
Abstract
Background:
Growing numbers of adults are being diagnosed as autistic or having ADHD later in life, leading to a range of emotional responses and queries around identity. This review explores the process of identity reconstruction in late-diagnosed autistic and ADHD adults, examining both shared and distinct aspects of identity in each group, to better understand how diagnosis affects self-perception and to guide future post-diagnostic support.
Methods:
Following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Joanna Briggs Institute (JBI) guidelines, we entered search terms relevant to autism, ADHD, delayed diagnosis, and identity into multiple databases. After screening titles and abstracts, two raters reviewed full-text articles to determine their inclusion with substantial inter-rater reliability. We extracted and coded qualitative data, with themes identified through thematic analysis.
Results:
The search strategy identified a total of 6894 articles, of which 5470 were duplicates. Reviewers screened 1423 articles. A final set of 25 articles was identified, with 12 articles exploring ADHD diagnoses and 13 articles exploring autism diagnoses. Our thematic analysis of the articles suggests that individuals experience a profound reevaluation of their identity following diagnosis in adulthood. Three overarching themes were identified, reflecting experiences shared across autism and ADHD, as well as distinctions unique to each condition: 1. Reconfiguring the self; 2. Finding the self through others; and 3. Emotional integration of the self. Participants grappled with confusion, reinterpretation of past experiences, and developed a more authentic sense of self, a process that was facilitated through finding belonging among neurodivergent peers. Emotionally, this process required navigating grief, internalized stigma, and negative self-perceptions. Diagnosis was transformative, offering validation and empowerment to participants. Overall, the process of diagnosis appears to foster growth toward a more integrated identity.
Conclusions:
Findings from this review highlight both shared and condition-specific impacts on identity, highlighting a need for post-diagnostic support that acknowledges the identity-related impacts of diagnosis in both autism and ADHD. Current evidence largely reflects majority populations, highlighting a gap in understanding of how underserved groups, such as ethnic minorities, experience and negotiate identity after diagnosis. Clinicians should be aware of the need for community connection, self-acceptance, and informed decision-making about disclosure, and provide affirming, tailored care following diagnosis.
Community Brief
Why is this an important issue?
There is a rising increase in adults being diagnosed with autism or ADHD later in life, especially those from marginalized or underrepresented groups. Receiving a diagnosis as an adult can be both a relief and a challenge. It often leads people to rethink who they are, how they understand their past, and how they see their future. This process can be complex and emotional, with a huge impact on well-being. Learning more about this experience helps families, professionals, and communities better support those who receive a late diagnosis.
What is the purpose of the review?
We reviewed published studies to find all the available studies that may have looked into the process of identity changes in people who have been diagnosed as autistic or ADHD in adulthood. We wanted to understand how the diagnosis changes the way people see themselves and to identify what kind of support might help them after diagnosis.
What did the authors do to review the literature?
We designed a search method to find all the articles that discussed identity in adults following clinical autism and ADHD diagnoses. We searched multiple academic databases and the reference lists of the articles that were included in the review.
What studies did the authors find?
Through a screening process, we found 25 sources about Autistic and ADHD experiences of identity following adulthood diagnosis. Twelve of these sources focused on the experiences of autistic individuals, and 13 of these focused on the experiences of ADHD individuals. We then did a thematic synthesis to describe key themes within the texts.
In summary, what did those studies show?
We found three overarching themes from the included literature as follows: Reconfiguring the self, Finding the self through others, and Emotional processing of the self. We found that after being diagnosed, people often rethought who they were, which was a complex process of making sense of past experiences and learning to accept themselves in a new way. Some found relief, but others felt uncertain or overwhelmed. Many described a mix of emotions, including grief, frustration, and empowerment. The diagnosis affected how people felt about their place in the world. Some felt more connected after finding communities, but many still struggled with feeling different or misunderstood. Deciding whether to tell others about their diagnosis was a complex process.
What are the remaining gaps in the literature?
The limited diversity of people in the included studies may influence the way we understand identity development in late-diagnosed autistic and ADHD adults and reduce how broadly these findings can be applied. More research is needed to explore how factors like cultural background, formal vs. self-diagnosis, and personal views on diagnosis shape identity. It is also important to include people from more marginalized and underrepresented groups, as autism and ADHD are still underdiagnosed in these communities, and they are therefore more likely to experience late diagnosis. Long-term studies are also needed to better understand how identity changes over time and how support needs may shift.
Based on this review, what do the authors recommend?
We hope our review can lead to the development of better support for autistic and ADHD people in the time following their clinical diagnosis in adulthood. This support should be informed by research and consider the process of identity development from an intersectional lens. Future research and development of supports should be centered around the views and needs of the autistic and ADHD communities so they can improve the lives of people who are diagnosed in adulthood.
Autism and ADHD are lifelong neurodevelopmental conditions that shape adult identity in ways that impact well-being, resilience, and inclusion. Autism involves differences in social communication, repetitive behaviors, and sensory sensitivities, whereas ADHD is defined by inattention, hyperactivity, and impulsivity. 1 Although distinct, both conditions share overlapping characteristics, 2 and previous research has noted co-occurrence.3,4 Considering both conditions together provides an opportunity to explore patterns that may be shared or distinct. Research increasingly recognizes both conditions not only for the challenges they present—such as underemployment, mental ill-health, and accessibility issues5–7—but also their strengths, including passionate interests and creative thinking styles. 8 Recent qualitative research highlights notable similarities in the experiences of identity between autism and ADHD in late-diagnosed adults. 9 This review examines identity development and its link to well-being in late-diagnosed autistic and/or ADHD adults. Considering both conditions concurrently enables a nuanced understanding of their shared and distinct identity experiences, particularly given the high co-occurrence of ADHD in autistic individuals. 10 This informs more inclusive frameworks that acknowledge the complexity of co-occurring neurodivergence. Here, we synthesize qualitative and quantitative findings from the past decade to identify key factors influencing the formation of neurodivergent identity 1 formation.
Changes in diagnostic criteria, increased awareness, co-occurring diagnoses, and accumulation of diagnostic labels over time have contributed to the emergence of an “undiagnosed” generation of adults now receiving diagnoses in adulthood.5,11–13 Late diagnosis is influenced by many contextual factors, including feature presentation (including a less obvious presentation or camouflaging), geography, healthcare access, and cultural norms. 14 Certain groups are less likely to be diagnosed in childhood than others, such as females who are likely to be referred 5 years later than males15–17 and ethnic minorities who are between 46% and 69% less likely to receive a diagnosis.18–20 In Western contexts such as the United Kingdom and United States, researchers have found higher rates of autism identification among children of mothers with greater wealth and higher education,21,22 suggesting lower socioeconomic groups face health inequities and are more often underdiagnosed. Similarly, children with access to health insurance and those from dual-income families are more likely to receive an ADHD diagnosis and treatment. 23 First Nations individuals from countries such as Canada and Australia also experience disparities in autism diagnoses and research representation,24,25 while disparities in ADHD are still understudied. These findings highlight systemic disparities and suggest individuals from disadvantaged or underrepresented groups often reach adulthood without identification or support, encountering a diagnostic process that is emotionally complex and often following years of unmet needs or misunderstanding.
Late-diagnosed individuals often experience a wide range of emotional responses to receiving their diagnosis. Some report feelings of relief and validation, while others experience shock, disappointment, or disbelief.26,27 Despite these mixed reactions, diagnosis in adulthood can have significant benefits, often triggering a process of self-reflection and narrative reconstruction26,28 that can lead to empowerment 29 and self-acceptance. 30 Developing a positive neurodivergent identity can contribute significantly to psychological well-being, including reduced levels of anxiety and depression.31,32 It can also foster unique thinking styles, openness to new experiences, and greater resilience. 33 However, barriers such as social stigma, communication difficulties,31,34 and past experiences of discrimination, bullying, or exclusion, can undermine the formation of a positive identity and lead to challenges with self-esteem.35,36 Understanding these social barriers is essential for interpreting how identity development and well-being are described across research in late-diagnosed autistic and ADHD adults.
Supportive factors—such as external validation, community belonging, and access to learning opportunities—can enhance identity formation.37,38 From a social identity perspective, neurodivergent individuals may experience autism and ADHD as minoritized identities, shaped by stigma, exclusion, and unequal access to support. Recognizing the intersection of neurodivergent identity with other marginalized or underserved identities can illuminate how cumulative social stressors influence identity development and well-being. Reframing these experiences through the social model of disability situates personal challenges within broader systemic barriers, promoting a shift from deficit-based perspectives to one emphasizing social inclusion and empowerment. 39
While this concept of identity has been explored in previous research, few studies have explored the similarity of experiences in autism and ADHD. Davies et al. 37 conducted a systematic review of quantitative research on autistic identity and found that positive autistic identity was associated with improved mental health and well-being, and identified a need for peer support and/or self-directed support services to cultivate positive autistic identity. A study from Porras Pyland et al. 40 found that specific groups—namely, black and male participants—were more likely to reject an ADHD identity. Furthermore, older age at diagnosis was associated with greater integration of ADHD into one’s self-concept. However, no studies have systematically examined the parallels in identity development between autism and ADHD, nor addressed the unique process of identity reconstruction that occurs following adult diagnosis.
We guide this review by applying the social model of disability. In the context of autism and ADHD, the social model of disability advocates for removing social obstacles by promoting positive language and shifting focus from deficits toward positive societal change, inclusive structures, and individual potential. 41 Rather than framing autism and ADHD as individual deficits, this review adopts a perspective that societal norms and environmental mismatches contribute to disadvantage. From this perspective, neurodivergence can be understood as a socially situated identity, shaped by patterns of recognition, marginalization, and access to supportive social contexts. Considering the medical processes of diagnosis, this review also considers a biopsychosocial perspective as reflected in the World Health Organization International Classification of Functioning, Disability and Health. This review is primarily guided by Social Identity Theory, 42 which posits that individuals maintain identity by affiliation with valued groups and social comparisons. For late-diagnosed autistic and ADHD adults, diagnosis can act as a gateway to group identification. This group-based perspective helps explain how social connections following diagnosis can shape self-perception and well-being.43,44 The selection of Social Identity Theory also reflects our team’s collective expertise and lived experience with neurodivergence, which informed our focus on identity as socially situated. We also consider other perspectives on identity, such as Narrative Identity Theory 45 and Minority Stress Theory, 46 in the Discussion to capture different dimensions of identity formation. These theoretical lenses are applied as a post hoc interpretation of the findings related to identity in late-diagnosed autistic and/or ADHD adults but are not used to guide the initial conceptualization or analytic framework of the review.
In underserved groups, such as LGBTQIA + community members 47 and culturally and linguistically diverse populations, 48 positive identity development can enhance well-being, while inadequate support can harm mental health. These findings highlight the importance of understanding identity formation in autistic and ADHD individuals, particularly as both conditions frequently co-occur 10 and share overlapping traits. 49 Despite this, research has largely examined autism and ADHD separately, and few studies have explored identity reconstruction following late diagnosis or compared experiences across populations. This review explores autism and ADHD identity concurrently. A comparative review is essential to guide inclusive post-diagnostic supports, inform policy, and identify priorities for future research. Our review aims to systematically synthesize research on the shared and distinct experiences of identity reconstruction in late-diagnosed autistic and/or ADHD adults, and identify factors that may facilitate or hinder positive identity reformation.
Methods
Search strategy
This systematic review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines 50 (see Supplementary Data) and the Joanna Briggs Institute 51 methodological framework. We created the protocol in June 2024 (CRD42024554473), amended it, and submitted it to PROSPERO in September 2024 (CRD42024588592), accessible via the PROSPERO website. We conducted searches in June 2024 across APA PsycINFO, PsycArticles, PubMed, Scopus, Web of Science, and ERIC, using refined terms for autism/ADHD*, late-diagnosis*, and identity* (full search terms in Supplementary Data). We only included peer-reviewed English-language studies, with no date restrictions. We required studies to examine identity from the perspective of adults formally diagnosed with autism or ADHD at age 18 or older, and to be published in English.
We excluded articles if they (1) were gray literature: that is, case reports, opinion pieces, and dissertations; (2) were systematic reviews or meta-analyses; and (3) if they included any participants diagnosed under the age of 18. We also excluded articles with mixed groups where data could not be split between adults and adolescents. The searches yielded 6894 articles. We manually searched the bibliographies of screened articles for additional articles, which yielded an additional 130 articles for screening.
Eligibility ratings
Two reviewers (P.M. and M.L.B.) screened all potential articles in a two-stage process. We first assessed titles and abstracts, including uncertain citations for full-text review. We obtained and read full texts and contacted four authors to request access. We resolved disagreements by team consensus, with moderate agreement for abstract screening (Cohen’s kappa = 0.60) and substantial agreement for full-text screening (Cohen’s kappa = 0.70). We included 25 articles in total.
Quality appraisal of included studies
We critically appraised studies for methodological quality using the Mixed Methods Appraisal Tool 52 (MMAT). P.M. appraised each study individually using the MMAT. We tracked appraisal results in a spreadsheet table (see Supplementary Data). A second reviewer (M.L.B.) appraised a proportion of studies (10%), achieving an inter-rater reliability of 100%. Previous reviews 53 have used similar proportions of multi-rater appraisal for rigor. We discussed disagreements and resolved them together. We did not use the MMAT to exclude studies but to provide insight into the methodological rigor of each study, which in turn informed the confidence in the synthesized findings of this review.
Data extraction and synthesis
P.M. independently extracted data from all included studies, and M.L.B. double-extracted a 10% subset, yielding 80% agreement. Data included first-order constructs (participant quotes) and second-order constructs (author interpretations) related to identity, enabling a grounded review of findings based on participants’ original experiences. 54 Where one article 55 was a modified Delphi study, the authors drew data from the fourth round, as earlier rounds focused on community involvement for survey development. Extracted information covered bibliographic details, study design and methodology, sample size and demographics, age at diagnosis and time since diagnosis, theoretical frameworks, results (quotes and interpretations), and limitations.
We synthesized data using a “thematic synthesis” approach, developed by Thomas and Harden 56 due to the qualitative nature of the majority of the studies. Where one study was quantitative, P.M. extracted data relevant to identity and then coded these into themes. A thematic synthesis approach is both integrative and interpretative, and therefore allowed us to align results across studies and conduct transparent analyses of the data.
The lead author (P.M.) initially read the data to develop familiarity with recurring topics and language. P.M. then coded the data. We initially coded first-order quotes and second-order interpretations independently, and we generated these codes inductively based on recurring concepts. Our team reviewed and refined the code together following the first iteration of codes. P.M. synthesized data, and the authors discussed codes across multiple iterations to consider how best to group them. Based on the research team feedback, we grouped codes into descriptive subthemes and overarching themes to describe the results.
Community involvement and author positionality
We conducted this review as part of a doctoral project without collaboration from independent members of the autism or ADHD communities. P.M. is a researcher and allied health professional with lived experience of self-identification and adulthood diagnosis of neurodevelopmental conditions. M.L.B. is a member of the neurodivergent community. B.P.J. is a cognitive psychology researcher who is Queer and has lived experience of sensory disability. A.S.R. is an educational and developmental psychologist and autism researcher. Our collective positionalities, as researchers, clinicians, and members of the neurodivergent community, informed the conceptualization of the review, including the selection of Social Identity Theory as the primary theoretical framework. Our understanding of identity as socially situated, shaped by marginalization and access to recognition, guided our focus on factors influencing identity formation following adulthood autism and ADHD diagnosis. Our positionalities strengthened and supported our approach to meaning-making during analysis. This aligns with qualitative research that recognizes the value of positionality and reflexivity in interpreting lived experience.
Results
Overview of included studies
The searches generated 6894 studies, of which 5740 were duplicates. We screened the remaining 1423 studies and excluded 1375 studies at this stage. We conducted full-text reviews on the remaining 48 studies, and excluded 23 for being (A) gray literature, (B) lack of diagnoses in adulthood, (C) no results pertaining to autistic/ADHD identity, and (D) no access. For the study with no access, we emailed the author, but we received no response and excluded the article. In total, we included 25 studies in the review (Fig. 1), with 12 studies focusing on ADHD diagnoses and 13 focusing on autism diagnoses. We found no studies that explored the experiences of dual diagnosis. We found that most studies met the MMAT criteria, with only a small number lacking a clear research question or representative themes.
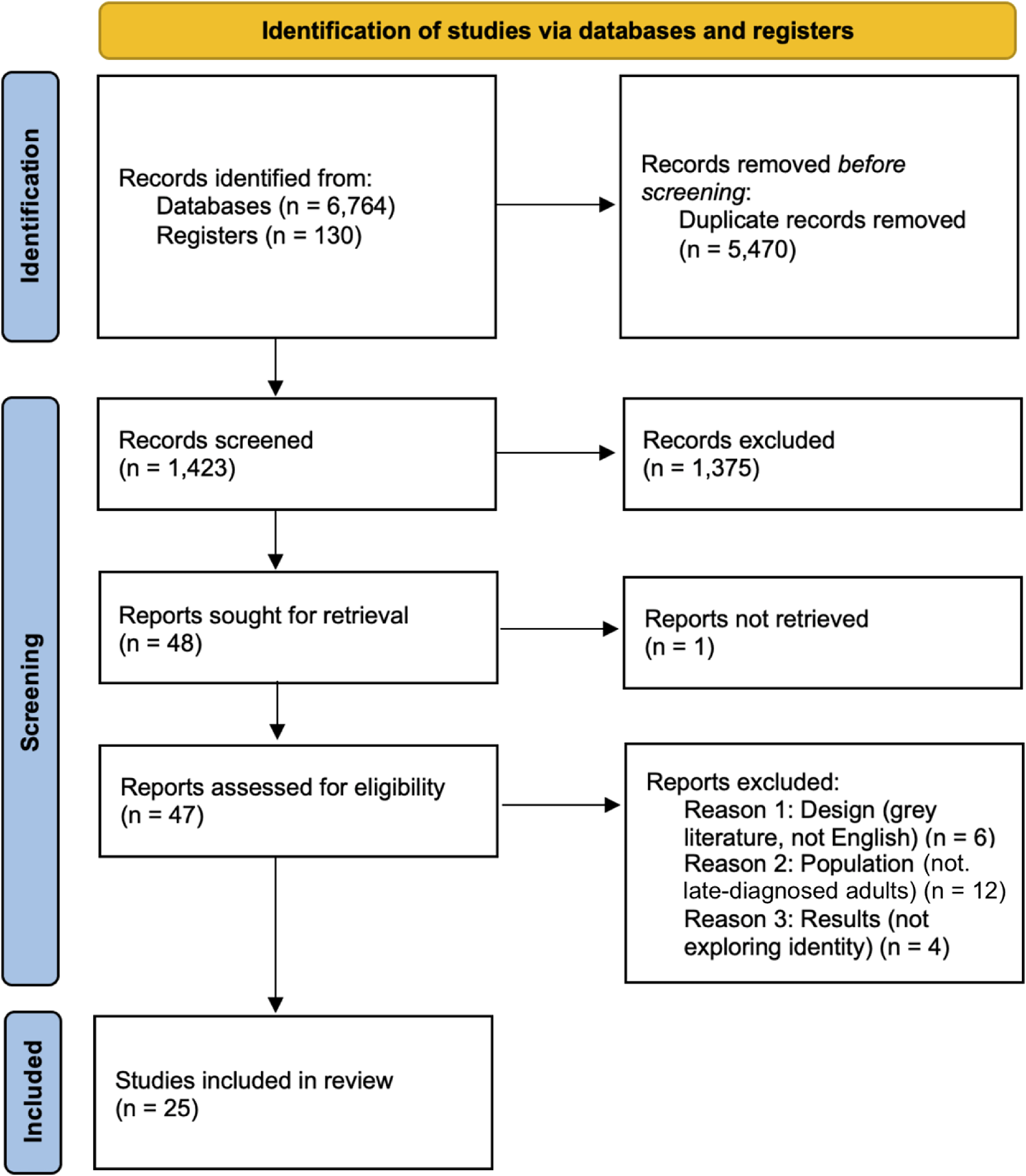
Article screening and inclusion using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 28
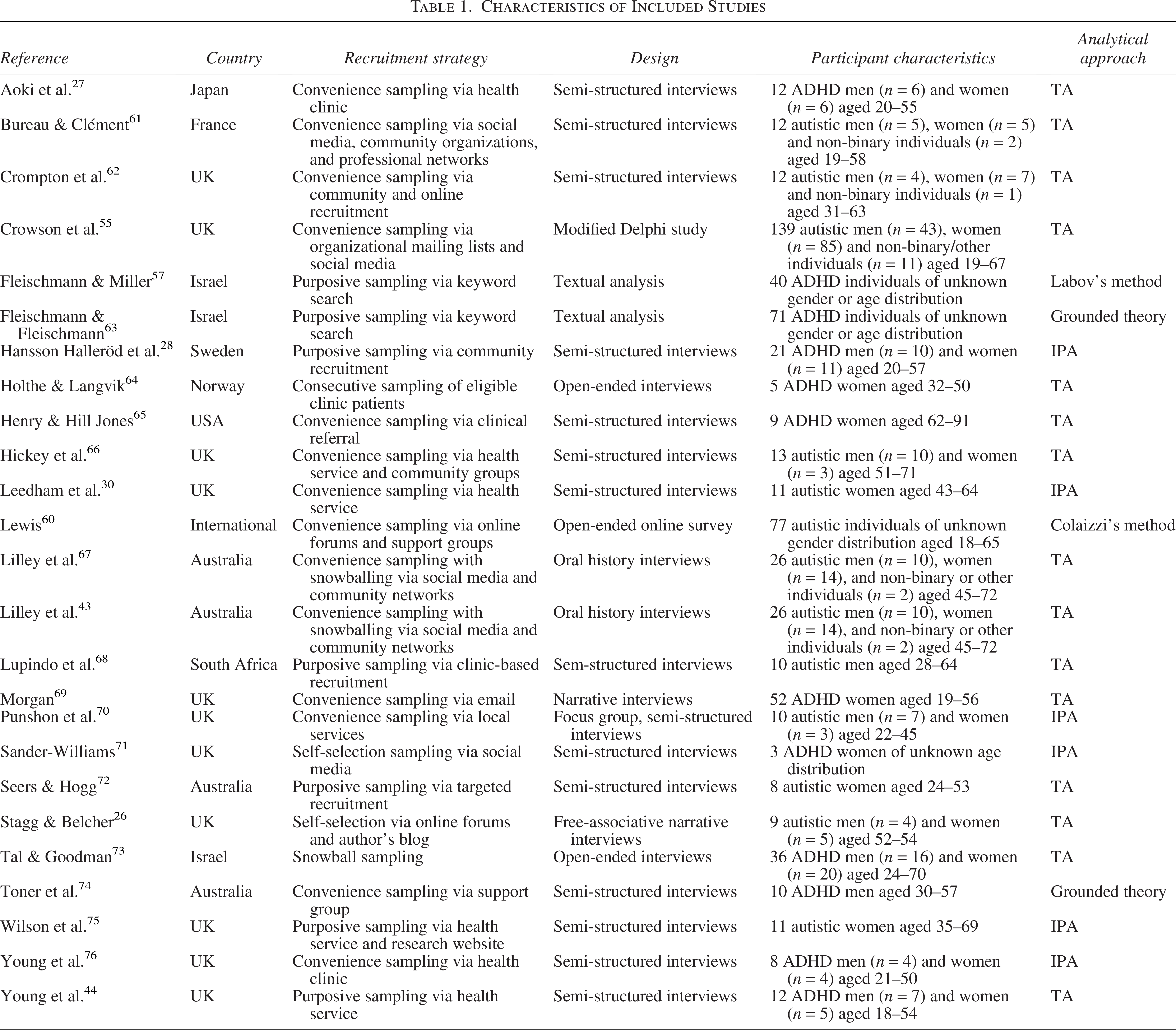
Among the included studies, only one 55 employed a longitudinal design using a modified Delphi approach, while the remainder were cross-sectional and qualitative in nature. Most relied on interviews, with a single study incorporating surveys. 55 Although the dominant analytic strategy was thematic synthesis (TA; 15 studies), there was some methodological diversity as two studies used grounded theory, and several adopted phenomenological approaches such as Interpretative Phenomenological Analysis (IPA) and Colaizzi’s method. One study drew on Labov’s narrative method, 57 which analyzes the structure of personal stories within verbal monologues.58,59 The majority of studies were conducted in Western countries, and one study was conducted with an internationally based participant group. 60 Further study characteristics are displayed in Table 1.
Characteristics of Included Studies
Limitations
Studies reported a range of limitations. The most common issues were with sample characteristics, such as small sample sizes (56%) and homogeneity within samples (85%). Methodological challenges were also noted, including recruitment bias (28%), reliance on qualitative approaches (32%), and absence of diagnostic verification (16%). Other limitations related to study design, such as variation in time since diagnosis (20%), lack of longitudinal data (16%), and recall bias (20%). A smaller proportion highlighted the absence of participatory methods (8%), and 12% of studies did not explicitly acknowledge any limitations.
Participant characteristics
The included studies involved 643 neurodivergent participants, with 13 studies on late autism diagnosis (n = 364) and 12 on late ADHD diagnosis (n = 279). Recruitment strategies varied, with the majority being convenience sampling (56%). Ages ranged from 18 to 69, and 62% were female (male = 34.44%, non-binary = 0.04%). Of 371 participants whose ethnicity was reported, 56 (15.09%) identified as non-White. No studies detailed sexual orientation, although one recorded LGBTQ+ status. 55 Education levels, reported variably, were grouped as “some secondary,” “secondary,” “higher education,” and “postgraduate education” by the authors of the present study. One study described participants’ socioeconomic status as “middle-class.” 68 Ten studies reported age at diagnosis, ranging from 18 to 69 (median of reported means = 41.23), and eight reported time since diagnosis, ranging from 0 to 20 years (median of reported means = 2.89). Full participant characteristics are available in the Supplementary Data.
Synthesis
Table 2 displays the superordinate themes and subthemes of the present review.
Overarching Themes and Subthemes and Their Frequency in Autistic and ADHD Populations
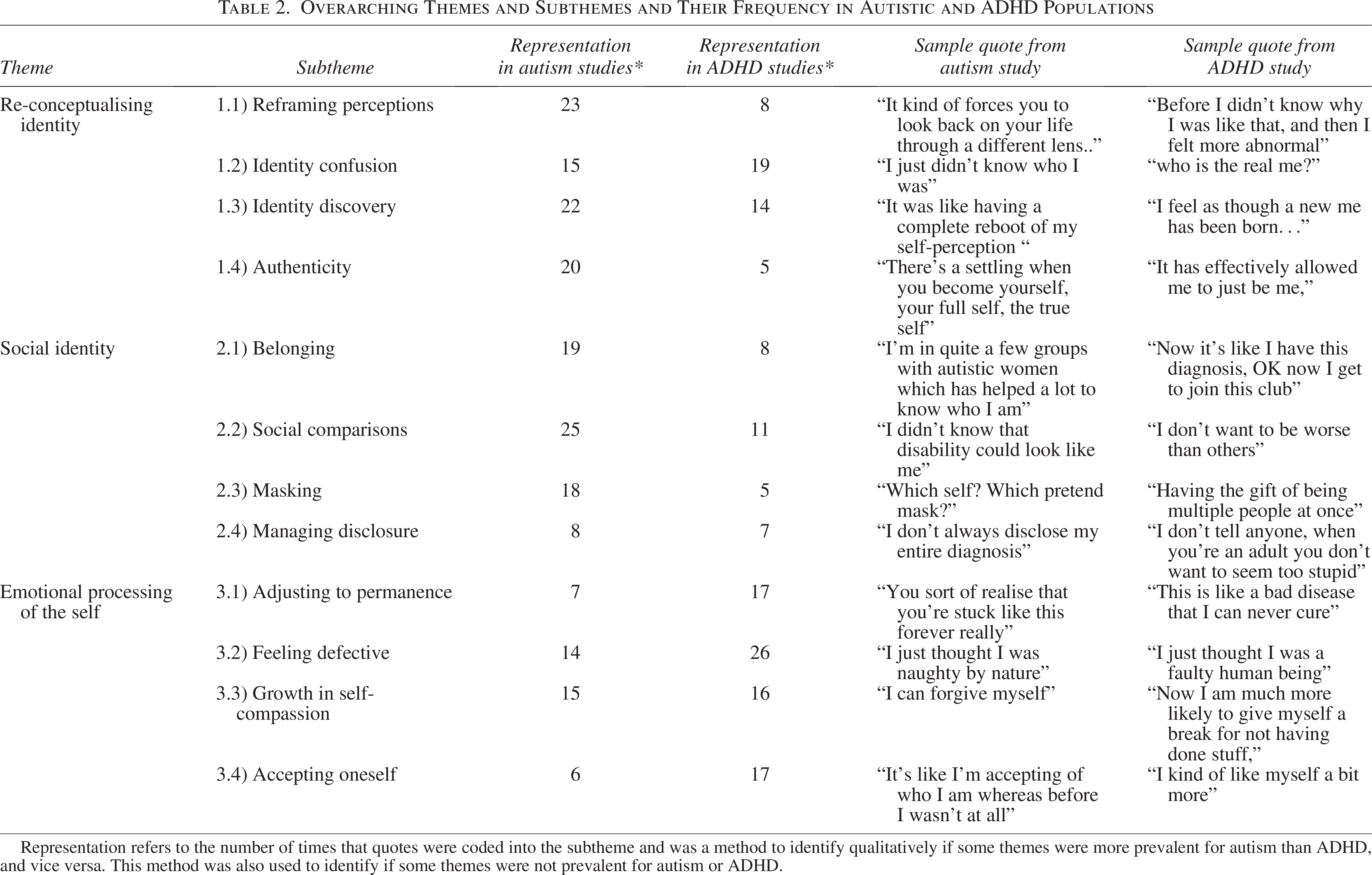
*Note. Representation refers to the number of times that quotes were coded into the subtheme and was a method to identify qualitatively if some themes were more prevalent for autism than ADHD, and vice versa. This method was also used to identify if some themes were not prevalent for autism or ADHD.
Theme 1: Reconfiguring the Self
The overarching theme of Reconfiguring the Self consisted of four subthemes: 1.1 Reframing perceptions; 1.2 Identity confusion; 1.3 Identity discovery; and 1.4 Authenticity. Across multiple studies, many participants described an ongoing cognitive meaning-making process in which they reconciled, redefined, and realigned their sense of self in light of their diagnosis. This process involved navigating confusion, uncertainty, reinterpretation, and ultimately progressing toward a more authentic and integrated self-understanding.
Across six studies of 136 autistic and 21 ADHD participants, participants reported reinterpreting their self-concept, past experiences, and perceiving differences through the lens of their diagnosis (1.1 Reframing perceptions). The diagnosis prompted a retrospective reevaluation. As one participant described, diagnosis “forces you to look back on your life through a different lens,” 62 prompting reflection and reinterpretation of prior experiences. This reframing contributed to greater self-acceptance. This encompassed participant reports they had always known they were “different” from others but now had an answer as to what this difference was, with one stating, “I finally knew that I was not alone who felt different.” 60 For some participants, the diagnosis enabled a shift from feelings of failure and shame toward self-understanding and compassion. Across studies, many participants stated that the diagnosis was pivotal in making sense of their identity, saying “I know who I am now,” 30 and eventually led to self-acceptance.
Although many participants described feelings of relief or validation through reinterpreting their self-concept, nine studies of 170 autistic and 36 ADHD participants reported that participants experienced uncertainty, doubt, and disorientation while integrating the diagnosis into their self-concept (1.2 Identity confusion). Some autistic individuals described a longstanding lack of identity clarity. In one study, a participant described this experience as “not understanding the ‘why’ of myself.” 60 Following diagnosis, several autistic participants questioned the reasons behind their diagnosis, experiencing emotions such as anger and confusion. Another question commonly reported in studies was “who is the real me?” 44 with participants struggling to understand how their diagnosis shaped their true self in the pursuit of deeper self-understanding and identity. Several studies found that some autistic and ADHD individuals struggled to understand how their diagnosis shaped their identity and behavior. This was framed by questions of “how much of me is ADHD…” 28 and “… am I just anything other than these symptoms?” 30 In some studies, researchers noted participants experienced doubt about the legitimacy of their diagnosis, questioning whether they were “… making this up.”43,71 They also described an “identity problem,” 44 struggling to integrate the new diagnosis into their existing sense of self, which created tension between past and present identities.
In nine studies of 46 autistic and 201 ADHD participants, authors described a transformative postdiagnosis journey in which some participants explored, redefined, and deepened their self-understanding (1.3 Identity discovery). It was reported in both autistic and ADHD participants that, for many, their diagnosis sparked new insights into who they were, enabling them to make sense of their identity. Studies described participants engaging in self-reflection, through which they gained insight that fostered self-acceptance, increased confidence, and a greater appreciation of both their challenges and strengths. In some studies, participants began defining themselves by their diagnosis, noting that the more they learned about their condition, the more they felt it defined them. Several studies reported shifts in identity, with certain participants describing a ‘new’ version of themselves. This was also accompanied by some confusion, as one participant noted, “Do I have to start all over again or will I become someone else now?” 28 A number of studies identified a need for professional support in helping individuals develop a more positive post-diagnostic identity.
Nine included studies of 78 autistic and 41 ADHD participants highlighted a process whereby many participants embraced their authentic selves, often facilitated by the clarity and validation that diagnosis provided (1.4 Authenticity). Participants in these studies noted their diagnosis provided them with ‘permission’ to be themselves, with some participants noting they now felt “free.”30,44 Some studies reported that participants experienced greater happiness with who they are following their diagnosis, no longer feeling a need to fit into social norms. Five studies60,67,68,72,75 reported participants experiencing a greater sense of self-authenticity following their diagnosis. Autistic participants most commonly described this experience of being “authentic”; however, a small proportion of participants diagnosed with ADHD also noted the process of being diagnosed had allowed them to “just be me” 44 and be content with who they are.
Theme 2: Finding the self through others
Four subthemes were identified within this overarching theme of Finding the self through others: 2.1 Belonging; 2.2 Social comparisons; 2.3 Masking; and 2.4 Managing disclosure. Some participants underwent a process of developing their self-concept shaped by their relationships, social roles, and group memberships. This also involved navigating the connection and tension between the internal self and external societal views.
Across ten studies involving 100 autistic and 29 ADHD participants, a number of participants described developing feelings of belonging and validation through connections with others who shared and affirmed their neurodivergent experiences (2.1 Belonging). Multiple studies highlighted participants’ longstanding struggles to belong in groups of neurotypical peers, with one noting, “I just didn’t fit in, and I felt terrible.” 26 Following diagnosis, a participant noted that their newfound diagnosis “robs you of that right to be like everyone else.” 26 Across studies, participants described gaining a sense of belonging and identity through connections with others who shared similar experiences. Participants occasionally described this as a “club”28,44 or a “tribe.”43,75 Studies described participants’ growing acceptance and belonging through connections with others sharing neurodivergent experiences, exemplified by one participant: “[belonging] somewhere with other people somewhere who are like me.” 30 Participants, particularly in studies of late autism diagnosis, valued peer support, noting that sharing experiences helped develop self-understanding.
Nine studies comprising 100 autistic and 33 ADHD participants found that participants made sense of themselves by comparing their traits and experiences to those of others (2.2 Social comparisons). Many felt different or like an “alien” 26 but didn’t realize “what it was.”26,65 Postdiagnosis, connections with others, often online, supported identity development and validation, as one participant explained: “because you read things and you’re like, that’s me and that’s me and that’s also me.” 43 Certain studies observed participants felt devalued by comparisons, with one noting a participant “didn’t want to be worse than other people.” 28 Some also compared themselves to ‘neurotypical people’ with one participant in a study reporting that “it must be boring to be neurotypical.” 44 Participants navigated stereotypes, including disbelief that “disability could look like me,” 61 with autistic individuals questioning their diagnosis due to life successes (“I have a job, I have a wife, I can speak” 43 ) and facing skepticism from others who believed they “seem completely normal.” 43 This experience hindered diagnosis, as clinicians’ preconceived expectations led them to say ‘you can’t have Asperger’s’ and ‘you can’t be autistic,’” since the participant had finished university, had children, or had a job. 72 In ADHD participants, one study 64 linked social comparisons to gendered expectations, with participants reporting added challenges: “women are expected to be able to do all the clean-up and routine work,” and, as one noted, “people think you’re a bad mother” for being late to take her child to day care.
In five studies comprised of 52 autistic and 58 ADHD participants, authors described participants adopting different personas or “masks” to meet social expectations, often resulting in a fragmented identity (2.3 Masking). Both autistic and ADHD individuals reported switching between multiple versions of themselves. One ADHD participant described this as “having the gift of being multiple people at once,” 73 while an autistic participant reported that they had “just kind of been all these characters and I didn’t know who I was.” 67 In ADHD participants, they referred to the experience as having different personalities, “the one on medication or the one off medication.” 44 Studies described the experience of playing roles, with autistic participants noting that they often feel like “performers.” 67 One ADHD participant 74 noted that their life is “chaotic, but that’s behind the scenes,” and they maintain a pretence to avoid seeming “pitiful” to others. Following diagnosis, studies exploring late autism diagnoses reported challenges with fully unmasking or revealing authentic selves, with participants having spent years hiding their true identity. One participant reported, “I’m so good at trying to be neurotypical that I’ve forgotten how to be autistic.” 43
Four studies, of 29 autistic and 21 ADHD participants, reported that a number of participants navigated challenges in disclosing their diagnosis, balancing openness and privacy by selectively sharing with trusted individuals (2.4 Managing disclosure). Fear of judgment led some participants to conceal their diagnosis or cite alternative conditions to minimize stigma, as one explained: “I say that I have dyslexia, ADHD sounds so ugly in everyday speech.” 28 One ADHD participant reported that they do not tell anyone about their diagnosis as they “don’t want to seem too stupid.” 28 Another autistic participant reported fears that others will “see me differently” 68 if they were to disclose their diagnosis. Selective disclosure was common, with participants comfortable sharing their diagnoses with individuals they were emotionally close with, but being guarded in professional settings, as one noted: “professionally I’ve been really guarded because I don’t want anyone to judge me.” 75 Some participants claimed they met only certain criteria of their diagnosis, as one noted: “I say that I have ADHD and that I have only two things in it … they shouldn’t think that I have everything.” 28
Theme 3: Emotional integration of the self
Four subthemes: 3.1 Adjusting to permanence; 3.2 Feeling defective; 3.3 Growth in self-kindness; and 3.4 Self-acceptance underpinned Theme 3: Emotional integration of the self. Many participants went on an internal journey to emotionally come to terms with their identity, often struggling with challenging emotions, internalized negativity, and ultimately moving toward viewing themselves in a kinder way. While Theme 1 explored the cognitive and existential reinterpretation of identity postdiagnosis, this theme focuses more closely on the emotional dimensions of that journey. Namely, how participants processed their sense of worth, shame, and kindness toward themselves.
Seven studies of 21 autistic and 86 ADHD participants described the emotional and cognitive process of many participants in coming to terms with the lifelong nature of their diagnosis, including feelings of grief and overwhelm, exemplified by one participant who described it as “like a bad disease that I can never cure.” 64 (3.1 Adjusting to permanence). One participant noted that the idea of being “stuck like this forever” was “a bit overwhelming.” 30 Several studies reported that participants expressed confusion and doubt about how to interpret their diagnosis and its implications for their identity and future. A subset of participants believed that the diagnosis did not alter who they were but rather provided additional understanding of an already existing self, with some describing this as being “still me.”28,44
Existing research also noted that participants’ internalized shame, stigma, and self-blame before and during the diagnostic process contributed to their interpretation of neurodivergent traits as personal flaws (3.2 Feeling defective). Twelve studies of 109 autistic and 220 ADHD participants found that participants frequently viewed themselves as “different,” often perceiving these differences as flaws, which contributed to low self-confidence prior to diagnosis. A minority of participants reported a further decrease in self-confidence following diagnosis, describing it as something that “robs” them of confidence. 26 Another participant associated their diagnosis as making them “worth less” than others. 26 In certain studies, researchers noted that some participants experienced deep feelings of personal failure, interpreting these failures as reflections of their character. For example, an autistic participant and an ADHD participant both described feeling like a “bad person.”26,28 Multiple studies reported longstanding self-blame, as participants experienced certain behaviors being associated with negative qualities such as “lazy.” 70 Following their diagnosis, a number of participants struggled due to their adoption of negative societal views about autism and ADHD. These views created internalized stigma, with one participant reporting that “her diagnosis of autism and ADHD ‘crossed the line and I couldn’t cope with it because of my own internalized ableism.’” 69
In 11 studies of 152 autistic and 149 ADHD participants, authors described the process reported by participants in cultivating self-compassion and embracing their strengths following diagnosis (3.3 Growth in self-kindness). This included forgiving themselves for past difficulties and recognizing they were not to blame, as reflected in participants reporting “I intend to forgive myself for the past” 63 and “I am much more likely to give myself a break for not having done stuff.” 44 Some studies reported that participants with ADHD began to embrace positive traits associated with their diagnosis, for example, they can “think creatively,” 27 are “spontaneous,” 25 and “go with the flow.” 64 They learned to shift from self-criticism to being kind to themselves and work within their differences. Multiple participants also described feeling “empowered”60,63 and strengthened by this diagnosis, giving them a sense of control and a more positive identity.
Ten of the included studies, comprising 41 autistic and 148 ADHD participants, described participants’ journeys toward embracing their diagnosis and developing a more stable and positive self-view, characterized by increased self-confidence, self-worth, and self-acceptance (3.4 Self-acceptance). The concept of ‘acceptance’ was frequently reported, with some participants expressing sentiments such as being “accepting of who I am”68,75 and learning to “accept those things about myself that I really cannot change.” 63 Although many participants reported low confidence prior to diagnosis, some studies indicated that the diagnosis encouraged individuals to “like myself a bit more” 44 and see themselves “as ‘a human.’” 69
Discussion
We synthesized qualitative evidence from 25 studies exploring identity development following a late diagnosis of autism and/or ADHD in adulthood, generating a comprehensive picture of current evidence to inform clinical practice. Our analysis identified three superordinate themes, representing the experiences of over 600 adults diagnosed with autism and/or ADHD in adulthood. These themes (1: Reconfiguring the self, 2: Finding the self through others, and 3: Emotional integration of the self) reflect a complex intrapersonal and interpersonal process of adaptation.
Receiving a diagnosis prompted a reinterpretation of the past and present self-conceptions, leading to increased self-understanding and, in some cases, self-acceptance. This supports existing literature suggesting that autism and ADHD diagnoses can trigger shifts in identity.77,78 However, late-diagnosed adults often experience confusion and doubt during identity reconstruction, highlighting the support needs of late-diagnosed adults navigating such transitions.
Social identity processes played a central role. Participants re-negotiated their sense of belonging across neurotypical and neurodivergent contexts. For many, connecting with others who shared similar experiences fostered their sense of self, aligning with evidence that social connection enhances quality of life for autistic and ADHD individuals.79,80 Some participants grappled with social comparisons and found it difficult to reconcile societal expectations with their diagnosis. These tensions were associated with reduced self-compassion and well-being. 75 In ADHD research, stereotyping is more commonly associated with internalized societal stigma (e.g., Mueller et al. 81 ). Disclosure of diagnosis involved strategic choices about who to tell and how much to share. Because studies rarely reported on co-occurring conditions, we could not determine whether individuals feel more comfortable disclosing their ADHD or autism diagnosis. Social Identity Theory 42 helps explain how diagnosis acted as a social label that enabled participants to reclassify themselves into meaningful groups, reconstruct their identity, and foster a sense of belonging that supported self-understanding. Participants’ experiences of seeking validation, acceptance, and empowerment through neurodivergent communities reflect Social Identity Theory’s focus on in-group identification and social comparison. However, Social Identity Theory only partially accounts for the complexity of identity reconstruction and internalized stigma observed in this review.
Participants also described a journey of grief, stigma, and self-doubt, alongside empowerment and self-compassion. These findings align with previous research on postdiagnostic identity development, which highlights the emotional labor involved in overcoming internalized stigma and achieving a greater self-understanding. 62 Receiving a late diagnosis of autism or ADHD can disrupt an individual’s existing life narrative, prompting a reinterpretation of past experiences and integration of new understandings. These emotional processes reflect the inherent challenge of reconstructing a coherent self-concept after a diagnosis that redefines past and present experiences. Narrative identity theory 45 contextualizes this process by framing identity as an evolving life story that provides coherence and meaning to one’s experiences.
These findings suggest that identity formation following a late autism or ADHD diagnosis is a complex interplay of reflection, emotional processing, and social negotiation. Across all studies, diagnosis often served as a pivotal moment, prompting individuals to reconsider personal meaning, social belonging, and self-narratives. While many participants experienced empowerment, self-compassion, and affirmation, others reported confusion, doubt, and distress, indicating that identity reconstruction can involve both positive and challenging experiences. These processes were influenced by systemic factors such as public discourse, stigma, and access to affirming spaces.
Parallels and distinctions between autistic and ADHD identity
This review uniquely examines the prevalence of particular experiences between autistic and ADHD populations. Given the high rates of co-occurrence,3,4 it is particularly important to explore experiences that may be condition-specific rather than shared across groups. Although we could not control for co-occurring diagnoses (i.e., participants diagnosed with both autism and ADHD), certain experiences occurred more frequently in autism studies than in ADHD studies. Among the 13 autism-focused studies, all highlighted experiences of authenticity, reframing perceptions, and navigating social comparisons and group belonging. Autistic adults frequently described using their diagnosis to reinterpret past social experiences and situate themselves within supportive communities, reflecting a strong emphasis on social identity processes. In contrast, of the 12 ADHD-focused studies, 10 reported experiences of negative self-views, adjusting to permanence, and self-acceptance. Participants described chronic self-criticism and feelings of failure linked to societal expectations, highlighting an intrapersonal focus on identity reconstruction. These findings echo existing literature showing that ADHD adults frequently experience chronic self-criticism and a sense of failure due to societal invalidation of the condition. 82 However, researchers should approach direct comparisons with caution due to overlap and co-occurrence of conditions, as well as methodological differences across studies. Limited reporting of co-occurring autism and ADHD prevented us from rigorously exploring these differences. Future research should explore this area more thoroughly, including studies that directly compare experiences in autism, ADHD, and co-occurring autism-ADHD (AuDHD) populations. Autism interventions may focus on fostering community connection and reframing personal narratives, whereas ADHD supports should emphasize positive self-perception and integration of the diagnosis into one’s self-concept. Taken together, our review shows identity reconstruction involves both condition-specific and shared challenges, suggesting a need for personalized support addressing social and intrapersonal factors.
Parallels with other underserved groups
These findings align with identity development processes observed in other underserved communities. Like LGBTQIA+ individuals83,84 and ethnic minority groups, 85 autistic and ADHD adults navigate complex processes of identity disclosure, internalized stigma, and societal pressures, including workplace demands86,87; Minority Stress Theory, 46 originally developed in the context of LGBTQIA+ populations, helps explain these experiences. Participants reported long-term stress from being misunderstood and internalizing negative societal messages, with cumulative distal and proximal stressors persisting due to unmet support needs. Consistent with this theory, identity concealment contributed to psychological distress, while social support mitigated these effects, illustrating that neurodivergent identity formation involves internalized stigma, concealment, and community-mediated resilience, highlighting the importance of an intersectional approach.
Limitations of the included studies
The included studies provided valuable insights but also presented several limitations that readers should consider when interpreting this review. The most commonly reported limitation was sample homogeneity. The sample was predominantly White (49%) and female (44%), with substantial missing data for gender, ethnicity, LGBTQIA+ status, and socioeconomic status. This limits the generalizability of findings, particularly for individuals from underserved groups. Autism and ADHD continue to be underdiagnosed in minority ethnic groups.19,88 Existing literature notably underrepresents First Nations peoples, reflecting broader inequities in access to diagnosis and research participation. This gap restricts understanding of identity development in cultural contexts shaped by colonization, community frameworks, and distinct health system barriers. The large proportion of female participants likely reflects diagnostic biases that shape which individuals reach adulthood without recognition. However, this overrepresentation reduces the representativeness of men and non-binary participants whose experiences may differ from those captured in the current review. Given the marginalization of non-binary voices in research, future studies should seek to center these voices to better understand their unique perspectives. Future studies should explore cultural perspectives on neurodivergence and the barriers that contribute to delayed diagnosis. Although the qualitative studies offered rich insights, the small sample sizes limit generalizability. In addition, recruitment bias may have led to overrepresentation of individuals more accepting of their diagnoses, and underrepresenting those who reject or distance themselves from their neurodivergent identity. The lack of longitudinal data restricts insight into how identity evolves over time. These limitations suggest that the themes identified, while meaningful, may not fully capture the complexity and diversity of identity development in late-diagnosed adults. Robust designs are needed to ensure that post-diagnostic supports meet the needs of all individuals.
Strengths and limitations of the present review
Although previous research has examined neurodivergent identity more generally or across the lifespan, this review specifically synthesizes findings related to identity formation in adults diagnosed later in life. This group faces distinct challenges, including negative impacts on well-being 68 likely due to missed opportunities for support services and interventions. 89 These challenges have received limited attention in prior reviews.
This review is not without limitations, including that we did not involve independent community members. It is important to note, however, that two members of the research team are members of the neurodivergent community, and we approached this research with sensitivity to the needs and perspectives of the neurodivergent population. A second limitation relates to the search strategy. The initial search likely missed some relevant literature, as indicated by the inclusion of additional studies following backwards chain searching. Nonetheless, this iterative approach strengthened the review by reducing the risk of missing relevant studies. This review focused exclusively on adults with a formal diagnosis to ensure specificity. While this provides clarity on identity development following official recognition, it excludes individuals who self-identify, and no data was provided by articles on whether individuals self-identified prior to formal diagnosis. Self-identification has also been shown to foster self-understanding and acceptance. 85 Adults who self-identify as autistic or having ADHD often struggle to access support and experience loss of opportunities due to stigma. 90 While no authors described statistics on self-identification prior to diagnosis, Wylie’s 91 model suggests that individuals engage in a process of self-recognition before receiving a clinical diagnosis, which could shape identity development in ways not captured here. For the present review, focusing on formally diagnosed adults allowed this review to more clearly examine how clinical recognition shapes identity. The focus on peer-reviewed, English-language studies and the inability to access one eligible paper may have introduced reporting bias. Participants with more prominent or positive identity experiences may have been overrepresented. Finally, while this review examines broad patterns across autistic and ADHD adults, it is important to recognize that neither group is monolithic in identity. These results therefore may not reflect the experiences of all autistic or ADHD individuals. Despite these limitations, the consistency of themes across the 25 studies suggests that the findings are reliable. Future research should systematically investigate how factors such as age at diagnosis and intersecting social identities influence identity development, to allow for a more nuanced understanding of individual differences and ensure that post-diagnostic supports are tailored to diverse needs.
We conducted this thematic synthesis using both first- and second-order data, yielding deep insights into participants’ experiences. As with all thematic synthesis, we applied a level of interpretability. However, we conducted the review rigorously and reproducibly. A co-rater supported the screening, data extraction, and quality assessment processes following established guidelines (e.g., Oliver et al. 53 ), enhancing the robustness of findings. We undertook coding with reflective discussions with the authorship team, comprised of senior researchers and clinicians with knowledge and experience in the field. This strengthens analytical depth and theoretical coherence. Based on the MMAT appraisal, most studies were moderate-to-high quality. Despite some methodological limitations and potential reporting bias, the consistency and richness of findings provide moderate confidence in the synthesized conclusions. Finally, this review uniquely integrates findings across both autism and ADHD populations, addressing a notable gap in existing literature.
Clinical implications
This review has clear implications for clinical practice and policy. It underscores the need for improvements in adult diagnostic pathways and post-diagnostic support for autistic and ADHD individuals. The importance of community support is evident, as participants consistently described its positive impact on well-being as a direct result of their connection with others (subtheme 2.1: Belonging). These findings highlight the role of peer networks in shaping identity and fostering resilience. Clinicians and organizations should offer post-diagnostic peer group programs that facilitate identity exploration, as participants highly valued the benefits from connection (subtheme 2.1: Belonging) and to openly discuss their diagnosis in safe spaces (subtheme 2.4: Managing disclosure). Clinical assessments should also move away from deficit-based language, which can reinforce internalized shame (subtheme 3.2: Feeling defective). Instead, assessments should align with a social model of disability by recognizing individuals’ adaptive traits, strengths, difficulties, and the systemic barriers they face.
Conclusions
We conducted this synthesis to provide a comprehensive account of identity formation in late-diagnosed autistic and/or ADHD adults. Across the 25 included studies, evidence suggests that receiving a diagnosis in adulthood prompts a complex reassessment of identity, with profound psychosocial implications. The challenges of delayed recognition, along with the availability of community, validation, and support, actively shape identity construction. These findings highlight a need for future work prioritizing the promotion of models of care that affirm the development of a positive neurodivergent identity.
Footnotes
Acknowledgments
P.M., A.S.R., B.P.J., and B.C.Y.L. designed the search strategy. P.M. ran the initial searches and completed data screening, data extraction, and quality assessments. M.L.B. contributed to data screening, data extraction, and quality assessments. P.M. drafted the initial article, and A.S.R., B.P.J., and B.C.Y.L. contributed to the final version of the article.
Authorship Confirmation Statement
This article has been submitted solely to Autism in Adulthood.
Data Availability
Template data collection forms and data extracted from included studies are available from the corresponding author upon reasonable request. Any additional materials used in this review are included in the Supplementary Data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This systematic review was funded under the Research Training Program (RTP) scholarship from the Australian Government.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.