
Abstract
Background:
Autistic individuals exhibit greater vulnerability to mental health challenges than the general population, yet they lack access to adequate mental health care. Barriers to seeking and receiving adequate mental health care, such as minority stress, adverse life events, discrimination, and stigmatization can result in increased reliance on general and psychiatric emergency departments (ED/PsyED) during mental health crises. There is however limited research detailing PsyED use in autistic adults.
Methods:
This large-scale retrospective chart review analyzed PsyED visits by autistic adults (aged 16 to 63) in an urban psychiatric hospital in Canada from 2018 to 2020. Data were collected from 345 autistic patients who had 1027 PsyED visits during this 3-year period. Demographic information, psychiatric and neurodevelopmental diagnoses, and reasons for PsyED visits were characterized. Predictors of reasons for visiting PsyED were examined using mixed-effects logistic regressions. Differences between single-time and recurrent visitors were explored.
Results:
Autistic patients were mostly white (56.2%), Canadian citizens (79.1%), heterosexual (50.7%), and assigned male at birth (72.2%). Many were of low socioeconomic status, with one-third earning less than 15,000 Canadian dollars yearly. Most (84.3%) had at least one co-occurring mental health condition, with 54.8% having two or more. Rates of attention-deficit/hyperactivity disorder and intellectual disability were both around 20%. Most frequent reasons for visits included suicidality (42.9%), aggression (24.6%), and mood symptoms (16.1%). Reasons for visiting PsyED were associated with specific mental health and neurodevelopmental diagnoses. Recurrent visitors (40.3%) did not differ in sociodemographic characteristics from single-time visitors, but had more complex clinical presentations.
Conclusion:
Mental health needs of autistic adults were high and complex in the PsyED setting, particularly those needing recurrent emergency visits. Addressing service gaps and barriers to ongoing mental health support is essential to enhance the continuity of care.
Community Brief
Why is this an important issue?
Autistic adults are more likely to experience mental health difficulties and face challenges in accessing adequate mental health care. When mental health needs are not properly addressed, it can lead to increased use of emergency department (ED) or psychiatric emergency department (PsyED), oftentimes in crises. Understanding who are the autistic adults seeking emergency mental health care and why they visit the PsyED is crucial for improving services and outcomes.
What was the purpose of this study?
We aimed to better understand the profile of autistic adults who visited the PsyED. More specifically, we wanted to document their sociodemographic characteristics and their mental health history. We also wanted to better understand why they visited the PsyED and examine factors linked to these reasons. Finally, we wanted to explore the differences between those who visited only once and those who visited PsyED recurrently.
What did the researchers do?
We reviewed medical records of 1027 PsyED visits by 345 autistic patients, aged 16 years or older, at an urban psychiatric hospital in Canada from 2018 to 2020. From the sociodemographic information provided by autistic patients and written text-based records by PsyED clinicians, we identified patient sociodemographic characteristics, mental health and neurodevelopmental diagnoses, and reasons for visits. We also examined which sociodemographic characteristics or mental health and neurodevelopmental diagnoses were most associated with specific reasons for visits. Finally, we explored how single-time and recurrent visitors differed on sociodemographic characteristics, mental health and neurodevelopmental diagnoses, and reasons for visits.
What were the results and conclusions of the study?
Autistic adults using PsyED often faced significant psychosocial challenges, including low income and high rates of co-occurring mental health conditions. Most visits were driven by crises such as suicidal thoughts and behaviors, aggression, or severe mood symptoms. Specific co-occurring diagnoses were linked to reasons for seeking emergency care. Recurrent visitors were more likely to present with suicidality or substance-related issues, while single-time visitors were more likely to seek help for mood or anxiety symptoms, but they did not differ in sociodemographic characteristics.
What is new or controversial about these findings?
This large-scale study is one of the few to systematically characterize and examine PsyED use in autistic adults. Findings show that autistic adults visiting PsyED have complex mental health needs that require specific attention from clinicians and the health care system to ensure adequate care.
What are the potential weaknesses in the study?
The study was based on reviews of medical records, which did not include sufficient information about the social contexts that are essential to fully understand what brings an autistic adult to the PsyED. The information identified relied on the account of the clinicians and came from a specific group of autistic people using PsyED care, hence does not necessarily reflect the mental health experiences of the broader autistic population, nor does it sufficiently include the autistic person’s perspective. The findings are specific to one Canadian urban hospital, which may not reflect situations in rural areas or other countries, including those with privatized health care.
How will these findings help autistic adults now or in the future?
The findings underscore the need for more tailored and accessible mental health support for autistic adults during mental health crises. These findings can guide health care providers and policymakers in developing autism-informed mental health services that also address systemic barriers, ensuring adequate mental health service from prevention efforts to emergency care.
Introduction
Autistic individuals are more likely to experience mental health challenges than the general population, with symptoms emerging early and persisting throughout their lives. 1 Studies show approximately 79.0% of autistic adults meet the criteria for at least one lifetime psychiatric disorder, compared with 48.8% of the general population, and over 57.0% have two or more co-occurring diagnoses, with depression and anxiety being the most prevalent. 2 There is substantial heterogeneity between studies regarding the prevalence of specific co-occurring conditions. However, large-scale meta-analyses show that across ages, the overall pooled prevalence estimates of mental health diagnoses in autistic people are about 20% for anxiety disorders, 13% for sleep-wake disorders, 12% for disruptive, impulse-control, and conduct disorders, 11% for depressive disorders, 9% for obsessive-compulsive disorder (OCD), 5% for bipolar disorders, and 4% for schizophrenia spectrum disorders. 3 The pooled prevalence of concurrent diagnoses of personality disorders (PDs) is estimated at 12.6%, with clusters A (paranoid, schizoid, schizotypal) and C (avoidant, dependent, obsessive-compulsive) PDs being the most common. 4 Mental health concerns in autistic individuals may in fact be even more widespread than previously reported due to risks of under-recognition, highlighting the importance of specialized mental health services.5,6
Autistic individuals also face increased occurrence of physical health issues, many of which are chronic or pain-inducing (e.g., epilepsy, hypermobility spectrum disorders, gastrointestinal problems).7–9 These factors could contribute to elevated rates of physical as well as psychiatric care-seeking,10–12 as physical health challenges can have detrimental impacts on mental health. 1
Social determinants of health are critically relevant to the well-being of autistic individuals. In the general population, social determinants typically encompass socioeconomic status particularly educational attainment and income, 13 membership in ethnic minority groups (often due to systemic racism and its downstream effects such as reduced opportunities and segregation), 14 and LGBTQ+ community membership, which similarly faces discrimination and marginalization. These factors contribute to minority stress, which has well-documented impacts on both physical and mental health. Autistic individuals constitute a minority group and are subject to substantial minority stress, 15 compounded by a high incidence of adverse life events and traumatic experiences.16–19 Moreover, a significant proportion of autistic individuals also have other marginalized identities, notably LGBTQ+.20–23 In addition, autistic people are disproportionately affected by socioeconomic disadvantage,24,25 facing numerous barriers to employment.26,27 Even when employed, they often earn less than their neurotypical peers with comparable educational backgrounds25,28 and encounter discrimination in the workplace and broader social contexts.29,30 Taken together, these intersecting social determinants exert particularly strong influences on the well-being of autistic individuals and may contribute to their elevated mental health difficulties.
Despite heightened needs, autistic individuals encounter significant barriers to care including limited access to providers with dual expertise in autism and co-occurring psychiatric conditions.10,31–36 These mental health challenges are particularly affected by the fact that autistic people are vulnerable to recurrent adverse experiences, including abovementioned physical health and social determinants as well as challenging interactions with health care services,37–40 which can contribute to not seeking care when needed or waiting until the problem requires emergency care.34,41 The social and clinical factors contributing to the increased use of emergency services among autistic individuals10,11,42,43 remain insufficiently understood. Identifying these factors is essential for developing care that meets autistic people’s needs and effectively supports their self-determination and well-being.40,44
Studies have reported “behavioral issues” as a primary reason for emergency visits among autistic individuals. However, most research has focused on autistic youth11,42–45 and the underlying causes of these behaviors remain poorly understood. These so-called behavioral issues are often responses to broader contextual factors, such as distressing environments, challenging transitions, minority stress, and limited opportunities for self-determination,46–48 and can reflect communication breakdown or physical illnesses. 49 A recent retrospective chart review found that among those diagnosed with autism or intellectual disability (ID), the primary reasons for psychiatric emergency department (PsyED) visits were aggression toward others (36.4%), suicidal ideation (22.56%), and self-injurious behaviors (11.6%). 39 Suicidal ideation was less frequently reported as the primary reason in children (13.20%) compared with adults (29.37%), whereas aggression toward others was more common in children (53.96%) than adults (21.60%). However, it remains unclear which difficulties are specifically associated with autism versus ID, as the sample included individuals with either or both diagnoses. To our knowledge, no comparable study has investigated independent samples that would allow for a clearer distinction between these two populations. Furthermore, the available literature focuses mostly on emergency service use among autistic children and adolescents, hence a gap remains in understanding how these patterns and reasons differ in autistic adults.
Few studies have examined factors associated with recurrent emergency department (ED) visits (for psychiatric or non-psychiatric reasons) in autistic populations. Identified risk factors so far include a history of aggression, immigrant family background, family distress, previous ED visits within the past year, exposure to multiple negative life events, and residence in rural areas.12,40,42,50 In the general population, the demographics of recurrent ED visitors (RVs) differ from single-time ED visitors (SVs).51–54 However, there is currently limited research exploring these differences within autistic populations. Available evidence comparing SVs and RVs suggests that more frequent ED visits among autistic individuals are associated with female sex assigned at birth, older age, illness severity, and prior ED visits.44,55 As these samples were younger and included a substantial proportion of individuals with ID, it is unclear whether the same factors apply to autistic adults and those without ID. Given the increased rates of repeated emergency service utilization, especially for psychiatric reasons,45,55,56 understanding factors contributing to recurrent visits is crucial for informing tailored and preventive care for autistic individuals.
This large-scale, systematic chart-review study aimed to describe the characteristics and service use patterns of autistic individuals aged 16 years and above who received PsyED care at a large metropolitan psychiatric hospital, the Centre for Addiction and Mental Health (CAMH) in Toronto, Canada between 2018 and 2020. We addressed two primary research questions: 1) Who are the autistic patients presenting to the PsyED? and 2) Why are they visiting the PsyED?
To address question 1, we described the sociodemographic (i.e., age, sex assigned at birth, gender identity, sexual orientation, sociocultural background, and socioeconomic status) and clinical (i.e., neurodevelopmental diagnoses such as ID and attention-deficit/hyperactivity disorder [ADHD], and psychiatric diagnoses) profiles of all autistic PsyED visitors between 2018 and 2020. Exploratory analyses were conducted to examine differences between those with a single-visit (SVs) and those with more than one visits (recurrent visitors, RVs) on these same variables. Given the descriptive and exploratory nature of this first objective, no specific hypothesis was formulated.
To address question 2, we identified the primary reasons for presenting to the PsyED and explored whether specific sociodemographic variables or neurodevelopmental and psychiatric diagnoses were associated with these reasons. We hypothesized that specific past/current psychiatric diagnoses would predict the immediately relevant reasons for PsyED presentation. For example, individuals previously diagnosed with depressive disorders would be more likely to present for managing mood symptoms. Again, exploratory comparisons between SVs and RVs aimed to understand potential differences in crisis-related needs.
Methods
Study design and data source
Through a retrospective chart review (approved by the CAMH Research Ethics Board, REB# 008/2020) we collected data from the PsyED charts of all CAMH patients (across outpatient, ED, and inpatient settings) who have ever been formally given a clinical diagnosis of autism before, at, or after their PsyED visits. The Research Ethics Board approved this retrospective review of health records with a waiver of informed consent, as contacting large numbers of former PsyED patients would have been impracticable and the research presented minimal risk to privacy (data were analyzed in deidentified form) and patient welfare (results would not change care the individuals already would have received). The CAMH PsyED is the largest psychiatric ED in the Greater Toronto Area; it is not part of a general hospital ED and therefore might have more autism awareness and sensitivity. Ontario has a single-payer, universal health care system, where residents receive publicly funded hospital inpatient, ED, and outpatient physician services. CAMH PsyED is freely accessible to Ontario residents; non-Ontario residents can also access care via inter-province reciprocal billing agreements, private insurance, or out of pocket. We examined charts during a 3-year period, between January 1, 2018, and December 31, 2020, of autistic individuals aged 16 years and older as CAMH PsyED only accepts patients of this age range. The charts included all PsyED visits of CAMH patients (1) with a formal physician-recorded autism diagnosis (i.e., DSM-5 Autism Spectrum Disorder or equivalent prior DSM/ICD diagnoses) in CAMH’s electronic medical record (EMR) system (including ED, inpatient, and outpatient visits) at the time of data extraction (January 8, 2021); and (2) visited CAMH PsyED between January 1, 2018, and December 31, 2020. Their EMR-recorded autism diagnoses could be given prior to, at, or after the index PsyED visit; the timing when the autism diagnosis was recorded in the EMR was not available to us. In other words, the PsyED clinicians might or might not have been aware of the individual’s autism diagnosis at a specific PsyED visit.
A designated investigator (P.J.) accessed the text-based medical records through the EMR database. Charts were copied and stored as Word documents in a research-dedicated, secured drive within CAMH’s firewall. Charts were anonymized by trained research assistants (RAs) to remove identifiable names, including those of patients, families, physicians, and frequented organizations, and were organized chronologically by year. For each PsyED chart, a trained RA read the anonymized chart-texts in full to extract data using a standardized data extraction form in SPSS. Each chart was then audited twice, independently, by different RAs to ensure accuracy. Each RA-auditor reviewed the entire information extracted against the same full chart-texts to ensure it was accurate and nothing had been missed in the original extraction (audit 1) as well as the first audit (audit 2). Whenever there was a disagreement, the three RAs would discuss to reach a consensus, supported by the study coordinators (P.B. and C.C.) and the senior author (M.-C.L.). In short, by the end of the data extraction and audit process, each chart was reviewed by at least three independent RAs (except for 158 visits, where one RA completed two roles, leading to the charts being reviewed by two different persons). For autistic patients with repeated PsyED visitation through these 3 years, the relevant information from each visit was extracted separately. Unique individuals across all chart records (i.e., visits) were then identified, with their demographic data aggregated when appropriate based on the Medical Record Number linked to each chart, after the completion of chart text-data extraction.
Variables
The present study focused on sociodemographic, diagnostic, and PsyED use information. See Supplementary Table S1 for detailed definition of variables. All sociodemographic and diagnostic variables used data from the first PsyED visit of each unique autistic patient in the 3-year period. Demographic information included age at first visit and sex assigned at birth, both obtained from the EMR’s demographic data section. Gender identity, sexual orientation, main language spoken, and whether patients were born in Canada and had a Canadian citizenship status were extracted from a routine health equity self-reported questionnaire used in the PsyED. Socioeconomic variables, extracted from the same health equity questionnaire, included education level (8 categories from “no formal schooling” to “postgraduate degree or professional designation”), gross family income (asked as follows: “What is your Family Income before taxes?”), and income type (No income, Employed, Insurance, Disability Insurance, Social assistance, Pension). Diagnostic information included whether the patient had co-occurring ID or ADHD diagnoses, as well as the presence of past and/or current psychiatric diagnoses noted in their text-based charts, including depressive disorders, anxiety disorders, schizophrenia or schizoaffective disorders, other psychotic disorders, OCD, borderline personality disorder (BPD), other clinically specified PDs/traits (i.e., mixed PD, unspecified PD, cluster A, B or C traits), eating disorders, post-traumatic stress disorder (PTSD), bipolar disorders, substance use disorders (SUD), and other mental health or neurodevelopmental disorders not described above (e.g., Tourette’s disorder, learning disabilities, fetal alcohol syndrome, genetic syndromes, sensory processing disorder, language impairment, oppositional defiant disorder, insomnia/hypersomnia, somatization disorder, paraphilia). Symptoms that were noted in the History of Present Illness section were also extracted and coded (see Supplementary Table S1). Medical (physical health) diagnoses were recorded when the information was available. Medication use was coded as a binary variable (yes/no) whenever any mention of medication use appeared in the chart.
Finally, PsyED use information included the number of visits between 2018 and 2020 and the primary reason(s) for presentation on each visit, classified into 11 categories: suicidality (i.e., suicidal thoughts and/or behaviors), aggression (i.e., verbally or physically violent behaviors that led to voluntary or involuntary PsyED visits), self-harm, mood symptoms, anxiety symptoms, psychotic symptoms, substance intoxication, substance withdrawal, medication adjustment, housing concerns (i.e., coming to the PsyED because they wanted to have a bed/place to stay while they were in between resources or because they needed a bed for the night), and other reasons (i.e., any reason not covered by the previous categories, such as disorganization, agitation, seeking an assessment or mental health service, relationship problems, dangerous behaviors, emotional dysregulation, sleep disturbances, wanting help with substance use, compulsive behaviors, etc.). Each visit could have more than one primary reason if they were noted in the chart.
Analysis
Using data from the first visit of each autistic patient, we used descriptive statistics to illustrate the sociodemographic and clinical characteristics of the whole sample (n = 345) and separately for SVs (n = 206) and RVs (n = 139). As over half of the sample had only one visit during the 3-year study period, RVs were defined as individuals with two or more visits during this period. Sociodemographic categories with fewer than five patients were combined in the descriptive tables to minimize identifiability. We used a missing data pattern plot to visualize missing data on the sociodemographic variables and found no obvious pattern, suggesting data were unlikely missing by systematic ways. Chi-squared tests identified the differences between SVs and RVs regarding sociodemographic variables and Fisher’s exact tests identified differences in co-occurring diagnoses. Because information on medical diagnoses was not systematically recorded in the charts, only descriptive statistics were performed.
We used descriptive statistics to detail primary reasons for the PsyED visits. Fisher’s exact tests identified differences in these primary reasons between SVs and RVs. Tests for differences between SVs and RVs were adjusted for a false discovery rate (FDR) at 0.05 using the Benjamini–Hochberg procedure.
Then, to examine the associations between the primary reasons for PsyED visits and sociodemographic variables (here we a priori selected age, sex, family income, income type, and sexual orientation), psychiatric diagnoses, and neurodevelopmental diagnoses (ADHD and ID), we used mixed-effects logistic regressions to account for the non-independence of recurrent visits in the 3-year period. For analytic purposes, family income was dichotomized as above or below $15,000 annually, as over two-thirds of the sample who answered the question (n = 116/162) was below this cutoff. Income type was categorized into employed, pension, or insurance and assistance (including Ontario Works, a provincial social assistance program). Sexual orientation was categorized as heterosexual or non-heterosexual. An overall “schizophrenia spectrum disorders” category was used to combine those with “schizophrenia or schizoaffective disorders” and “other psychotic disorders.” A random-effects term was included to account for the correlation of visits from the same individuals. For each primary reason for PsyED visits, two separate mixed-effects logistic regression models were performed: one examined the sociodemographic factors, and the other assessed the psychiatric and neurodevelopmental diagnoses. The Benjamini–Hochberg procedure was applied across all primary reasons to control the FDR at 0.05. Missing data for any variable were retained as missing, and analyses were conducted using a complete-case approach. To supplement this approach, for the models examining sociodemographic variables we further performed multiple imputation while correcting for multiple comparisons to gauge robustness of findings in contrast with the primary complete-case analyses; this was not done for the models examining psychiatric and neurodevelopmental diagnoses as there were no missing data. All analyses were conducted using SPSS version 29, except for logistic regressions, for which we used the glmer function of the lme4 package in R (version 2024.04.2 + 764).
Results
Research question 1: PsyED visitors description
A total of 345 unique autistic patients (assigned male at birth, AMAB = 249, assigned female at birth, AFAB = 96) visited the PsyED during the study period. Autistic patients were between 16 and 63 years of age at their first visit (mean, M = 29.35, standard deviation, SD = 11.02) and 19 were below 18 years-old (5.5%), while the majority of the sample (n = 259, 75%) were between 19 and 35 years-old. Patients visited the PsyED between 1 (n = 206 SVs, 59.7% of sample) and 65 times in the 3-year period, for a total of 1027 PsyED visits. A total of 55 (15.9%) autistic patients visited twice, 29 (8.4%) visited 3 times, 12 (3.5%) visited 4 times, 10 (2.9%) visited 5 times, 6 (1.7%) visited 6 times, 6 (1.7%) visited 7 times, and 21 (6.1%) visited 8 times or more. Hence, the patients who came to the PsyED once during the study period (SVs, n = 206/1027) accounted for 20% of visits, while patients who visited 8 times or more accounted for 452 visits (44% of visits). The mean number of visits during the 3-year period was 2.99 (SD = 6.29) per patient in the total sample, but raised to 19.97 (SD = 20.50, Median = 9) in RVs. Age was not significantly different (p = 0.12) between SVs (M = 28.60, SD = 10.46) and RVs (M = 30.47, SD = 11.74).
Since our study period included the early months of the COVID-19 pandemic, we also examined these descriptive statistics stratified by visits before and after March 17, 2020 (i.e., the start of COVID-19 lockdown in Ontario). There were 810 visits before the lockdown from 297 individuals (166 SVs and 131 RVs) and 217 visits during the lockdown from 48 new individuals (40 SVs and 8 RVs). Forty-six RVs with their first visits before the COVID-19 lockdown also contributed to these 217 visits. Hence, a total of 94 individuals visited 217 times after the lockdown. The sociodemographic and co-occurring diagnoses compositions of the before- and after-lockdown samples were highly similar. Slight differences were observed in primary reasons of presentation, with only one remaining significant after multiple-comparison correction: substance intoxication was more frequent after lockdown (17.5%) than before (8.4%, adj-p = 0.001).
Research question 1: Sociodemographic characteristics (Table 1)
The majority of the autistic patients were AMAB (n = 249, 72.2%), and of those who reported the information, 69% were cis-gender men (n = 201, 58.3% of full sample), 67% identified as white (n = 194, 56.2% of full sample), and 79.5% reported being heterosexual (n = 175, 50.7% of full sample). They mostly reported being born in Canada (n = 225, 79.8% of those who answered, 65.2% of full sample), were Canadian citizens (n = 273, 95.5% of those who answered, 79.1% of full sample), and spoke English as their main language (n = 324, 95.3% of those who answered, 93.9% of full sample). In total, 54 autistic patients (15.7%) did not complete high school and 45 (13.0%) had a university/college degree, while education level was not mentioned for 33.6% (n = 116) of the full sample. Gross family income was generally low, with 33.6% (n = 116) of the full sample reporting earning less than 15,000 Canadian dollars per year; however, this variable was not reported in 53.0% (n = 183) of patients and it is possible that patients living in group homes or other types of housing reported individual income. Income type was predominantly from social assistance, insurance or pension (n = 131, 38.0%), with comparatively few earning money through employment (n = 41, 11.9%). Proportion of missing data for certain variables was substantial.
Sociodemographic variables did not differ significantly between SVs and RVs. Canadian citizenship was more prevalent in RVs (p = 0.03); however, this finding was likely influenced by the high rate of missing citizenship data for SVs.
Research question 1: Clinical characteristics (Table 2)
At their first PsyED visits, autistic patients (n = 345) had between zero and six psychiatric diagnoses other than autism, ADHD and ID (M = 1.88, SD = 1.40); 10.7% (n = 37) only had a diagnosis of autism, 29.6% (n = 102) had one additional psychiatric diagnosis (excluding ID and ADHD), and 54.8% (n = 189) had two or more. As to co-occurring neurodevelopmental diagnoses, 19.7% (n = 68) of the sample had a diagnosis of ID and 20.3% (n = 70) had a diagnosis of ADHD, and 2.3% (n = 8) had both. The most frequent psychiatric diagnoses noted in the PsyED charts were depressive disorders (32.8%), anxiety disorders (31.3%), schizophrenia or schizoaffective disorders (16.8%), SUD (15.7%), and OCD (13.9%). Psychiatric diagnoses not specified in Table 2 were combined into an ‘other mental health diagnosis’ category (30.4%). The substances used were noted in 42 out of the 54 autistic individuals with SUD; the most frequent ones were alcohol and cannabis, but in many cases more than one substance was identified.
Sociodemographic Characteristics of Unique Autistic Patients for Total Sample and by Visitor Type
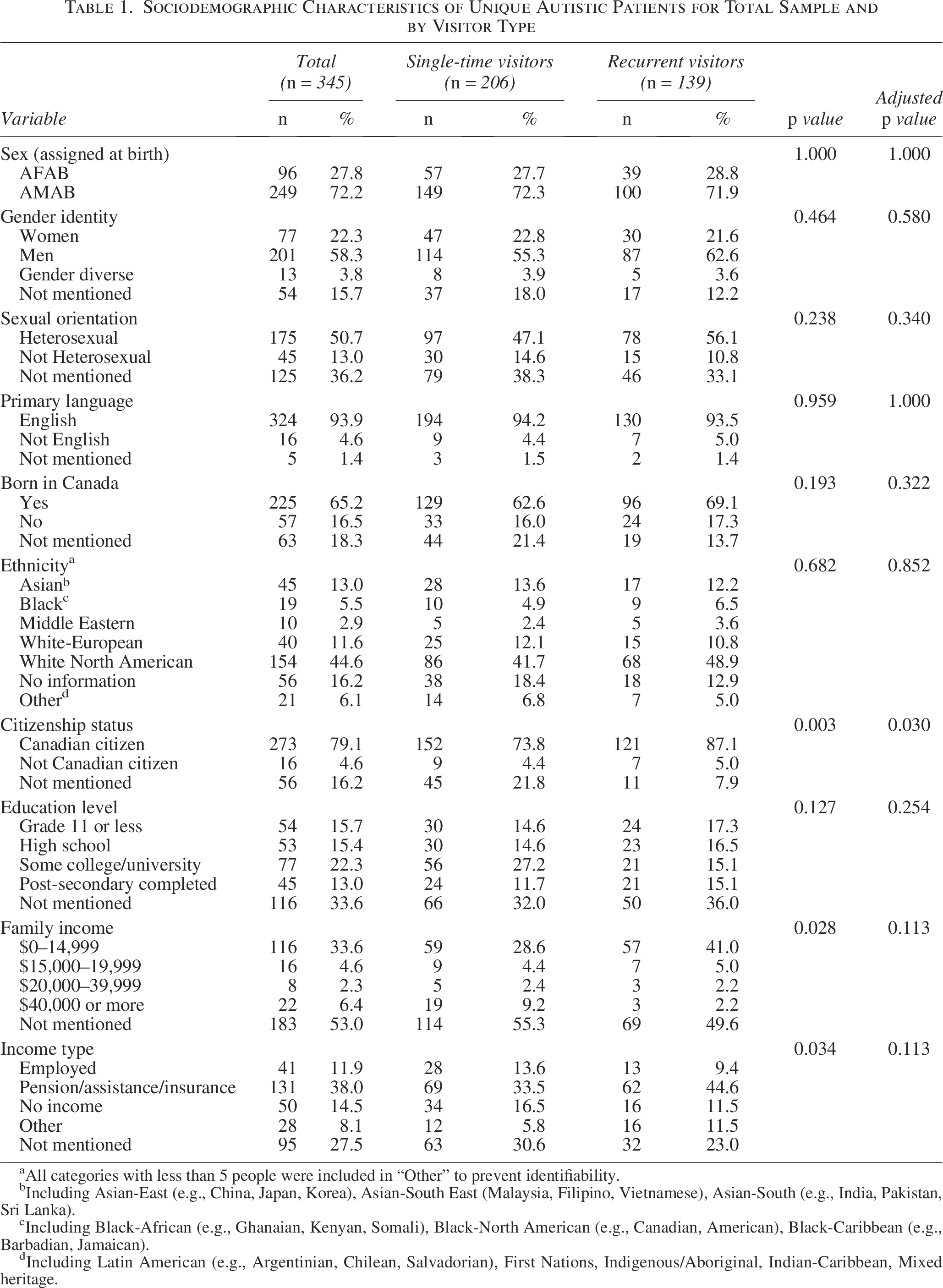
All categories with less than 5 people were included in “Other” to prevent identifiability.
Including Asian-East (e.g., China, Japan, Korea), Asian-South East (Malaysia, Filipino, Vietnamese), Asian-South (e.g., India, Pakistan, Sri Lanka).
Including Black-African (e.g., Ghanaian, Kenyan, Somali), Black-North American (e.g., Canadian, American), Black-Caribbean (e.g., Barbadian, Jamaican).
Including Latin American (e.g., Argentinian, Chilean, Salvadorian), First Nations, Indigenous/Aboriginal, Indian-Caribbean, Mixed heritage.
Co-occurring Neurodevelopmental and Psychiatric Diagnoses from Most to Least Frequent, for Total Sample and by Visitor Type, by Unique Autistic Individuals
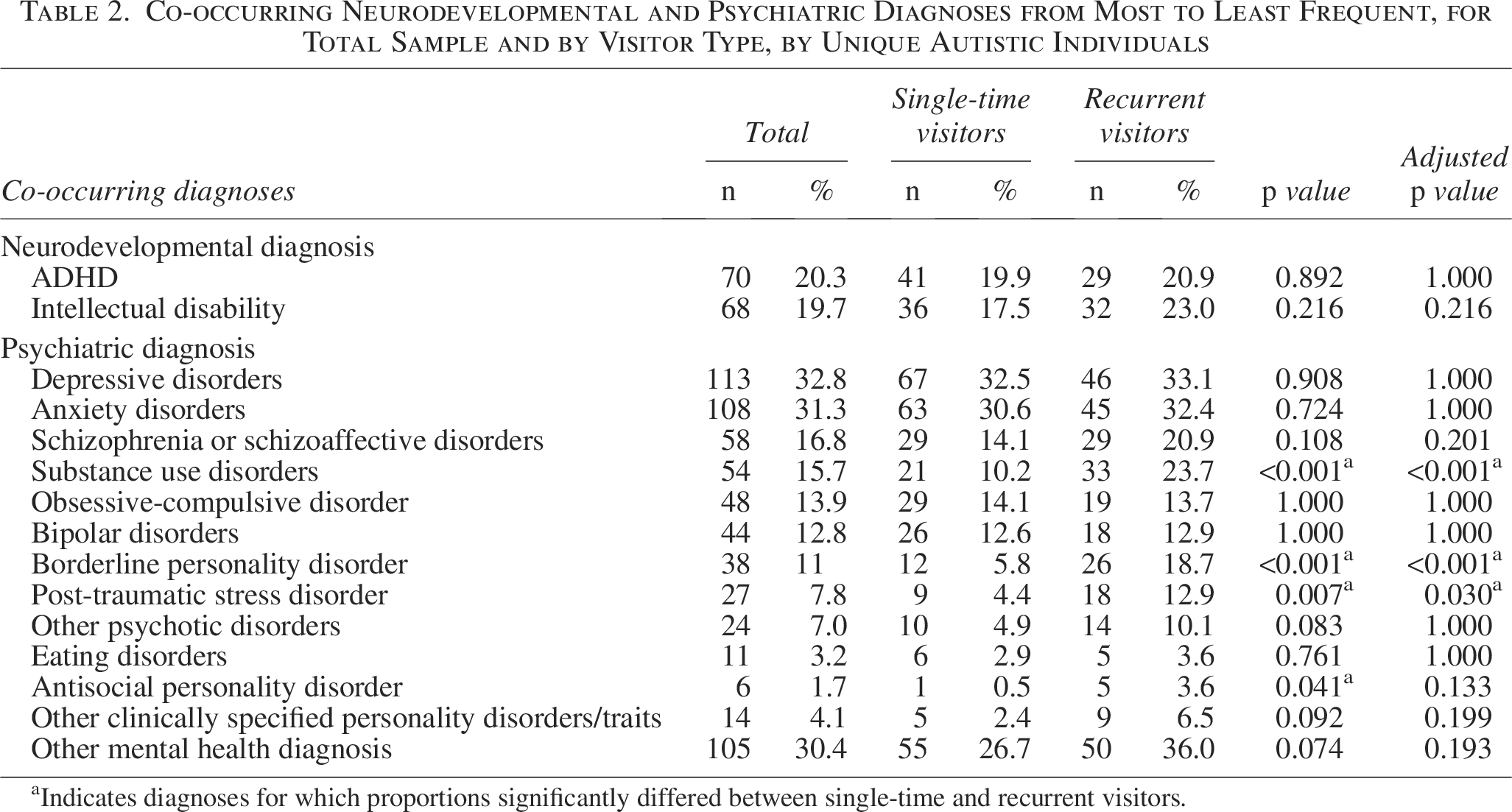
Indicates diagnoses for which proportions significantly differed between single-time and recurrent visitors.
Furthermore, 88 individuals (25.5% of sample) had other medical diagnoses noted in their chart (a total of 131 different diagnoses). The most frequent ones were seizure disorders or epilepsy (n = 11) and gastrointestinal conditions (n = 10, including Crohn’s disease, colitis, irritable bowel syndrome), followed by asthma (n = 8), fibromyalgia (n = 8), diabetes (n = 8), genetic syndromes (n = 7, including Down, Prader-Willi, Fragile X, Apert, Williams, and Stickler syndromes), hypertension (n = 7), cardiac conditions (n = 6), and other conditions with less than 5 people with the diagnoses (e.g., osteoporosis, arthritis, osteoarthritis, fetal alcohol syndrome, Elhers-Danlos syndrome, hyperlipidemia, migraine, infections, blood diseases, cerebral palsy, obstructive sleep apnea, hyperthyroidism, hernia, traumatic brain injury, etc.).
Medication use information was available for 176 patients, representing 51.0% of the sample. Among these, 81.25% were taking medication, with no significant difference (p = 0.61) between SVs (80.20%) and RVs (82.67%). RVs had a higher number of psychiatric diagnoses (M = 1.69, SD = 1.34) than SVs (M = 1.23, SD = 1.13, p = 0.002) and were significantly more likely to have the diagnoses of SUD (p < 0.001), BPD (p < 0.001), and PTSD (p = 0.03) in their clinical profiles. No significant differences were found between SVs and RVs in other diagnostic categories, including ID and ADHD.
Research question 2: Primary reasons for presenting to PsyED (Table 3 and Fig. 1)
We examined the primary reasons for PsyED visits (n = 1027). The most common reasons for presentation were suicidality (n = 441, 42.9%), aggression (n = 253, 24.6%), mood symptoms (n = 165, 16.1%), psychotic symptoms (n = 144, 14.0%), and substance intoxication (n = 106, 10.3%). Reasons not captured in Table 3 were coded as “other reasons” (n = 207, 20.2%). Many of the visits for which the “other reasons” category was coded were visits for which more than one primary reason was endorsed. For example, some patients presented with suicidality and also with disorganization or relationship problems. Figure 1 shows an UpSet plot illustrating the intersections of the 11 primary reasons categories. When we examined only the first visit for each autistic individual (n = 345) the most common reasons remained the same, with comparable intersection patterns.
Primary Reason for Presentation from Most to Least Frequent, for Total Sample and by Visitor Type, by Visits

Indicates reasons for presentation for which proportions differ between single-time and recurrent visitors.
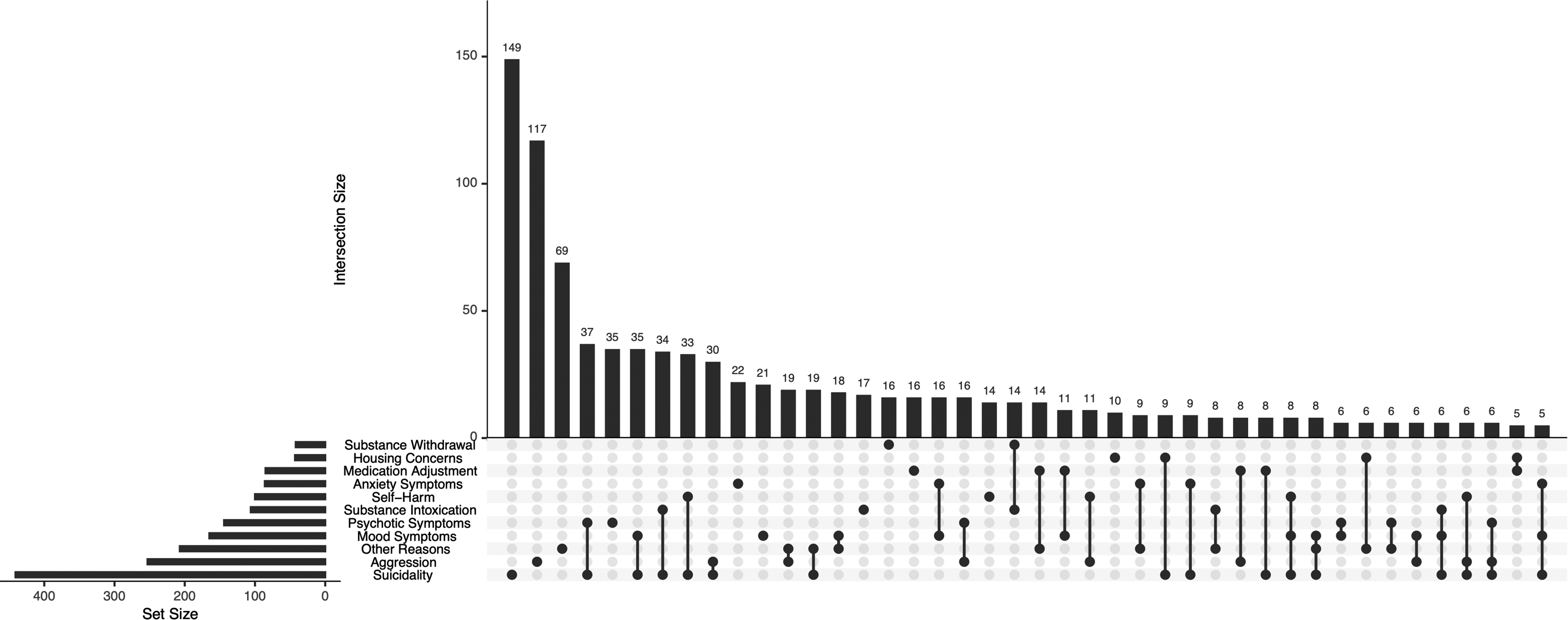
Co-occurrence patterns of primary reasons for psychiatric emergency department visits. Each bar above represents the size of an intersection between one or more presenting reasons. Bars with only one dot below represent the frequency of that reason presenting alone, while bars with connected dots below indicate the frequency of these categories overlapping. Bars on the left show the total frequency of each reason category. Intersections with less than five occurrences were not shown to minimize re-identification risk.
Summary of Odd Ratios of Significant Diagnosis Correlates for Each Primary Reason for PsyED Presentation

Schizophrenia spectrum disorders include schizophrenia, schizoaffective disorders, and other psychotic disorders.
ID, intellectual disability; BPD, borderline personality disorder; Other PD/T, other clinically specified personality disorders/traits; SUD, substance use disorders.
Research question 2: Correlates of primary reasons presenting to PsyED (Table 4)
After correcting for multiple comparisons, the mixed-effects logistic regressions indicated no significant effects of sociodemographic factors (age, sex, family income, income type, sexual orientation) on primary reasons presenting to the PsyED. This pattern remained the same when the models were re-run after multiple imputation for missing sociodemographic data.
As hypothesized, certain psychiatric diagnoses noted in the chart were significantly associated with an increased likelihood of presenting at the PsyED with directly associated symptoms. Autistic patients with depressive disorders had higher odds of presenting with mood symptoms (odds ratio, OR: 2.572, 95% confidence interval, CI: [1.595, 4.142], p = 0.001), SUD was strongly associated with substance withdrawal as the primary presenting reason (OR: 19.437, 95% CI: [8.500, 50.565], p < 0.001), and schizophrenia spectrum disorders were strongly associated with presenting with psychotic symptoms (OR: 4.793, 95% CI: [2.702, 8.501], p < 0.001).
Beyond these anticipated associations, the data also offered novel insights. Suicidality was most associated with a diagnosis of BPD (OR: 4.243, 95% CI: [2.517, 7.151], p < 0.001), while a diagnosis of ID was associated with lower odds of presenting with suicidality (OR: 0.514, 95% CI: [0.316, 0.837], p = 0.048). Aggression was associated with other clinically specified PDs/traits (OR: 2.473, 95% CI: [1.270, 4.735], p = 0.015) or ID (OR: 3.441, 95% CI: [2.421, 4.922], p < 0.001), while the diagnoses of depressive disorders (OR: 0.365, 95% CI: [0.219, 0.590], p < 0.001), anxiety disorders (OR: 0.444, 95% CI: [0.252, 0.756], p = 0.012), BPD (OR: 0.221, 95% CI: [0.143, 0.336], p < 0.001), and SUD (OR: 0.534, 95% CI: [0.342, 0.816], p = 0.012) were associated with lower odds of presenting with aggression. Depressive disorders were associated with significantly lower odds of presenting with psychotic symptoms (OR: 0.318, 95% CI: [0.145, 0.698], p = 0.028). No diagnoses were significantly associated with primary presenting reasons of anxiety symptoms, substance intoxication, self-harm, medication adjustment, housing concerns, or other reasons.
SVs were more likely to present for anxiety (p = 0.037) or mood symptoms (p = 0.022) whereas RVs were more likely to present for suicidality (p < 0.001), substance intoxication (p = 0.004), and substance withdrawal (p < 0.001).
Discussion
This large-scale, 3-year retrospective chart review study provides much-needed characterization and novel insights into the PsyED use of autistic individuals over the age of 16 years in Toronto, Canada. A total of 345 autistic patients visited the PsyED 1027 times during 2018 to 2020, most of whom who reported sociodemographic information were white (67%), had a Canadian citizenship (95.5%), AMAB (72.2%), cis-gender men (69%), and heterosexual (79.5%). Over two-thirds of the autistic patients who provided family income information reported less than $15,000 annually. The majority (73.3%) of the 345 patients had at least one co-occurring psychiatric diagnosis, and around 20% had an ID or an ADHD diagnosis, respectively. Demographic variables did not differ between SVs and RVs. Suicidality and aggression were the most and second common reasons for PsyED presentation. BPD significantly predicted presenting for suicidality while other PDs/traits and ID significantly predicted presenting for aggression. RVs (40.3%) differed from SVs in mental health diagnoses and primary reasons for PsyED presentation.
Sociodemographic characteristics of autistic PsyED patients
The socioeconomic status of autistic patients in this study was notably low compared with the general population in Ontario. Even though family income information was missing for more than half of our sample, among those who provided this info, there were over two-thirds of the autistic patients with family income of less than $15,000 annually, while the median total family income in Ontario was approximately $89,000 in 2018 57 and the median individual income was $42,900 for that same year. 58 The Market Basket Measure set the poverty line threshold for Toronto between $48,000 and $49,000 for that same period. 59 Furthermore, the source of income showed an overwhelming reliance on social assistance programs like pensions and government-based disability support, with only 11.9% earning money through employment, despite education levels being well distributed (53% of those who answered with some college, university or post-secondary education completed), thus highlighting employment barriers and difficulties faced by autistic individuals.26,27,60 Studies on social determinants of health and inequities have shown that lower socioeconomic status significantly increases the risks of mental health disorders and of using mental health services61,62 and that individuals presenting to the ED for mental health reasons tend to have lower socioeconomic status than those seeking ED care for other reasons.63,64 It is however unclear whether the present sample had a lower socioeconomic status compared with non-autistic PsyED visitors. It has been reported that income of autistic adults was significantly lower than that of the general population60,65 and in 2017, 24.1% of autistic individuals in Canada were considered “low-income.” 60 With low-income and unemployment being significant social determinants of emergency mental health care use, 66 autistic adults with mental health needs are at increased risks of getting caught in a cycle of inconsistent, inaccessible, and inadequate care and needing (or being forced) to rely on emergency services for mental health support. 36
Findings from the current study show that sociodemographic variables did not differ between recurrent and single-time visitors, which was unexpected. Previous studies investigating the link between recurrent ED use and sociodemographic variables in the general population consistently show associations with homelessness, unemployment, financial instability, residing in areas with high social or material deprivation, but not with age, gender or race.66,67 In autistic people, the only sociodemographic factors previously identified to be associated with recurrent ED use were AFAB and older, but this was investigated only in younger samples.45,60 It is possible that a floor effect (i.e., the autistic PsyED patients in this study have already experienced substantial negative social determinants), combined with missing data, led to insufficient statistical power to detect such differences or that by adulthood these factors are no longer significant predictors of recurrent visits in the autistic population.
Clinical profile of autistic patients and their reasons for visiting PsyED
The clinical profiles of the autistic PsyED patients mirrored the previous literature on the mental health profiles in autistic adults, with heightened neurodevelopmental and mental health diagnoses4,68 including depression, anxiety, and psychotic disorders.3,11 As expected, specific diagnoses aligned with certain primary reasons presenting to PsyED: depressive disorders associated with presentation for increased suicidality and mood disturbances,69,70 ID associated with presenting for aggression,11,12 and schizophrenia spectrum disorders associated with presenting with psychotic symptoms.45,71
Suicidality was the most common reason for PsyED presentation and the strongest correlate of recurrent visits. All diagnoses associated with recurrent PsyED use—SUD, BPD, and PTSD—have been linked to increased suicidality in autistic people.17,72–74 These results are consistent with what is reported in the general population, where recurrent ED use is associated with PDs, substance use and self-harm.66,67,75 The heightened prevalence of suicidality, including suicidal attempts and mortality, among autistic individuals is a significant concern, 76 particularly considering the high rates of exacerbating factors such as minority stress, interpersonal difficulties, loneliness, trauma exposure, lack of self-determination, and elevated psychiatric disorders.1,15,48,77–79 These factors may constitute important prevention and intervention opportunities such as the prioritization of initiatives to integrate trauma-informed interventions designed by and for autistic individuals to reduce suicidal ideation. 80 Previous research has also made recommendations to support autistic adults presenting to the ED with suicidality, including sharing resources that were developed by and for autistic people to support the navigation of the mental health care system. 77
Aggression presentation did not differ between visitor type or sociodemographic factors, yet was associated with certain clinical profiles—positive associations with ID or other PD/Ts and negative associations with depressive disorders, anxiety disorders, BPD and SUD. While the links between aggression and ID, 81 SUD, 82 or PDs 83 are well documented, our findings of the negative association with BPD differ from established connections in the general and autistic populations.84–86 A deeper look into the autistic population with a coexisting BPD label is a logical next step that would help uncover specific contributing clinical profiles, including possible misdiagnosis of both conditions. While substance use was a major factor for PsyED attendance in our cohort with 15.7% of autistic patients with a documented SUD diagnosis, the negative association between SUD and presenting to PsyED with aggression points to key opportunities to understand autism-unique substance use reasons, patterns, and SUD profiles, which may differ between autistic and non-autistic individuals. 87
Recurrent visitors
The proportion of RVs in this cohort (40.3%) may appear higher than that reported in other ED studies focusing on patients with mental health diagnoses (but not specifically within a PsyED).67,75,88 This discrepancy likely stems in part from differences in how RVs are defined. Due to data characteristics, we operationalized RVs as individuals with two or more PsyED visits over a 3-year period. By contrast, previous studies have used more stringent criteria. For instance, using a threshold of three or more visits within a single year, Gentil et al. 67 reported 27% RVs in a Quebec general population-based cohort of patients with mental health disorders who visited six general EDs in Quebec, while Richard-Lepouriel et al. 88 found 22% of recurrent PsyED visitors in a Swiss sample. In fact, close to what was reported in these cohorts, 24.3% of autistic patients in our cohort had three or more visits over the 3-year period.
Limitations and future directions
Important limitations should be considered when contextualizing the findings. Firstly, although the quantity and level of detail in the reviewed charts were significant methodological strengths, the information available was still sparse. We lack sufficient contextual information regarding what led autistic individuals to visit the PsyED. For example, while chart-records noted that patients came voluntarily, as opposed to cases where they were brought in by the police, it remains unclear whether this care-seeking decision reflected true agency or was shaped by factors such as limited alternatives for care, housing, or pressure from the entourage.
In addition, the primary reasons for visits were derived from clinical notes. Although patient statements were sometimes quoted, we did not have direct access to their perspectives of why they visited the PsyED. Due to the nature of the one-time emergency care setting (as opposed to longitudinal outpatient assessments), we also did not have the full information about their personal history, support networks, adverse life events, family context, physical health background, prior interactions with health care providers and services, or their overall level of self-determination in life and in seeking care. These gaps limit our ability to draw precise conclusions. Addressing them using complementary data sources is an essential next step for improving how emergency mental health services meet the specific needs of autistic adults. Service use patterns may be a product of the interactions between clinical profile, patient intersectional identities, and the type of support offered. Future research detailing the relationship between patient profiles and PsyED disposition could provide an important perspective on improving PsyED service design for autistic adults.
Second, many self-reported sociodemographic variables had high rates of missingness, which could have been influenced by patient capacity, clinical urgency at the time of visit, or comfortability to report. As a result, the reported effects (and a lack thereof) of sociodemographic factors known to impact mental health presentation and care-seeking behaviors, such as income, gender identity, and sexual orientation, must be interpreted with caution. Indeed, missing or inconsistent data on sociodemographic variables pose analytic and interpretive challenges. To inform clinically meaningful quality improvement actions from research, better quality and consistently collected sociodemographic data are needed. Another limitation to data exhaustiveness stems from the fact that both sociodemographic and diagnostic information were drawn from patients’ first visits only, which limits sensitivity to changes in status over time.
Third, the availability of data supporting inclusion may have influenced sample ascertainment. EMR chart selection for the autistic sample relied on the availability of confirmed autism diagnoses at the time of extraction (January 8, 2021), which was our sole identifier of inclusion. The autism diagnoses could be known before, at, or after the indexed PsyED visit, which may have introduced variability in service and clinical encounter patterns in the data. Longitudinal follow-up of patients would be informative to better understand their care pathways and assess the adequacy of services received, which requires a different study design.
Fourth, we analyzed charts from an urban mental health hospital in Canada. This factor affects the generalizability of the findings to rural communities and general hospital settings, where access to mental health services, including inpatient care and specialized staff, may be more variable (e.g., patients presenting with mental health difficulties might not be seen by a mental health team).
Fifth, despite descriptive analyses showing similar sample composition and co-occurring diagnoses before and during the COVID-19 pandemic, it seems that visits for substance intoxication increased during the lockdown. It is difficult to confidently interpret these patterns with our limited data covering only the first 10 months of the COVID-19 pandemic, although they were roughly aligned with reported pandemic influences.89,90
Lastly and importantly, the inclusion of a matched sample of non-autistic individuals is beyond the scope of and resource available for this project, so direct comparisons of our findings to a non-autistic PsyED patient population cannot be made at this time. It would be informative to explore differential use of the PsyED between autistic and non-autistic adults in future studies.
Conclusion
This study enriches the limited literature on the clinical profiles of autistic adults seeking psychiatric emergency care. Existing research on emergency mental health service use among autistic individuals largely focuses on young people and general hospital ED use, and rarely includes such a diverse sample.30,45,91 A key strength of this study is the use of large-scale PsyED chart data over a 3-year period, which provides detailed mental health profiles and a comprehensive overview of autistic patients with varying mental health crises and symptom severity. Findings provide important clinical implications to this high-risk, high-care-need subpopulation of autistic people, as the identified reasons and correlates for PsyED visits highlight key areas for future research and targeted mental health preventative and interventional efforts.
Authors’ Contributions
V.C. contributed to conceptualization, data curation, formal analysis, investigation, article drafting and revisions. M.F. contributed to conceptualization, data curation, investigation, validation, article drafting and revisions. C.C. contributed to data curation, methodology, validation, investigation, formal analysis, project administration, and article revisions. V.L. contributed to data curation, formal analysis, article drafting and revisions. L.L.Y.M. contributed to article drafting and revisions. C.-H.J.L. contributed to methodology, investigation, formal analysis, visualization, and article revisions. P.B. contributed to data curation, methodology, validation, project administration, and article revisions. C.P.-T. contributed to article drafting. P.J. contributed to conceptualization, methodology, data curation, and article revisions. S.H.A. contributed to conceptualization and article revisions. H.-Y.L. contributed to conceptualization and article revisions. A.S. contributed to conceptualization and methodology. J.Z. contributed to conceptualization and article revisions. Y.L. contributed to conceptualization, methodology, resources, project administration, and article revisions. M.-C.L. contributed to conceptualization, data curation, methodology, investigation, formal analysis, article drafting and revisions, resources, project administration, funding acquisition, and supervision.
Footnotes
Acknowledgments
The authors would like to thank the following colleagues who provided substantial support for data extraction and organization: Marina Charalampopoulou, Nishka Gupta, Abby Kazdan, Olivia Mendoza, Rianna Sarbajna, Areeba Sharafuddin, and Nahid Sultana. We would also like to thank Michelle Dawson for her valuable comments on the article.
Author Disclosure Statement
The authors declare no conflict of interest. M.-C.L. has received editorial honorarium from SAGE Publications.
Funding Information
This study received funding from the Innovation Fund of the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario (CAM-20-004, CAM-20-005) and the Canadian Institutes of Health Research Sex and Gender Science Chair (GSB 171373).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.