
Abstract
Background:
Autistic adults experience disproportionately high rates of depression, yet Diagnostic and Statistical Manual of Mental Disorders, 5th ed., text rev. (DSM-5-TR) diagnostic criterion descriptions may not fully reflect their lived experiences, impacting opportunities for identification and support. Autism-related differences, such as alexithymia, interoception, cognitive styles, and sensory processing, may influence how autistic adults perceive, experience, and describe depression. This study examines whether autistic adults’ descriptions of depressive symptoms align with, or diverge from, DSM-5-TR criteria descriptions, to inform more accurate diagnostic practices.
Methods:
We conducted an exploratory qualitative study with 109 autistic adults and 13 caregivers, who reported on the autistic adult they support. Participants described depressive symptoms relative to their typical autistic baseline via an online survey (n = 112) or semi-structured interview (n = 10). Using direct content analysis, we identified symptoms consistent with DSM-5-TR symptom descriptions, and through inductive analysis, we identified additional features outside DSM-5-TR criteria.
Results:
Participants described depressive symptoms that both aligned with and diverged from DSM-5-TR descriptors. Participants often expressed depressed mood as anger or irritability, or as emotional numbness. Anhedonia involved a loss of enjoyment in deep interests (autistic anhedonia), a source of emotional regulation. They described fatigue as a pervasive physical heaviness and reported depression attacks, characterized by sudden, overwhelming suicidal ideation. Participants described depression as influencing autistic characteristics, including variations in sensory sensitivities, stronger insistence on sameness and routine, changes in hyperfocus within deep interests, and self-injurious behavior. They also reported that emotional awareness and expression difficulties, alongside heightened sensitivity and dysregulation, intensify during depression.
Conclusion:
Autistic adults described depressive symptoms, which we coded against DSM-5-TR criteria, and while most symptom descriptions aligned with DSM-5-TR criteria, some differed in form or expression. For some, reports suggested a bidirectional relationship between autistic characteristics and depression. Further understanding of autistic adults’ depressive symptoms is critical to improving diagnostic accuracy and guiding the design of autism-informed assessment tools.
Community Brief
Why was this study done?
Depression is common in autistic adults, but assessment typically relies on diagnostic criteria and screening measures developed for non-autistic populations and not well validated for autistic adults. This can contribute to missed or delayed recognition when presentations differ from expected symptom descriptions.
What was the purpose of this study?
This study aimed to understand how autistic adults describe their depressive symptoms and whether their descriptions align with or differ from the criteria in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed., text rev. (DSM-5-TR).
What did the researchers do?
We conducted an online survey and interviews with 109 autistic adults and 13 caregivers who reported on an autistic adult they support. Participants described how depression affected their emotions, thoughts, behaviors, and daily life. We analyzed their responses to identify common themes.
What were the results of this study?
Autistic adults reported many depressive symptoms that aligned with DSM-5-TR criteria, but also described some differences:
Depressed mood often felt like anger, irritability or emotional numbness rather than sadness. Anhedonia (loss of pleasure) often meant losing emotional connection and joy in deep and focused interests, which are usually an important source of emotional regulation. Some people described continuing their interests, but without the same enjoyment. Fatigue felt like physical heaviness rather than general tiredness. Although broadly consistent with DSM-5-TR concentration and indecisiveness criteria, participants often described executive-function impacts (task initiation, time management) and disrupted hyperfocus. Depression attacks, which they described as sudden, intense suicidal thoughts with a sense of losing control. Depression-related variations in autistic characteristics, such as fluctuations in sensory sensitivities, increased repetitive behaviors, and self-injurious behavior.
What do these findings add to what was already known?
This study provides new insights into how autistic adults describe depressive symptoms and how these descriptions align with DSM-5-TR criteria. Current diagnostic tools may not fully capture these symptom expressions, potentially leading to misdiagnosis or delays in receiving support.
What are potential weaknesses in this study?
This study relied on self-reported diagnoses and participants’ recall of symptoms, which may affect accuracy. Autistic adults with intellectual disability and people from diverse backgrounds were underrepresented, which limits generalizability.
How will these findings help autistic people now or in the future?
These findings provide a greater understanding of how depressive symptoms may be expressed and described by autistic adults, which may support recognition of depression-related change. By comparing lived descriptions with DSM-5-TR symptom criteria, the study indicates that many symptoms align with these criteria but may be expressed in ways that differ from how they are described in DSM-5-TR. This includes depressed mood expressed as irritability, anger, or emotional numbness, and autistic anhedonia, where deep and focused interests may be maintained while felt enjoyment or emotional connection is reduced. The results can inform autism-informed assessment prompts and guide the development of assessment tools that better capture autistic presentations, reducing missed or incorrect diagnoses and supporting timely access to care.
Depression is common among autistic adults, with lifetime prevalence estimates approaching 37%, nearly four times that of non-autistic adults. 1 Depression is associated with reduced quality of life, 2 increased loneliness, 3 greater difficulty maintaining employment, 4 and heightened strain on formal and informal support systems.5,6 Despite these significant risks and impacts, autistic adults’ own descriptions of depression remain rarely explored. 7 Recognition and diagnosis are complicated by diagnostic overshadowing, in which autism characteristics obscure signs of co-occurring depression. 8 Diagnostic frameworks such as the Diagnostic and Statistical Manual of Mental Disorders, 5th ed., text rev. (DSM-5-TR), 9 and depression measures were constructed and validated in neurotypical samples. Emerging evidence suggests they have limited sensitivity in autistic adults. 10 A recent review found that more than 90% of autistic people with depression reported experiences not encompassed in the DSM-5-TR criteria, 7 highlighting incongruence between diagnostic models and lived experience. Autistic adults also report substantial barriers to accessing adequate mental healthcare, 11 yet the absence of clear descriptions of depression in autistic people leaves practitioners without a reliable evidence base to guide assessment. This gap delays accurate identification and restricts timely access to appropriate supports.
Several features of depression, such as altered sleep or reduced social engagement, are also frequently experienced by autistic people.8,12 This overlap can obscure clinical recognition, leading to misattribution of symptoms to autism rather than co-occurring depression, delaying diagnosis and limiting access to support. The DSM-5-TR outlines criteria for mood disorders, most commonly major depressive disorder.9,13 Diagnosis requires at least five symptoms, including either depressed mood or anhedonia, along with changes in sleep or appetite, psychomotor activity, energy, self-worth, cognition, and/or suicidal ideation. 9 In 2022, the DSM-5-TR expanded these criteria to include irritability, anger, and somatic presentations as alternatives to depressed mood, features often reported by autistic adults experiencing depression.7,8,14 While these additions acknowledge broader variability, gaps remain in how these criteria reflect autistic adults’ descriptions of depressive symptoms.
Variations in how autistic people experience and describe depressive symptoms may be influenced by several underlying mechanisms identified in studies of depression and, in some cases, other co-occurring mental health conditions such as PTSD.15–17 These mechanisms may influence how autistic people perceive, express, and report depressive symptoms. 8 Alexithymia limits the ability to identify and describe emotions;15,18,19 interoceptive differences alter awareness of internal bodily states; 20 sensory processing differences heighten sensitivities to environmental stimuli;21–23 cognitive characteristics, including strong preferences for consistency or difficulty shifting from established patterns, can limit available coping options in some contexts;24,25 and reliance on self-soothing behaviors functions as an emotion regulation strategy.26–28 Their recurrence across multiple conditions, including depression, indicates that these mechanisms may contribute to variability in how depressive symptoms are described, particularly when compared with DSM-5-TR descriptors. This underscores the need to gather and systematically evaluate autistic people’s and their caregivers’ accounts of depressive symptoms.
Much of what is currently known about depression in autistic adults has been derived from standardized depression measures that were developed and validated in non-autistic populations. 29 These tools have not been validated for autistic adults and do not account for autism-related mechanisms that influence how symptoms are expressed and described. 10 Given the overlap between autistic characteristics and features of depression, elevated scores on these measures may not accurately indicate the presence of depression in autistic adults. For example, one study found that autistic adults without clinically diagnosed depression nevertheless scored significantly higher on a depression inventory than non-autistic peers without depression. 30 Despite these limitations, studies using such tools suggest that autistic adults who score highly often report features such as social withdrawal, changes in sleep or appetite, diminished motivation, and negative self-appraisal.8,29 Although some of these features overlap with DSM-5-TR symptom domains, there remains uncertainty about how autistic adults themselves describe depressive symptoms and whether these align with diagnostic criteria.
To date, no qualitative studies have examined whether autistic adults’ descriptions of depressive symptoms align with, or diverge from, DSM-5-TR criteria, leaving uncertainty about how depression is identified and assessed in this population. In contrast, qualitative research on other mental health conditions in autistic people, including anxiety31,32 and PTSD,
17
has shown that autistic people report some symptoms consistent with diagnostic frameworks, alongside additional signs not reflected in standard criteria. Few studies involving autistic people with depression suggest that mood disturbance may influence autistic characteristics, such as repetitive behaviors and deep and focused interests (commonly termed ‘special interests’).33,34 These findings highlight the value of qualitative approaches and support their use in depression research with autistic adults to examine whether reported symptoms align with DSM-5-TR descriptions or reveal variations. This study uses an exploratory qualitative design to investigate autistic adults’ descriptions of depressive symptoms, incorporating caregiver perspectives as complementary viewpoints and as proxies for those unable to self-report through study methods. It addresses the following research questions:
How do the depressive symptoms described by autistic adults and their caregivers align with the DSM-5-TR criteria for depressive disorders? What depressive symptoms do autistic adults and their caregivers report that do not align with the DSM-5-TR criteria for depressive disorders?
Method
Ethics statement
Our research team conducted the study from November 2023 to May 2024, following ethical clearance from Griffith University Human Research Ethics Committee (2023/725). All participants provided written informed consent after receiving information about their rights, including the right to withdraw at any point. We used identifying information only for scheduling and administrative purposes and stored all data securely in accordance with Griffith University’s data protection protocols. We deleted video recordings after six months and retained only anonymized transcripts for analysis.
Participants
We used theory-based sampling 35 to recruit autistic adults who had experienced depression. To participate, individuals needed to be at least 18 years old, live in Australia, and have either a formal or self-identified autism diagnosis. They also needed to report a past or current depression diagnosis or believe they would receive one if accessible. We disseminated recruitment materials through autism-specialized clinics, social media, institutional research broadcasts, and partnerships with community organizations. We included phrases such as “Help us learn how autistic adults experience depression” to support engagement. We closed recruitment when we reached our time and funding limits. We offered participants a $20 Wish Gift Card (accepted by 78%) and allowed them to complete the study via either an online survey (with talk-to-text functionality) or an online interview. We also provided support resources in case participants experienced distress.
Of the 253 adults who accessed the study, we excluded 83 due to incomplete registration, duplicate entries, missing consent, or concerns about response integrity. To screen for response integrity, we used a combination of logic checks and consistency-based criteria, drawing on methodological guidance from Pellicano et al. 36 We do not report specific screening procedures to preserve the integrity of future online autism research. Of the 170 eligible participants, 113 completed the online survey (73% of 154 who selected this option) and 10 completed an interview (59% of 17), resulting in a final sample of 122 participants: 109 from autistic adults and 13 from caregivers of autistic adults. Eighty percent of participants were either experiencing depression at the time of the study or had received treatment for depression in the previous three months, and 84% reported a formal depression diagnosis. Seven of the caregiver submissions involved collaborative responses with the person they supported. Given the small number of caregiver responses and the study’s focus on lived experience, we presented self-reports separately and did not compare across respondent types. In this paper, we use the term ‘participants’ to refer to both autistic adults and those described by caregivers. Participant details are included in Table 1.
Demographic Characteristics of Participants
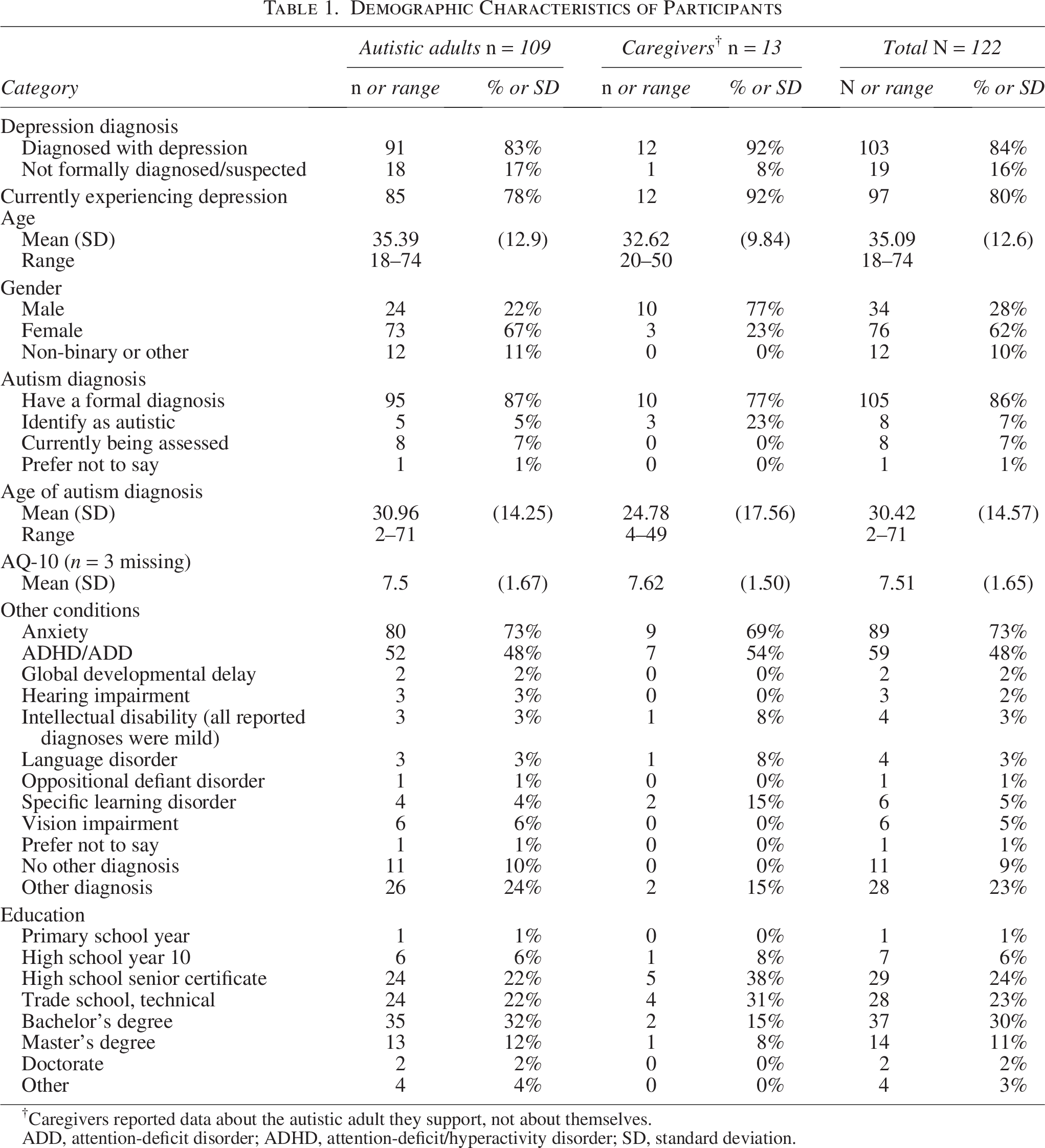
†Caregivers reported data about the autistic adult they support, not about themselves.
ADD, attention-deficit disorder; ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation.
Eighty-six percent of participants reported a formal autism diagnosis. To provide a descriptive measure of autistic characteristics, we administered the Autism Quotient-10 (AQ-10 37 ), a 10-item screening tool with adequate validity in autistic populations. Although the AQ-10 has shown good discriminant validity, it demonstrated low internal consistency in this sample (Cronbach’s alpha = 0.40), and we used it only for descriptive comparisons across diagnostic groups. The self-identifying group had a mean (standard deviation [SD]) AQ-10 score 6.59 (1.66), and the formally diagnosed group had a higher mean (SD) score 7.67 (1.61), consistent with expected autistic profiles. Most participants reported co-occurring anxiety (73%), and many had attention deficit hyperactivity disorder (48%). Eighty-five percent were born in Australia, 73% had at least one parent born in Australia, and 80% spoke only English at home. Caregiver respondents included four partners, four parents, two siblings, one cousin, and one psychologist.
Procedure
We used REDCap, a secure web-based platform, 38 to screen participants and administer the study. We required participants to complete eligibility questions before accessing the main survey or booking an interview. Survey participants answered questions using either typed responses or speech-to-text input. Interview participants joined via Microsoft Teams. We recorded and automatically transcribed each interview, and the first author manually reviewed transcripts for accuracy. We used the same question schedule for both formats, which asked participants to describe how depression affected their behavior, emotions, thinking, and body in comparison to their usual self. Interviews lasted between 12 and 108 minutes (mean = 39 minutes). We administered the AQ-10 at the end of both the survey and interview formats. To support accessibility in interpreting response scales, we included visual aids (e.g., a beacon image) to illustrate gradations of intensity and help participants select their responses. For interviews, we emailed participants a secure link to complete the AQ-10 independently, or with researcher support during the session. One participant opted to complete it with support.
Analysis approach
The first author transferred, cleaned, and managed data using Excel for qualitative responses and SPSS (version 29) for descriptive statistics. We used direct content analysis 39 to code experiences aligning with DSM-5-TR depressive symptoms (i.e., depressed mood, diminished interest, appetite changes, sleep disturbances, psychomotor issues, fatigue, feelings of worthlessness, concentration difficulties, and suicidal ideation). We used inductive content analysis to code experiences that did not align with DSM-5-TR criteria. We developed a coding framework that incorporated both DSM-5-TR criteria and additional inductive codes generated from the data. Each code was operationally defined to support analytic consistency. For constructs not represented in the DSM-5-TR, definitions were informed by relevant literature19,20,26,40–47 and refined through an iterative coding process. This approach was extended across all additional categories, ensuring clear operational definitions of categories outside the DSM-5-TR criteria. The complete coding framework, including DSM-5-TR and inductive codes, is provided in Supplementary Table S1. To ensure findings reflected common experiences, we excluded categories reported by fewer than 10% of participants.
The first author segmented responses into smaller units of meaning to code distinct concepts with precision. For example, in the statement “Lethargy, really exhausted and tired all the time, and I can’t do my work anymore,” we coded the first segment as ‘Fatigue’ and the second as ‘Impaired Functioning’ (DSM-5 Criterion B). An autistic researcher with a psychology background reviewed the full coding dataset and met with the first author to resolve discrepancies through discussion. They reached 95.14% agreement on coding accuracy and refined the framework iteratively through feedback cycles.
Community input statement
This study was developed in response to autistic community–identified research priorities, including the need to better understand mental health and well-being in autistic adults that reflects the lived experiences of autistic people.48–50 Although the project was not co-designed from its inception, autistic advisors and contributors with lived experience were involved in informing the study materials and the interpretive process. The lead author, a parent of an autistic person with intellectual disability, drafted the initial survey and interview questions. An autistic psychologist revised the materials to ensure clarity and accessibility. Three additional community members, including autistic adults with and without intellectual disability and another parent, provided further feedback. An autistic research assistant contributed to initial inductive coding and helped develop preliminary category definitions. A second autistic researcher conducted a full review of the final codes. These participatory contributions strengthened the study’s conceptual coherence and ensured that our interpretations remained grounded in autistic perspectives. The process prioritized accessibility, contextual sensitivity, and communication approaches aligned with autistic preferences, consistent with inclusive research practices recommended in autism research. 51
Results
DSM-5-TR symptoms of depression
This section presents participant-reported symptoms organized by DSM-5-TR criteria. For each criterion, we summaries how the symptom was described, highlight autism-related variations in expression that may influence clinical recognition, and report the proportion of participants who described each symptom. Table 2 presents DSM-5-TR symptoms that autistic adults described as consistent with DSM-5-TR descriptors. Table 3 presents DSM-5-TR depressive symptoms that autistic adults described differently from DSM-5-TR criteria descriptors, outlining variations in their manifestation. Frequencies are provided separately for self-report and informant reports in Supplementary Table S2; self-report and informant comparisons were not undertaken due to sample size.
DSM-5-TR Depression Criteria and Categories with Definitions, Percentages, and Examples
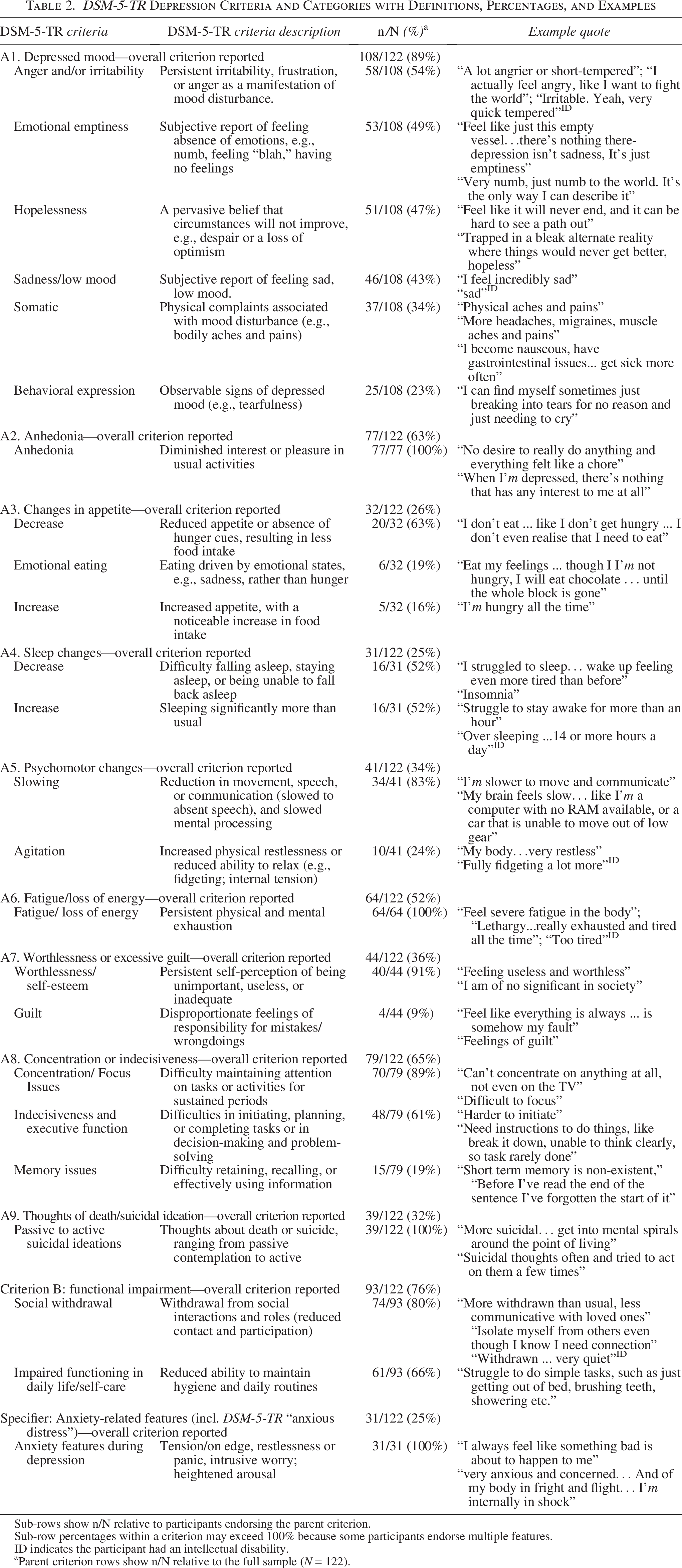
Sub-rows show n/N relative to participants endorsing the parent criterion.
Sub-row percentages within a criterion may exceed 100% because some participants endorse multiple features.
ID indicates the participant had an intellectual disability.
aParent criterion rows show n/N relative to the full sample (N = 122).
Autism-Related Alternative Expressions Within DSM-5-TR Depressive Criteria
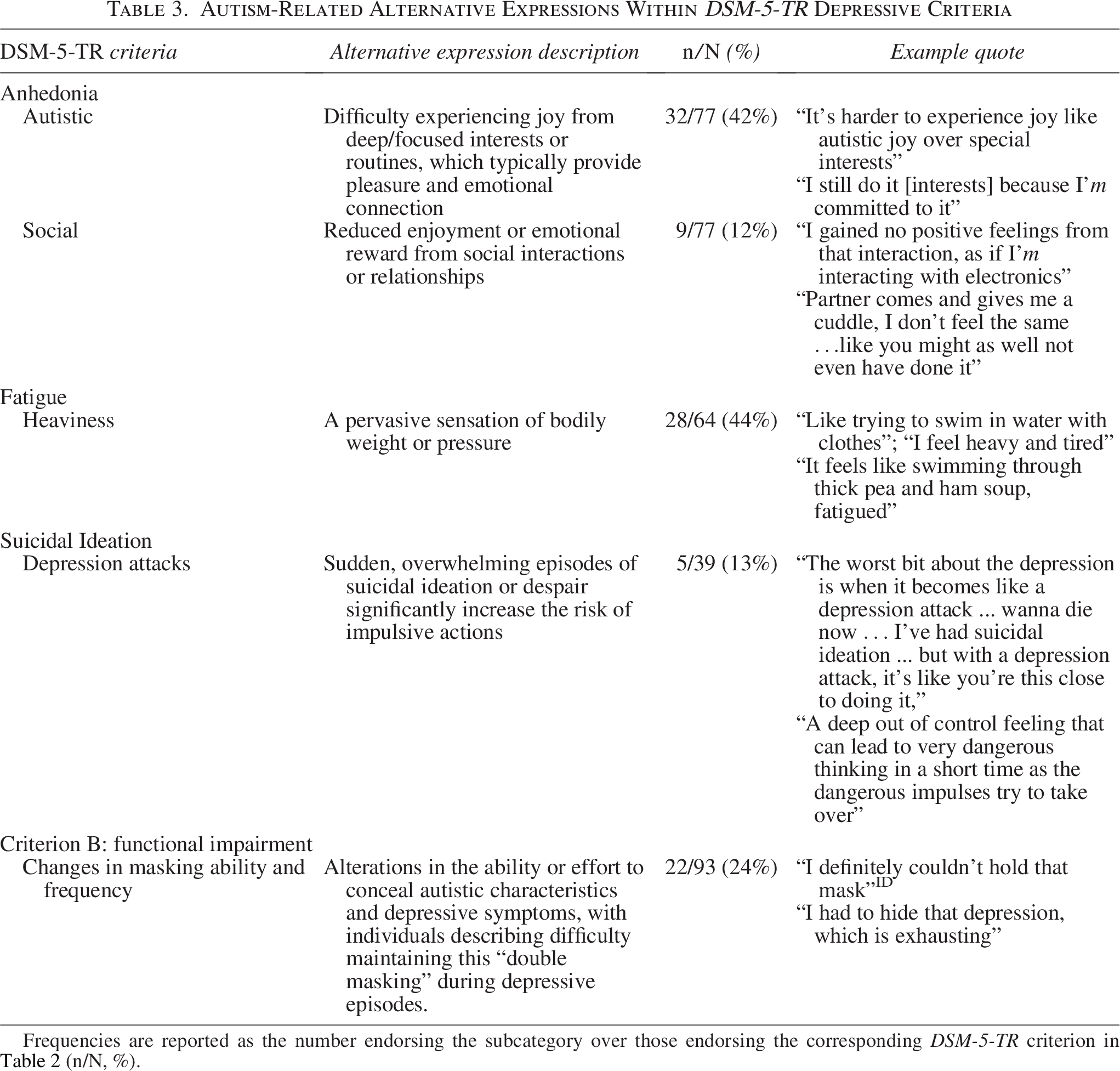
Frequencies are reported as the number endorsing the subcategory over those endorsing the corresponding DSM-5-TR criterion in Table 2 (n/N, %).
Criteria A1: Depressed mood
Depressed mood emerged as the most common symptom, reported by 89% of participants, encompassing a range of emotional, cognitive, and somatic experiences. Sadness (43%) was often described as heavy and overwhelming. Crying or the urge to cry was reported by 23% of participants. Emotional emptiness, numbness, or a flat affect (49%) reflected an absence of feeling, a sense of hollowness, and disconnection from emotions. Hopelessness and despair (47%) involved convictions that circumstances would not improve, that the emotional state was unending, and that life lacked meaning, often reinforced by repetitive negative thinking and difficulty disengaging from pessimistic thoughts.
Anger and irritability (54%) were the most common manifestations of depressed mood. Participants described irritability as heightened reactivity to minor stressors, leading to agitation, impatience, or short-tempered responses. They sometimes directed anger at societal norms or interpersonal frustrations, which could manifest as verbal outbursts. Somatic features during depressed mood (34%) included headaches or migraines, muscle tension, generalized body pain, gastrointestinal discomfort, and difficulties regulating body temperature. During coding, anger and irritability were sometimes described alongside somatic complaints (e.g., headaches, gastrointestinal distress). This co-occurrence was not systematically analyzed but was noted as a recurring feature in several accounts.
Criteria A2: Anhedonia
Participants described anhedonia (63%) in ways that aligned with DSM-5-TR descriptors, including a lack of joy or emotional disconnection from previously enjoyable activities. They also described two forms not specified in DSM-5-TR: autistic anhedonia (42%) and social anhedonia (12%). Autistic anhedonia referred to losing the ability to experience joy from deep or focused interests that usually provided self-worth and emotional regulation. Participants noted that this loss left them emotionally less stable during depressive episodes, and they often continued these activities out of habit or obligation rather than genuine enjoyment. Social anhedonia referred to losing the sense of reward from social interactions. Participants described once-enjoyable connections feeling empty, with little motivation or desire to seek out or maintain contact.
Criteria A3: Changes in appetite
Changes in appetite were reported by 26% of participants, encompassing both increases and decreases in food intake, similar to DSM-5-TR descriptors. Most (63%) described a loss of appetite, as well as a loss of thirst, the absent internal hunger cues, such as not eating for an entire day without feeling hungry or noticing the stomach growling without any sensation of hunger. Increased appetite was reported by 16%, and emotional eating by 19%.
Criteria A4: Changes in sleep
Changes in sleep patterns were reported by 25% of participants, consistent with DSM-5-TR descriptors of insomnia or hypersomnia. Of those reporting changes, 52% described either increased or decreased sleep, with an equal split between the two, and 13% reported erratic or highly irregular patterns. Some participants noted using sleep as a way of escaping from depression, while others reported difficulties falling or staying asleep that contributed to daytime exhaustion. Regardless of sleep duration, sleep quality was described as insufficient.
Criteria A5: Psychomotor changes
Psychomotor changes consistent with DSM-5-TR descriptors of agitation or retardation were reported by 34% of participants. This included 28% who described physical slowing and 8% reported agitation. Slowing was experienced as the body feeling frozen or sluggish, often accompanied by a similar slowing of mental processes that affected focus and communication. Agitation was characterized by fidgeting and an inability to relax or remain still.
Criteria A6: Fatigue
Participants described fatigue (52%) in ways that met DSM-5-TR descriptors, including profound lethargy and pervasive fatigue, marked by a lack of energy that impaired both physical and mental functioning. Some (44%) characterized it as a sensation of heaviness, akin to moving through quicksand, an experience not in the DSM-5-TR criteria. Mental fatigue left some feeling mentally drained, making even routine tasks unmanageable.
Criteria A7: Feelings of worthlessness and excessive guilt
During depressive episodes, participants frequently described feelings of worthlessness (33%) and, less commonly, excessive guilt (3%), together reported by 36% overall. These experiences were often linked to how they believed others perceived them and to a perceived inability to meet expectations. They characterized worthlessness through pervasive negative self-talk, a sense of insignificance, and a heightened awareness of failure, which contributed to social withdrawal. Excessive guilt centered on unmet personal and social responsibilities, such as parenting, partnering, or work roles. Feelings of worthlessness and guilt align with DSM-5-TR descriptions, although DSM-5-TR specifies that self-reproach or guilt should not arise solely from perceived personal shortcomings. Participants nevertheless described these experiences as excessive or disproportionate, often relating them to their own expectations of fulfilling specific roles. The internalized sense of failure fueled a cyclical pattern of negative thinking, self-criticism, and self-loathing during depressive episodes.
Criteria A8: Diminished ability to concentrate or indecisiveness
Participants described concentration and decision-making difficulties (65%) that met DSM-5-TR descriptors, including poor attention, indecisiveness, and difficulties making decisions. Participants (89%) reported changes in sustaining attention, often due to “mental fog,” short attention spans, or frequent mind-wandering, which disrupted daily activities. Decision-making felt overwhelming for 61%, with even simple choices becoming unmanageable, consistent with DSM-5-TR definitions of indecisiveness. Participants also described experiences outside DSM-5-TR descriptors, including executive function difficulties such as task initiation and time management problems, and disruptions in hyperfocus, characterized in autistic adults by immersive, sustained engagement with specific tasks or interests, often described as a “flow” state, which they were unable to initiate or maintain during depressive episodes. This loss differed from general concentration difficulties described in DSM-5-TR, as it reflected the absence of a distinct, highly focused cognitive mode rather than a broad reduction in attentional capacity. One in five (19%) reported memory issues, further compounding their cognitive difficulties.
Criteria A9: Recurring thoughts of death or suicide
Participants (32%) described recurrent thoughts of death or suicidal ideation during depressive episodes, generally aligning with DSM-5-TR descriptions. These experiences ranged from passive contemplation, a desire to escape life without specific plans, to active ideation, including planning or attempts. They also described depression attacks, intense episodes where suicidal ideation escalated rapidly, accompanied by a profound sense of losing control and an urgent impulse to act, an experience not represented in DSM-5-TR. Despite the severity of these thoughts, participants identified protective factors, such as family and loved ones, that helped prevent them from acting on their impulses.
Criteria B: Functional decline and social withdrawal
Social withdrawal was common during depressive episodes, reported by 61% of participants, and aligned with the DSM-5-TR Criterion B definition of functional impairment. However, participants’ descriptions highlighted forms of impairment not specified in DSM-5-TR, such as avoiding interactions to reduce sensory input, manage emotional and cognitive overwhelm, and create space to process thoughts. This withdrawal often led to reclusive behavior, a preference for solitude, and difficulties communicating even with close family members. Heightened sensory sensitivities further intensified these behaviors, prompting avoidance of overstimulating environments and neglect of daily responsibilities and social commitments, contributing to isolation. Half of participants (50%) described experiencing declines in daily functioning and self-care during depressive episodes, including difficulties maintaining household tasks or meeting personal needs.
Some participants also described changes in their masking strategies: For some, masking became increasingly exhausting and at times impossible to sustain, while others intensified masking during depression to avoid drawing concern or to protect themselves in social interactions (i.e., stigma). Although masking may superficially appear to preserve social functioning, the sustained cognitive and emotional effort required often depleted resources needed for other daily activities, thereby contributing to overall functional decline.
Specifier: Anxious distress and Anxiety-Related features
Approximately one-quarter of participants (25%) described anxiety-related experiences during depressive episodes, including persistent worry, physiological arousal, panic, and intrusive thoughts. These accounts align in part with the DSM-5-TR “anxious distress” specifier, which includes symptoms such as feeling tense, unusually restless, or fearing something awful might happen. Participants reported feeling on edge, easily startled, and in a heightened state of alertness. Some described intense emotional spirals, catastrophic thinking, and a constant sense of impending threat, often accompanied by physical symptoms such as increased heart rate, nausea, and sweating. Functional impacts included disrupted sleep, agitation, and social withdrawal. Several participants noted difficulty distinguishing between anxiety and depression, or reported that their typical anxiety patterns became more intense or harder to manage during depressive episodes. Others described ruminative looping or hypervigilance that contributed to emotional exhaustion, distrust of others, and distorted self-perception. While some of these features may reflect co-occurring anxiety disorders, participants generally framed them as embedded within their depression.
Non-DSM-5-TR potential indicators of depression report experiences
Participants described experiences of depression that included depression-related changes in autistic characteristics, as well as behavioral and affective features not addressed within DSM-5-TR criteria. Table 4 provides an overview of each category, including descriptions and selected quotes.
Non-DSM-5-TR Additional Depression Indicators
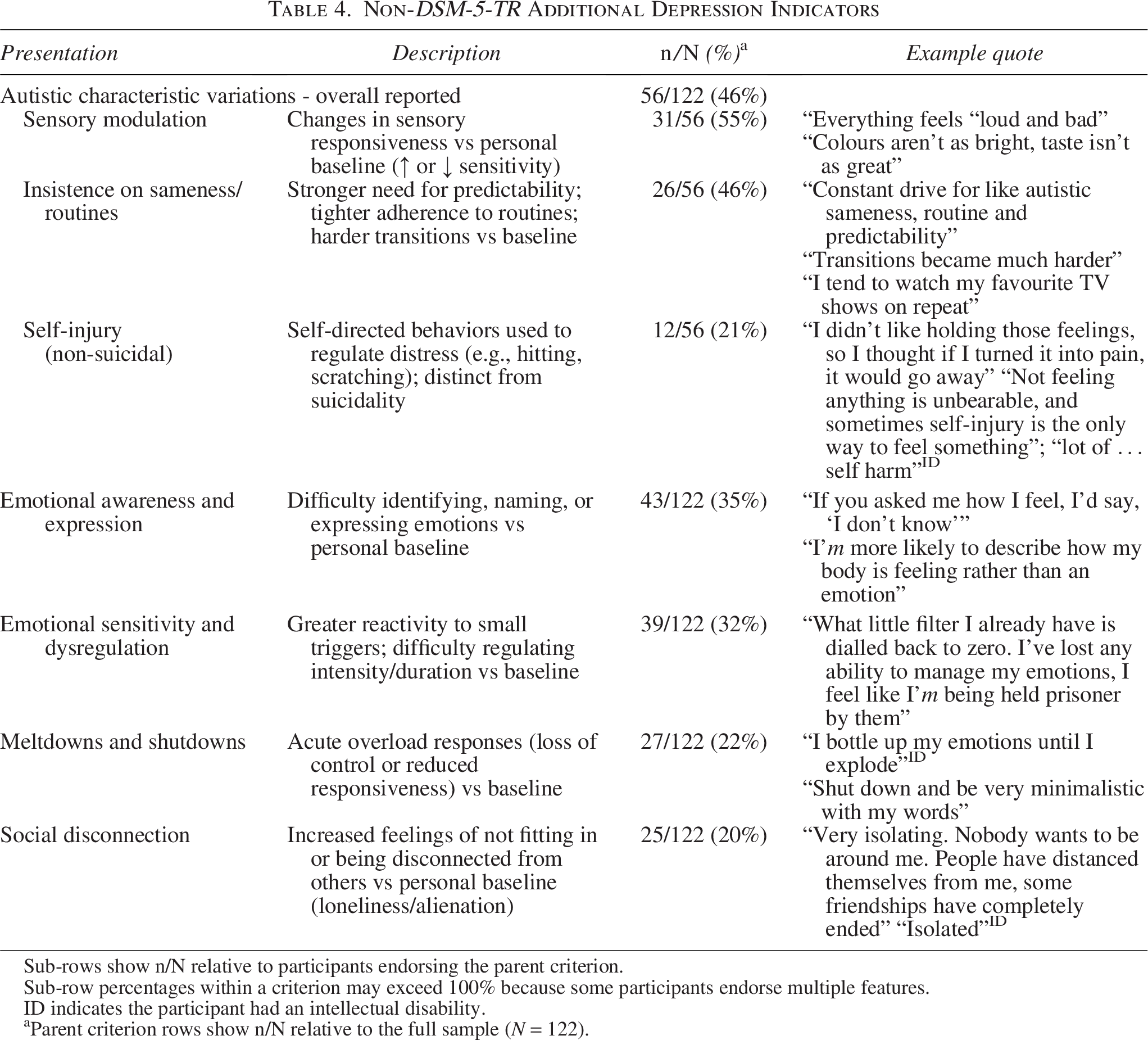
Sub-rows show n/N relative to participants endorsing the parent criterion.
Sub-row percentages within a criterion may exceed 100% because some participants endorse multiple features.
ID indicates the participant had an intellectual disability.
aParent criterion rows show n/N relative to the full sample (N = 122).
Depression-Related changes in the expression of autistic characteristics
Participants (46%) described depression-related shifts in how they experienced and expressed their autistic characteristics during depressive episodes, particularly in sensory sensitivities and repetitive behaviors. Sensory changes included increased sensitivity (hypersensitivity), where sounds, lights, or textures became overwhelming, and/or decreased sensitivity (hyposensitivity), where sensory experiences felt dulled, such as colors appearing less vibrant and tastes less pronounced. These sensory shifts were described as altering how participants connected with their physical environment, sometimes contributing to a sense of detachment.
Depression-related changes in repetitive behaviors included a heightened focus on predictability and control, with participants intensifying engagement in familiar routines and repetitive activities, such as repeatedly watching familiar TV shows, maintaining strict food preferences, and stimming more frequently to process emotions and create stability. Some also described experiencing reduced cognitive flexibility, including increased rumination and difficulty shifting away from distressing thoughts. Difficulty with transitions and stronger adherence to plans or routines were also reported. Participants also described engaging in self-injurious behaviors (SIBs), including cutting, skin-picking, or tattooing, as a coping mechanism for emotional numbness or distress. While SIB is not a characteristic of autism, some participants noted patterned, ritualistic elements to these behaviors that were often repeated during each depressive episode. They described SIB as a regulatory strategy that provided temporary relief through sensory input and emotional release, helping them process feelings of being overwhelmed or reconnect with their physical sensations.
Behavioral
Participants described depression-related behavioral changes such as increased meltdowns and shutdowns. Meltdowns were characterized as episodes of intense emotional vulnerability, often triggered by seemingly minor events when stress was already heightened. Shutdowns involved complete withdrawal, sometimes becoming non-verbal or experiencing a reduced ability to communicate, as participants attempted to cope with sensory overload or emotional overwhelm.
Affective
Participants described three depression-related affective shifts: increased emotional sensitivity, reduced emotional awareness, and social disconnection. Increased emotional sensitivity was characterized by reduced tolerance for interpersonal input and demands, with minor interactions triggering heightened tension and emotional dysregulation. Participants also reported increased sensitivity to others’ emotions, which intensified distress and made emotional stability harder to maintain. Reduced emotional awareness was described as a marked change in the ability to identify and articulate emotions, with some participants portraying depression as feeling lost, confused, or scared. Others described a sense of bodily disconnection, including physical numbness or muted physical sensations, which they experienced not as a primary sensory change, but as part of feeling emotionally detached from themselves. Participants often sensed changes within themselves but struggled to interpret or express them, with some only recognizing these changes when pointed out by others.
Social disconnection reflected a perceived inability to form meaningful connections despite wanting social support. This differed from social withdrawal, as participants actively sought connection but often felt misunderstood, alienated, or disconnected. This contributed to relational strain, including disrupted friendships, tense family relationships, and an intensified sense of isolation. Some reported feeling lonely even when physically around others, compounding the impact of depression.
Discussion
We examined how autistic adults described depressive symptoms, mapping these to DSM-5-TR criteria. While core symptoms often aligned with DSM-5-TR symptom definitions, participants also identified distinct indicators, including two provisionally termed constructs, “autistic anhedonia” and “depression attacks”, and described depressed mood more often as anger or irritability and emotional numbness than as sadness. Additional indicators of depression included heightened emotional sensitivity, reduced emotional awareness, SIB, masking and alterations in autistic characteristics that could obscure or mimic mood-related change. Qualitative research on anxiety and PTSD in autistic adults has likewise reported patterns of both overlap with diagnostic frameworks and additional autism-related presentations.15–17 Therefore, although core depressive presentation appears similar across autistic and non-autistic adults, understanding how symptoms are experienced, expressed and communicated in the context of autistic characteristics, and interpreting them alongside DSM-5-TR criteria, is essential to avoid missed or inaccurate diagnosis.
Variations in symptom presentations aligned with DSM-5-TR
While most participants described symptoms consistent with DSM-5-TR criteria for depressed mood, their affective presentations often diverged from patterns reported in non-autistic populations. 52 Anger, irritability, and emotional numbness were more often reported than sadness or crying, contrasting with qualitative reviews of depression in non-autistic adults, where sadness predominates. 52 Under the 2022 DSM-5-TR update, anger and irritability are now recognized as diagnostic indicators in adults, yet little research has examined their presentation in autistic populations. Such symptoms may instead be misattributed to individual disposition or emotional dysregulation, rather than potential markers of mood disturbance. Notably, in this study, anger and irritability were often described alongside somatic complaints, suggesting a possible combined presentation that warrants closer clinical attention. Sensory processing differences represent another potential mechanism: heightened sensitivity has been linked to greater anger and aggression risk, 53 whereas blunted responses under high stress may manifest as emotional numbness. 54 The prominence of anger and irritability highlights their clinical importance, both as autistic manifestations of depressed mood and in relation to depressive severity and suicide risk.55–57
Participants described anhedonia, an affective symptom reflecting diminished capacity to experience pleasure, in ways consistent with and divergent from DSM-5-TR criteria. One autism-related presentation, here referred to descriptively as autistic anhedonia, involved a loss of emotional reward from highly focused, identity-defining interests that ordinarily support mastery, emotion regulation and well-being. 44 Unlike DSM-defined anhedonia, 9 these activities were often maintained despite diminished enjoyment, driven by predictability and self-regulation, which may obscure the loss of pleasure from close others and mental health practitioners, increasing the risk of under-recognition. When changes in engagement with deep or focused interests occur alongside other depressive features and functional decline, they should be conceptualized within the same anhedonia construct that informs depression diagnoses in non-autistic adults, noting that the affected activities may be fewer in number yet central to identity. Supporting the clinical relevance of this pattern, recent research examining how psychologists assess depression in autistic adults found that changes in both the enjoyment and the focus of such interests were consistently identified as critical markers of a mood disturbance. 14
Some participants described what they termed depression attacks, acute episodes of overwhelming depressive affect characterized by sudden hopelessness, intense physiological distress, and, for many, suicidal ideation with increased urge to act. These episodes emerged abruptly and resolved quickly, resembling the rapid escalation seen in panic attacks or PTSD flashbacks, 9 but centering on depressive rather than fear-based affect. Participants described depression attacks as discrete affective crises rather than gradual mood decline, a distinction of clinical importance given the elevated suicide risk among autistic adults.58,59 This episodic presentation aligns partly with DSM-5-TR Criterion A9 (suicidality), yet may be missed or underrepresented on standard depression measures that ask about persistent symptoms over days or weeks and frame suicidal ideation in general rather than episodic terms (e.g., Patient Health Questionnaire-9 [PHQ-9], Beck Depression Inventory-II [BDI-II]).60,61 Frequency-based items should therefore supplement them with questions about sudden, short-lived spikes in suicidal thinking or urges without clear triggers, as these crises may not be captured in routine screening. Psychologists assessing autistic adults for depression have noted depression attacks as clinically meaningful, yet underrecognised, 14 highlighting the need for research on how best to identify and respond to these episodes.
Additional indicators of depression in autistic adults
Alongside DSM-5-TR symptoms, participants described additional indicators of depression, such as meltdowns, shutdowns, heightened emotional sensitivity, SIB, and variations in autistic characteristics. These features are clinically important because they can co-occur with depressive episodes in autistic people and may complicate recognition when they overlap with, mimic, or are misattributed to baseline autistic presentation, contributing to diagnostic overshadowing and delayed recognition.8,12,29 The temporal relation between these features and depression severity remains uncertain: they may precede, accompany or follow mood disturbance, and early changes are easily missed, particularly when mood shift is subtle or masked. Masking itself may also lead to diagnostic overshadowing or delayed recognition, since camouflaging can conceal affective disturbance and perpetuate low mood while appearing outwardly adaptive.34,62 Clarifying this relationship is crucial for guiding accurate clinical recognition and timely intervention. In the meantime, monitoring these features alongside DSM-5-TR symptoms may support earlier detection and reduce the likelihood that depression in autistic adults is recognized only once symptoms have become acute.
Depression was described as altering autistic cognitive–behavioral styles, with participants reporting stronger reliance on sameness, routine, and environmental control to manage internal distress and reduce sensory or situational demands. These strategies often served an immediate regulatory function but could also constrain engagement in restorative activities or reinforce avoidance,27,63,64 potentially sustaining low mood. For some participants, SIB were also described as serving a regulatory role by providing sensory input or emotional release during depressive episodes. Both these cognitive–behavioral patterns 64 and SIB65,66 reflect attempts to manage distress, yet they may also limit coping flexibility and contribute to ruminative cycles. 66 Importantly, such regulatory strategies are also observed in anxiety,31,67 which commonly co-occurs with depression in autistic adults. 1 This overlap complicates clinical interpretation, as behaviors may reflect regulatory coping, depressive processes, or anxiety-related mechanisms. Clinically, these findings emphasize the importance of assessment approaches that explore the reasons for behaviors, rather than relying solely on their presence or severity, to distinguish mood-related features from autistic characteristics or co-occurring conditions.
Some participants described their depressive experiences as involving reduced affective clarity, making it more difficult to recognize and articulate emotions compared with their usual state. Difficulties in emotion awareness are often linked to alexithymia, which, while typically considered a trait, 68 may intensify during depressive states, 69 potentially amplifying the challenges participants described. Interoceptive differences commonly reported by autistic people may also contribute by limiting awareness of gradual internal changes, producing the impression of abrupt, high-intensity shifts once emotions reach a threshold.47,70 It is possible that, in combination with broader emotional processing differences experienced by autistic people,13,71 these mechanisms contribute to the sudden, high-intensity expressions participants described, including meltdowns, shutdowns, and heightened sensitivity. Therefore, practitioners should actively assess and monitor emotion awareness and regulation alongside other depressive indicators, as this may help reduce delays in recognizing depression and providing timely support.
Relational stress, experiences of rejection, and stigma surrounding both autism and depression may have cumulative effects, contributing to feelings of worthlessness and guilt. While social disconnection is a recognized feature of depression, 52 for autistic adults, it may also reflect the cumulative impact of chronic exclusion and unmet mental health needs.11,72 Participants’ accounts suggested that masking was sometimes used to manage relational stress. Although masking may provide short-term protection,26,41 it may also increase the risk of obscuring depressive symptoms when practitioners misinterpret it as a baseline autistic presentation. Masking depression alongside autistic characteristics can therefore conceal significant distress. Recognition requires probing beyond surface presentation and creating environments where autistic adults feel safe enough to reduce masking. Creating such therapeutic contexts may, in turn, enable autistic adults to unmask, which may support more accurate identification of depressive symptoms and guide the use of adapted assessment approaches, consistent with recent evidence highlighting the importance of safe and supportive therapeutic environments for autistic adults.11,73
Limitations, strengths and future research
Strengths
This study demonstrates several strengths that enhance the credibility and applicability of its findings. We included both self-identified and formally diagnosed autistic adults, enabling examination of depression presentations across a range of lived experiences and increasing ecological validity. 74 Limited caregiver participation nonetheless provided valuable additional perspectives and supported triangulation of findings. 75 We employed a rigorous direct content analysis, 39 using coding frameworks adapted to account for autism-related factors when interpreting depression presentations. This approach, informed by prior autism research and co-developed with autistic advisors, ensured alignment with neurodiversity affirming principles.
Limitations and future research
Several limitations should be considered when interpreting these findings. The self-selected sample may not reflect the full heterogeneity of the autistic population, particularly in terms of gender diversity, age, socioeconomic status, co-occurring conditions, and cultural backgrounds. Underrepresentation of autistic adults with intellectual disability and non-speaking individuals further restricts insight into how different communication modes and support needs influence the experience and recognition of depression. 76 While most participants (80%) were experiencing or recovering from depression, which may have influenced recall, evidence indicates that discussing distressing experiences can temporarily increase negative mood and stress. 77 The absence of formal clinical confirmation of depression prevents assuming alignment with verified diagnoses; however, this approach prioritized lived experience and reduced participation barriers.
Future research should investigate how autistic characteristics and associated features, such as alexithymia, sensory differences, interoceptive processing, and co-occurring attention-deficit/hyperactivity disorder, influence depression presentations. Studies should also include greater representation of autistic adults with intellectual disability, non-speaking individuals, and those from culturally diverse backgrounds. Several recent guidance documents outline principles for conducting inclusive research with these groups, emphasizing accessible formats, co-design, and flexibility.78–80 Integrating perspectives from caregivers and practitioners alongside autistic adults would enhance understanding of how depression is recognized across contexts. Finally, co-designed, autism-informed assessment tools that incorporate these influences hold potential to improve diagnostic accuracy and clinical decision-making.
Clinical implications
While autistic adults may experience depression symptoms consistent with DSM-5-TR criteria, the form, prominence, and expression of these symptoms can differ. Our findings suggest that practitioners can build on their existing skills in assessing depression by carefully interpreting autistic adults’ descriptions of mood, motivation and functioning in relation to DSM-5-TR depressive symptom domains, while considering autistic communication styles, sensory experiences, emotional processing, and interests. This interpretive work typically requires specific training and experience in autism-informed mental health assessment, consistent with practice standards for psychologists in some countries, such as Australia, that require the ability to adapt practice to support people with developmental disabilities. 81
Maintaining daily routines or interests should not be assumed to indicate psychological well-being, as flat or calm affect and continued engagement, including loss of enjoyment in usual interests, may mask distress. Screening should therefore include direct questions about changes in sensory tolerance, routines, engagement in core interests, and less typical affective displays. Given that autistic adults in this study more often described depressed mood as anger, irritability or emotional numbness than as sadness, practitioners should regard new or intensified anger and irritability, particularly when accompanied by somatic complaints, withdrawal or reduced functioning, as potential markers of depression.
Practitioners should also assess for co-occurring anxiety, given its high overlap and bidirectional relationship with depression in autistic adults, and distinguish anxiety-driven distress from depressive symptoms when planning support. 17 SIB warrants active monitoring for suicide risk, especially in autistic adults with intellectual disability. Assessment should also include screening for alexithymia and interoceptive differences, as these may reduce an individual’s ability to recognize internal states and obscure the onset of depression. Reviewing responses to depression measures at the item level, rather than relying solely on total scores, and incorporating observations from caregivers or others who know the person well, can further improve diagnostic accuracy.
Because autistic cognitive, sensory and communication characteristics may influence how autistic adults experience and describe depressive symptoms, they may also influence how autistic adults respond to screening items, even when the underlying symptom is present. For example, depressed mood items may be under-endorsed when low mood is experienced as anger, irritability or emotional numbness, and if anhedonia items are not endorsed, practitioners can ask whether enjoyment, drive or sustained engagement in deep interests has reduced compared with the person’s usual baseline. As such, we recommend supplementing standard screens with a small number of follow-up questions that probe baseline changes in interests, routines, social connections, mood or affect, and somatic experiences.
When interpreting somatic items such as sleep, appetite and energy, practitioners should use follow-up questions to clarify how recent changes compare with the person’s usual autistic baseline, including any pre-existing sleep or health conditions. For example, fatigue may be reported as physical heaviness rather than tiredness. Creating supportive contexts where autistic adults feel safe to reduce masking may also help reveal mood changes otherwise hidden. Embedding these considerations into practice can enhance recognition and provide timely, individualized, and practical support for depression in autistic adults. Developing autism-informed clinical guidelines for recognizing and diagnosing depression is a critical next step to ensure that practitioners can apply these considerations in practice, explicitly linking autistic adults’ descriptions and behaviors back to familiar DSM-5-TR depressive constructs to minimize diagnostic overshadowing and practitioner uncertainty.
Authors’ Contributions
Conceptualization, data curation, methodology, formal analysis, writing—original draft preparation, writing—review and editing, project administration, E.H. Conceptualization, writing—review and editing, supervision, D.A, N.D. and J.P.
Footnotes
Acknowledgments
The authors acknowledge Dr. Rachelle Wicks for sharing her experience and expertise during the study design and analysis of this project.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
This work was supported by the Australian Government Research Training Program (RTP) Stipend Scholarship.
Institutional Review Board Statement
This study was approved by the Human Research Ethics Committee of Griffith University (2023/725).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Permission to share demographic data from this study was obtained during the ethical approval process.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.