
Abstract
Background:
Adults increasingly self-identify as autistic without a formal diagnosis, yet little research has systematically investigated (a) the unique characteristics, experiences, and needs of self-identifying adults and (b) their preferences regarding diagnosis. Understanding the unique needs and preferences of self-identifying adults is necessary to better support them.
Method:
We conducted a cross-sectional, mixed-methods study of U.S. autistic adults who either self-identified as autistic (n = 147) or had a formal autism diagnosis (n = 115), recruited via the survey platform Prolific. Participants were compared on (a) demographic characteristics, (b) autistic traits and experiences, (c) psychosocial outcomes, (d) support needs, and (e) beliefs about autism. Moreover, self-identifying participants reported whether they wanted a diagnosis, why or why not, and what barriers they faced.
Results:
Self-identifying autistic adults were similar to diagnosed adults in autistic traits, including diagnostic traits (>93% of both groups scored ≥14 on the Ritvo Autism and Asperger Diagnostic Scale-14 Screen). However, self-identifying autistic adults differed from diagnosed adults in significant ways. Self-identifying adults were more likely to be cisgender female (53.5% vs. 27.0%), experienced worse mental well-being (ds = −0.41), were more likely to experience unmet support needs (71.4% vs. 47.0%), and faced unique barriers to receiving support (most frequently a lack of resources). The majority (68.7%) of self-identifying adults wanted a formal diagnosis but faced barriers in doing so. Self-identifying adults named a number of reasons for wanting a diagnosis (e.g., validation, access to certain services), but also grounds for hesitation (e.g., fear of stigma and discrimination).
Conclusion:
Adults who self-identify as autistic are similar to diagnosed adults in their autistic traits but face more barriers to accessing services and may be uniquely vulnerable to experiencing adverse psychosocial outcomes. Psychosocial outcomes in self-identifying autistic adults may be improved by increasing access to diagnosis and/or psychosocial services.
Community Brief
Why is this an important issue?
More and more people are self-identifying as autistic without a formal diagnosis. However, we don’t know much about who is self-identifying as autistic, what their experiences are, what needs they have, and whether they want an autism diagnosis. Getting a better understanding of self-identifying adults’ perspectives could help us better support their needs.
What was the purpose of this study?
This study compared the perspectives and needs of self-identifying and formally diagnosed autistic adults. More specifically, we wanted to understand who was self-identifying as autistic, what their experiences were as autistic people, what needs they had, their views on autism, and how those things were similar or different from autistic adults with formal diagnoses. We also wanted to understand if self-identifying autistic adults wanted an autism diagnosis and why (or why not)—and if they did, what barriers kept them from getting one.
What did the researchers do?
We surveyed U.S. autistic adults who self-identified as autistic and autistic adults who had a formal autism diagnosis. Participants were recruited on the online survey platform Prolific. We asked participants about their backgrounds, autistic traits, experiences, mental health and well-being, support needs, and beliefs about autism. We compared the experiences of self-identifying autistic adults to those of adults who had a formal diagnosis. We also asked self-identifying autistic adults if they wanted an autism diagnosis and about barriers to diagnosis.
What were the results and conclusions of the study?
Self-identifying autistic adults were very similar to formally diagnosed adults in their autistic traits. Self-identifying autistic adults more often identified as cisgender female, had worse mental well-being, and had more unmet support needs. Most self-identifying adults wanted an autism diagnosis but faced challenges doing so. The most common barrier to diagnosis and services was a lack of resources (e.g., financial).
What is new or controversial about these findings?
We already knew that self-identifying autistic adults often encountered barriers when seeking a diagnosis, but we didn’t know much about their general mental health and well-being or about the barriers they face when it comes to accessing supports. We also did not know that most self-identifying adults want a diagnosis. This is the first study to report greater unemployment, worse mental well-being, and greater unmet support needs among self-identifying autistic adults.
What are potential weaknesses in the study?
Like other online studies, our participants aren’t representative of all autistic adults. Study participants often learned about their autism diagnosis or identity later in life and were more likely to be employed than autistic adults in the general population. Also, the sample is based in the United States and may not reflect experiences in non-Western cultures.
How will these findings help autistic adults now or in the future?
Our findings are a call to action for supporting the unique needs of self-identifying autistic adults. The findings may help clinicians and policymakers better understand how to support self-identifying adults’ needs.
Keywords
Background
A growing number of adults identify as autistic despite not having a formal diagnosis, a process known as self-identification. 1 In recent years, research has begun to explore different aspects of self-identification, including characteristics of self-identifying autistic adults,2,3 barriers to diagnosis,1,4 and identity development processes.5,6 Interest in self-identification has been driven in part by concerns from self-identifying adults, who face unique barriers to diagnosis (e.g., self-identifying adults may lack the resources necessary to pursue a diagnosis, or may fear invalidation from health care professionals1,7) and support (e.g., self-identifying adults may face reduced access to services due to a lack of a formal diagnosis 8 ). As a consequence of these barriers, self-identifying adults may be at greater risk for poor psychosocial outcomes compared with adults who have a formal diagnosis. However, while some studies have compared self-identifying and diagnosed adults on certain psychosocial variables (reviewed below),3,9 no research has comprehensively examined support needs and psychosocial outcomes among self-identifying adults.
Research on self-identification has grown substantially in recent years, producing important insights regarding self-identifying autistic adults. 10 First, it is important to note that while the validity of self-identification is often met with skepticism (e.g., by medical providers, members of the public, and sometimes members of the autistic community1,7,11), multiple studies now demonstrate that self-identifying autistic adults differ little from diagnosed adults in terms of their self-reporteda autistic traits,2,13–16 including social preferences, communication ability, repetitive behavior, sensory sensitivity, monotropism (e.g., focused interests), cognitive rigidity, and social camouflage. As one recent scoping review concluded, “adults who self-identify as autistic seem to have a reasonably accurate recognition of autism/autistic traits in themselves (p. 689).” 10
However, while self-identifying autistic adults exhibit similar levels of autistic traits compared with their diagnosed counterparts, self-identifying autistic people may face unique challenges due to lack of formal diagnosis. A formal diagnosis of autism can be seen as proof that one is authentically autistic 11 ; without one, self-identifying adults may experience self-doubt, struggle to understand themselves, and face unique social stressors (e.g., invalidation from peers, family members, and medical professionals1,7,11). Because these experiences—self-doubt, invalidation, and a lack of positive autistic identity—are associated with worse psychosocial outcomes in autistic adults,7,17–19 self-identifying adults may be at greater risk of experiencing poor mental health and well-being.
Lacking a formal diagnosis can also be a barrier to accessing accommodations or supports. Due to the emphasis placed on formal diagnosis by many current systems of care, self-identifying adults face unique barriers to access for a wide array of services. 8 Without a formal diagnosis, self-identifying adults are unlikely to have had access to autism-specific support services as children, such as psychotherapy, speech and occupational therapy, and school-based accommodations and services. 20 Formal diagnosis as a child not only opens the door to receiving such services but also to mechanisms for paying for them (e.g., via Medicaid, in some parts of the United States). 20 Self-identifying people may also be disqualified from accessing certain services as adults, such as accommodations in higher education and the workplace.21–23 These disadvantages only compound existing challenges accessing physical and mental health care faced by self-identifying and diagnosed autistic adults alike, which include frequent invalidating and unhelpful encounters with health care professionals and systems.24–26 While a comprehensive review of support systems is outside of the scope of the present study, it should be noted that these systems vary meaningfully across (and within) countries, as do requirements for formal diagnosis.
Despite these unique challenges, very few studies have explored mental health and well-being outcomes in self-identifying autistic adults. One study found comparable levels of quality of life between self-identifying and diagnosed adults (but did not explore other outcomes).3,27Comprehensive research comparing these groups on multiple outcomes is still needed.
More empirical research has explored self-identifying adults’ experiences seeking (or not seeking) a formal diagnosis. Research indicates that self-identifying adults face a wide array of barriers in seeking a formal diagnosis, 28 including the fear of not being believed, mistrust of health care professionals, a lack of adult autism specialists, stigma associated with autism, and a lack of resources (e.g., money, insurance) and supports necessary to navigate complex and burdensome health care systems.1,7 Notably, not all self-identifying adults wish to have a formal diagnosis; research shows that some adults who self-identify feel that self-diagnosing is sufficient for their goals and/or challenge the usefulness of formal diagnosis altogether.6,29 Other self-identifying adults do not wish to pursue a formal diagnosis due to a lack of financial resources, limited availability of clinicians, fear of invalidation, and other concerns. 7 While these perspectives have been documented in qualitative research, the overall proportion of self-identifying adults who do (or do not) want a diagnosis has not, to our knowledge, been assessed quantitatively. In addition, further research documenting self-identifying adults’ reasons for wanting (or not wanting) a formal diagnosis is warranted.
Despite the growing literature on self-identification, there are important gaps in our understanding of who self-identifies and why. Regarding who self-identifies, critical questions remain regarding the psychosocial outcomes and support needs of self-identifying adults; while qualitative research has articulated how self-identifying adults face unique psychological and practical disadvantages (e.g., regarding the development of positive autistic identity or access to support services) that may negatively impact their mental health and well-being, little research has actually tested whether self-identifying adults experience worse psychosocial outcomes overall—or assessed the prevalence of support needs in this population. 10 In addition, while multiple studies have now indicated that self-identifying and diagnosed adults exhibit similar levels of autistic traits,2,13–16 this question may still benefit from further testing and replication.
Regarding why adults self-identify, while some qualitative research has outlined adults’ perspectives on diagnosis, little research has articulated specific reasons for wanting or not wanting a diagnosis, nor which reasons are most common. 10 Similarly, while studies have identified barriers faced by individuals seeking formal diagnoses,1,7 further research is necessary to better understand how many self-identifying adults actually want a diagnosis, as well as to contextualize common barriers alongside other elements of self-identifying adults’ experiences (e.g., psychosocial outcomes and support needs). On the whole, while existing research has begun to paint a picture of self-identifying adults and their experiences, further work is necessary to best identify and meet the unique needs of this population.
Present study
The present study seeks to add to our understanding of the unique characteristics, needs, and experiences of self-identifying autistic adults in the United States by providing both quantitative and qualitative evidence. Regarding the question of who self-identifies (RQ1), we investigated whether self-identifying autistic adults (a) are more likely to belong to certain demographic groups, (b) have different autistic traits or experiences, (c) face different support needs and/or barriers to accessing care, (d) experience different psychosocial outcomes (i.e., depression, anxiety, and mental well-being), and (e) understand autism differently, relative to formally diagnosed adults. For the latter, because autistic people tend to understand autism differently from non-autistic people 30 and researchers have speculated that people may self-identify based on an evolving concept of autism,31,32 we investigated differences in how diagnosed and self-identifying adults defined autism. Regarding the question of why self-identifying adults self-identify (RQ 2), we investigated (a) how many self-identifying adults wanted a diagnosis, (b) reasons for wanting or not wanting a diagnosis, and (c) barriers to seeking a diagnosis. In exploring these questions, we hope to provide new evidence regarding the needs and experiences of self-identifying adults that can be used to advocate for solutions to their unique challenges.
Author positionality
Author positionality is critical for autism research since studies that neglect autistic perspectives are at greater risk of causing harm to members of the autistic community. 33 The research team for the present study included autistic and allistic researchers. The research aims and design were initially drafted by the first (allistic) author and then collaboratively revised by the neurodiverse research team to ensure scientific rigor and relevance for the autistic community. This collaboration continued throughout the rest of the study, with autistic and allistic researchers involved in research design, data collection, data analysis, interpretation of results, and article drafting and revision.
Methods
All methods were preregistered at https://osf.io/vwa3u/.
Participants
Participants included 262 U.S. adults recruited via the online survey platform Prolific. Prolific users volunteer to complete online surveys in exchange for monetary compensation, and research shows that the platform provides higher-quality data (e.g., fewer invalid or low-attention responses) than other online data collection platforms. 34 Prolific users complete detailed demographic questionnaires before participating in studies, allowing us to recruit specifically from users who reported having an autism diagnosis or identifying as being on the autism spectrum. Participants were U.S. adults aged 18 years and above who identified as autistic and could read and write in English; we applied no other inclusion or exclusion criteria. Screening procedures are detailed below.
Procedure
All study procedures were approved by the Stony Brook University institutional review board (IRB2023-00245). We invited Prolific users who reported identifying as autistic to participate in a survey “to learn about the experiences of autistic people who received a formal diagnosis, as well as those who do not have a formal diagnosis.” Participants completed a one-time online questionnaire delivered via Qualtrics, designed according to best practices for survey research with autistic participants35,36; participants rated the survey as easy to understand and use.b The survey took approximately 20 minutes to complete, and participants received payment of $7.50 via the Prolific platform. The survey is available at https://osf.io/vwa3u/. All participants provided informed consent electronically by reading the research consent form and selecting “I agree to participate in this study.”
We filtered survey responses to ensure the final dataset included only non-duplicated, high-attention responses from eligible respondents (U.S. adults 18 years and above who identified as autistic). In addition to Prolific’s built-in demographic screening, we included screening items (adapted from prior research 2 ) in our questionnaire to ensure that all participants identified as autistic (“Do you identify or are you diagnosed as autistic, on the autism spectrum, or with another identity or condition on the autism spectrum, (e.g., Autism Spectrum Disorder (ASD), Autistic Disorder, Asperger’s, Pervasive Developmental Disorder-Not Otherwise Specified (PDD-NOS)?”); we removed 12 respondents because they did not identify as autistic. An additional 11 respondents either did not consent to participate or returned to Prolific without completing the survey and were removed. One duplicate response was removed. Last, as an attention check, we asked respondents to provide their age (in years) and their birth year and removed respondents whose values did not align; we excluded 13 respondents for this reason, and an additional seven were excluded because they did not respond to the birth year question.
Measures
Demographic measures
Demographic measures included age, gender, sexual orientation, race/ethnicity, educational attainment, and employment status. Age was measured in years. Categorical variables were measured using detailed multiple-choice items and operationalized for primary analyses in broader categories; for example, gender identities such as nonbinary, transgender, and genderqueer are all considered “transgender/gender expansive” in primary analyses. Supplementary Data S1 provides detailed categories for each demographic item, while simplified categories are presented in Table 1.
Demographic Characteristics by Group

Simplified for the sake of analysis; see Supplementary Data S1 for complete demographic details.
Subgroups are not mutually exclusive.
Autistic traits and experiences
Autistic traits were assessed using the Comprehensive Autistic Trait Inventory (CATI). 13 The CATI is a valid and comprehensive assessment of autistic traits across six subscales: social interactions, communication, social camouflage (i.e., masking), repetitive behaviors, cognitive rigidity, and sensory sensitivity. The CATI has been validated in both diagnosed and self-identifying populations. 13 Cronbach’s alpha for the full CATI in this sample was α = 0.91, and subscale alphas ranged from α = 0.79 (for sensory sensitivity) to α = 0.87 (for social interactions). Moreover, the Ritvo Autism and Asperger Diagnostic Scale-14 Screen (RAADS-14) 37 was used to assess the clinical characteristics of autism spectrum disorder (ASD). The RAADS-14 was developed as a diagnostic screening tool and has been used with undiagnosed, diagnosed, and self-identifying populations. 15 The reliability of the RAADS-14 in this sample was α = 0.81.
The survey also assessed certain other aspects of participants’ experience of autism, including the age they first became aware that they were autistic (in years), their childhood and current speaking ability, and whether they had family members or friends who identified as autistic and/or had a diagnosis. Speaking ability was assessed with a multiple-choice item asking participants how much of the time speech is a reliable form of communication for them.
Autistic social identity was assessed with a multidimensional measure of social identification adapted for autistic people.17,38 The social identity measure has a total score, representing the overall degree of social identification, and subscales including satisfaction (positive feelings about one’s group), solidarity (in-group bond and commitment), centrality (centrality of the identity to the individual’s self-concept), self-stereotyping (seeing oneself as similar to other members of the group), and in-group homogeneity (seeing members of the group as similar to one another). The total score had a reliability of α = 0.91, while subscales ranged in reliability from α = 0.71 (centrality) to α = 0.91 (solidarity and self-stereotyping).
Support use and need
Respondents were asked what social and health services they currently receive, what services they have received in the past, and what services they need more of, using a list of services drawn from the 2018 Pennsylvania Autism Needs Assessment. 39 Service categories included mental and behavioral health services (e.g., mental health counseling, behavioral support, drug and alcohol counseling), physical health services (e.g., specialized medical care, neurology services, benefits counseling, medication management, reproductive care), functional support services (e.g., speech/language therapy, occupational therapy, physical therapy), case management services (e.g., case management, supports coordination, medication management, one-to-one support), social development services (social skills training, sexual health education, relationship counseling), and vocational services (e.g., vocational training, transition planning, supported employment, career counseling).
Psychosocial outcomes
Psychosocial outcomes included depression symptom severity, anxiety symptom severity, mental well-being, and disability-related impairment. Depression and anxiety symptom severity were assessed using the Patient Health Questionnaire-4 (PHQ-4), 40 a brief measure of core symptoms of major depressive disorder (i.e., depressed mood and anhedonia) and generalized anxiety disorder (i.e., feeling nervous and worrying). The reliability of the depression items in this sample (i.e., the Patient Health Questionnaire-2, or PHQ-2) was α = 0.87, and the reliability of the anxiety items (i.e., the Generalized Anxiety Disorder-2, or GAD-2) was α = 0.85. Mental well-being was measured with the Warwick-Edinburgh Mental Well-Being Scale (WEMWBS), 41 a measure that has been used in the past with autistic adults.42,43 The reliability for the WEMWBS in this sample was α = 0.94. Disability-related impairment was measured using the World Health Organization Disability Assessment Schedule-II (WHODAS-II) 12-item, which has been validated in autistic adults. 44 The reliability of the WHODAS-II in this sample was α = 0.89. Last, participants were asked whether they considered themselves to be disabled and could answer “yes,” “no,” or “unsure.”
Understandings of autism
We assessed beliefs about what constitutes autism via a single open-ended item: “How would you define autism, in your own words?” This approach is consistent with prior research investigating how autistic individuals define autism. 30 These open-ended data were coded using content analysis, detailed below. Furthermore, we asked participants whether they considered autism to be a disability; participants could respond “yes,” “no,” or “unsure.”
Reasons for (not) wanting a diagnosis
All self-identifying participants were asked, “If there were no barriers to receiving a formal diagnosis from a professional, would you want one?” and could respond “yes,” “no,” or “unsure.” All self-identifying participants were then asked why they would or would not want a formal diagnosis. The wording of this question depended on the participant’s prior responses; participants who reported wanting a diagnosis were asked, “Why would you want a formal autism diagnosis?” while participants who reported not wanting a diagnosis were asked, “Are there any reasons why you would want a formal autism diagnosis?” Responses were coded using content analysis, detailed below.
Barriers to diagnosis and services
Self-identifying participants who reported wanting a formal diagnosis were asked, “What are the barriers that keep you from receiving a formal autism diagnosis?” Participants who reported having unmet support needs were asked, “You said that you need more supports than you currently receive. What are the barriers that keep you from getting the support you need?” Responses were coded using content analysis, detailed below.
Analysis
All data cleaning and analysis were conducted in R. 45 Code is available at https://osf.io/vwa3u/.
Research question 1: Who self-identifies as autistic?
To answer the first research question, we compared self-identifying participants to diagnosed participants on demographic measures, autistic traits and experiences, supports used and needed, psychosocial outcomes, and understandings of autism, as detailed above. Comparisons of dichotomous and nominal variables (e.g., support use) were conducted using chi-square tests, comparisons of ordinal variables (e.g., educational attainment) were conducted using Mann–Whitney tests, and comparisons of continuous variables were conducted using t-tests. All tests used complete cases. All p values were adjusted to ensure a false discovery rate of 0.05. 46
Research question 2: What are autistic adults’ reasons for self-identifying?
To answer the second research question, we first reported the proportion of self-identifying participants who want a formal diagnosis. We then detailed their reasons for wanting (or not wanting) a formal diagnosis, as well as barriers to seeking a formal diagnosis. This information is derived from open-ended responses via content analysis, a form of qualitative data analysis where text data (in our case, participants’ responses to open-ended questions) is coded for the presence or absence of certain themes (in our case, a certain reason for wanting a diagnosis or a certain barrier to receiving one). 47 We used an inductive approach, deriving codes from the data rather than specifying codes ahead of time; this approach allowed us to learn about participants’ perspectives without imposing preconceived categories that may not be accurate or useful.
Teams of two authors coded each open-ended item using the following steps. First, the authors read through the open-ended responses independently to identify potential themes. Teams then met to develop a draft codebook. Each author then independently applied this draft codebook with a random sample of 50 responses, coding each response for the presence or absence of each theme. Once a sample was coded by both authors, intercoder reliability was assessed with Gwet’s AC1 (a measure of reliability designed for use in contexts with high agreement, e.g., sparse codes). 48 Any codes that did not meet our preregistered reliability cutoff (AC1 ≥ 0.80) were then revised and applied to a new sample of 50 responses. This process was repeated until all codes passed this threshold, at which point the full sample was coded using the final codebook. Detailed methodological notes, including code development steps, results from reliability calculations (Supplementary Tables S2.1–S2.11), and final codebooks for each item, are provided in Supplementary Data S2.
Results
Sample description
Supplementary Data S1 provides detailed demographic information for the full sample and by group (self-identifying and diagnosed). Average participant age was 35.8 years (SD = 10.1). Cisgender men (39.2%) and women (42.0%) were approximately evenly represented in the full sample, and 18.8% of participants identified as transgender/gender expansive (the most common identity being nonbinary). A majority (53.3%) of participants identified with a sexual identity other than straight, the most common being bisexual (22.6%). Approximately two-thirds (68.3%) of the sample was White non-Hispanic. Regarding education, participants ranged from less than high school (1.5%) to professional or doctoral degrees (2.3%), with a majority having received some college degree (55.6%). Regarding employment, a majority (70.2%) reported being employed.
Research question 1: Who self-identifies as autistic?
Demographic characteristics by group
Table 1 presents demographic characteristics by group. Compared with participants with a diagnosis, participants who self-identified were more likely to be cisgender female (53.5% vs. 27.0%) and less likely to be cisgender male (26.4% vs. 55.9%; padj < 0.001). Participants in both groups were similarly likely to identify as transgender/gender expansive (20.1% vs. 17.1%). Self-identifying participants were also more likely to be unemployed (17.0% vs. 6.1%, padj = 0.034). Participants who self-identified did not significantly differ from those with a diagnosis on age, sexual identity, race/ethnicity, education level, or other levels of employment.
Autistic traits and experiences by group
Table 2 presents measures of autistic traits and experiences by group. Participants who self-identified reported slightly more challenges with social interactions per the CATI (ds = 0.35; padj = 0.017), but did not differ on other domains. On the RAADS-14, groups did not differ on their sum score or in the proportion of participants who met the clinical cutoff of ≥14 (94.5% of self-identifying participants did, while 93.9% of diagnosed participants did). Across self-identifying and diagnosed adults, sum scores for the CATI (161.7 vs. 161.5) and RAADS-14 (29.8 vs. 28.8) were highly similar.
Autistic Traits and Experiences by Group
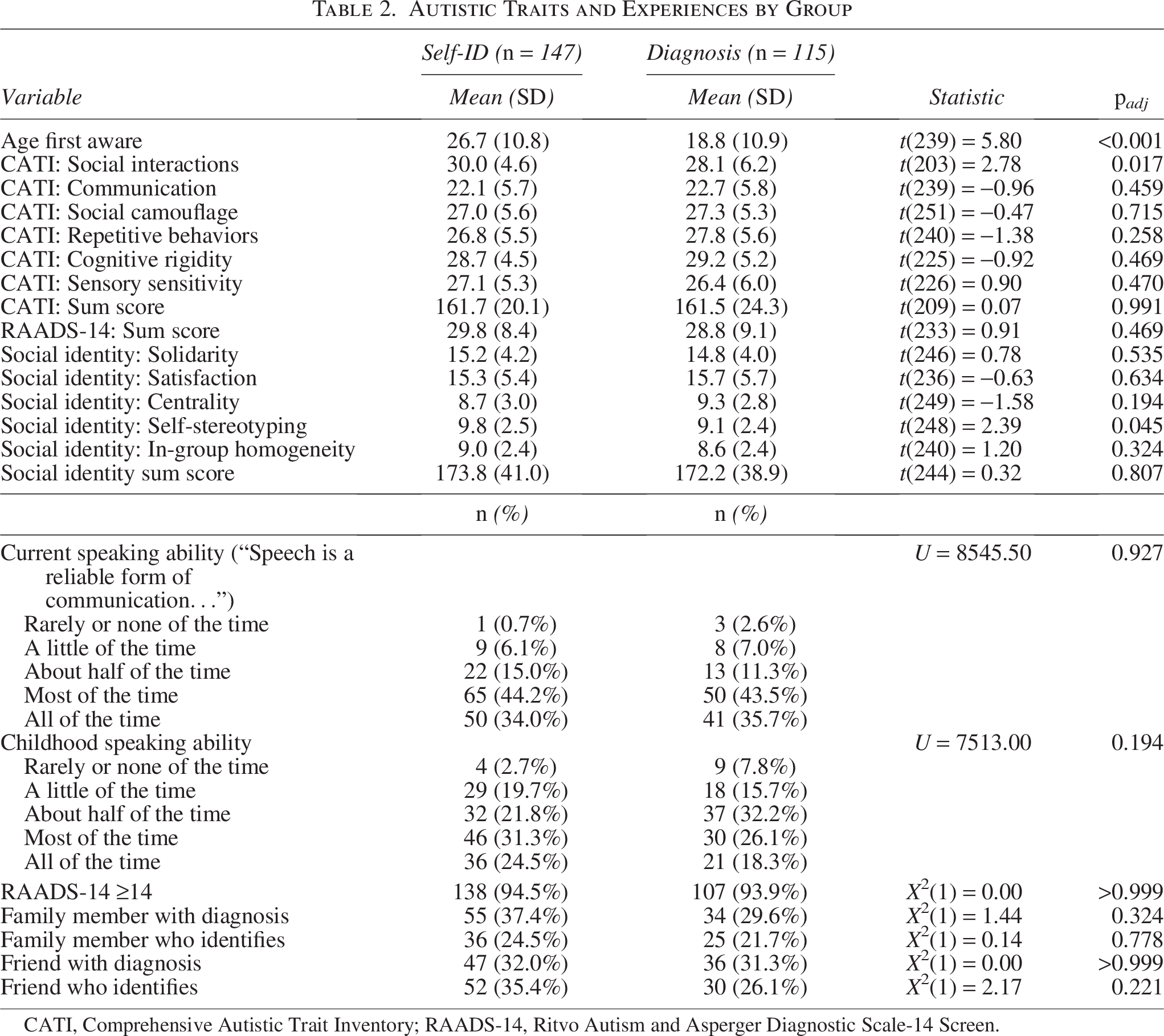
CATI, Comprehensive Autistic Trait Inventory; RAADS-14, Ritvo Autism and Asperger Diagnostic Scale-14 Screen.
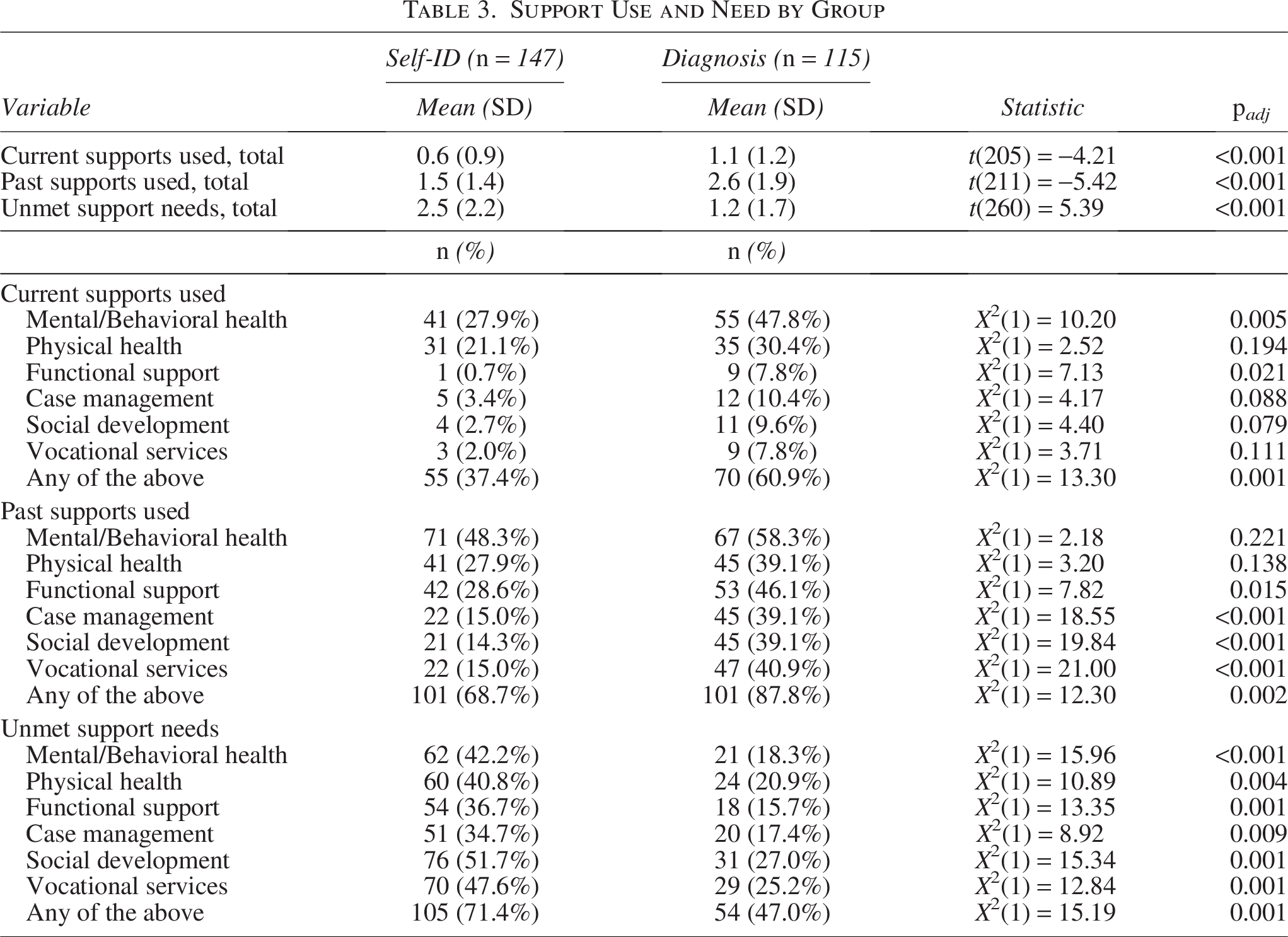
Support Use and Need by Group
On a measure of social identity, self-identifying participants reported slightly more self-stereotyping (ds = 0.28; padj = 0.045) but did not otherwise differ. Self-identifying participants reported becoming aware that they were autistic at a significantly later age than diagnosed participants (26.7 years old compared with 18.8 years old; padj < 0.001). Notably, the average age first aware was above 18 years old in both groups. Groups did not differ with respect to self-reported speaking ability (at present or during childhood) or in whether they had family members or friends who had a diagnosis and/or self-identified.
Support use and need by group
Table 3 presents detailed results regarding support use and unmet need by group, and these results are presented visually in Supplementary Figure S1. Compared with participants who had a diagnosis, self-identifying participants reported significantly less current and past support utilization and significantly more unmet need for support. Differences were substantial; across the six categories of supports measured, self-identifying participants accessed approximately half as many categories of supports at the time of the survey (0.6 categories vs. 1.1, or ds = −0.48; padj < 0.001), approximately three-fifths as many over the course of their life (1.5 categories vs. 2.6, or ds = −0.67; padj < 0.001), and experienced need in approximately twice as many categories (2.5 vs. 1.2, or ds = 0.65; padj < 0.001). Collapsing across the six categories, self-identifying participants were less likely to access any current supports (37.4% vs. 60.9%; padj = 0.001), less likely to have used supports in the past (68.7% vs. 87.8%; padj = 0.002), and more likely to experience current unmet need (71.4% vs. 47.0%; padj = 0.001).
The barriers participants faced in accessing needed supports are detailed in Supplementary Data S2 (Supplementary Table S2.15). The most frequently cited barrier to needed supports was a lack of resources (i.e., cost, time, and other practical constraints); 61.0% of participants who reported unmet need cited this as a barrier. Other commonly cited barriers included a lack of providers in the participant’s area (20.9%) and cognitive and emotional barriers such as fear, hopelessness, and a lack of motivation (18.7%). Participants in both groups cited each barrier at similar rates, with one exception: self-identifying participants were more likely to cite a lack of resources as a barrier (69.0% vs. 48.6%, padj = 0.0497; see Supplementary Table S2.16).
Psychosocial outcomes by group
Table 4 presents psychosocial outcomes by group, and Supplementary Figure S2 presents distributions of psychosocial outcomes by group and compared with population norms. Participants who self-identified reported significantly worse mental well-being compared with those who had a diagnosis (ds = −0.41, padj = 0.005). Self-identifying participants reported slightly more depression and anxiety symptoms, as well as slightly more disability-related impairment, although these differences were not statistically significant after p-value adjustment. Self-identifying participants were significantly less likely to identify as disabled, with only 53.1% identifying as such, compared with 81.4% of diagnosed participants (padj < 0.001).
Psychosocial Outcomes by Group
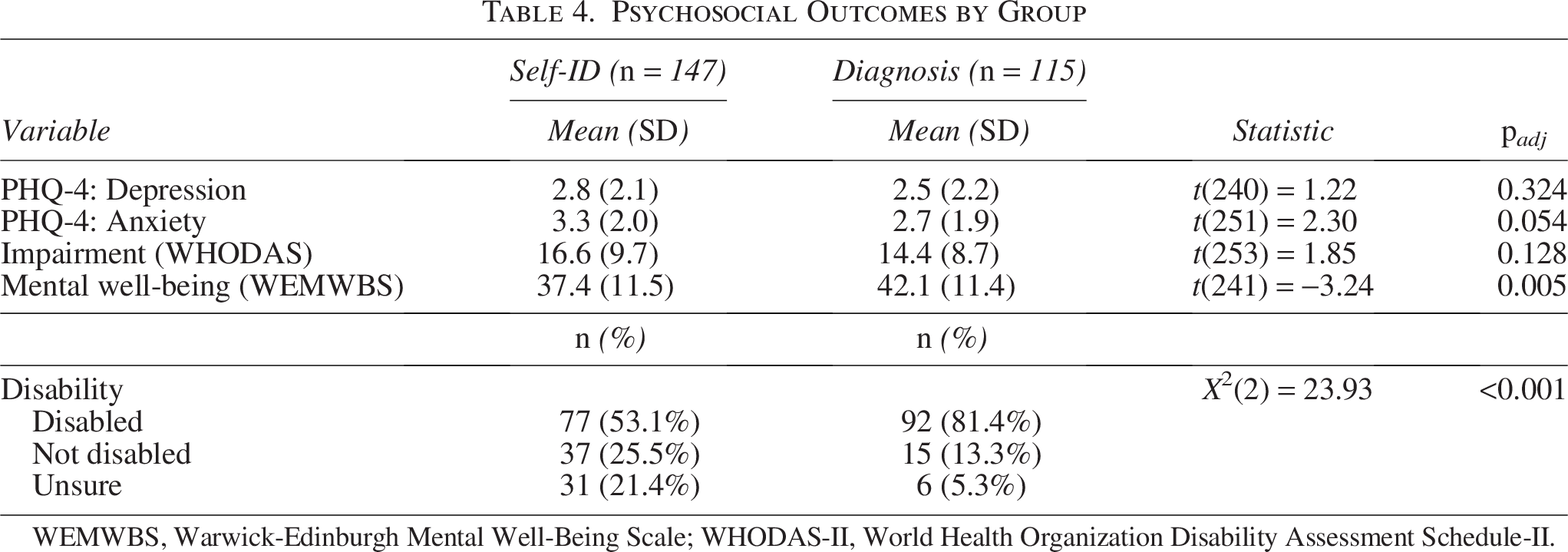
WEMWBS, Warwick-Edinburgh Mental Well-Being Scale; WHODAS-II, World Health Organization Disability Assessment Schedule-II.
Beliefs about autism by group
A complete list of codes for autism definitions is provided in Supplementary Data S2 (Supplementary Table S2.17). No significant group differences emerged in definitions across groups (Supplementary Table S2.18). Participants in both groups frequently gave responses that invoked diagnostic traits (58.6%) or referred to aspects of mental processing or brain function (58.6%). Other frequently invoked themes included comparison to the non-autistic population (e.g., “ones brain operates differently from others”; 35.2%) and the use of clinical terms (e.g., “a disorder”; 33.3%).
In addition, participants reported whether they thought autism constituted a disability. Participants who self-identified were less likely to say that autism is a disability (38.8% vs. 56.5%), less likely to say that it isn’t (14.3% vs. 19.1%), and more likely to report being unsure (46.9% vs. 24.3%, padj = 0.004).
Research question 2: What are autistic adults’ reasons for Self-Identifying?
The majority of self-identifying participants—68.7% (95% CI: 61.2%, 76.2%)—reported wanting a formal diagnosis; only 6.8% (95% CI: 2.7%, 10.9%) reported not wanting a diagnosis, and an additional 24.5% (95% CI: 17.5%, 31.4%) reported “maybe” wanting a diagnosis.
A complete codebook for participants’ reasons for wanting a diagnosis is available in Supplementary Data S2 (Supplementary Table S2.12). The most commonly cited reason for wanting a diagnosis was for confirmation/validation of autistic identity (59.2%), especially confirmation in one’s own eyes (e.g., “to make me feel more confident on what I have”; 34.7%). More than a quarter of self-identifying respondents reported wanting a diagnosis in order to help them access some kind of support or service (27.9%), most frequently accommodations (17.0%) and disability benefits (6.1%). Other commonly cited reasons for wanting a diagnosis include better understanding oneself (e.g., “so I can know why I’ve always felt different”; 17.7%) and for the benefit of others (e.g., “so others can understand me better”; 10.9%).
Reasons for not wanting a diagnosis are available in Supplementary Data S2 (Supplementary Table S2.13). Among all self-identifying participants, the most common reason for not wanting a diagnosis was fear of facing stigma, prejudice, or discrimination (e.g., “discrimination from the medical establishment,” “stigma from employers”; 42.8%); participants reported wanting to avoid stigma in a variety of domains, including medical care (8.3%), parenting (4.9%), employment (4.2%), and immigration (3.5%). Other participants noted that getting a diagnosis could be burdensome (e.g., “too much trouble”; 11.8%). A third of self-identifying participants (33.1%) said that there were no reasons why they wouldn’t want a diagnosis.
Self-identifying participants who wanted a diagnosis reported a variety of barriers that kept them from receiving one (Supplementary Data S2, Supplementary Table S2.14). The most commonly cited barriers were a lack of resources (e.g., “cost and time”; 60.0%) and challenges with the health care system, specifically challenges finding adult autism specialists (e.g., “it seems most autism professionals are for children”; 22.0%) and concerns related to inadequate insurance or knowledge regarding health care systems (e.g., “no health insurance,” “I don’t know where I need to go for one”; 34.0%). Other barriers included fear of discrimination or judgment (e.g., “they won’t take me seriously”; 8.0%), physical or mental health conditions (e.g., “depression and anxiety keep me from doing almost anything”; 7.0%), and emotional barriers (e.g., “I’m too embarrassed to ask for testing”; 5.0%).
Discussion
Understanding the experiences of self-identifying adults—as well as how these experiences align with or diverge from those of officially diagnosed adults—is a necessary step toward meeting their needs. The present study adds to a burgeoning literature on self-identification through a comprehensive set of mixed-method analyses designed to confirm prior findings and examine new questions. Our findings identify unique challenges faced by self-identifying adults—including lower mental well-being, higher unmet support needs, and a frequent lack of resources—and articulate potential pathways for addressing these challenges.
Our findings reaffirm that self-identifying adults are similar to formally diagnosed adults in terms of their self-reported autistic traits (a finding that echoes previous research2,13–15) Notably, the proportion of self-identifying and diagnosed adults in our sample who met the RAADS-14 clinical cutoff of ≥14 (94.5% and 93.9%, respectively) closely mirrored the findings of a study that administered the RAADS-R with self-identifying and diagnosed adults (93.9% of self-identifying adults and 91.6% of diagnosed adults met the RAADS-R clinical cutoff of ≥65). 15 Furthermore, self-identifying adults were far more likely to be women, a finding that is consistent with research on the underdiagnosis of autism in girls and women.49,50 Autistic women face numerous barriers to diagnosis, among them diagnostic overshadowing and misdiagnosis, 49 differences in presentation and camouflaging relative to autistic men, 51 and traits that go underrecognized by family members (who are often relied on as collateral reporters in diagnostic evaluations). 52 In the presence of these barriers, autistic women may be more likely to rely on self-identification rather than formal diagnosis. Moreover, self-identifying adults were more likely to be unemployed, a difference that could relate to broader psychosocial difficulties in this group. Research from the early 2010s reported a trend in the opposite direction (an insignificantly higher percentage of unemployed participants with a formal autism diagnosis), so our finding might reflect rising—if generally low—employment rates among formally diagnosed autistic people. 53
Self-identifying adults experienced significantly worse mental well-being compared with their diagnosed counterparts. While both groups experienced elevated depression, elevated anxiety, and worse mental well-being compared with population norms, self-identifying adults experienced particularly poor well-being outcomes. Notably, differences in emotional health were larger in this study than in a previous study, which compared diagnosed and self-diagnosed autistic adults recruited through autism organizations. 3 This inconsistency may owe to differences in measurement approach (the WEMWBS used in the present study asks about positive experiences [e.g., “feeling good about myself”], while the Adult ADHD Quality of Life Scale psychological health subscale used in the prior study asks about negative experiences [e.g., feeling anxious or overwhelmed]) or sampling (neither study’s sample was perfectly representative; this study used Prolific participants, while the previous study selected for individuals who were already connected with autism organizations, support groups, and providers).
Differences in mental well-being may relate to differences in support use and need across groups; self-identifying adults used fewer supports than their diagnosed peers (both at the time of the survey and in the past), and more than two-thirds of self-identifying adults reported needing more services than they received. Failing to access needed supports can contribute to poor psychosocial outcomes and unemployment. 54 Furthermore, the most commonly cited barrier to accessing services was a lack of resources (e.g., money, suitable insurance), a barrier disproportionately experienced by self-identifying participants. Thus, some self-identifying adults may face a “vicious cycle” where a lack of necessary supports leads to poorer psychosocial and employment outcomes, which in turn make it harder for adults to access the supports that they need. The fact that self-identifying adults also accessed fewer supports in the past may also contribute, as they do not benefit from the same continuity of care as autistic adults who access services earlier on. As access to supports is shaped by structural and policy factors (e.g., the presence of providers in an area, requiring suitable private health insurance to access a service), our findings are somewhat specific to the U.S. context; this limitation is discussed further below.
Notably, despite reporting similar levels of functional impairment, self-identifying adults were significantly less likely to identify as disabled. This could reflect internalized ableism in self-identifying adults, as they may be forced to function without recognition of, or support for, their needs. This could also indicate that a formal autistic diagnosis functions as a sort of gatekeeper for disability identity among some self-identifying adults. Last, this may also relate to self-identifying adults’ reluctance to see autism itself as a disability; self-identifying adults in this study were less likely to say that autism is a disability but were also less likely to say that it is not a disability, and relatedly more likely to report being unsure.
In terms of autistic social identity, we found similar degrees of social identity between self-identifying and diagnosed adults across most constructs; self-identifying adults felt similar levels of in-group solidarity, derived a similar amount of satisfaction from their autistic identity, saw autism as a similarly central part of their identity, and were roughly as likely to see autistic people as similar to each other, though they did engage in slightly more self-stereotyping. The broad similarities in autistic identity observed in our study are consistent with prior research. 3 These results suggest that not having a formal diagnosis does not act as a substantial barrier to the development of autistic social identity for most self-identifying adults.
Critically, we found that the majority of self-identifying adults wanted a diagnosis; very few reported not wanting a diagnosis. The most commonly cited reason for wanting a diagnosis was for validation or confirmation of the respondent’s autistic identity (either for themselves or for others), a finding that corroborates prior qualitative and mixed-methods research on the importance of validation as a reason for diagnosis-seeking.c 10 A sizable minority of respondents also reported wanting a diagnosis in order to help them access accommodations, benefits, or other services.
Why, in spite of these reasons, do these adults not have one? Participants identified a number of barriers that kept them from obtaining a diagnosis as an adult, most frequently a lack of resources (e.g., financial) and challenges related to the health care system (e.g., a lack of autism specialists in their area or not having health insurance). These findings are consistent with prior research on barriers to formal diagnosis among self-identifying adults, which has also identified a lack of resources and access to adult autism specialists as meaningful barriers.1,7 It should be noted that a lack of resources was identified as a prominent barrier to accessing needed supports as well.
While most self-identifying participants reported wanting a formal diagnosis, many participants expressed some degree of ambivalence. Many participants feared the stigma, prejudice, and discrimination they may face as a result of having a formal diagnosis. Others invoked various systems—systems of care, as well as employment, legal systems, and others—in their responses. Thus, while some participants felt that a formal diagnosis could help them navigate certain systems (e.g., helping them access supports or accommodations), some also feared that it could make navigating other systems harder or riskier (e.g., opening them up to discrimination from medical providers or employers). Despite this ambivalence, however, less than 1-in-10 self-identifying participants reported definitely not wanting a diagnosis, emphasizing that most people still prefer the diagnosis even if this positions them as more vulnerable in some ways. Overall, self-identifying participants generally wanted a formal diagnosis but saw both benefits and drawbacks. It is notable that while some benefits and drawbacks are likely unique to the U.S. context (e.g., legal implications of diagnosis), the most commonly cited reasons for and against (to validate one’s identity; facing stigma from oneself or others) are likely to generalize across a number of legal and cultural contexts.
Recommendations for supporting self-identifying adults
How can the needs of self-identifying adults best be supported? We join with others7,8 in advocating for individuals’ ability to access needed services regardless of whether or not they have a formal diagnosis. However, our results also suggest that lacking a formal diagnosis is not the most important barrier to care for self-identifying adults; less than ten percent of self-identifying participants experiencing unmet need cited this as a barrier, while more than two-thirds cited a lack of resources. Therefore, connecting self-identifying adults to needed supports cannot be achieved by addressing diagnostic barriers alone. Our findings suggest that interventions addressing self-identifying adults’ basic needs (including housing, finances, and access to affordable health care) are likely to improve their ability to access critical supports. These interventions may be targeted toward self-identifying adults specifically, or they may be offered more broadly; strong social welfare policies (e.g., financial assistance to low-income individuals, health care support for un- and underinsured adults) can be an important source of aid for self-identifying adults in need. Furthermore, interventions that can be delivered at low or no cost and outside of traditional health care settings (e.g., online single-session interventions55,56) can circumvent some of the common barriers to traditional supports (e.g., cost, location, or a lack of providers). A strong agenda for supporting self-identifying autistic adults would include (a) supporting basic needs through targeted or universal social interventions, (b) enhancing access to traditional supports by addressing common barriers, and (c) developing and disseminating new forms of support that circumvent such barriers.
Limitations
The most notable limitation in the present study is its sample, which was drawn from an online survey platform (Prolific). Prolific participants are a self-selecting group who tend to be younger, have lower incomes, and have lower levels of employment when compared with the general population (although they may still be more representative of the general population than many community-based samples). 57 Notably, our participants tended to be later-diagnosed and have higher employment levels than autistic adults as a whole. 58 Selection bias is particularly notable for self-report and online studies of autistic adults, as these procedures remain inaccessible to many autistic adults, including those with intellectual and cognitive disabilities and those with communication difficulties. 59 Furthermore, all participants lived in the United States, and findings may not generalize to autistic adults in other countries. Readers should therefore note that characteristics of our sample may not generalize across all autistic adults. In particular, our sample may underrepresent autistic adults who either (a) have intellectual, cognitive, or communication difficulties that preclude them from participating in studies like this or (b) are older, financially better off, and employed (and therefore less likely to participate in online surveys more broadly). Cross-country generalizations should be made with caution, attending to similarities and differences in cultural and policy contexts.
Further limitations are owed to study design and survey length. Because this is a cross-sectional survey, we cannot speak to the stability or progression of study variables over time. Furthermore, the use of brief measures for assessing certain variables (e.g., the PHQ-2 for depressive symptoms) may be seen as a limitation. While the PHQ-2 and GAD-2 are valid and reliable screening measures for depression and anxiety, 40 they are coarse measures of symptom severity and do not allow for more fine-grained analysis of specific symptoms.
From a clinical standpoint, it might be a limitation that we have no data on how self-identified autistic adults would fare on formal behavior-based diagnostic assessments such as the Autism Diagnostic Observation Scale-2. 60 While self-identifying participants reported similar levels of autistic traits, self-reported autistic traits correspond poorly to formal diagnosis. 12 Yet formal diagnostic interviews are themselves subject to limitationsd—and behavior-based, deficit-only assessments created by non-autistic people often underrecognize traits autistic people show before and after meeting current behavioral criteria. 51 Still, we cannot determine how many self-identifying participants in the present study would receive a formal diagnosis if given the opportunity.
Future directions
Future research should aim to identify and test effective ways of connecting self-identifying autistic adults with the supports that they need. Research may also seek to test more rigorously (e.g., through longitudinal or experimental designs) the causal effects of such supports on psychosocial outcomes in self-identifying populations. Future research may also seek to investigate why self-identifying autistic people may be less likely to view themselves as disabled (and to view autism as a disability). Last, studies may seek to replicate our findings in larger, more broadly representative samples (e.g., those not drawn from online survey platforms); a large, population-based analysis would have advantages over the current study, including the ability to examine subgroups (e.g., racial, sexual, and/or gender minority adults) and intersecting identities. Examinations of self-identification across countries (this was a U.S. sample) and cultures could also help build the field’s understanding of self-identification in different contexts.
Conclusion
Self-identifying autistic adults are similar to diagnosed adults in many ways (e.g., in self-reported autistic traits and understandings of autism) but different in others (e.g., in psychosocial outcomes). While levels of mental health and well-being are poor in both groups relative to the general adult population, levels of mental well-being may be particularly low among self-identifying adults. Moreover, self-identifying adults face unique barriers to accessing diagnoses and services, most notably a lack of resources. As efforts are made to improve psychosocial outcomes in all autistic adults, attention should be paid to the unique challenges faced by self-identifying adults, whom researchers should actively seek to include in autism research. Improving the lives of self-identifying autistic adults may require improving access to diagnosis, access to effective services, and/or improving self-identifying adults’ material conditions.
Footnotes
Author Disclosure Statement
J.L.S. serves on the Scientific Advisory Board for Walden Wise and the Clinical Advisory Board for Koko and receives book royalties from New Harbinger, Oxford University Press, and Little, Brown Book Group. She is co-founder and chief scientific advisor for Navi. No Navi products were used or are referenced in the present article. Other authors have no interests to disclose.
Funding Information
This research was supported by Psi Chi, via a Graduate Research Grant, and by the Stony Brook University Department of Psychology, via the John Neale Endowed Graduate Student Excellence Award in Clinical Psychology.
Authorship Confirmation Statement
I.L.A. contributed to study conceptualization, research design, survey development, data analysis, article writing, and revision. E.G. contributed to study conceptualization, research design, survey development, data analysis, and article revision. J.C. contributed to study conceptualization, research design, survey development, data analysis, and article revision. S.K.K. contributed to study conceptualization, research design, survey development, and article revision. A.H. contributed to study conceptualization, research design, survey development, and data analysis. J.A.G. contributed to study conceptualization, research design, and survey development. J.L.S. contributed to study conceptualization, research design, and survey development. A.N.G. contributed to study conceptualization, research design, survey development, data analysis, and article revision. The article has been submitted solely to Autism in Adulthood.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.