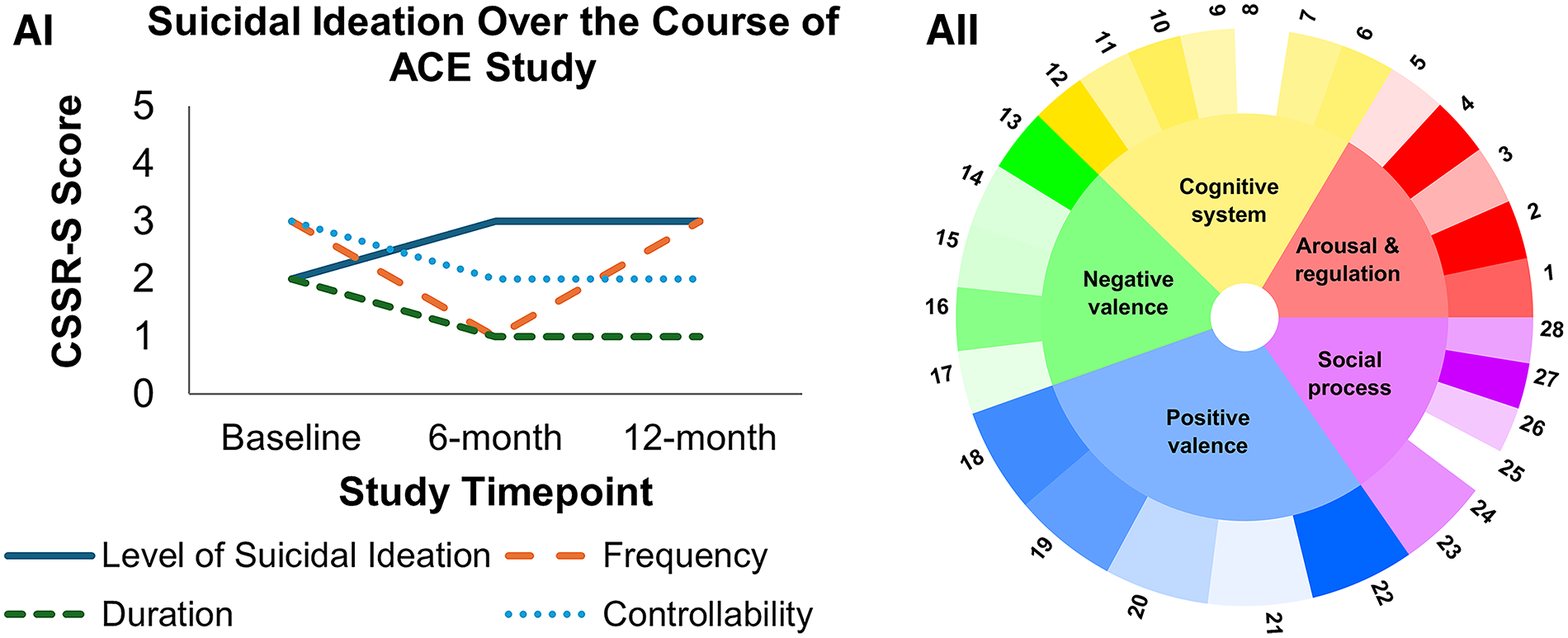
Sam is 38 years old, diagnosed autistic in adulthood, nonbinary (female at birth), White, and non-Hispanic participant. The IQ was 123, ADOS-2 comparison score was 6 (range 0–10; cutoff: 4), and total CATI score was 138 (middle 50%: 93–132). They presented as melancholic, with sometimes discordant affect (e.g., joking about death). Regarding lifetime, Sam had three aborted suicide attempts, and active suicidal thoughts with some intent to act but without specific plan. They indicated 6-month history of nonspecific active suicidal thoughts without intent (Fig. 2A-I).

(Continued).
Responses to the new items we developed provided a broad picture of RDoC domains for Sam (Fig. 2A-II). Sam rated many traditional risk factors, such as burdensomeness and low belongingness, 101 as “not at all” true of them. They rated many positive valence features (difficulty motivating, anhedonia) as “very much” true of them. Other highly endorsed facets included low self-compassion, perseverative self-critical thoughts, interoceptive difficulties, and sleep difficulties.
The neuroimaging connects the self-report data to mechanisms. Criticism (Fig. 2B-III) increased activity in brain networks associated with body processing (sensation, interoceptive, pain networks). Sam described criticism as physically painful, consistent with their description of their suicidal thoughts as pertaining to ending pain. However, criticism also decreased activity in emotion- and arousal-associated brain networks (Fig. 2B-V), and praise resulted in widespread decreased neural reactivity. This helps explain self-reports of numbing and anhedonia by suggesting that Sam actually lacks reactivity versus struggles to identify emotions. Flashing checkerboards produced similar widespread decreased neural reactivity, which Sam reported caused them to “space out” (Fig. 2B-IV), consistent with their endorsement of some dissociation items. Dissociation often happens in the context of sensory overstimulation.102,103 However, adding vibration mitigated this effect 104 as shown by relatively increased reactivity across brain networks in comparison with checkerboards alone (Fig. 2B-IV). The meta-analytically derived suicide network, which more strongly represents visual processing regions than the other a priori networks, was more active than other networks; this could be a function of processing the intense visual stimulus along with its feedback to emotion circuitry.
Data from EMA and physiology indicated that high desire to die/hurt themself in real-world situations associated with physiological arousal and self-reported affective states. An index of general arousal, sympathetic tone as measured by skin conductance, was high preceding episodes of elevated desire to die (Fig. 2C-VI) and/or self-harm (Fig. 2C-VI). Other physiological indices associated with high sympathetic arousal and emotion regulatory control demonstrated this pattern as well (Fig. 2C-VII). From the EMA data, desire to die and felt arousal (r = 0.3, p < 0.01) and negative affect (r = 0.39, p < 0.01) correlated positively, but the desire to die was not correlated with positive affect. Increased negative affect also correlated with the desire to self-harm (r = 0.24, p = 0.01). This mirrored their response to the new item bank, “I think about self-harm as a way to calm my emotions.”
Thus, our multimethod assessments suggested broadly decreased neural reactivity to positive and sensory information as a mechanism for Sam’s self-report of anhedonia, consistent with our clinical identification of higher order blunting construct. 105 High neural reactivity to negative information explains why Sam’s negative affect and increased arousal preceded proximal real-world suicidal thoughts. The data identified possible clinical directions (i.e., improving self-compassion and increasing reactivity via training in savoring of positive experiences,106,107 use of somatic intervention strategies 108 ) that would have been harder to identify via a single method and slower to discover had we only considered one construct at a time. For example, focusing first on negative valence would miss the critical role of positive valence, and introducing a negative social stimulus without the sensory component would miss the restorative effect of sensory input for Sam. Overall, this example concurred with Glenn et al.’s 31 conclusions regarding the value of understudied RDoC constructs (i.e., positive valence) for suicide research.
Summary
Suicide is a priority for autism research but research is in its infancy. We argue that the RDoC provides a methodological framework that can support faster and more comprehensive scientific advances on mental health and suicide in autism. RDoC emphasizes dimensional and translational research on mental health. It provides guidance on including different units of analysis and domains (Table 1) and emphasizes the importance of focusing on dimensional processes, development, and the environment (Table 2).
The Pitt ACE is as an example of an RDoC-informed study developed via a participatory approach and designed to generate information on the nature of daily emotional experiences and fundamental mechanisms underlying mental health and suicidality in autism across adulthood. It is an example that offers many transferable lessons for others who wish to apply this approach. We presented strong justification to include different units of analysis in suicide research, such as self-report (including potentially the development of new measures), physiology, behavior, and circuits. Units of analysis can also be combined to enhance their impact, as demonstrated by our use of physiology to trigger self-report surveys. RDoC domains can be assessed in multiple ways, including as the basis of a conceptual model, by drafting individual questions for questionnaires or surveys that tap different domains, or through the selection of structured tasks. Finally, the environment can be captured through inclusion of items/questionnaires of potential environmental contributors, by asking questions in real time in daily life as experiences in the environment unfold, or through tasks that elicit different environmental experiences such as sensory sensations. There are many topics identified above that warrant further study in suicide research and have been understudied in autism to date.
Although the examples from the Pitt ACE provide some direction, there are additional needs for future suicide research in autism. Although a year’s follow-up is a start, longer term studies would elucidate the interplay between mental health and physical and cognitive aspects of aging in autism. Research in other populations indicates that chronic stress may accelerate aging 109 and there is a higher risk for suicide among those with cognitive decline or older age. 110 Furthermore, because we aimed to include as many units of analysis and domains as feasible, this limited eligibility to autistic adults who could complete self-report measures and understand task instructions. Future research is needed to understand how suicidal intent presents in those less able to self-report. We began with a focus on developing measures and methods and identifying mechanisms, all critical first steps to improve understanding of suicide in autism and to support future research. Ultimately, the goal is to translate this into more focused prevention, intervention, and service options.
Footnotes
Acknowledgments
Most importantly, the authors are especially grateful to the participants who support this research. They acknowledge the Pitt ACE co-investigators, including Lan Yu, Paul Pilkonis, David Brent, Helmet Karim, Aiden Wright, Yukari Takarae, Oliver Lindheim, Satish Iyengar, Judy Chang, Valire Copeland, Jessie Northrup, and Jamie Kulzer. They also thank the Pitt ACE consultants, including Anne Kirby, Jessica Schwartzman, Zack Williams, Neil Jones, Gabriel Dichter, Christina Nicolaidis, Beatriz Luna, and Kaite Gotham. The authors thank the community advisors, Lisa Morgan, Moreniké Giwa Onaiwu, Camille Proctor, Lu Randall, Paula Kauffman Oberly, Jamie Upshaw, and the Pittsburgh Adult Autism Research Community Collaborative (PAARCC) group for their input and guidance throughout this research. They appreciate the guidance of their Scientific Advisory Board, including Drs. Susan White, Shanter Alexander, Vanessa Bal, Christa Labouliere, Chelsea Potts, Mikle South, and Daniel Wilkenfeld. This work would not be possible without the amazing staff and trainees, including Sarah Brammell, Betsy Butler, Rebecca Cohen, Mario Crown, Safaa Eldeeb, Jacob Feldman, Holly Gastgeb, Laura Greenert, Rachel Harris, Amanda Johnston, Claire Klein, August Saunders, Kristen MacKenzie, Anna Lausberg, Amy Ionadi, Lillian Manna, PJ McCarroll, Emily Nettesheim, Shelby Parsons, Teal Raffaele, Lynda Rose, Olivia Boden, Christine Savoie, Shannon Sloan, Michelle Perrin, Derica Su, Katy Zeglen, and the University of Pittsburgh Office of Academic Computing.
Author Disclosure Statement
G.J.S. has a patent through the University of Pittsburgh that is licensed by Apollo Neuroscience; this work is not discussed here. The authors have no other conflicts to disclose.
Funding Information
This work was funded by NIMH P50MH130957. LA was supported by NIMH T32MH018951 during the preparation of this manuscript.
Authorship Confirmation Statement
All the authors approved this article. All authors contributed to conceptualization. C.A.M. received the funding for this work and wrote the first draft. All authors reviewed and edited. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.