
Abstract
Background:
Many autistic individuals struggle with poor mental health and low self-esteem, in part, due to internalized stigma. Given the strengths-based perspective of the neurodiversity framework, it is likely that endorsing it or its subcomponents could serve as a protective factor against poor mental health and low self-esteem among autistic individuals.
Methods:
The present study sought to investigate (1) the relationship between endorsement of the neurodiversity framework and self-esteem and (2) whether this relationship differed between autistic and non-autistic adults. A diverse sample of 123 autistic adults and 104 non-autistic adults living in the United States completed an online survey.
Results:
Autistic participants reported having significantly lower self-esteem compared with non-autistic participants. We conducted linear regressions, with aspects of the neurodiversity framework as predictor variables, autism status as the moderator, self-esteem as the criterion variable, and demographic differences between autistic and non-autistic samples as control variables. There was a significant interaction between autism status and the Autism as Difference subscale of the neurodiversity framework in predicting self-esteem. In particular, endorsing this facet of the neurodiversity framework was associated with significantly higher self-esteem for autistic participants compared with autistic individuals who endorsed low levels of this facet. However, there was no difference in self-esteem for non-autistic participants who endorsed different levels of the Autism as Difference subscale.
Conclusion:
Although autistic participants indicate worse self-esteem than non-autistic participants, endorsing aspects of the neurodiversity framework may have a buffering effect on this relationship by mitigating aspects of internalized stigma. Further work must be conducted to elucidate causal relations, but the present study sets a foundation for improving mental health in autistic adults.
Community Brief
Why is this an important issue?
A lot of autistic people have low self-esteem, meaning that a lot of autistic people have negative feelings about themselves. There are many reasons for this. One possible reason is that autistic people believe the negative things that society says about autism and autistic people. People who do not agree with these negative messages about autism have different ways of thinking about autism. In contrast to the medical model, the neurodiversity framework is a different way of thinking about brain differences, such as autism. It says that people with brain differences are valuable just the way they are, and that other people should accept them.
What was the purpose of this study?
As researchers, we wanted to see whether agreeing with the neurodiversity framework was related to self-esteem in autistic adults. We also wanted to see whether the relationship between agreeing with the neurodiversity framework and self-esteem differed between autistic and non-autistic adults.
What did the researchers do?
We asked people to complete an online survey, and 227 of them gave us complete answers to the questions. We analyzed the results from these 227 people. The survey asked about self-esteem and agreement with the neurodiversity framework. We split up the neurodiversity framework into three parts: (1) disagreeing with negative attitudes toward autism, (2) thinking that autism is permanent and unchangeable, and (3) thinking that autism is just a difference and not a problem.
What were the results of the study?
We found that autistic people reported lower self-esteem than non-autistic people. We also found that, among autistic people, thinking autism is just a difference and not a problem was related to higher self-esteem. However, among non-autistic people, thinking autism is just a difference was not related to higher self-esteem.
What do these findings add to what was already known?
Our findings agree with other research that says that autistic people have lower self-esteem than non-autistic people. The research adds to what was already known by identifying how the neurodiversity framework might be helpful for autistic people’s self-esteem.
What are the potential weaknesses in the study?
This was a correlational study and not an experiment. This means that we could not see whether agreeing with certain aspects of the neurodiversity framework caused higher self-esteem.
How will these findings help autistic adults now or in the future?
These findings are a good first step for thinking about how to improve self-esteem in autistic adults in the future. Our findings may be helpful as a base for other researchers to find plans to improve mental health for autistic people.
Introduction
Self-esteem, or a person’s attitudes and sense of respect toward themselves, has repeatedly been shown to correspond with mental health and overall well-being in a variety of populations, thus making it an important target of research.1,2 Individuals on the autism spectrum are at risk for lower self-esteem compared with non-autistic individuals.3,4 At the same time, autistic individuals are at higher risk for mental health concerns, suicidality, and interpersonal victimization and trauma.5–8 Understanding and improving self-esteem in this population are vital tasks for researchers and clinicians. The neurodiversity framework, or the perspective that autism and other diagnoses reflect neutral or positive differences in brain functioning rather than pathological deficits, provides a potential pathway for higher self-esteem among autistic individuals due to its nonstigmatizing message.9–11 However, given the broad nature of the neurodiversity framework and the diverse meanings attributed to it, specific facets of this framework may be more predictive of self-esteem in autistic adults than others. 12 Therefore, in the present study, we seek to understand the relationships between self-esteem and different facets of the neurodiversity framework among autistic adults in comparison with non-autistic adults within the cultural context of the United States.
Self-esteem in autistic adults
Self-esteem has been continuously shown to be lower in autistic people in comparison with non-autistic people. 3 Research has been conducted on possible correlations between self-esteem and different aspects of autism, finding both positive and negative effects on self-esteem. For example, some autistic people who held negative views of their autism diagnosis were also found to have lower self-esteem than those who held positive views of their autism diagnosis. 13 Although identifying with the autistic community can be beneficial to collective self-esteem (i.e., positive view of one’s group), autistic people may experience challenges with building relationships with other autistic individuals due to struggling with social communication. 3 Such barriers could ultimately negatively impact their individual self-esteem. It is important to understand factors that relate to individual self-esteem, as collective and individual self-esteem may not always fully coincide. 3
Yet another possibility that might contribute to the discrepancy in self-esteem between autistic and non-autistic adults may be perceived stigma, or the sense that others view autism or autistic people in a negative and stereotypical way. Allport 14 hypothesized that individuals who experience oppression over time may internalize prejudicial attitudes, leading to self-hatred. Autistic people tend to be dehumanized or infantilized more frequently than non-autistic adults, which may contribute to the consistently lower self-esteem found in autistic adults. 15 In modern media, autistic characters are often portrayed as emotionless, robotic, or unable to experience happiness, which can spread harmful stereotypes about autistic adults and eventually could impact the way that non-autistic people interact with autistic people. 16 This portrayal of autistic people may impact the amount of perceived stigma that autistic adults experience, which is negatively correlated with self-esteem. This may potentially contribute to why autistic adults tend to have lower self-esteem in comparison with non-autistic adults. 17
Neurodiversity framework
Although not the first framework to situate autism or disability outside or against the medical model, the neurodiversity framework has become a popular alternative perspective in recent years. 18 The term “neurodiversity” was popularized by Judy Singer, Harvey Blume, and the autistic self-advocacy community in the late 1990s to describe those who had different brains, mirroring the idea of biodiversity, or biological diversity.11,19–21 While initially created in reference to autism, the term neurodiversity has grown to encapsulate other neurological differences as well. The neurodiversity framework is one that poses autism and other neurological differences as a part of the natural diversity of human brains and aims to create societal change to support people with neurological differences.22,23 It takes a strength-based approach, working to highlight the different strengths that neurodivergent people may hold and advocates for society to provide them support in different settings and environments such as at school or work. Although positioning neurodivergent conditions in a nonpathological manner, most neurodiversity advocates continue to view autism and other neurodivergent conditions as disabilities. 24 Therefore, this framing does not deny the struggles that neurodivergent individuals face, but instead contextualizes these struggles within a society that upholds barriers to full inclusion and dignity of disabled individuals.
Historically, the autistic community has conversed about the benefits and struggles of autism. 22 Initially, autism was viewed purely from a medical lens as a neurodevelopmental disorder that had a range of presentations as well as several common features. 25 Within such a medicalized lens is an implicit or explicit focus on cure or treatment by medical or psychological professionals. 26 However, with the growth of the internet, an autistic community was formed where discussions were held discussing both the difficulties and positive aspects of autism in broader contexts. 22 Through these conversations, the term neurodiversity was eventually coined as an alternative to the medical narrative surrounding autism.
The neurodiversity framework holds a few similarities to the social model of disability. The social model rejects the individualistic framing of the medical model and suggests that disability is also a product of disabling barriers and attitudes within society, making it similar to the neurodiversity framework in its rejection of a decontextualized, deficit-based perspective.20,27 The neurodiversity framework, however, explains that even if society were able to accommodate neurodivergent people, some would still experience difficulties. It is important to note that the neurodiversity movement does not reject that certain aspects of autism may be debilitating or disabling in current society, but it places the burden of most disability on lack of societal support for those who need it. 28
Although the neurodiversity framework holds a central theme of acceptance and respect for neurodivergent individuals, this framework is multifaceted. This becomes apparent when examining public perceptions of the neurodiversity framework. Past research has found that individuals may emphasize different subcomponents of the neurodiversity framework in their conceptualizations of this paradigm.12,29,30 In addition, quantitative research focused on scale development regarding the neurodiversity framework has found evidence for factor structures with multiple factors rather than unidimensional scales.31,32 For example, the Autism and Neurodiversity Attitudes Scale (ANAS) utilized in the current study consists of facets related to rejection of stigmatizing views of autism, beliefs about the permanence of autism, and views of autism as a neutral or positive difference rather than deficit. 32 Because individuals’ level of endorsement of the neurodiversity framework may vary at both the total and subcomponent level, it is important to understand endorsement of the neurodiversity framework from a multidimensional approach.
In addition, different cultures have variations of neurodiversity and disability rights movements that are specific to these social, cultural, and legal contexts.18,33,34 For example, debates about language use (i.e., person-first vs. identity-first language) depend on linguistic and cultural norms, and the academic literature has often focused on English-language contexts. 34 Without considering cultural variation, neurodiversity advocates and scholars carry the risk of incorrectly extrapolating Western norms into other linguistic and cultural contexts, thus utilizing neurodiversity frameworks in a colonial manner. 34 We focus on the American context within this study rather than combining responses from individuals across English-speaking countries due to the specific cultural, social, and legal contexts that Americans experience in relation to autism, such as health care, educational, employment, and disability policies.
The neurodiversity framework and self-esteem
The neurodiversity framework’s rejection of a deficit-based perspective may impact the self-esteem of autistic adults. While it acknowledges the challenges that autistic adults face, validating day-to-day struggles of autistic adults, it does not portray individual challenges as the entirety of autistic experiences. Instead, it emphasizes the role that societal conditions play in many of the difficulties caused by these challenges and highlights some of the unique strengths held by autistic individuals. In contrast, medical models often emphasize the “deficits” that might be present in autistic adults, which may cause internalized stigma as some people feel that there is something inherently wrong with them. This internalized stigma may contribute to lower self-esteem among autistic adults. 35
Due to the perception of autism as a disorder, there has been tremendous effort from both researchers and clinicians to find a cure to autism or to reduce behaviors associated with autism. 36 This may further the internalized stigma that some autistic adults have about their identity and contribute to creating a negative self-perception surrounding their autistic identity. The neurodiversity framework rejects the idea that autism needs to be cured. While it acknowledges that there are some autistic people who do need support, it also points out that some common symptoms of autism, such as repetitive movements and lack of eye contact, are not inherently harmful and thus do not need to be fixed. 10
In addition, efforts of normalization are rejected by proponents of the neurodiversity framework, who choose to highlight the different strengths that autistic people have and the unique ways that autistic people may be able to contribute to society.20,26 This could impact self-esteem, as the neurodiversity framework explains that while autistic people may have distinct support needs, there is nothing inherently wrong with being autistic or needing support. Furthermore, the shift to a strength-based perspective may help improve self-esteem because it helps create a positive identity about autism. 10
Current study
Given the higher risk for particular mental health difficulties and interpersonal victimization among autistic adults,5–8 it is important to investigate factors related to self-esteem, which may be lower among autistic adults but may serve as a target of intervention to buffer against further psychological distress.1,3 The neurodiversity framework provides an affirming, nonpathologizing lens for conceptualizing autism. Thus, it may serve to facilitate self-esteem in autistic adults because their autistic experiences are central to this framework. Indeed, other researchers have examined the relationship between self-esteem, psychological distress, in-group identification, and endorsement of general neurodiversity-affirming attitudes toward autism among a Polish sample of autistic adults. 9 These researchers found that self-esteem was positively related to a general neurodiversity-affirming attitude toward autism among autistic adults.
The present study serves to extend previous research by examining the role of autism status in the potential relationship between endorsement of specific facets of the neurodiversity framework (as applied to autism) and self-esteem within the American cultural context among both autistic and non-autistic adults. In particular, through survey research, we hypothesize that autistic adults will endorse lower self-esteem compared with non-autistic adults, based on previous literature. 3 We anticipate that autism status will serve as a moderator, such that the neurodiversity framework will be associated with greater self-esteem among autistic participants, but be nonsignificantly related to self-esteem in non-autistic participants. Such a difference would highlight the specific role that the neurodiversity framework may play for autistic individuals.
Methods
Sample and procedure
After researchers gained approval from the Arizona State University IRB, participants were recruited to participate in an online survey. Inclusion criteria consisted of being at least 18 years of age and currently living in the United States. Data were collected as part of a larger study on scale development in early 2020. Participants were recruited through social media (e.g., Facebook, Reddit) and through emails sent to autism-related organizations. Participants in the study were entered into a raffle to win one of 40 $25 gift cards. After completing informed consent online, participants completed demographic questions and the following measures, as well as other measures for the larger study (see VanDaalen, 2021, 37 for information on other data collected).
Several measures were taken to mitigate against fraudulent responses at various stages of the research process. First, a raffle was used for gift card compensation to incentivize participation but not guarantee payment to fraudulent responders. In addition, the online survey with the study questions was separate from the raffle. The link to the raffle entry website was provided at the end of the study question survey. Fraudulent responders were hypothesized to be more likely to only respond—or respond multiple times—to the raffle entry website rather than the study questions themselves. Indeed, there were many more raffle entries compared with responses to the study questions. The first author screened responses with respect to location and response time. Specifically, the location of responses via IP address was screened, such that participants who were responding from outside of the United States had their data excluded from analysis. Given that eligible participants must reside in the United States, participation from outside the country was unlikely to be valid responses by participants operating in good faith. Finally, Qualtrics CAPTCHA was used in the questionnaire, and complete questionnaires with implausibly short response times (e.g., less than 1 minute) were excluded.
Measures
Self-esteem
The Rosenberg Self-Esteem Scale was used to assess self-esteem. 2 It has been widely used for this purpose, including among autistic individuals. 3 Participants rated their agreement to 10 items on a 4-point Likert-type scale, with higher scores indicating greater self-esteem. Cronbach’s alpha for this study’s sample was 0.81, indicating strong reliability.
Neurodiversity framework
The ANAS was used to assess endorsement of the neurodiversity framework with respect to autism. 32 Participants rated their agreement to 17 items on a 5-point Likert-type scale regarding neurodiversity-affirming views of autism. It has a strong reliability with a Cronbach’s alpha of 0.93 in this sample. This scale consists of three subscales: Autism Anti-Stigma, Autism Permanence, and Autism as Difference. The Autism Anti-Stigma subscale has 10 items related to stigmatizing views of autism (e.g., negatively scored “I feel sorry for families of autistic people”), with higher scores indicating less negative views about autism. It has a Cronbach’s alpha of 0.93 in this sample, indicating strong reliability. The Autism Permanence subscale consists of three items related to the idea that autism is a permanent, unchangeable characteristic of a person that cannot be cured (e.g., “Autism is hard-wired into the way someone’s brain works”). It has a Cronbach’s alpha of 0.65 in this sample. Finally, the Autism as Difference subscale consists of four items that portray autism as a neutral difference rather than a pathological concern (e.g., “Autism is a form of natural human variation, not a disorder or deficit”). It has a Cronbach’s alpha of 0.67 in this sample. The Autism and Neurodiversity Attitudes Scale has demonstrated convergent validity among both autistic and non-autistic adults with respect to general antidisability prejudice and sociopolitical engagement. 32
Analytic approach
To assess whether autistic adults report having lower self-esteem than non-autistic adults, we conducted independent-samples t-tests. Before conducting t-tests, assumptions of independence of observations, approximate normal distribution for each level of the independent variable, and homogeneity of variance were assessed using histograms and Levene’s test. To assess whether autism status will moderate the hypothesized relationship between endorsement of the neurodiversity framework and self-esteem, we conducted a series of hierarchical multiple regressions with self-esteem as the outcome variable. Before conducting the regressions, we conducted bivariate correlations and produced scatter plots to assess the linear relationship between independent and dependent variables. Assumptions related to independence of observations, normal residuals of the dependent variable, and avoiding multicollinearity across main study variables were tested, indicating that the data were suitable for multiple regressions. In addition, we mean centered continuous variables before creating interaction terms to improve interpretability and minimize multicollinearity. Due to the possibility that there would be additional demographic differences between autistic and non-autistic groups, chi-square analyses were conducted to evaluate the presence of additional differences, which would be used as control variables in the linear regressions. For significant interactions, we conducted simple slopes tests to more readily interpret interaction effects. 38 These tests plot the predicted values of self-esteem for autistic versus non-autistic participants at high versus low values of the other independent variable, while calculating the slopes for these predicted values at each level of the moderator value. As per the procedures outlined by Dawson, high and low values of the independent variable signify values one standard deviation above and below the mean. 39
Researcher positionality and community involvement
Given the role that researcher positionality can play in the selection of research topic, methodology, and approach to analysis, the researchers engaged in reflective practice throughout the project and note aspects of our positionality in this article. Specifically, the first author is a cisgender, neurodivergent White woman who endorses the neurodiversity framework of autism. The other researcher identifies as an Asian American genderqueer person and has consumed content relating to the importance of identifying as neurodivergent. Both researchers have made conscious and reflective efforts to avoid biases when drawing conclusions based on the data collected and discussed how our positionalities give us a perspective into the experiences of underdiagnosed and later diagnosed populations within the autistic community, such as women and people of color. In addition, both researchers are conducting research in the context of the United States and within the psychology discipline, thus engendering certain norms and practices at a cultural and professional level, while recognizing the limitations of these norms and practices. For example, although the quantitative approaches that are often valued in psychology provide important insights, they do not fully capture the experiences of individuals who are limited by Likert-type response options. 40 There was no other community involvement in this work.
Results
Participant characteristics
After data cleaning, data were analyzed from 508 participants. Of these, 227 participants indicated that they were either autistic or non-autistic, and these individuals were included in the subsequent analyses. Excluded participants indicated that they were unsure whether they were autistic, did not answer the question, or reported an “other” response. See Supplementary Data A for further details on this question and its responses. Participants were included even if they did not provide complete responses to all study questions. Demographic questions ranged from having no missing data to having missing data from 12 (5.3%) participants. For main study variables, there was a missingness rate of 6.2% for self-esteem, 1.3% for ANAS stigma, 1.3% for ANAS permanence, and 2.2% for ANAS difference. According to the independent samples t-tests and chi-square analyses, rates of missingness for study variables did not significantly differ by demographic variables. These results, combined with Little’s missing completely at random (MCAR) test [χ2 (74180) = 45298.23, p = 1.00], indicate that data were MCAR. Therefore, we utilized listwise deletion to address missing data within each statistical test.
The sample consisted of individuals from all regions of the United States, with a mean age of 34.46 (see Table 1 for additional demographic information). Chi-square analyses were conducted to assess demographic differences between the autistic and non-autistic samples. Compared with men and women, nonbinary participants were more likely to be autistic, χ2 (3, N = 226) = 12.01, p = 0.007. In addition, transgender participants were more likely to be autistic, and cisgender participants were more likely to be non-autistic, χ2 (3, N = 227) = 19.01, p < 0.001. There were no sample differences in terms of race, although the sample was primarily White. There were differences in terms of ethnicity. Autistic participants were more likely to be Latinx, whereas non-autistic participants were more likely to not self-identify as Latinx, χ2 (2, N = 225) = 7.17, p = 0.028. Finally, there were differences in sexual orientation, such that autistic participants were more likely to be bisexual, and non-autistic participants were more likely to be heterosexual, χ2 (5, N = 224) = 17.27, p = 0.004. Sample differences regarding sexual orientation and gender identity are consistent with previous research indicating the demographics of autistic communities.41–43
Participant Demographic Information (N = 227)
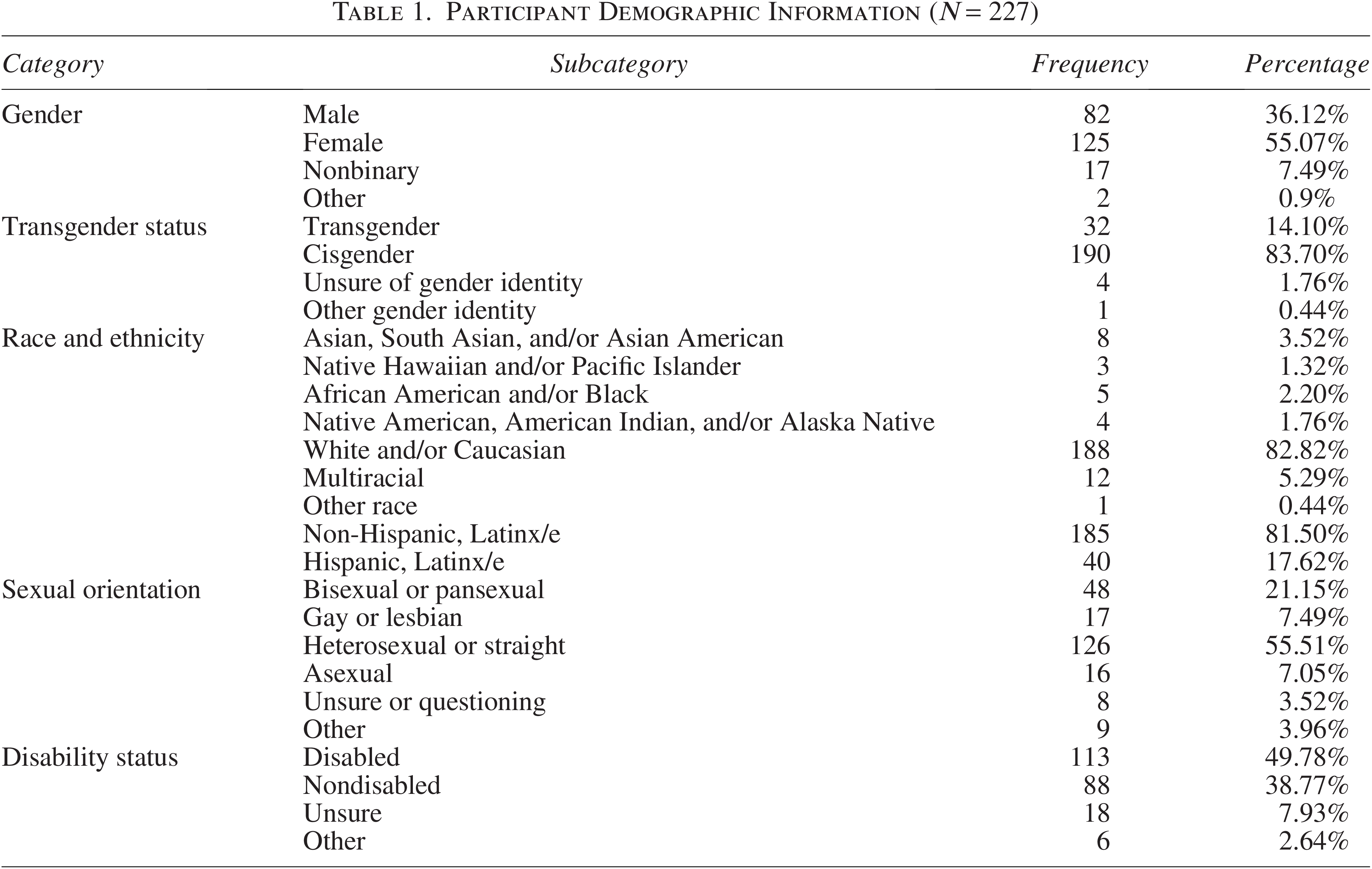
Due to disparities in access to an accurate autism diagnosis across gender, race/ethnicity, immigration status, age, and socioeconomic lines, we considered both people with professional diagnoses (n = 76) and self-identification without professional diagnosis (n = 47) as autistic.44–49 In addition, given the focus of this study on identity and potentially internalized stigma, including both self-identified and professionally diagnosed autistic participants is warranted, as there are similarities in these factors between these groups. 50 Participants with professional diagnoses reported a range of diagnosis age from between 2 and 5 years at the youngest to 63 years at the oldest, with most participants (n = 22) receiving a professional diagnosis between 26 and 35 years of age.
Mean difference, correlational and moderation analyses
As hypothesized, autistic adults reported significantly lower levels of self-esteem compared with non-autistic adults, t (211) = 4.60, p < 0.001. There was a medium effect size, with Cohen’s d of 0.63. 51 Due to demographic differences across samples, hierarchical multiple regressions were also conducted, with self-esteem as the outcome variable, to control for the potential effects of sample variability. In the first step, dummy variables of demographic differences (i.e., nonbinary, transgender, Latinx, and bisexual identities) were entered into the model, which explained 2.4% of the variance in self-esteem, F(4,208) = 1.25, p = 0.29. After controlling for demographic differences between samples, being autistic (β = −0.29, p < 0.001) was significantly negatively predictive of self-esteem, explaining 9.6% of the variance, F (5, 207) = 16.55, p < 0.001.
Bivariate correlations were conducted between self-esteem, the overall ANAS, and each of the subscales of ANAS. Self-esteem was significantly and positively correlated with the overall ANAS and each of its subscales, with small-to-moderate effect sizes. 51 See Table 2 for additional information, as well as Supplementary Table SB for information regarding correlations with control variables.
Descriptive Statistics and Bivariate Correlations
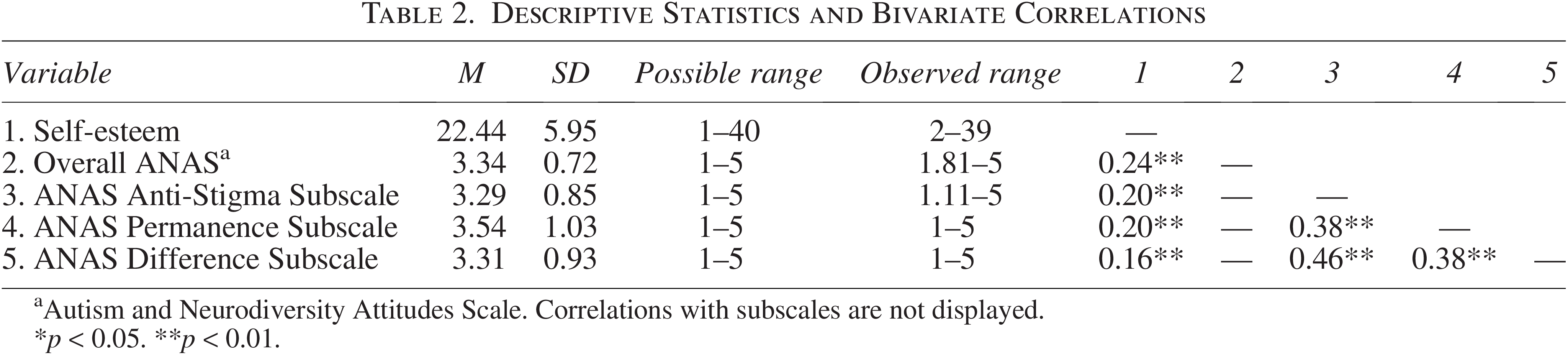
Autism and Neurodiversity Attitudes Scale. Correlations with subscales are not displayed.
*p < 0.05. **p < 0.01.
To investigate whether autism status moderated the relationship between self-esteem and endorsement of the neurodiversity framework, a series of hierarchical linear regressions were conducted. Specifically, the first block contained the demographic controls described previously, the second block contained the neurodiversity scale or subscale of interest alongside autism status, and the third block contained the product of the relevant neurodiversity scale or subscale and autism status, as well as demographic controls. Each of the subscales of the ANAS was included as a predictor in a total of three different regression analyses. In addition, to better compare our study with previous work that utilized more holistic measures of the neurodiversity framework (e.g., Ferenc et al., 2023), we conducted a fourth regression analysis utilizing the combined ANAS. Of these tests, the only one that yielded a significant interaction was the one that included the Autism as Difference subscale as a predictor, F (7, 205) = 5.38, p < 0.001. See Table 3 for further information about the different models. Our hypothesis regarding the moderating role of autism on the relationship between self-esteem and endorsement of the neurodiversity framework was partially supported.
Regression Results Predicting Self-Esteem

Autism and Neurodiversity Attitudes Scale.
*p < 0.05. **p < 0.01.
SE, standard error; CI, confidence interval; LL, lower limit; UL, upper limit; VIF, variance inflation factor. Autism status: 1 = Autistic, 0 = non-autistic.
To interpret the significant interaction between autism status and endorsement of the Autism as Difference subscale of ANAS, simple slope tests were conducted. These analyses revealed that the regression slope for the association between self-esteem and endorsement of Autism as Difference was significant and positive among autistic participants [t (205) = 3.50, p = 0.001], but was nonsignificant among non-autistic participants [t (205) = −1.56, p = 0.12], as illustrated in Figure 1. Therefore, for autistic participants—but not non-autistic participants—viewing autism as a nonpathological difference was related to greater levels of self-esteem.
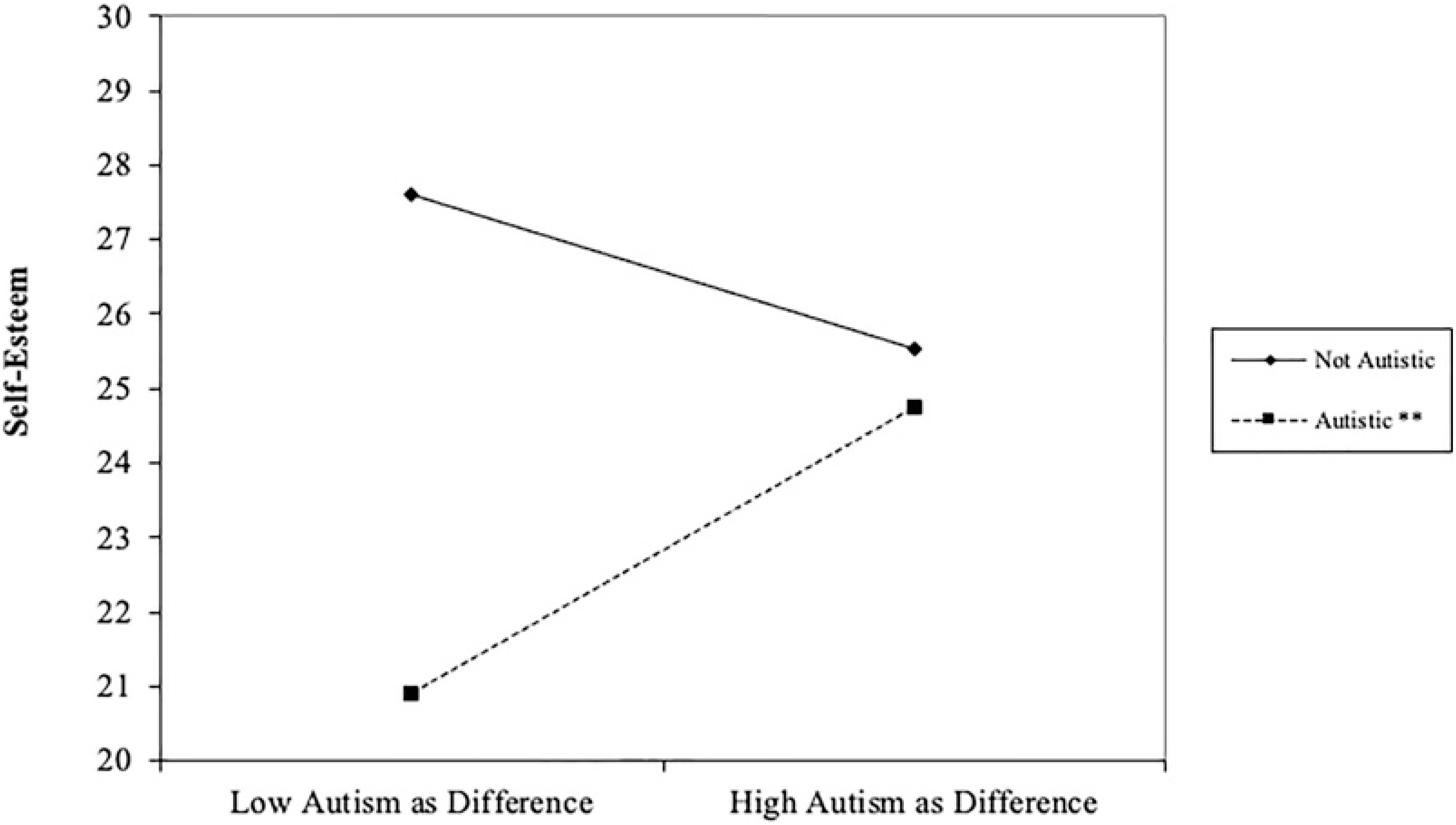
Autism Status as Moderator on Autism as Difference subscale predicting self-esteem. Autism as Difference is plotted at one standard deviation above (“high”) and below (“low”) the mean. **Slope difference at p < 0.01.
Discussion
As hypothesized, autistic adults in our sample reported significantly lower self-esteem than non-autistic participants, with a medium effect size. This is consistent with previous literature on self-esteem in autistic populations.3,4 The prevalence of this pattern, both in our own sample and in a diverse set of samples across studies, indicates that low self-esteem is a concern for autistic adults in a widespread manner and not an isolated incident. There are many possible explanations for this disparity, including societal stigma,15,35 harmful stereotypes,16,52 social isolation and victimization, 53 co-occurring mental health diagnoses such as depression, 54 and internalized negative views of autism.3,13 We examined endorsement of the neurodiversity framework as a potential correlate of self-esteem in autistic and non-autistic samples, given the theoretical connections between this framework and nonstigmatizing views of autism.
Partially supporting our hypotheses, autism status only moderated the relationship between self-esteem and one subscale of the ANAS, the Autism as Difference subscale. In other words, autistic participants who endorsed the Autism as Difference subscale had higher self-esteem than participants with lower endorsement of this subscale. This is consistent with the theoretical foundation and activist roots of the neurodiversity framework, which served to portray autism as a neutral or positive difference rather than using a deficit-oriented approach. It is also consistent with research that demonstrates that holding a neurodiversity-affirming view of autism is associated with self-esteem in an autistic Polish sample. 9 Similar to the scale used in the present study, the scale of autism attitudes developed by Ferenc and colleagues 9 focuses on beliefs about the cause of autism and the value of curing it, centrality of autism to identity, and emotional attitudes toward autism. However, the measure is combined into a total score rather than separate subscales, so it is difficult to assess which aspects of the neurodiversity framework would be most predictive of self-esteem or well-being in autistic populations.
The association between Autism as Difference and self-esteem among autistic participants is consistent with research with other marginalized populations who have fought against pathologization. For example, scholars have drawn parallels between the neurodiversity framework’s approach to autism and LGBTQ rights advocates’ approaches to pathologization of sexuality and gender in psychiatric domains.55–57 Due to the belief that being LGBTQ is not a mental disorder and thus does not need to be “cured,” LGBTQ rights advocates have recommended removing homosexuality from the DSM, argued against the use of therapies to change sexual orientation, and questioned the status of diagnoses related to gender dysphoria in the DSM. This is similar to arguments made by some individuals in the neurodiversity movement against the usage of applied behavioral analysis (ABA) for autistic individuals and against research that focuses on prevention or eradication of autism. 57 Within LGBTQ communities, internalized heterosexism and transphobia have been shown to be associated with poorer mental health and self-esteem.58,59 In addition, mental health bodies such as the American Psychological Association take strong stances against sexual orientation change efforts, or conversion therapies, due to both the lack of scientific evidence for efficacy and for the evidence of harm caused to vulnerable groups by such therapies. 60 These findings and stances against conversion therapies demonstrate evidence and a recognition of how pathologization of a nonpathological trait can harm marginalized individuals. Instead, viewing autism as a difference rather than a deficit reframes autism in a manner that circumvents pathologization. Although sexual orientation, gender, and disability identity development processes and social movements differ, their parallels indicate similarities and the potential for coalition-building across identity groups, especially given the overlap between autistic and transgender communities in terms of population. 43
It is notable that only the Autism as Difference subscale of the ANAS and not the Anti-Stigma or Autism Permanence subscales contained the significant finding. This pattern could be explained by several reasons. First, the Autism Permanence subscale contains the most neutral language of the three subscales that portray statements (e.g., “People with autism are most often born with it”) rather than value judgments, opinions, or emotions that are more present in the other subscales (e.g., “Being diagnosed with autism is a tragedy”; “There is nothing wrong with being autistic”). On the contrary, self-esteem is closely tied to subjective and evaluative self-perceptions that may be more responsive to content framed with emotional or value-laden language. Thus, it makes sense that the relatively neutral Autism Permanence did not significantly correlate with self-esteem, while the Autism as Difference subscale—containing more evaluative language—did. The Autism Permanence subscale also includes many implicit references to autism as an essential, biological trait. Although individuals may use bioessentialist arguments to advocate for neurodiversity-affirming agendas or traditional biomedical agendas in autism research and treatment, such bioessentialist arguments do not in and of themselves assume that autism is positive or negative, just that it exists at a biological level rather than a purely behavioral or emotional phenomenon. 61 This falls into parallel with research that indicates that essentialist notions of sexual orientation of sexual minorities do not predict political party affiliation or support for particular political candidates. 62 Regardless of political or sociocultural goals, anyone can hold beliefs about bioessentialism, which tend to be common with respect to both sexuality and autism status. 63
Although we hypothesized that autism status would moderate the relationship between destigmatizing messages related to autism (i.e., Anti-Stigma subscale) and self-esteem, it did not. This would have been consistent with Allport’s claims regarding the relationship between oppression and self-esteem. 14 However, other research reveals that the relationship between stigma, self-esteem, and belonging to a marginalized group is more situation-dependent and contextual. 64 One potential explanation for our findings may involve the significant overall positive correlation between the Anti-Stigma scale and self-esteem, regardless of autism status. This may reflect findings that have demonstrated how engaging in self-affirmation of one’s values and a sense of authentic pride decreases the likelihood of engaging in prejudicial evaluations of others.65,66 Although self-affirmation of values and pride differ from self-esteem, their similarities indicate that potentially a similar process may be occurring in the present study. Finally, it is also possible that this null finding was driven by our sample characteristics, such as a predominantly White sample that self-identified as disabled, with diagnoses other than autism. Further research should be conducted to investigate whether this pattern would apply among multiply marginalized autistic individuals or among autistic individuals without co-occurring conditions, for example. Accounting for intersectional experiences of autistic individuals may clarify whether there is a relationship between autism stigma and self-esteem for certain populations.
Limitations, Implications, and Conclusions
Despite the strengths and significance of this study in terms of its application of the neurodiversity framework for understanding well-being in autistic individuals using quantitative methods, there are limitations with respect to sample characteristics and study design. In terms of sample characteristics, recruitment for this study included both general venues and venues focused on disability. Thus, participants in this study were more likely to have a disability than the general population, even accounting for autism status, limiting generalizability. In addition, a significant proportion of the sample was unsure of their autism status, excluding a large number of potential participants. We used an autism-focused measure of endorsement of the neurodiversity framework. However, the neurodiversity framework is not limited to autism, and the lack of analysis utilizing a more general measure of endorsement of the neurodiversity framework limited our ability to assess how the relationship between endorsement of the neurodiversity framework and self-esteem functions in people with other disabilities. In addition, caution should be taken with interpreting data from anonymous online surveys. Although measures were taken to mitigate against fraudulent responses, it is possible that not all responses are genuine.67,68 This sample consists entirely of individuals living in the United States. Individuals living in other countries may have different cultural meanings ascribed to disability, autism, and neurodiversity,69–73 so results from this sample may not be fully applicable to those in other cultures. However, it is notable that this study has similar findings to those in a Polish population. 9 In terms of study design, limitations include the single-axis focus, the correlational design, and the limited constructs under study. The single-axis nature of this study meant that it focused on autism in isolation from other contextual factors, such as racism or sexism. However, autism and disability cannot be understood fully from this single-axis framework, 74 and future work should integrate a more explicit focus on intersectionality with a larger sample size for better understanding patterns within subgroups with adequate statistical power. This sample contained primarily non-Hispanic White participants, and future research should include improved recruitment strategies for a more racially diverse sample. In addition, this study uses a cross-sectional, correlational design that limits interpretability with respect to causal and longitudinal mechanisms. Future researchers should integrate longitudinal and experimental methods to investigate potential causal relationships between variables, paving the way for interventions to improve autistic mental health. Finally, there were limitations with respect to the constructs under study. Although individual self-esteem is an important aspect of mental health, future research should also assess other indicators of mental health, such as satisfaction with life or depressive and anxiety symptoms. In addition, it would be useful to investigate involvement with the neurodiversity movement and/or other autistic individuals, as these may uniquely relate to indicators of psychological well-being above and beyond neurodiversity-related attitudes.
While the study holds many limitations, its findings have several implications for addressing the disparity in self-esteem in autistic adults and future research directions. The findings of this study indicate the importance of shifting toward a narrative of understanding autism as a difference rather than a disease, as this framing has the potential to positively impact self-esteem within autistic adults. Shifting toward a strength-based perspective may also help reduce self-esteem disparities between autistic and non-autistic adults. Furthermore, these results should also be considered in advocacy, as it is important to increase the understanding and education of autism as a difference that is worthy of respect, acceptance, and accommodation. This can help combat stigmas that non-autistic individuals may have in both personal (e.g., peers, friends, family) and professional settings. While stigma is not always related to self-esteem, reducing stigma through reframing autism as a difference may have positive, wide-reaching effects on self-perception and self-esteem in autistic adults. Finally, although individual self-esteem is an important factor in psychological well-being, further investigation into the role of collective self-esteem in terms of the neurodiversity movement and autistic mental health should be studied, due to the collective focus of the neurodiversity movement.
The present study adds to the existing literature that posits a relationship between attitudes toward autism and self-esteem in autistic individuals, especially with respect to the neurodiversity framework, in addition to providing further evidence of a discrepancy in self-esteem between autistic and non-autistic adult populations. Notably, the Autism as Difference subscale of the ANAS, rather than the subscales related to stigma or permanence, served as the significant predictor of self-esteem that differed between autistic and non-autistic participants. This indicates that the potential benefits of the neurodiversity framework go above and beyond a purely destigmatizing message relevant to autistic populations. Instead, this subscale includes elements of the social model of disability that do not view disability as an inherently negative and objective biomedical phenomenon, but one that is situated within the context of social and cultural values. As a population that faces significant risks for mental health concerns and societal marginalization, autistic adults merit particular attention for research and interventions that promote improved quality of life and acceptance from others, and many autistic adults have advocated for these research and intervention goals.75,76 The present study serves as a foundation for future work that could achieve these goals.
Footnotes
Authorship Confirmation Statement
R.A.V. led this project in terms of conceptualizing this work, designing the study, acquiring funding, collecting data, analyzing data, writing part of the original draft, and creating tables and figures. S.Y.L. contributed to this project through writing part of the original draft and assisting in data analysis and study conceptualization. All authors contributed to the editing of the article. This article has been given solely to this journal and is not published, in press, or submitted elsewhere.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.