
Abstract
Background:
Suicide is a leading cause of death for autistic people worldwide, but there is remarkably little research addressing suicide prevention strategies in this group, and virtually none that asks autistic people what they need and want.
Methods:
Overall, 3962 autistic people and 627 people who supported or were bereaved by the suicide of an autistic person (>95% UK-based) participated in our online surveys. We garnered their ideas for policies and interventions to prevent suicide in autistic people (Phase 1). We thematically analyzed 2373 suggestions, distilling these into 63 ideas which an independent sample prioritized (Phase 2). We identified shared and differential priorities between participants.
Results:
Across two samples of autistic and non-autistic people, differences were overshadowed by consensus on necessary pathways to suicide prevention. Paramount among these were the upskilling and resourcing of healthcare services to deliver timely, autism-specific support, and the improvement of diagnostic services, ensuring autistic people not diagnosed in childhood are assessed accurately, quickly, and with sensitive post-diagnostic care. Other priorities, across phases, emphasized a social, societal response to suicide in autistic people, one where reducing stigma and providing social support were favored over crisis apps, and where support should be embedded across the life course in relation to education, employment, and social care in the community.
Conclusion:
While UK-centric, the findings corroborate international calls for autism-specific support for people in crisis, delivered by those with specialist knowledge. These results also highlight the relationship between suicide prevention and timely autism diagnosis, and the essential need for post-diagnostic care. Mirroring shifts in national and international suicide prevention policy, participant priorities extend the focal point of suicide prevention beyond individuals in crisis, emphasizing the need for coordinated, multisector efforts to address systemic societal determinants of suicide: a strategic and expansive perspective thus far lacking in an autism context.
Community Brief
Why is this an important issue?
Suicide is a leading cause of death for autistic people, but there is virtually no research exploring how it can be prevented. To design approaches that are helpful and relevant to this group, we must understand the ideas, needs, and desires of autistic people and those who support and/or advocate for them (henceforth “supporters/allies”) with regard to ways to reduce the number of autistic people who experience suicidal thoughts and die by suicide.
What was the purpose of this study?
We wanted to hear ideas for ways to prevent suicide from autistic people and supporters/allies. We moreover wanted to identify which of these ideas were community priorities for reducing the suicide rate in autistic people.
What did the researchers do?
We conducted a two-phase study using two online surveys, both designed with feedback from autistic people and supporters/allies. In Phase 1, we asked autistic people and supporters/allies for their ideas for policies and interventions to prevent suicide in autistic people. We analyzed 2373 free-text responses and distilled these into 63 concrete ideas. In Phase 2, we asked a larger number of autistic people and supporters/allies to select their priorities. Altogether, 3962 autistic people and 627 supporters/allies participated in the two phases of the study, most (>95%) from the United Kingdom.
What were the results and conclusions of the study?
Across over 4000 people, autistic and non-autistic alike, there was strong agreement about the most important routes to suicide prevention in both phases of the study. Chiefly, participants highlighted that healthcare professionals should receive better training to respond quickly and appropriately to autistic people in crisis, and that autism-specific, tailored approaches are needed. Participants also felt that preventing suicide in autistic people depends, in part, on ensuring that undiagnosed autistic people are diagnosed quickly, accurately, and sensitively, and given suitable post-diagnostic support. Their priorities indicate that thinking about suicide prevention needs to move beyond focusing exclusively on people who are already in crisis. In addition to crisis measures, suicide prevention requires a broad and social focus, tackling autism stigma and discrimination, ensuring autistic people are accepted and supported in society, and that they have equal access to education, employment, health, and social care throughout their lives.
What is new or controversial about these findings?
There is virtually no research on ways to prevent suicide in autistic people, and extremely few published scientific articles that ask autistic people for their opinions on this matter. We believe ours is the first study to systematically identify and prioritise autistic people’s ideas for specific policies and practices for suicide prevention.
What are potential weaknesses in the study?
The priorities identified by our samples might not be shared by autistic people with learning disabilities, people of color, or people from other countries.
How will these findings help autistic adults now or in the future?
The ideas and priorities of autistic people and their supporters/allies offer governments concrete ways to prevent the development of suicidal crises in autistic people and help those who reach crisis point.
Worldwide, suicide is a leading cause of death for autistic people without learning disabilities 1 ,1,2 who are five times more likely to die by suicide than non-autistic peers 2 and who, undiagnosed, may comprise a considerable portion of all individuals who die by suicide. 3 Despite a decade of accelerated knowledge production 4 and recent recognition of autistic people in the UK suicide prevention strategy, 5 our practical knowledge around preventing suicide in autistic people remains severely underdeveloped. 4 Accordingly, we lack applied approaches to help autistic people in crisis, as well as nationally and internationally applicable policies and practices to preventatively reduce the number of autistic people who consider, attempt, and die by suicide.
Limited research on suicide prevention in autistic people has thus far focused almost exclusively, to our awareness, on the narrowest point within the scope of suicide prevention strategies: effective assessment and treatment of individuals at crisis point.4,6,7 These constitute “indicated” interventions, often based in the clinical domain, directed toward those already experiencing suicidal thoughts and feelings. “Selective” and “universal” interventions, often preventative and directed at high-risk groups and whole populations respectively, have received far less attention in an autism context, although recent calls for whole-of-government approaches position these as most likely to achieve substantive reductions in suicide deaths.8,9 Requiring longer-term commitment, selective and universal approaches typically address the social determinants of suicide and other serious health problems, such as poverty and reduced access to healthcare.8,9 Such societal factors interact with individual-level risk factors for suicide (e.g., life experiences, neurobiological profile), as well as creating inequities which result in disproportionate risk of lifetime adversity, and suicide, in certain groups.8,9 Literature informing interventions in the autism-suicide intersection has largely pertained to risk factors at the level of individuals and their close networks, 4 with less, if any, recognition of societal factors such as the education and employment inequities which contribute to financial and residential insecurity,10,11 reduced healthcare access, or the marginalization of autistic people in society—factors which autistic people themselves link to suicidal feelings.12,13 Societal and systemic disadvantages faced by autistic people, including those which reduce access to indicated interventions in the clinical domain, 14 warrant widening our lens as regards to suicide prevention strategy, considering more preventative actions in addition to crisis interventions.
Identifying appropriate pathways to suicide prevention in autistic people requires addressing another notable deficiency in research, policy, and practice so far: insufficient involvement of autistic people and those who know them well. Academic knowledge-production in the autism-suicide intersection, including the design and delivery of clinical interventions, has largely occurred without community involvement.4,7 Similarly, autistic people and those who support and/or advocate for them are still excluded from policy decisions in the spheres that affect suicide rates—for instance, employment, health, and social care.8,9 To the best of our knowledge, a single priority-setting exercise, in 2021, 15 attempted to identify community priorities and through these bridge research and policy gaps related to autism and suicide. Focusing on identifying research questions and issues of greatest import to autistic people and their supporters/allies, participants in the exercise highlighted the need to find short-term indicated interventions for those currently in crisis, as well as longer-term preventative solutions. Recommendations in the subsequent policy brief, derived by the authors from the experiences of autistic participants in the exercise, included indicated, selective, and universal approaches to suicide prevention, ranging from introducing accreditation and legislation to enable healthcare providers to assess and support autistic people with suicidal thoughts, to improving the diagnostic process and the delivery of person-centered care. The authors highlighted that partnership with autistic people and their advocates was essential, since autistic people may not benefit from approaches designed for non-autistic people.15,16 Despite promotion of the policy brief to UK policymakers, the vague four-point action plan within the UK suicide prevention strategy for autistic people, 5 which emerged in 2023, lacks targeted actions by specific parties with measurable outcomes, and does not clearly demonstrate community engagement in its formulation.
As such, we aimed, herein, to address the dearth of co-production and practical knowledge around preventing suicide in autistic people, building on the previous research-focused priority-setting exercise by identifying specific policies and practices for suicide prevention from the autism community. In Phase 1 of our two-phase approach, we invited ideas for suicide prevention (i.e., suggested courses of action to prevent suicide) from autistic people and those who know them well, welcoming ideas across the suicide prevention continuum, from crisis interventions to longer-term prevention of the suicidal trajectory. In Phase 2, we identified community priorities by asking participants to rank the ideas generated in Phase 1, exploring where priorities differed in relation to participant characteristics (their status as autistic or non-autistic, alongside, in autistic people, their gender, age, and diagnostic status). In doing so, we sought to guide crisis interventions in addition to preventative measures to address societal and systemic drivers of suicidal thoughts in autistic people, thus reducing or eliminating the burden of suicidal thoughts and behavior. 17
Methods
Participants
We collected cross-sectional quantitative and qualitative data from two samples via online surveys (see Fig. 1). In both instances, we set eligibility criteria that participants should be autistic people over age 16 (self-identifying or formally diagnosed), individuals who presently supported and/or advocated for an autistic person, and/or who had been bereaved by the suicide of an autistic person (henceforth collectively “supporters/allies”). We recruited participants principally through social media and through UK charity mailing lists, including that of Autism Action (previously the Autism Centre of Excellence at Cambridge).
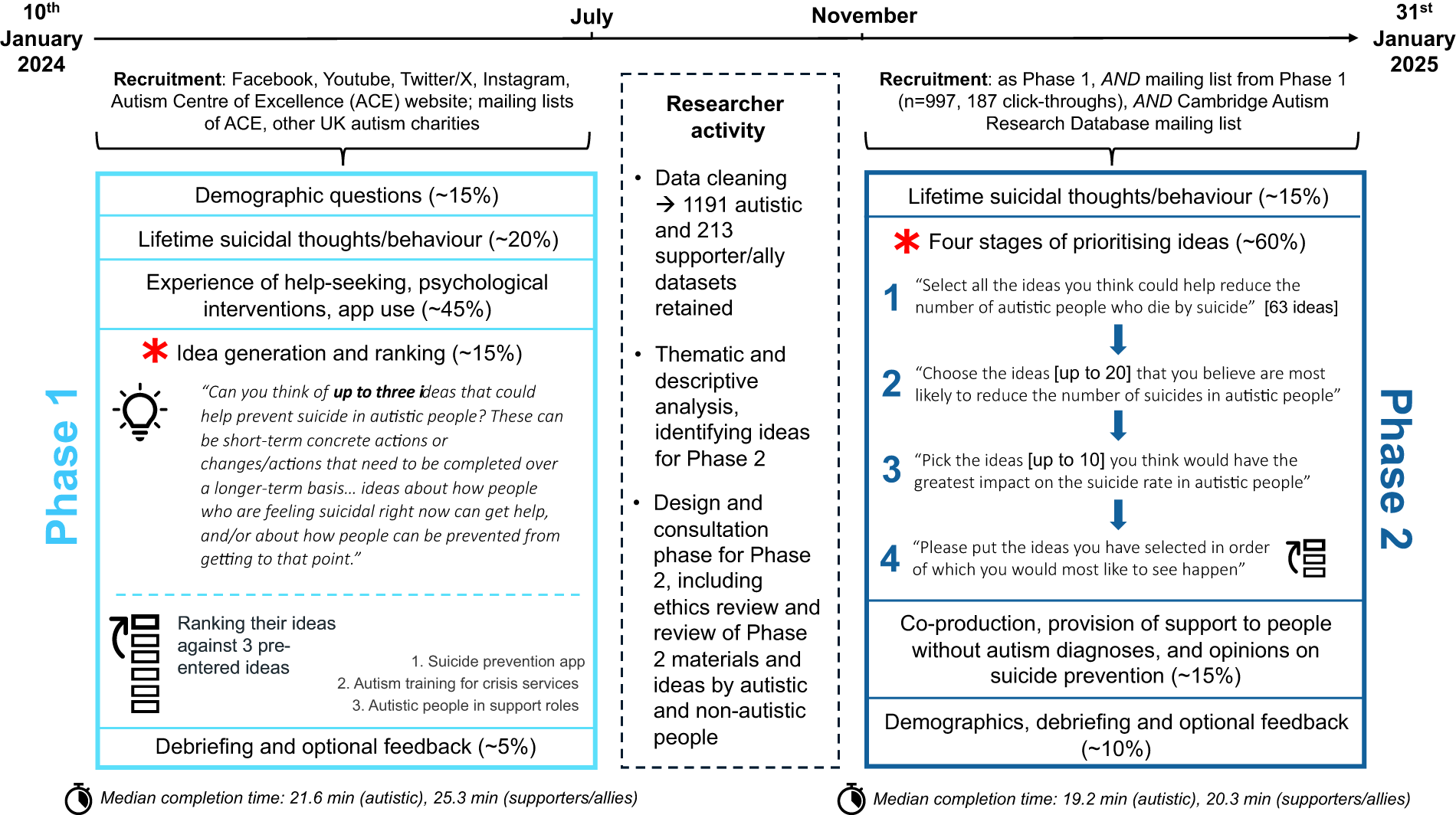
Flowchart of study timeline. Depicts the time course of the two-phase study; researcher activity, including recruitment periods and analysis of Phase 1 data; and participant activity in the Phases 1 and 2 surveys, including median completion times for autistic participants and supporters/allies in both phases. Red asterisks mark the sections which are the focus of this article; other aspects of the data are reported elsewhere.14–16
Following data cleaning (involving automated fraud detection measures and visual inspection for meaningful qualitative responses; see Supplementary Data S1), we retained data from 1404 Phase 1 participants (94.7% from the United Kingdom) and 3167 Phase 2 participants (all UK-based). Phase 1 included 1191 autistic participants and 213 supporters/allies; Phase 2 included 2771 autistic participants and 396 non-autistic supporters/allies. Notably, in Phase 1, we did not record if supporters/allies were themselves autistic, so we refer to these participants simply as supporters/allies. In Phase 2, we ascertained the neurotype of supporters/allies such that we could principally compare autistic participants and non-autistic supporters/allies; a small proportion of the autistic group (22.7%) also identified as supporters/allies of at least one other autistic person, as indicated in Table 1 (Supplementary Data S2).
Participant Demographic Information for Phases 1 and 2 Surveys
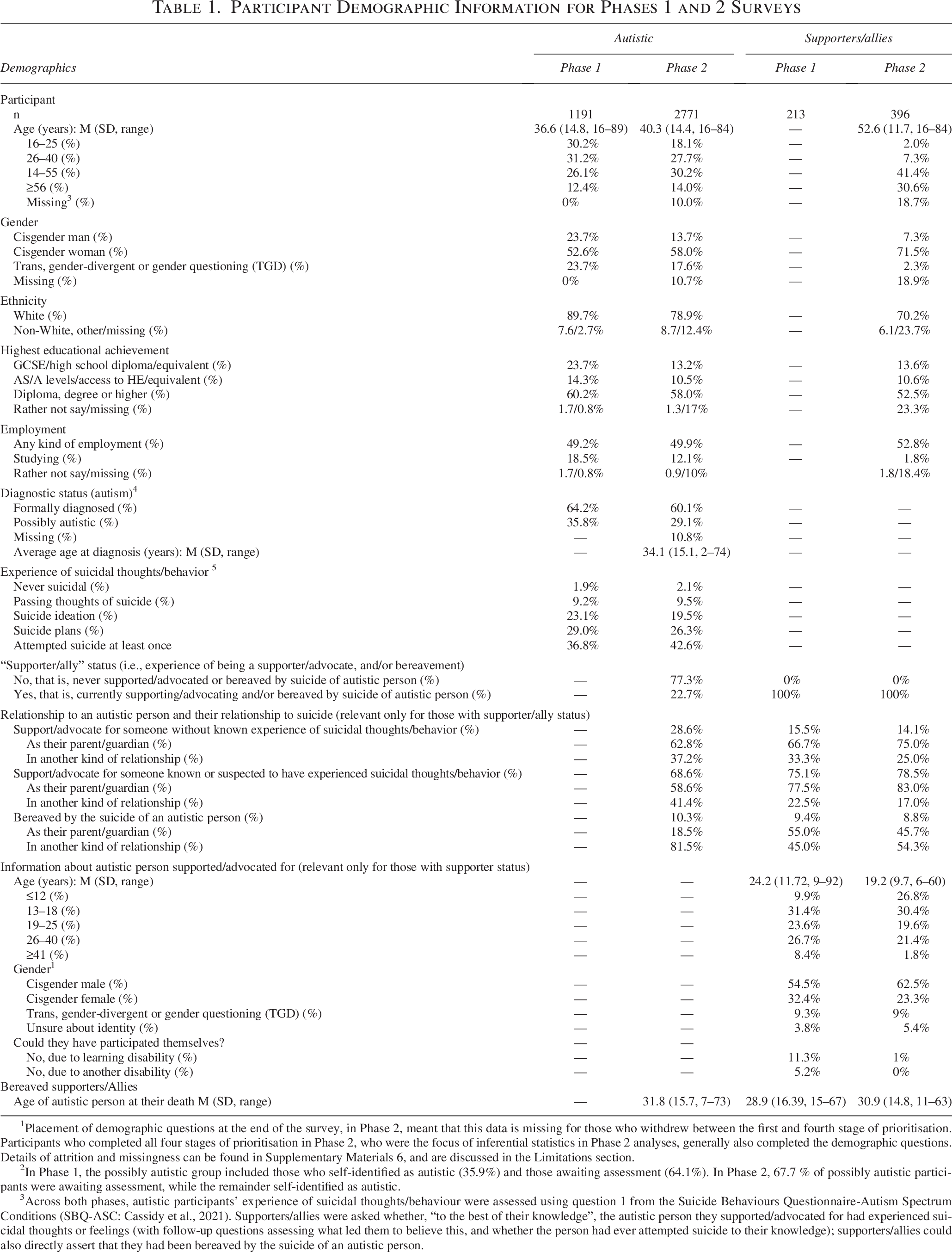
Placement of demographic questions at the end of the survey, in Phase 2, meant that this data is missing for those who withdrew between the first and fourth stage of prioritisation. Participants who completed all four stages of prioritisation in Phase 2, who were the focus of inferential statistics in Phase 2 analyses, generally also completed the demographic questions. Details of attrition and missingness can be found in Supplementary Materials 6, and are discussed in the Limitations section.
In Phase 1, the possibly autistic group included those who self-identified as autistic (35.9%) and those awaiting assessment (64.1%). In Phase 2, 67.7 % of possibly autistic participants were awaiting assessment, while the remainder self-identified as autistic.
Across both phases, autistic participants’ experience of suicidal thoughts/behaviour were assessed using question 1 from the Suicide Behaviours Questionnaire-Autism Spectrum Conditions (SBQ-ASC: Cassidy et al., 2021). Supporters/allies were asked whether, “to the best of their knowledge”, the autistic person they supported/advocated for had experienced suicidal thoughts or feelings (with follow-up questions assessing what led them to believe this, and whether the person had ever attempted suicide to their knowledge); supporters/allies could also directly assert that they had been bereaved by the suicide of an autistic person.
Procedure
We received ethical approval from the Cambridge University Psychology Research Ethics Committee (PRE.2022.097; PRE.2024.048).
Phase 1
We advertised the survey as the first in a two-phase approach to gather suggestions (“ideas”) for suicide prevention from autistic people and their supporters/allies. After asking about their sociodemographic characteristics, experiences with suicide and help-seeking (reported elsewhere13,18), we invited participants to enter three ideas that could help to prevent suicide in autistic people (200 characters per idea). We then asked participants to rank their ideas in relation to three pre-entered ideas, based on feedback from the design stage: These were included as examples and a means of engagement for individuals who struggled to generate their own ideas. These were: (1) “An app specifically for autistic people which offers ways to stay safe, manage emotions and access support” [henceforth “tailored suicide prevention app”]; (2) “Support existing services, such as the Samaritans and other suicide prevention services, to become or be more autism-friendly” [henceforth “autism training for crisis services”]; and (3) “Invest in paid peer-support roles for autistic people. Autistic people could be trained, employed, and supported in roles such as offering post-diagnostic support; offering mentorship and befriending to other autistic people” [henceforth “autistic people in support roles”]. Afterward, we offered participants the opportunity to provide feedback on the survey before presenting them with debriefing information, including support resources.
Phase 2
We initially asked participants to indicate whether they were autistic, had experience of supporting an autistic person, and/or had experience of supporting an autistic person who died by suicide. After questions contextualizing their relationship to suicide, we guided participants through a four-step process where they prioritized 63 ideas about suicide prevention in autistic people, which had been derived from Phase 1 (see Fig. 1 and Supplementary Data S3). By the final stage, participants had eliminated all but a maximum of ten ideas, which they ranked from 1 to 10 in order of greatest importance. Subsequently, we offered participants the opportunity to explain their choices and express their views on co-production and provision of support to undiagnosed, possibly autistic individuals (reported elsewhere 19 ). After asking sociodemographic questions and giving participants the opportunity to provide survey feedback, we provided debriefing information.
Analysis
Phase 1
Most participants (89.5% of autistic, 93.9% of supporters/allies) offered ideas for suicide prevention (see Supplementary Data S3), while the remainder ranked our pre-entered ideas without entering their own. We computed descriptive data for how participants ranked the pre-entered ideas, and analyzed 2373 qualitative responses (2011 from autistic participants) using a thematic approach.20,21 For the autistic data, we followed an inductive approach via the typical steps of data familiarization, code generation, theme identification, review, and definition. To stay true to participant language while achieving data reduction, we refrained from making high-level abstractions and used participant language wherever appropriate to do so, which resulted in a greater number of themes and related subthemes than is typical for thematic analysis (see Supplementary Data S3 for further detail and reflexive considerations). We subsequently analyzed the supporters/allies’ data in a deductive approach, using codes identified in autistic responses. Having reached consensus on the themes within both sets of data, we ranked these by frequency of occurrence in both groups and present these in the Results section, juxtaposed against the way in which participants responded to the survey’s pre-entered ideas.
Our qualitative analysis of Phase 1 data informed the ideas we prioritized in Phase 2. We were mindful, throughout, of our positionality and took steps to recognize and minimize our subjective influence on our analysis (see Supplementary Data S3) while also acknowledging the role the observer unavoidably plays in qualitative research analysis. To ensure fairness in the progression of ideas to Phase 2, we took the themes that appeared most frequently in the autistic data as the basis from which to identify recurring specific ideas in the autistic and supporter data that were associated with those themes and their subthemes. We identified 63 such ideas, each re-occurring anywhere between 20 and 200 times (across autistic participants and supporters/allies). When we identified specific ideas communicated in slightly different ways across participants, as much as possible, we formulated these as succinct ideas that encapsulated these different exemplars. Independent autistic and non-autistic panels reviewed these for clarity and accessibility, as well as methodological appropriateness. Our entire research team, who were privy to examples of how Phase 1 raw data were formulated into ideas for inclusion in the Phase 2 survey (see Supplementary Data S3), also reviewed these ideas.
Phase 2
We compiled descriptive statistics to reflect the number of times each idea was endorsed by autistic and non-autistic participants in the first three stages of prioritization, and the frequency with which each idea appeared in the fourth stage of prioritization, irrespective of rank (see Supplementary Data S5). We focused inferential statistical analysis on the final stage, involving 2737 participants (see Supplementary Data S5 and S6 for demographic information and details of missing data). These were exploratory; although we expected that priorities might differ between autistic adults and those who support them (principally parents of younger individuals), we had no directional hypotheses concerning specific ideas. Similarly, while we expected differential priorities across autistic people of different ages, genders, and different diagnostic journeys,12,13 we made no specific predictions.
For the 21 ideas that occurred with the greatest frequency in stage four, we created binary variables reflecting whether each participant endorsed that idea as one of their priorities for suicide prevention. We modeled these as a within-subject factor with 21 levels (“Ideas”) in three mixed ANCOVA (alpha levels corrected to p < 0.017), aimed at identifying differential weighting of ideas in the following contrasts:
We explored significant two-way interactions between “Ideas” and between subject variables with planned univariate tests of each idea separately, holding covariates constant and correcting alpha levels at a false discovery rate (FDR) of p < 0.05. For gender identity and age group, we used cisgender men and the youngest group as reference categories for simple contrasts. As statistical assumptions of sphericity were violated for the Ideas factor, we adjusted for this by reporting Greenhouse-Geisser values throughout.
Positionality and community involvement
We are a neurodiverse team in which several authors are autistic, have lived experience of suicidal thoughts and/or behavior, of supporting someone through suicidal thoughts/behavior, and/or bereavement by suicide. One way that we attempted to avoid researcher preconceptions of optimal suicide prevention pathways was by seeking and incorporating feedback from autistic people and their supporters/allies concerning the design of the surveys, data analysis, and the phrasing of Phase 2 ideas, and our presentation and interpretations of the findings (see Supplementary Data S7).
Results
Across two samples, each comprising autistic and non-autistic people, participants’ ideas and selected priorities demonstrated strong consensus on essential pathways to suicide prevention. Chiefly, they championed the need for autism expertise to be integrated throughout healthcare systems, for autism-specific offerings for mental health to be delivered in a timely manner, and for reform of diagnostic pathways, which should be faster, more accessible, sensitive to lesser-known presentations of autism and co-occurring conditions, and inclusive of post-diagnostic support. Additional priorities emerged across the two phases as follows, indicating the need to embed suicide prevention measures across the life course.
Phase 1
Consistency across participant-generated and pre-entered ideas
We identified 22 themes in the qualitative data of Phase 1 participants (Fig. 2A; see Supplementary Data S4 for thematic table), some of which reflected aspects of the pre-entered ideas that these participants had ranked (Fig. 2B). Together with responses to these pre-entered ideas, the ten most frequent themes (see Table 2) created a clear picture of this sample’s priorities.

Phase 1 data: Qualitative themes (A) and responses to pre-selected items (B).
Quotations Supporting the 10 Most Frequent Themes and Subthemes in the Autistic Data
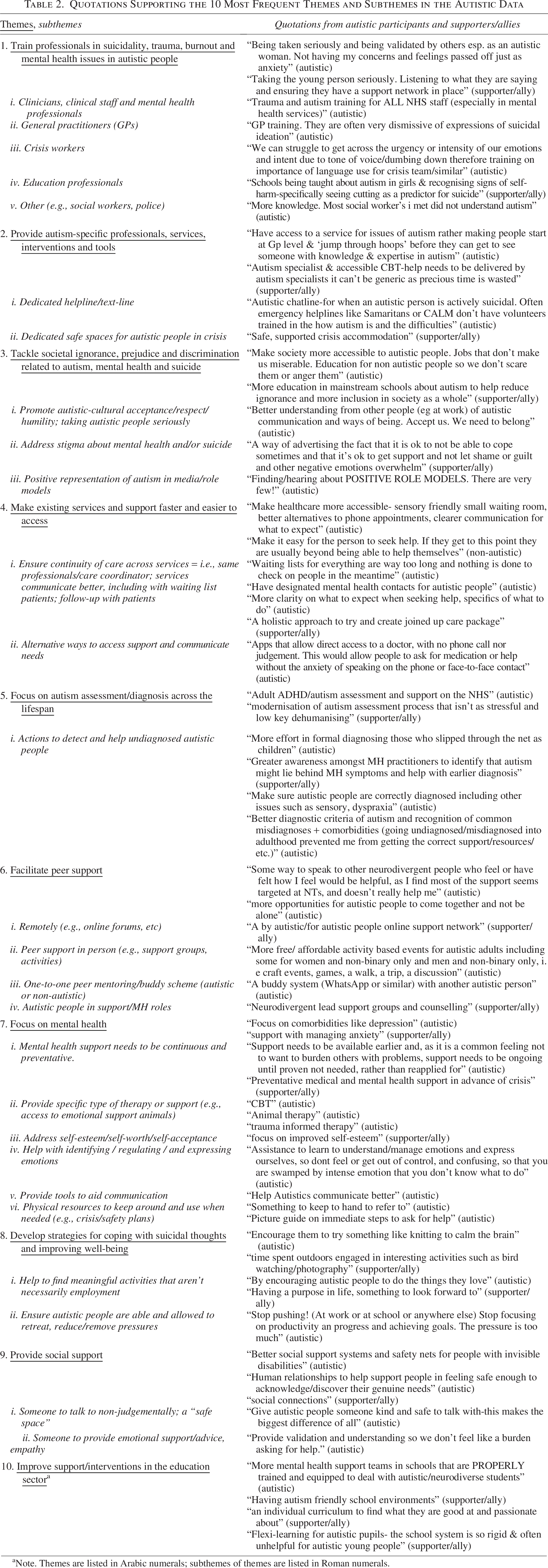
Note. Themes are listed in Arabic numerals; subthemes of themes are listed in Roman numerals.
Improvements to professional services were highlighted by most participants as an utmost priority for suicide prevention, with the training of professionals paramount for both autistic participants and supporters/allies. Relatively lower endorsement of “training for crisis workers,” as a pre-entered idea, was corroborated by relatively few mentions of these professionals in the qualitative data, in which participants predominantly spoke of healthcare (over 100 specific mentions) and educational professionals (43 specific mentions). Comments under this theme typically specified that training should enable professionals to understand autistic communication, recognize and respond appropriately to autistic presentations of suicidal thoughts, mental illness, burnout, and/or trauma; to “listen” and “take [the person] seriously.” These individually worded ideas indicate perceived areas where training is particularly needed, and suggest it must be expansive and specific, with some pointing to the insufficiency of currently mandated training within the United Kingdom. The insufficiency of current service provisions was also reflected in the second, fourth and seventh most frequent ideas in qualitative data from autistic participants: the need for specialist autism services, professionals, tools, and interventions (beyond the low bar of making existing pathways “autism-friendly”), for services to be easier and faster to access, and to focus on improving the mental health of autistic people.
The role of the social environment in suicide risk and its importance as a route to suicide prevention was indicated, first, by the high incidence of ideas related to reducing stigma and discrimination, and additionally by ideas pertaining to peer and generic social support. Very few qualitative responses related to “apps and technology-based approaches” were mirrored by a lower preference for a “tailored suicide prevention app” as a pre-entered idea. The most popular of the pre-entered ideas, “autistic people in support roles,” appeared largely akin to subthemes within the qualitative theme concerning “peer support” (the sixth most frequent in the autistic data). Formal support roles for autistic people were, in fact, a small proportion of ideas within this theme, which spoke more broadly about the need to establish “community.” The high frequency of ideas pertaining to stigma and to peer and social support, contrasted against the relatively lower frequency of others (e.g., apps and technology), spoke toward a social response to suicidality, one that prioritized peer and social support, and which situated tackling societal stigma and ill-treatment of autistic people as a foremost goal for suicide prevention.
Diverse roads to suicide prevention
Beyond our pre-entered ideas, several other kinds of idea were highly frequent in the qualitative data of Phase 1. Principal among these was a focus on autism assessment and diagnosis, which should be expedited, more accessible, and concerned with correctly identifying those missed for diagnosis as children. Other ideas pertained to finding resources to enable autistic people to cope with suicidal thoughts and improve their well-being; broader than apps, these might hinge on autistic passions and meaningful activity. Alongside focus on creating supportive, individualized educational systems (the tenth most frequent idea among autistic people), other highly frequent themes included ideas focusing on social care, employment and welfare, and the idea of education for autistic people on issues specific or highly relevant for them (e.g., burnout). The latter was frequently mentioned in the context of post-diagnostic support, which was coded separately only when expressed in very explicit terms.
Together, participant-generated ideas spanned crisis (indicated) to preventative (selective or universal) approaches. Frequently, ideas were expressed in the context of helping autistic people at crisis point, as was often the case for themes and subthemes pertaining to the training of professionals (theme 1); the provision of autism-specific services, professionals and interventions, such as helplines or text-lines (theme 2, subtheme i), and/or safe retreats (subtheme ii); improving access to existing services for people in crisis (theme 4, subtheme ii); providing psychological interventions (theme 7, subthemes ii, vi); developing strategies for coping with suicidal thoughts and improving well-being (theme 8); and identifying undiagnosed autistic people at risk of suicide and mental illness (theme 5, subtheme i). Themes were rarely, however, exclusively concerned with either crisis point or prevention. Selective or even universal approaches within these same themes were evident, for instance, in emphasis on early, preventative, and continuous mental health support (theme 7, subtheme i); continuity of healthcare, preventing patients from falling through the cracks and following up with them (theme 4, subtheme i); and autism diagnosis in childhood (theme 5). Themes more apparently weighted toward preventing the suicidal trajectory included addressing societal stigma and discrimination (theme 3); facilitating peer support (theme 6), or social support broadly (theme 9); and improving support in education (theme 10).
Differences and commonalities across participants
Across the Phase 1 qualitative data, the frequency of ideas appeared to differ across autistic people and supporters/allies. Unsurprisingly, the idea of supporting and educating those who support autistic people was more prevalent in the data from supporters/allies than that of autistic people, and their increased focus on the education sector reflected the fact that most supporters/allies were parents of young people. Broadly, autistic participants more frequently appeared to express the need for new systems and within-community support, while supporters/allies tended to emphasize the need for improvements to existing systems and generic social support. However, the most frequent kinds of idea were highly similar across autistic people and supporters/allies, highlighting the need for better professional understanding, autism-specific offerings, and accessible services to address mental ill-health.
Phase 2
Sample priorities across the staged prioritization process
Having endorsed ideas generated from the Phase 1 sample, the priorities of our Phase 2 sample are displayed in Table 3, which lists the 21 ideas that most frequently appeared in autistic participants’ final-stage priority lists, alongside their ranking in earlier stages and by non-autistic participants.
Ideas with the greatest number of selections in each round
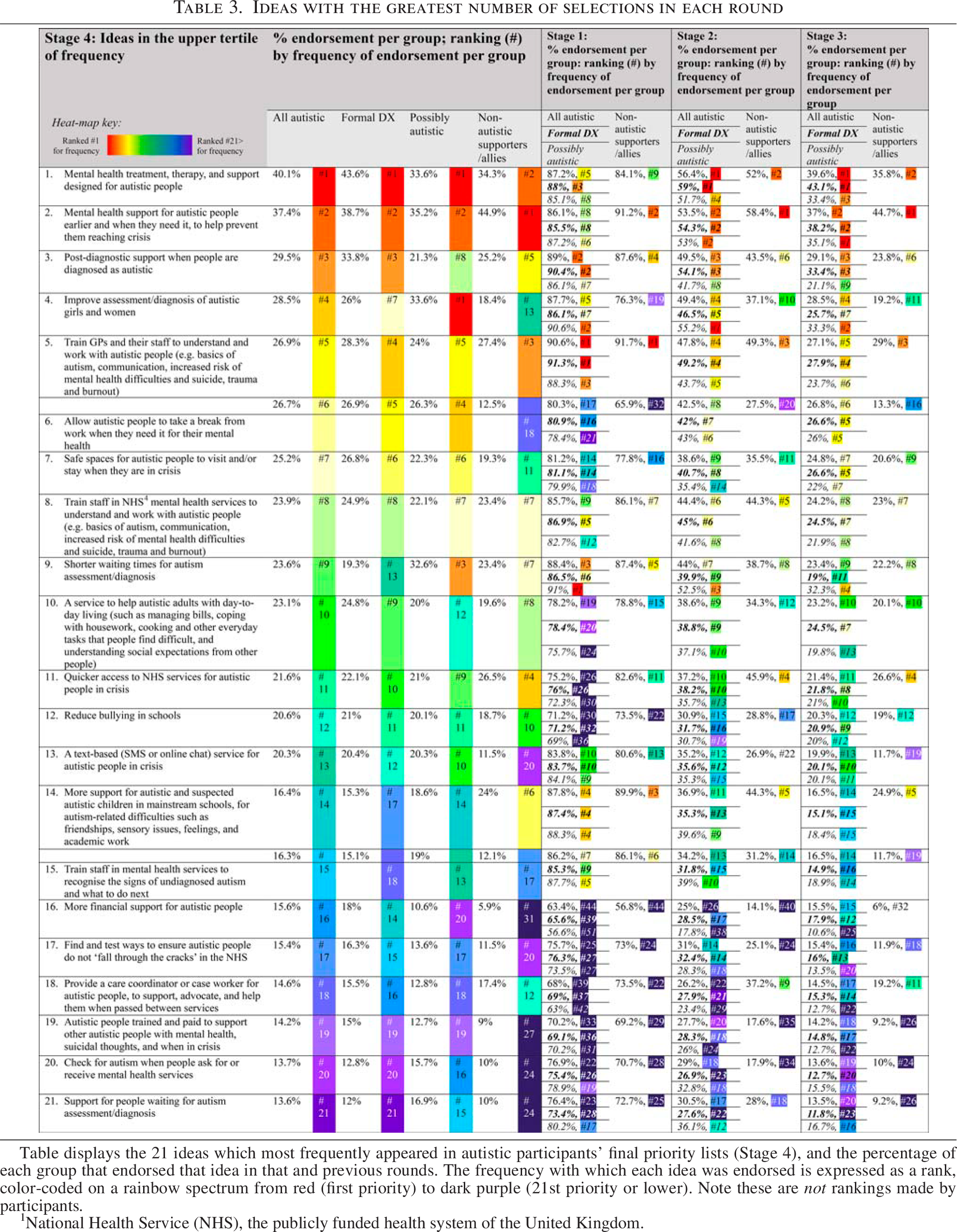
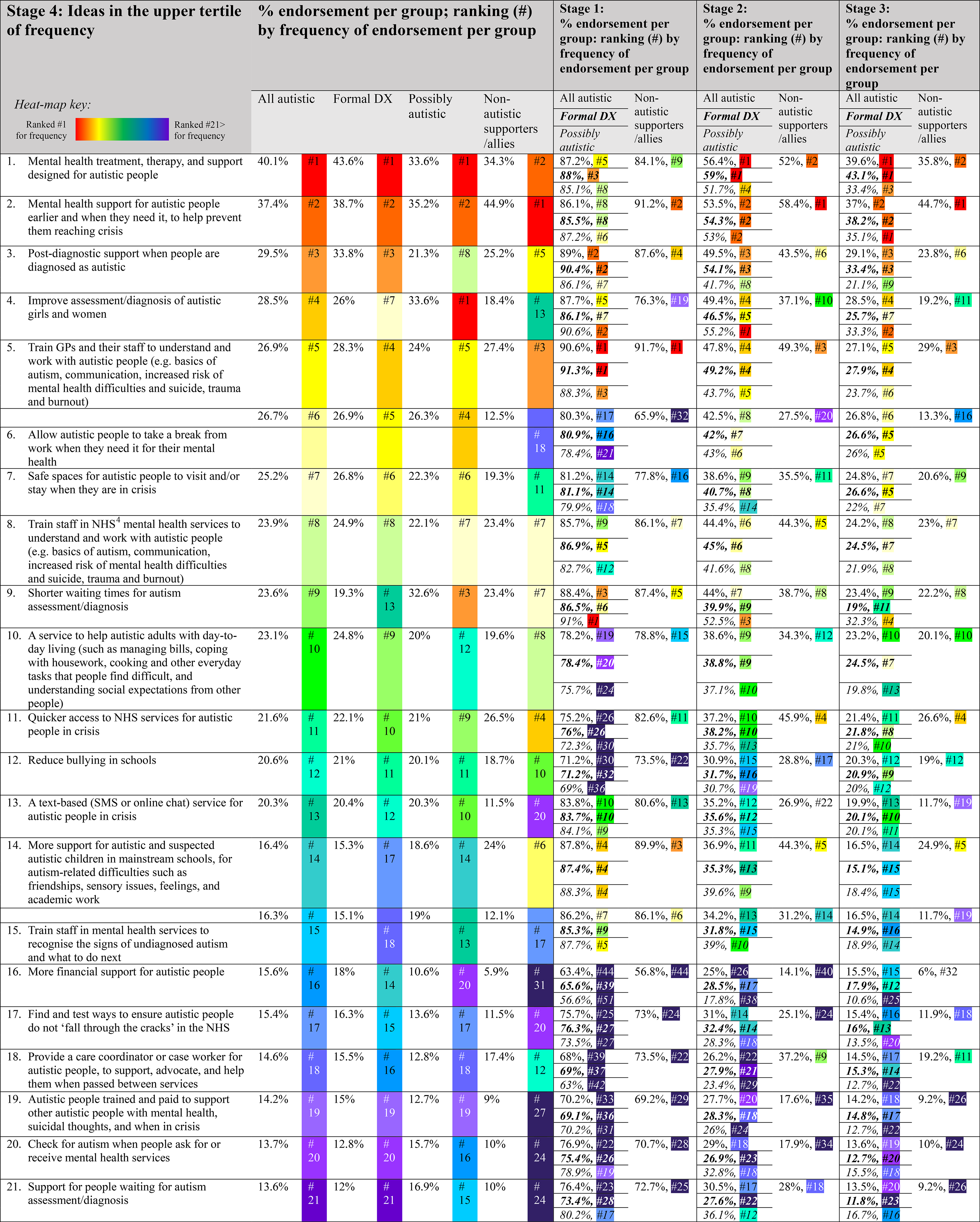
Table displays the 21 ideas which most frequently appeared in autistic participants’ final priority lists (Stage 4), and the percentage of each group that endorsed that idea in that and previous rounds. The frequency with which each idea was endorsed is expressed as a rank, color-coded on a rainbow spectrum from red (first priority) to dark purple (21st priority or lower). Note these are not rankings made by participants.
National Health Service (NHS), the publicly funded health system of the United Kingdom.
Refinement of priorities across stages resulted in the gradual relegation of some initially highly endorsed items, such as a text-based crisis service, while other items, such as tackling bullying at school, retained their popularity. Items consistently popular across stages for all participants were the need for early, preventative mental health support, support specifically designed for autistic people, improved access to diagnosis and post-diagnostic support, and better training for GPs 2 .
The priorities of Phase 2 participants ultimately spanned multiple sectors, indicating a complexity corroborated by their qualitative responses in our accompanying paper. 19 The ways in which participants grappled with considerations around the practical implementation of these ideas, such as the extent to which they should be co-produced and who should receive them, are detailed therein.
Differential priorities across neurotypes
Autistic and non-autistic participants significantly differed in their priorities, albeit with small effect sizes (ηp 2 < 0.02) (see Fig. 3 and Supplementary Data S8 for statistical notations). As in Phase 1, ideas related to the education sector had greater relative prevalence in supporters/allies, as did the importance of early, preventative mental health support; autistic participants, in contrast, gave more weighting to the ideas of a text-based crisis line, autistic people in supporting roles, identification and assessment of autistic girls and women, training of mental health professionals, more financial aid, and enabling withdrawal from work when needed.
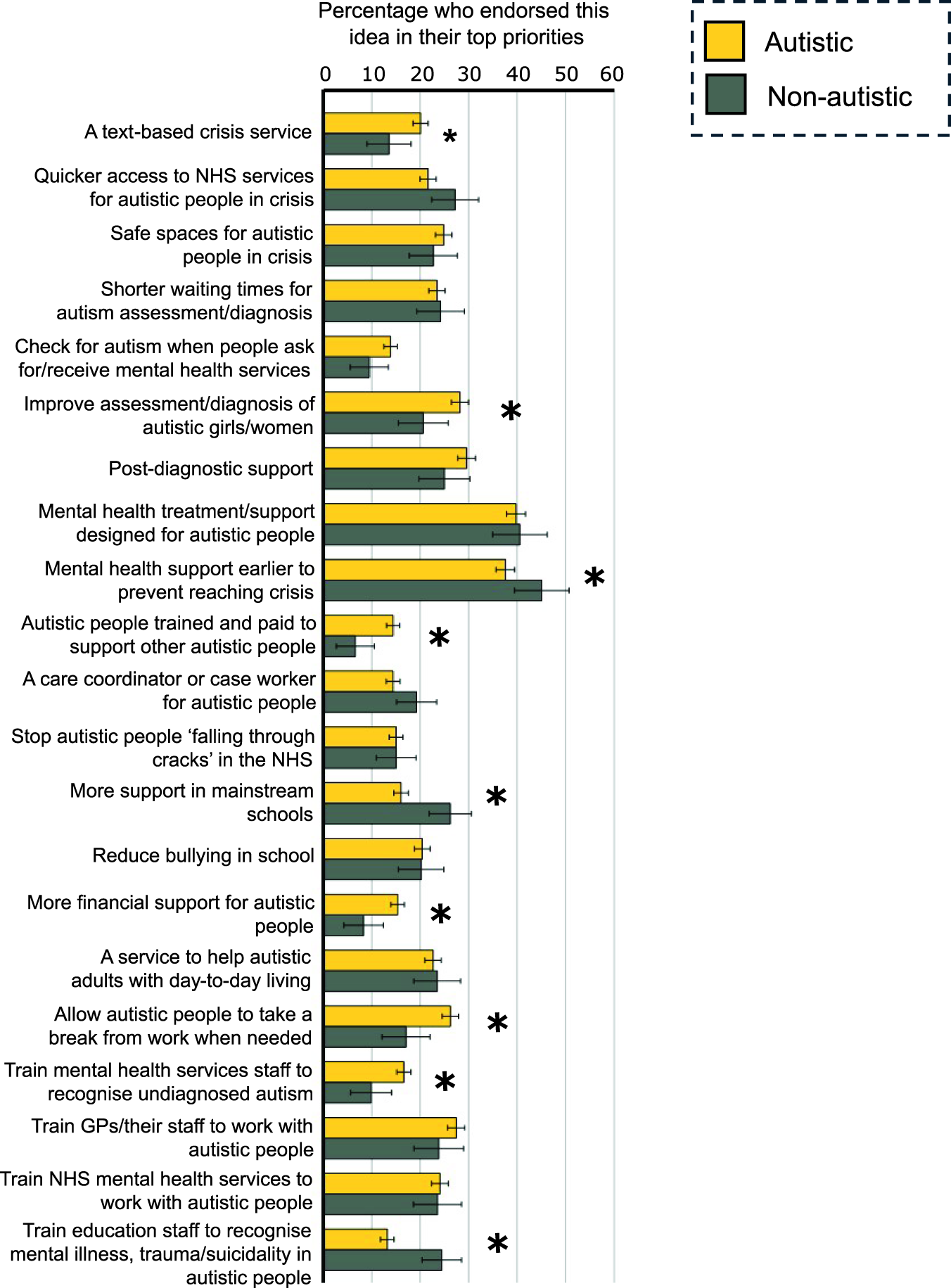
Differential prioritization of ideas for suicide prevention between autistic and non-autistic people. Depicts the percentage of autistic and non-autistic participants who endorsed each idea in their list of up to ten suicide prevention priorities. Group differences significant at an FDR-corrected threshold of p < 0.05 are marked with asterisks. Error bars reflect 95% confidence intervals.
Differential priorities across autistic people
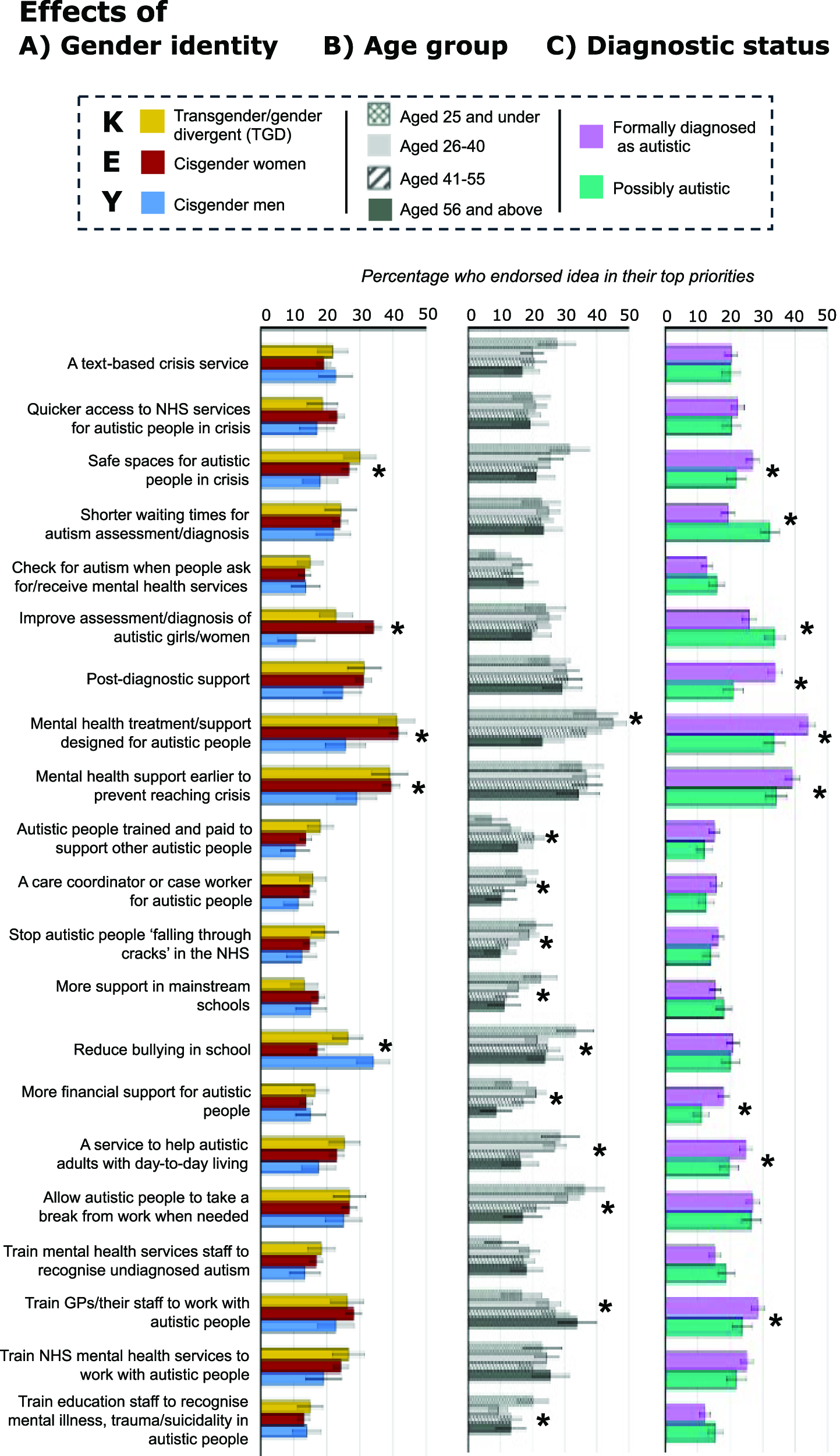
Within the autistic group, we also observed small (ηp 2 < 0.02) but significant differences in priorities in relation to the following individual differences (see Supplementary Data S9 for statistical notations).
Gender identity
These reflected that cisgender autistic men were more likely than cisgender women, and to some extent TGD participants, to prioritize tackling bullying in schools; the other groups were more likely to prioritize safe crisis spaces, tailored, early and preventative mental health support, and improved assessment and diagnostic of girls and women (Fig. 4A).
Effects of agender identity
Age
These reflected that the youngest group was more likely than older participants to prioritize tailored mental health support; improving coordination of NHS support; tackling bullying in schools; increasing support in mainstream education; support with day-to-day living; flexible breaks from work when needed; and improving autism recognition by education professionals (Fig. 4B). In contrast, the two oldest age groups were more interested in training for GPs and their staff, and peer support in mental health. The 26–40 age group placed a higher priority than other groups on the idea of a case coordinator or case worker for autistic people, and greater financial support.
Diagnostic status
These reflected that possibly autistic participants prioritized items related to obtaining a diagnosis; formally diagnosed participants were more likely to prioritize post-diagnostic support, along with safe spaces, tailored, early and preventative mental health support, greater financial aid, support with day-to-day living, and training for GPs and their staff (Fig. 4C).
Discussion
In a two-phase approach involving over 4000 participants, we collated and prioritized ideas for suicide prevention from autistic people and their supporters/allies. Phase 1 and 2 participants were highly consistent in their priorities, which, despite their UK-focus, reflect problems that exist worldwide. For instance, the need for autism-specific and tailored support in Phase 1 was mirrored by the high prioritization of support designed for autistic people in Phase 2, and research demonstrating reduced efficacy of psychiatric screening tools and psychological interventions in autistic populations,15,16 alongside the need for adapted approaches.6,22 The emphasis of Phase 1 participants placed on early, preventative mental healthcare was similarly reflected in the prioritization of early preventative support and upskilling of general practitioners (GPs) and other healthcare professionals in Phase 2. This echoes global problems of over-stretched healthcare services,13,23,24 insufficient professional understanding of autism and mental illness in autistic people,24–27 and unsatisfactory care for autistic people.13,14,23,26,28,29 Frequent requests in Phase 1 for free and easily accessible autism assessment across the lifespan corroborate well-established relationships between late diagnosis, mental health difficulties, and suicide,1,18,30 and Phase 2 participants joined academics31,32 in highlighting psychiatric populations as target groups for identifying undiagnosed autistic people. In Phase 2, ideas pertaining to autism assessment and post-diagnostic care constituted three of the final ten most frequently emerging ideas for suicide prevention—indicating that national crises in autism assessment33,34 and autistic mental health, 31 for our participants, are mirrors of each other.
The staged prioritization process of Phase 2 provided additional context for Phase 1 responses, which together appeared to reflect a microcosm of current thinking about suicide prevention. Emphasis on societal stigma, social support, and peer support, in Phase 1, was mirrored by strong endorsement of related ideas in the first stage of the Phase 2 prioritization process (Supplementary Data S5). Support for more generic ideas (e.g., teaching about neurodiversity in schools) decreased through the prioritization process, but more refined manifestations of these same themes from Phase 1, such as measures to reduce bullying, support everyday living in the community, and autistic people in paid support roles, remained popular to the final stage. To some extent, this process appeared to reflect deliberations 19 on the weighting of indicated, selective, or universal approaches, the latter of which are typically relegated by governments given their cost and long-term nature. 8 While the top ten prioritized ideas in Phase 2 included ideas pertinent to helping autistic people at a crisis point, they were slightly weighted toward selective actions intended to prevent autistic people from reaching a crisis point (as indeed indicated by the qualitative responses of these same participants). 19 Participants from Phase 1, given free rein and varied examples, also tended toward selective or even universal approaches. Indicated approaches are typically situated in the healthcare domain, 8 but the priorities of both of our samples clearly situate suicide in autistic people as a social problem, linked to exclusion, victimization, insufficient support, and barriers to equal and self-determined participation in society. 18 Accordingly, their priorities align with shifts in national and international policy toward coordinated, multisector responses addressing the societal determinants that give rise to suicidal distress.5,8,9,35 This perspective is lacking but urgently needed in an autism context to address these widespread inequities, necessitating policy changes in education, employment, welfare, health, and social care, and to ensure social inclusion.
Statistical comparisons of Phase 2 data reflected shared and differential priorities between autistic people and those who support them. As in Phase 1, autistic participants were more inclined than their supporters/allies to prioritize peer support, and placed greater emphasis on a text-based crisis service for autistic people, the need for breaks from work, financial support, and ideas associated with autism identification. Differences within the autistic group reflected age and gender differences in the factors that contribute to suicidal feelings and in help-seeking experiences. Autistic women and gender minorities, more likely than cisgender men to endorse physical and mental illness and difficulties accessing services when in crisis,13,18 were more likely than men to prioritize tailored and early mental health support, as well as safe spaces for autistic people in crisis. Women and possibly autistic people, overlapping groups, prioritized ideas associated with autism assessment and diagnosis, as per historic under-recognition of autism in people assigned female at birth 36 ; those with formal diagnoses were more likely to prioritize services which might be presumed to target diagnosed autistic people unless otherwise stated. Participants’ feelings about the provision of supports and services across diagnosed and undiagnosed individuals were, however, complex, as reported elsewhere. 19
Policy implications
There are several policy implications of these findings, and poignantly, as pertains to a UK context, these have minimal overlap with the present 4-point action plan for suicide prevention policy. 5 Two of four actions pertain to reviewing nationally collected data to “develop a clearer picture” and “identify areas of improvement to prevent suicide”; the third suggests the Department of Education “consider opportunities to provide support” to autistic children, and the fourth suggests that the Department of Health and Social Care “consider” results from an (incorrectly described) investigation of safety-planning. 6 We focus here on three implications supported by the priorities of autistic people and of supporters/allies, which move past reflection to recommended actions that should be coordinated across these and additional government departments. It is essential that any subsequent action be decided, designed and implemented in partnership with this community, 19 ensuring their needs and priorities are centered and potential harms avoided. 37
First, healthcare professionals, including GPs and those in mental health sectors, must be upskilled to understand the distinction between mental health conditions and autism, recognize differential presentations of mental illness, trauma, burnout, and suicidality, adapt their communication, and offer tailored interventions. A consistent high priority across phases, this was equally highlighted in the aforementioned 2021 policy brief, 15 which also urged legislation to prevent mental health services from rejecting referrals from autistic patients—a common experience among our participants 13 and those surveyed elsewhere.23,24,26 While beyond reasonable knowledge of our participants, there is growing evidence for several measures to appropriately assess17,38 and support 6 autistic people with suicidal thoughts and behavior. Autism-adapted safety plans, for instance, are rapid and inexpensive to implement, but clinicians lack confidence in their use. 39 Training and infrastructure to support implementation of existing tools and development of additional ones are desperately needed.4,15
Second, the capacity of diagnostic services must be increased to reduce waiting times and make diagnosis freely available to individuals of all ages, rather than a privilege related to socioeconomic advantages. 33 Focus on ensuring accurate diagnosis as early as possible is justified by robust evidence of an association between later age at autism diagnosis and mental health problems.30,40–42 Focus on ensuring the availability of assessments to undiagnosed autistic people is similarly justified by evidence that receiving a late-life diagnosis typically appears to improve well-being in the longer term, although it can invoke a turbulent period of adjustment which necessitates support.43–45 In additional qualitative data of our Phases 1 and 2 participants, reported elsewhere,12,19 participants suggested that accurate diagnosis can change or even save lives, through opening pathways to formal and/or informal support, receiving appropriate or adapted care for co-occurring mental health conditions (and addressing inappropriate care related to inaccurate diagnoses), facilitating individual sense-making and self-compassion, and facilitating connection with peers. 18 Consistent with literature describing the challenges of adapting to a late diagnosis,12,43,45 our data also demonstrates the vital importance of post-diagnostic support, 46 and low-cost solutions to address this need have been proposed.47–49
Third, systemic changes are required across education, employment, health, and social care to tackle marginalization of autistic people and embed support continuously throughout their lives. While UK suicide prevention policy broadly reflects expert consensus8,9 on the need for leveled, coordinated, and strategic approaches to address societal determinants of suicide, this kind of perspective is thus far absent from the startlingly limited policies pertaining to suicide prevention in autistic people, which also lack the tailored specificity highlighted as essential by our participants. Our participants concurred with academics8,9 that the greatest reduction in suicide deaths comes from disrupting the social determinants that build suicidal trajectories from childhood onwards, 19 including the societal stigma and insufficient educational support highlighted by Phase 1 participants. 18 The top ten priorities of Phase 2 participants are indicative of an inaccessible, inflexible, and burnout-inducing work culture combined with insufficient financial aid for disabled people;11,50 a rigid and reactive healthcare system,13,14 lacking appropriate spaces and interventions for people in crisis; 51 and a dearth of social care in the community. 11 The expansiveness of ideas across sectors and at different points in the suicidal trajectory 19 suggests that focus on any one, two, or three of the ranked priorities, alone, is unlikely to yield substantive reductions in suicide in autistic people; nor, as our accompanying paper 19 shows, is situating autistic suicidality as the purview of the mental health sector.
In summary and as elsewhere stated, 52 it is imperative that the whole-of-government approach applied to suicide prevention broadly 5 is translated to an autism context, and realized in a strategic plan, appropriately resourced, specific to this priority group and co-developed in partnership with the same. Of particular note in a UK context, we highlight that there exists legislation which should, in theory, include some of the measures suggested above; our data suggest, however, a significant policy-implementation gap, evidenced, for instance, in the number of Phase 1 participants rejected from healthcare services 13 in contravention of equality laws. Increased surveillance and accountability for the implementation of autism-related policies, involving community members, may be essential in ensuring legislation is enacted in society.
Strengths and limitations
Though boasting a large sample and a rigorous two-phase approach, there are several limitations pertaining to this work. Methodological decisions by the research group likely influenced participant decisions at numerous points, from our inclusion of pre-entered ideas in Phase 1 to our framing of the prioritization process in Phase 2. We took steps to minimize the influence of any individual preconceptions within the coding team, working closely and discussing all interpretations to consensus (see Supplementary Data S3). We progressed ideas to Phase 2 based on their frequency and co-occurrence, irrespective of other criteria such as their perceived feasibility or novelty. Notably, frequency or prevalence of themes is not typically construed as equal to their importance in qualitative analyses, 20 and we may have omitted some potentially promising ideas. Unavoidably, given the nature of the study, Phase 2 participants were constrained by the priorities of Phase 1 participants as interpreted and phrased by the research team. We did, however, seek and analyze the views of Phase 2 participants in a less constrained manner elsewhere. 19 The study was implemented by a neurodiverse team with autistic individuals in positions of influence. We attempted to incorporate feedback from non-academic community members throughout (see Supplementary Data S7), although our study fell short of optimal standards of community participation. These findings must not be interpreted as an exhaustive list of appropriate approaches to suicide prevention, particularly as specific ideas might have been difficult to generate, and participants could not be expected to be aware of emerging and developing approaches. 6 The potential benefits, harms, and limitations of the ideas prioritized here require careful exploration in partnership with autistic people, alongside consideration of pathways to implementation and appropriate means of evaluation. Future research should explore nuanced relationships between participant priorities and variables likely to be highly meaningful, such as, in autistic people, age at diagnosis and at the peak of suicidal thoughts; in supporters/allies, the age, diagnostic status, and co-occurring conditions of supportees; and in those bereaved by suicide, the circumstances of the bereavement. Given our relatively small but heterogeneous “supporter/ally” groups in both phases, we suggest cautious interpretation of the differential weighting of ideas and priorities between autistic participants and the “supporters/allies” of Phases 1 and 2, particularly as we did not ascertain the neurotype of Phase 1 supporters/allies, nor examine broader influences on participant priorities.
With insufficient representation in our sample, these priorities may not represent those of cisgender autistic men and gender minorities; individuals diagnosed as children; and autistic people with minority ethnic, racial, and cultural backgrounds, who may be disproportionately vulnerable to suicide and broader health and social inequities.53,54 Moreover, the priorities identified by our participants are unlikely to reflect the desires and needs of autistic people with learning disabilities and higher support needs, who are also at higher risk of suicide and self-harm but underrepresented in research.2,55 Many of these individuals, needing additional support to share their views, 56 would have been implicitly excluded by our approach. Notably, we may have introduced sample biases through our statistical focus, in Phase 2, on the final stage of the prioritization process. This decision, alongside that of focusing only on the 21 most frequently endorsed ideas in that stage, aimed to prevent an unwieldy number of analyses from obfuscating the clarity of findings and their interpretations. However, as demonstrated by the missing data in Table 1, a large proportion of participants withdrew from the survey before completing the fourth stage of prioritization. Placement of demographic questions at the end of the survey means little is known about participants who withdrew, but given the demanding prioritization process, they might conceivably have had a greater likelihood of co-occurring neurodivergence (e.g., ADHD or dyslexia, making concentration and reading more difficult), poorer physical health, more time pressures, and/or lower computer literacy.
Given that our data were collected in the United Kingdom, our findings may not be generalizable to other cultures and settings. Specifically, our findings reflect the infrastructure of UK services (as explicitly demonstrated in those ideas and priorities pertaining to “GPs” and the “NHS,” but implicit elsewhere) and the UK cultural landscape. Nonetheless, some of the priorities contained herein, and our related policy recommendations, are likely to be applicable to other similar or high-income environments, even if necessary to realize in the context of different public infrastructure: the need to upskill healthcare professionals and increase the capacity of mental health and diagnostic services, for instance, appear highly relevant to concerns raised in other countries,23,24,26,27 and may be similarly relevant to low- and middle-income settings. 57 However, other priorities not identified by us may exist in low- or middle-income settings where the majority of autistic people reside 58 and where, indeed, the majority of suicide deaths occur. 59 In low-resource settings where data about autism prevalence is not systematically collected and relatively greater proportions of the population are undiagnosed,60,61 the prevalence of suicide among autistic people is more nebulous than that derived from research in high-resource settings; 4 that said, existing data 2 are indicative that unrecorded, diagnosed and undiagnosed autistic people are likely to constitute a high proportion of suicide deaths in low- and middle-income settings. In countries that may lack political strategy for autism and where suicide prevention is superseded by other health priorities 62 participant priorities such as around decreasing waiting times for autism assessments or providing post-diagnostic and tailored mental health support, may not reflect the resources available for autistic adults or the scale of missed diagnoses. Specific pathways to and priorities for suicide prevention will necessarily differ in relation to culture, resources, and infrastructure across countries. As an initial step, however, we suggest that efforts to address health and social inequalities for autistic people across the world 63 must necessarily acknowledge that suicide appears to be a global threat. 2
Conclusions
Autistic people and their supporters/allies identified many pathways to suicide prevention. In addition to mental healthcare for individuals in suicidal distress, Phases 1 and 2 prioritized prevention through systemic change. Many of these recommendations are consistent with current approaches to suicide prevention (e.g., importance of support systems, prevention as priority)—approaches which, unfortunately, have been insufficiently applied in an autism context. Others highlight experiences that are likely to be relatively unique to autistic people (e.g., the importance of diagnosis and post-diagnostic support to long-term outcomes). Our recommendations are generally consistent with international suicide prevention frameworks, which we urge policymakers to adopt in an autism context, including specific nuances that are necessary for directly addressing increased risk within this priority group. In sum, there is an urgent need to reconceptualise suicidality in autistic people as a social problem requiring coordinated, sustained, and systemic effort across government, inclusive of education, employment, health, and social sectors, as well as communities, to reduce inequities and tackle marginalization. If acted on, we expect that these community priorities will ultimately reduce preventable death by suicide in autistic people.
Footnotes
Acknowledgments
The authors thank every participant who supported this two-phase project. The authors also thank the autistic people, and family members and loved ones of autistic people, who reviewed and offered feedback on our survey and communications and promotional material, including members of the Community Advisory Panel of Autism Action (previously the Autism Centre of Excellence at Cambridge) ; the ambassadors of this charity and outside organizations who aided our recruitment; and the Cambridge University Psychology Research Ethics Committee who reviewed this work. Finally, the first author would like to dedicate this paper to the memory of Professor Friedemann Pulvermüller, whose mentorship changed the course of her life and set the foundations of her future work.
Authors’ Contributions
Conceptualization and design: S.B.C., C.T.A., T.A.P., J.C., R.L.M., S.C., D.M., I.H., L.O., D.C., J.R.; data acquisition, analysis, and/or interpretation: all authors; however, R.L.M., T.P., T.C., and S.J.M. accessed the data herein; online advertising: T.A.P.; drafting: R.L.M.; and reviewing the work: S.J.M., M.P., E.W., T.P., C.T.A., T.A.P., C.S., T.C., H.H., D.M., J.R., I.H., L.O., J.C., D.C., D.H., and S.B.-C. All authors approved the final version to be published and accept responsibility to submit for publication.
Ethics Approval and Consent to Participate
Ethical approval of the study was granted by the Cambridge University Psychology Research Ethics Committee for both phases of the survey (PRE.2022.097; PRE.2024.048). All participants provided fully informed consent to take part in the study.
Consent for Publication
Consent to publish anonymized data was granted by participants.
Data Availability
The authors did not seek consent from participants to make our data publicly available. However, the authors welcome reasonable requests for access.
Author Disclosure Statement
R.L.M. and D.H. are deputy editors at Autism in Adulthood. Online promotion of both survey phases was funded by the charity Autism Action (previously the Autism Centre of Excellence at Cambridge), which initiated the project. T.A.P. and J.C. (employee and former employee of Autism Action) and S.B.-C., I.H., and L.O. (trustees of Autism Action) contributed to the design of the study, but not data analysis (while not being precluded from the data); they reviewed, agreed to, and accept responsibility for publication of the article. E.W., T.P., and M.P. receive funding from Autism Action for separate research on suicide prevention in autistic people. The remaining authors have no financial or personal interests to disclose. The article has been submitted solely to Autism in Adulthood.
Funding Information
Autism Action (previously the Autism Centre of Excellence at Cambridge) funded the online promotion of the survey used in this research. Pro bono support was provided by Teneo and Edmonds Elder to create and circulate communications and promotional materials. S.B.-C. received funding from the Wellcome Trust 214322\Z\18\Z. For the purpose of Open Access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission. S.B.-C. also received funding from the Innovative Medicines Initiative 2 Joint Undertaking under grant agreement No. 777394 for the project AIMS-2-TRIALS. This Joint Undertaking receives support from the European Union’s Horizon 2020 research and innovation program and EFPIA and AUTISM SPEAKS, Autistica, SFARI. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article, or in the decision to publish the results. S.B.-C. also received funding from Autism Action (previously the Autism Centre of Excellence at Cambridge), SFARI, the Templeton World Charitable Fund and the MRC. The authors are grateful to Cambridge University Development and Alumni Relations for anonymous donations. Any views expressed are those of the author(s) and not necessarily those of the funders, (including IHI-JU2). All research at the Department of Psychiatry in the University of Cambridge is supported by the NIHR Cambridge Biomedical Research Centre (NIHR203312) and the NIHR Applied Research Collaboration East of England. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.